BCI Training Effects on Chronic Stroke Correlate with Functional Reorganization in Motor-Related Regions: A Concurrent EEG and fMRI Study



Abstract
:1. Introduction
2. Materials and Methods
2.1. Subject
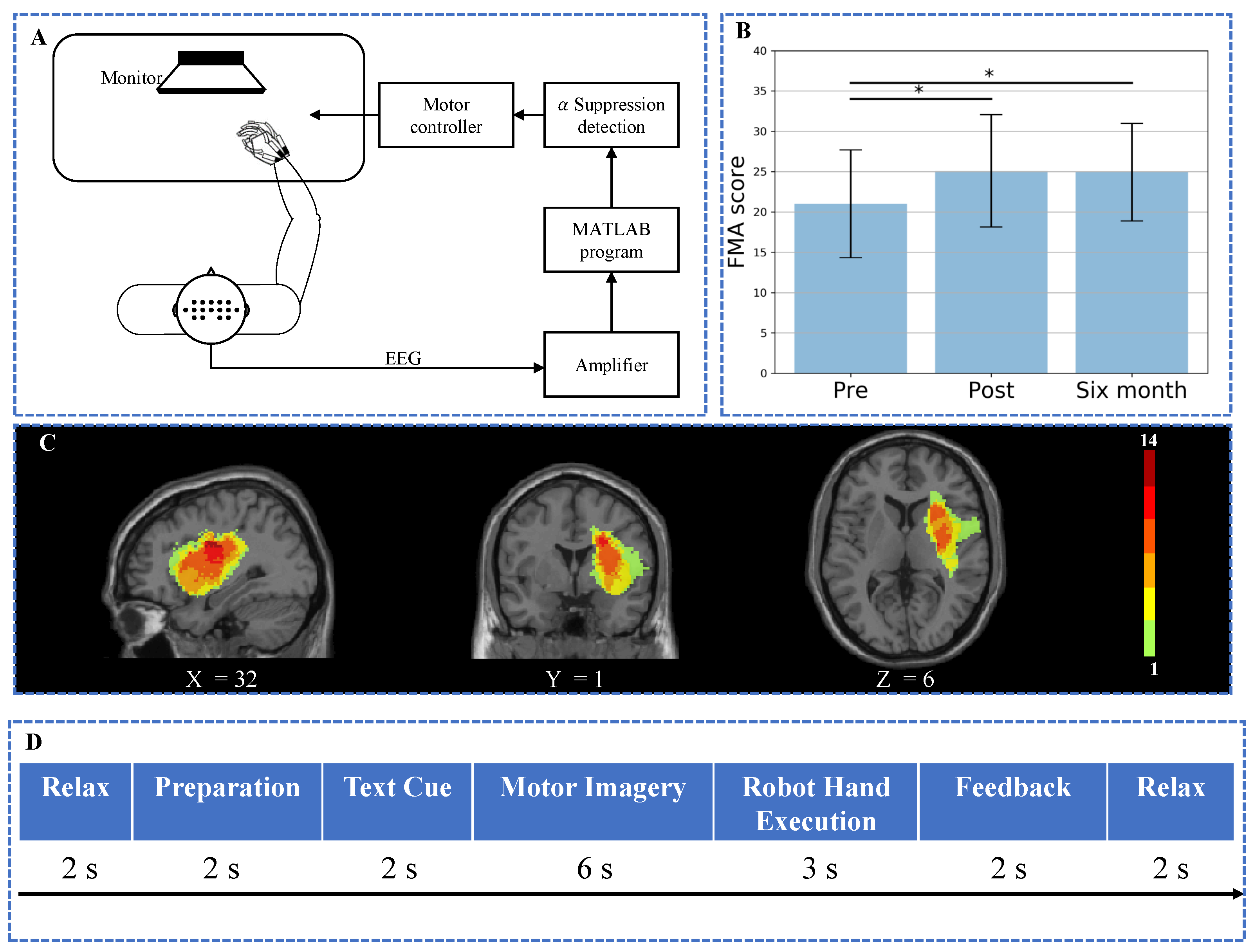
2.2. BCI Motor Imagery Training System
2.3. Interventional Protocols
2.4. MRI and EEG Data Acquisition
2.5. MRI Data Analysis
2.5.1. MRI Data Preprocessing
2.5.2. Seed-Based FC Analysis
2.6. EEG Analysis
2.6.1. EEG Preprocessing
2.6.2. Effective Connectivity Analysis
2.7. Statistics
3. Results
3.1. Results of Assessment Score
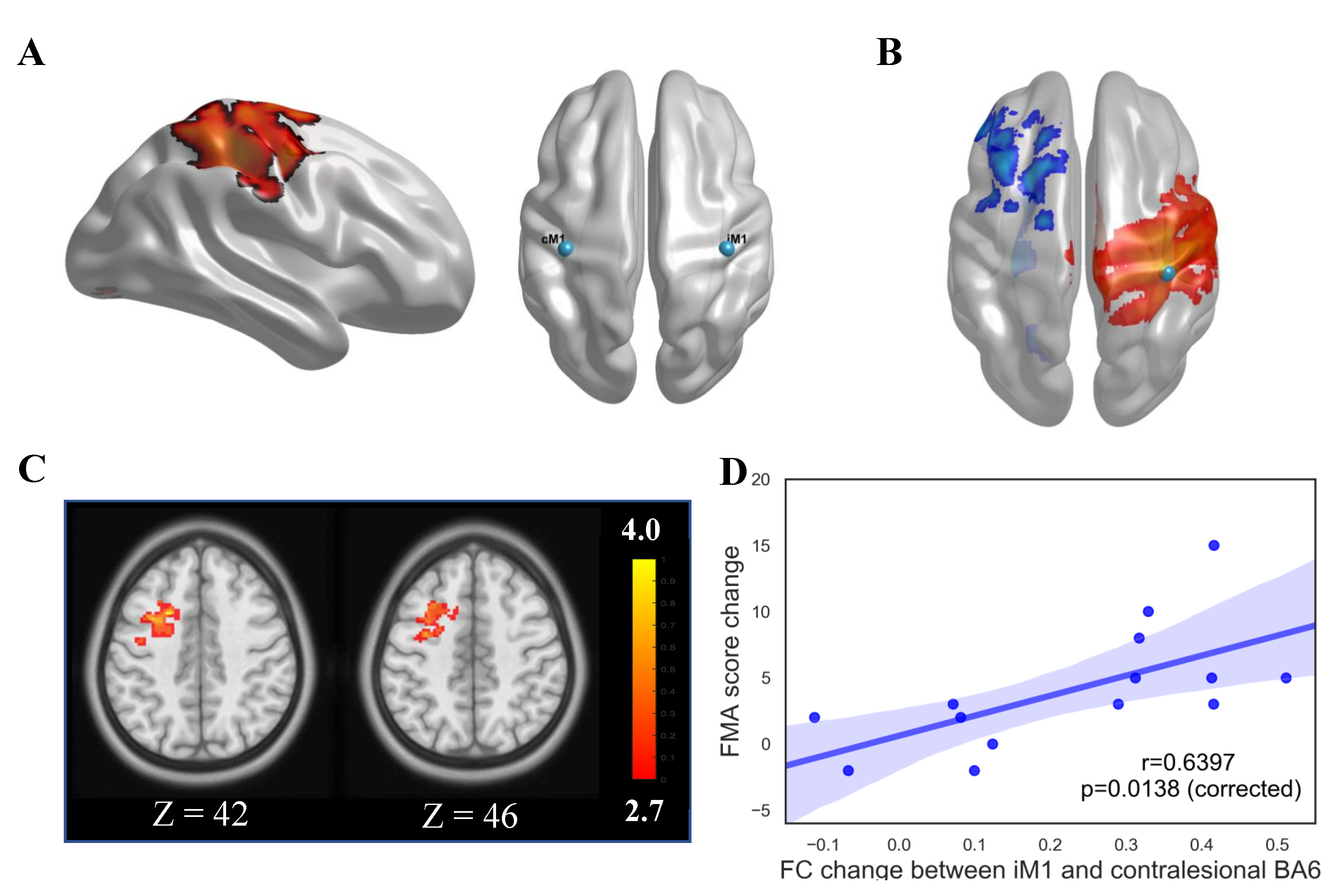
3.2. Results of Seed-Based FC Analysis
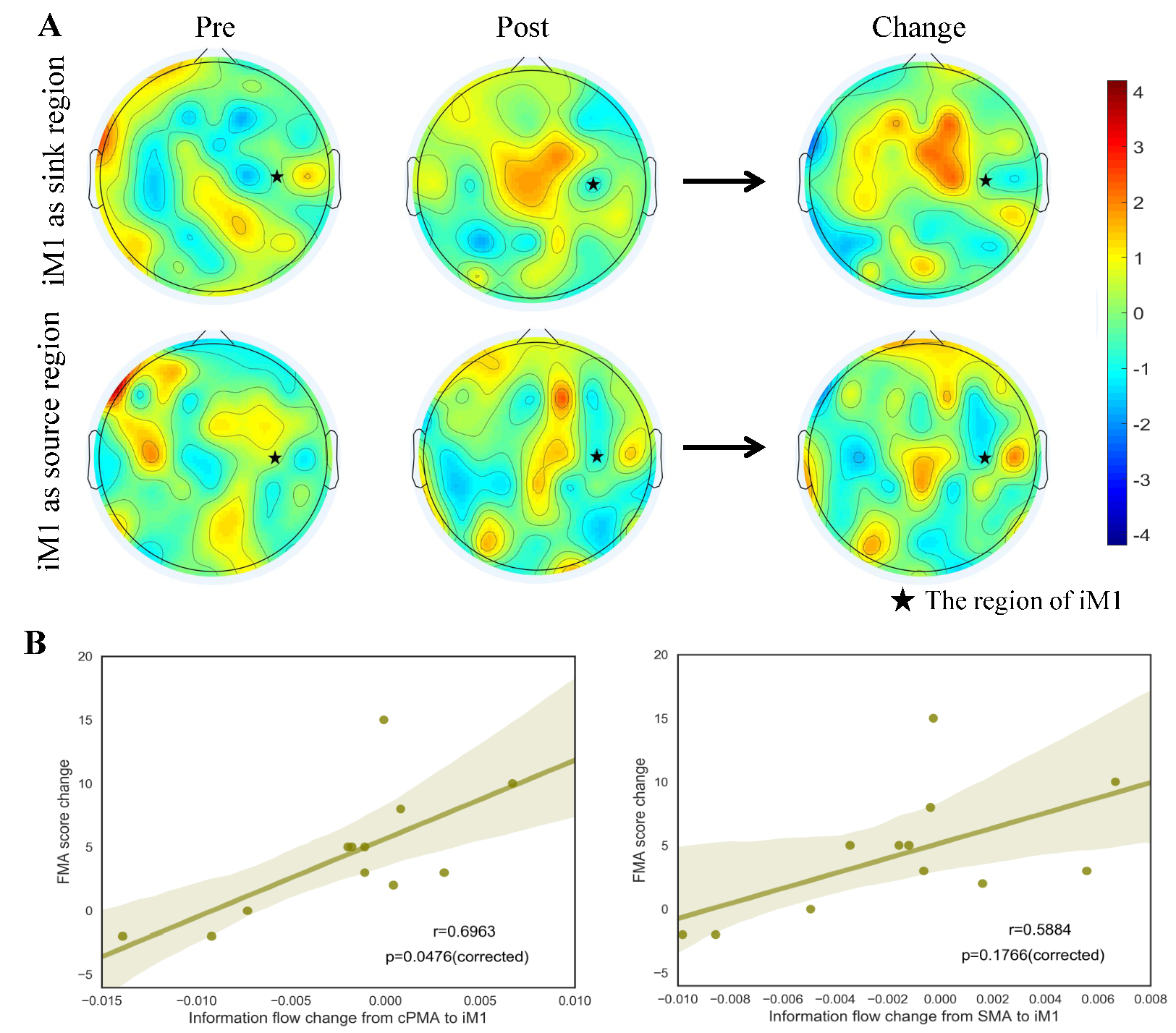
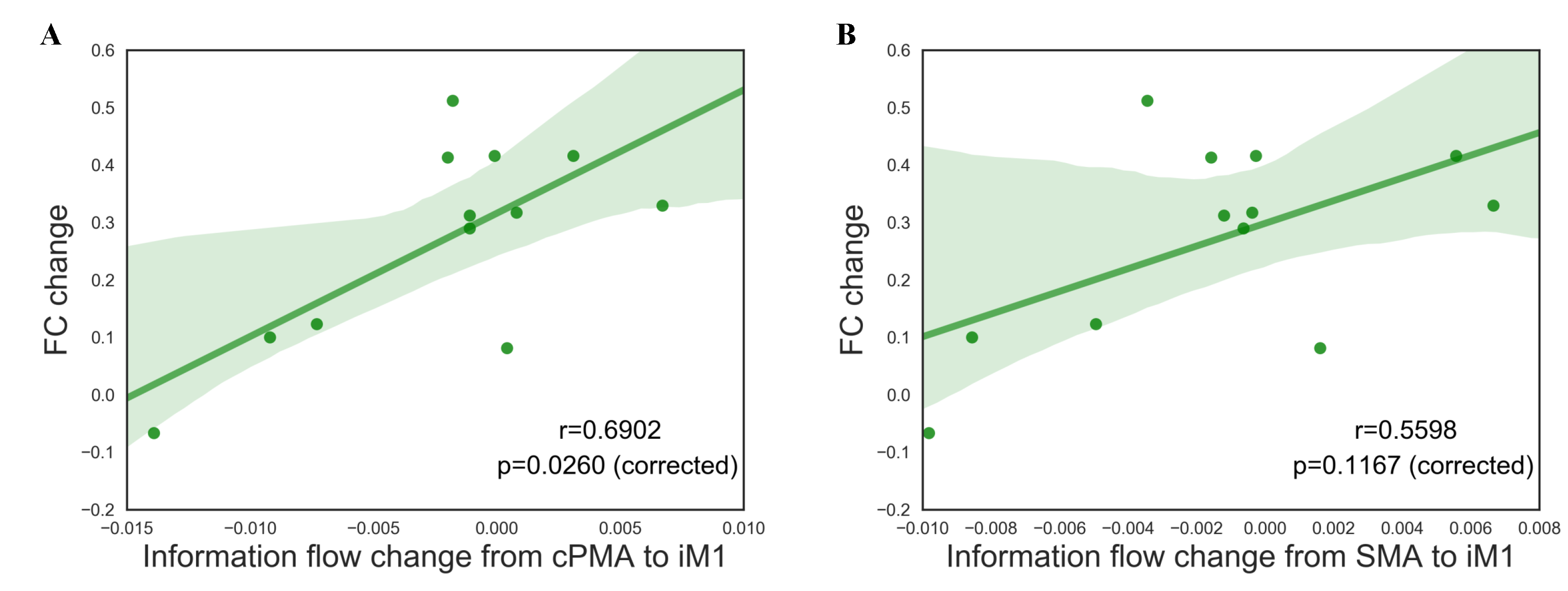
3.3. Results of Information Flow and Correlation Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wade, D. Measurement in neurological rehabilitation. Curr. Opin. Neurol. Neurosurg. 1992, 5, 682–686. [Google Scholar] [PubMed]
- Seitz, R.; Huang, Y.; Knorr, U.; Tellmann, L.; Herzog, H.; Freund, H. Large-scale plasticity of the human motor cortex. Neuroreport 1995, 6, 742–744. [Google Scholar] [CrossRef] [PubMed]
- Brewer, L.; Horgan, F.; Hickey, A.; Williams, D. Stroke rehabilitation: Recent advances and future therapies. QJM Int. J. Med. 2012, 106, 11–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hummel, F.C.; Cohen, L.G. Non-invasive brain stimulation: A new strategy to improve neurorehabilitation after stroke? Lancet Neurol. 2006, 5, 708–712. [Google Scholar] [CrossRef]
- Mane, R.; Chouhan, T.; Guan, C. BCI for stroke rehabilitation: Motor and beyond. J. Neural Eng. 2020, 17, 041001. [Google Scholar] [CrossRef]
- Broetz, D.; Braun, C.; Weber, C.; Soekadar, S.R.; Caria, A.; Birbaumer, N. Combination of Brain-Computer Interface Training and Goal-Directed Physical Therapy in Chronic Stroke: A Case Report. Neurorehabilit. Neural Repair 2010, 24, 674–679. [Google Scholar] [CrossRef]
- Prasad, G.; Herman, P.; Coyle, D.; McDonough, S.; Crosbie, J. Applying a brain-computer interface to support motor imagery practice in people with stroke for upper limb recovery: A feasibility study. J. Neuroeng. Rehabil. 2010, 7, 60. [Google Scholar] [CrossRef] [Green Version]
- Young, B.M.; Nigogosyan, Z.; Remsik, A.; Walton, L.M.; Song, J.; Nair, V.A.; Grogan, S.W.; Tyler, M.E.; Edwards, D.F.; Caldera, K.; et al. Changes in functional connectivity correlate with behavioral gains in stroke patients after therapy using a brain-computer interface device. Front. Neuroeng. 2014, 7, 25. [Google Scholar] [CrossRef] [Green Version]
- Ibáñez, J.; Monge-Pereira, E.; Molina-Rueda, F.; Serrano, J.I.; del Castillo, M.D.; Cuesta-Gómez, A.; Carratalá-Tejada, M.; Cano-de-la Cuerda, R.; Alguacil-Diego, I.M.; Miangolarra-Page, J.C.; et al. Low Latency Estimation of Motor Intentions to Assist Reaching Movements along Multiple Sessions in Chronic Stroke Patients: A Feasibility Study. Front. Neurosci. 2017, 11, 126. [Google Scholar] [CrossRef]
- Dobkin, B.H. Brain–computer interface technology as a tool to augment plasticity and outcomes for neurological rehabilitation. J. Physiol. 2007, 579, 637–642. [Google Scholar] [CrossRef]
- Bundy, D.T.; Wronkiewicz, M.; Sharma, M.; Moran, D.W.; Corbetta, M.; Leuthardt, E.C. Using ipsilateral motor signals in the unaffected cerebral hemisphere as a signal platform for brain–computer interfaces in hemiplegic stroke survivors. J. Neural Eng. 2012, 9, 036011. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biasiucci, A.; Leeb, R.; Iturrate, I.; Perdikis, S.; Al-Khodairy, A.; Corbet, T.; Schnider, A.; Schmidlin, T.; Zhang, H.; Bassolino, M.; et al. Brain-actuated functional electrical stimulation elicits lasting arm motor recovery after stroke. Nat. Commun. 2018, 9, 2421. [Google Scholar] [CrossRef]
- Soekadar, S.R.; Birbaumer, N.; Slutzky, M.W.; Cohen, L.G. Brain–machine interfaces in neurorehabilitation of stroke. Neurobiol. Dis. 2015, 83, 172–179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carter, A.R.; Shulman, G.L.; Corbetta, M. Why use a connectivity-based approach to study stroke and recovery of function? NeuroImage 2012, 62, 2271–2280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, X.; Seguin, C.; Zalesky, A.; Wong, W.W.; Chu, W.C.W.; Tong, R.K.Y. Synchronization lag in post-stroke: Relation to 1 motor function and structural connectivity. Netw. Neurosci. 2019, 3, 1121–1140. [Google Scholar] [CrossRef] [PubMed]
- Carter, A.R.; Astafiev, S.V.; Lang, C.E.; Connor, L.T.; Rengachary, J.; Strube, M.J.; Pope, D.L.W.; Shulman, G.L.; Corbetta, M. Resting interhemispheric functional magnetic resonance imaging connectivity predicts performance after stroke. Ann. Neurol. 2010, 67, 365–375. [Google Scholar] [CrossRef] [Green Version]
- Siegel, J.S.; Ramsey, L.E.; Snyder, A.Z.; Metcalf, N.V.; Chacko, R.V.; Weinberger, K.; Baldassarre, A.; Hacker, C.D.; Shulman, G.L.; Corbetta, M. Disruptions of network connectivity predict impairment in multiple behavioral domains after stroke. Proc. Natl. Acad. Sci. USA 2016, 113, E4367–E4376. [Google Scholar] [CrossRef] [Green Version]
- Da Silva, F.L. EEG and MEG: Relevance to Neuroscience. Neuron 2013, 80, 1112–1128. [Google Scholar] [CrossRef] [Green Version]
- Koenig, T.; Prichep, L.; Lehmann, D.; Sosa, P.V.; Braeker, E.; Kleinlogel, H.; Isenhart, R.; John, E. Millisecond by Millisecond, Year by Year: Normative EEG Microstates and Developmental Stages. NeuroImage 2002, 16, 41–48. [Google Scholar] [CrossRef]
- Friston, K.J. Functional and Effective Connectivity: A Review. Brain Connect. 2011, 1, 13–36. [Google Scholar] [CrossRef]
- Fasoula, A.; Attal, Y.; Schwartz, D. Comparative performance evaluation of data-driven causality measures applied to brain networks. J. Neurosci. Methods 2013, 215, 170–189. [Google Scholar] [CrossRef] [PubMed]
- Yeung, P.; Wong, L.; Chan, C.; Leung, J.; Yung, C. A validation study of the Hong Kong version of Montreal Cognitive Assessment (HK-MoCA) in Chinese older adults in Hong Kong. Hong Kong Med. J. 2014, 20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woodbury, M.L.; Velozo, C.A.; Richards, L.G.; Duncan, P.W. Rasch Analysis Staging Methodology to Classify Upper Extremity Movement Impairment After Stroke. Arch. Phys. Med. Rehabil. 2013, 94, 1527–1533. [Google Scholar] [CrossRef] [PubMed]
- Yuan, K.; Wang, X.; Chen, C.; Lau, C.C.Y.; Chu, W.C.W.; Tong, R.K.Y. Interhemispheric Functional Reorganization and its Structural Base After BCI-Guided Upper-Limb Training in Chronic Stroke. IEEE Trans. Neural Syst. Rehabil. Eng. 2020, 28, 2525–2536. [Google Scholar] [CrossRef] [PubMed]
- Tong, K.Y.; Pang, P.M.K.; Chen, M.; Ho, S.K.; Zhou, H.; Chan, T.W. Wearable Power Assistive Device for Helping a User to Move Their Hand. U.S. Patent 8574178B2, 5 November 2013. [Google Scholar]
- Kuhlman, W.N. Functional topography of the human mu rhythm. Electroencephalogr. Clin. Neurophysiol. 1978, 44, 83–93. [Google Scholar] [CrossRef]
- Choi, C.S.; Lim, H.; Kim, J.W.; Kang, Y.J.; Ku, J. Brain Computer Interface-Based Action Observation Game Enhances Mu Suppression in Patients with Stroke. Electronics 2019, 8, 1466. [Google Scholar] [CrossRef] [Green Version]
- Xu, K.; Huang, Y.Y.; Duann, J.R. The Sensitivity of Single-Trial Mu-Suppression Detection for Motor Imagery Performance as Compared to Motor Execution and Motor Observation Performance. Front. Hum. Neurosci. 2019, 13, 302. [Google Scholar] [CrossRef] [Green Version]
- Ono, T.; Shindo, K.; Kawashima, K.; Ota, N.; Ito, M.; Ota, T.; Mukaino, M.; Fujiwara, T.; Kimura, A.; Liu, M.; et al. Brain-computer interface with somatosensory feedback improves functional recovery from severe hemiplegia due to chronic stroke. Front. Neuroeng. 2014, 7, 19. [Google Scholar] [CrossRef]
- Perry, A.; Bentin, S. Mirror activity in the human brain while observing hand movements: A comparison between EEG desynchronization in the mu-range and previous fMRI results. Brain Res. 2009, 1282, 126–132. [Google Scholar] [CrossRef]
- Yan, C.G.; Wang, X.D.; Zuo, X.N.; Zang, Y.F. DPABI: Data Processing & Analysis for (Resting-State) Brain Imaging. Neuroinformatics 2016, 14, 339–351. [Google Scholar] [CrossRef]
- Chen, X.; Lu, B.; Yan, C.G. Reproducibility of R-fMRI metrics on the impact of different strategies for multiple comparison correction and sample sizes. Hum. Brain Mapp. 2018, 39, 300–318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delorme, A.; Makeig, S. EEGLAB: An open source toolbox for analysis of single-trial EEG dynamics including independent component analysis. J. Neurosci. Methods 2004, 134, 9–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oostenveld, R.; Fries, P.; Maris, E.; Schoffelen, J.M. FieldTrip: Open Source Software for Advanced Analysis of MEG, EEG, and Invasive Electrophysiological Data. Comput. Intell. Neurosci. 2011, 2011, 156869. [Google Scholar] [CrossRef] [PubMed]
- Niazy, R.; Beckmann, C.; Iannetti, G.; Brady, J.; Smith, S. Removal of FMRI environment artifacts from EEG data using optimal basis sets. NeuroImage 2005, 28, 720–737. [Google Scholar] [CrossRef] [PubMed]
- Granger, C.W.J. Investigating Causal Relations by Econometric Models and Cross-spectral Methods. Econometrica 1969, 37, 424–438. [Google Scholar] [CrossRef]
- Baccala, L.A.; Sameshima, K.; Takahashi, D.Y. Generalized Partial Directed Coherence. In Proceedings of the 2007 15th International Conference on Digital Signal Processing, Cardiff, UK, 1–4 July 2007; pp. 163–166. [Google Scholar] [CrossRef]
- Kay, S. Modern Spectral Estimation: Theory and Application/Book and Disk; Prentice-Hall Signal Processing Series: Advanced Monographs; PTR Prentice Hall: Upper Saddle River, NJ, USA, 1988. [Google Scholar]
- Coito, A.; Genetti, M.; Pittau, F.; Iannotti, G.R.; Thomschewski, A.; Höller, Y.; Trinka, E.; Wiest, R.; Seeck, M.; Michel, C.M.; et al. Altered directed functional connectivity in temporal lobe epilepsy in the absence of interictal spikes: A high density EEG study. Epilepsia 2016, 57, 402–411. [Google Scholar] [CrossRef] [Green Version]
- Astolfi, L.; Cincotti, F.; Mattia, D.; De Vico Fallani, F.; Tocci, A.; Colosimo, A.; Salinari, S.; Marciani, M.G.; Hesse, W.; Witte, H.; et al. Tracking the Time-Varying Cortical Connectivity Patterns by Adaptive Multivariate Estimators. IEEE Trans. Biomed. Eng. 2008, 55, 902–913. [Google Scholar] [CrossRef]
- Gerloff, C.; Richard, J.; Hadley, J.; Schulman, A.E.; Honda, M.; Hallett, M. Functional coupling and regional activation of human cortical motor areas during simple, internally paced and externally paced finger movements. Brain 1998, 121, 1513–1531. [Google Scholar] [CrossRef]
- Pagnotta, M.F.; Plomp, G. Time-varying MVAR algorithms for directed connectivity analysis: Critical comparison in simulations and benchmark EEG data. PLoS ONE 2018, 13, e0198846. [Google Scholar] [CrossRef]
- Groppe, D.M.; Bickel, S.; Keller, C.J.; Jain, S.K.; Hwang, S.T.; Harden, C.; Mehta, A.D. Dominant frequencies of resting human brain activity as measured by the electrocorticogram. NeuroImage 2013, 79, 223–233. [Google Scholar] [CrossRef] [Green Version]
- Kim, T.; Kim, S.; Lee, B. Effects of Action Observational Training Plus Brain–Computer Interface-Based Functional Electrical Stimulation on Paretic Arm Motor Recovery in Patient with Stroke: A Randomized Controlled Trial. Occup. Ther. Int. 2016, 23, 39–47. [Google Scholar] [CrossRef] [PubMed]
- Page, S.J.; Fulk, G.D.; Boyne, P. Clinically Important Differences for the Upper-Extremity Fugl-Meyer Scale in People with Minimal to Moderate Impairment Due to Chronic Stroke. Phys. Ther. 2012, 92, 791–798. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teasell, R.; Hussein, N. Stroke Rehabilitation Clinician Handbook 2020. 2020, p. 34. Available online: http://www.ebrsr.com/clinician-handbook (accessed on 5 November 2020).
- Gandolfi, M.; Formaggio, E.; Geroin, C.; Storti, S.; Galazzo, I.; Bortolami, M.; Saltuari, L.; Picelli, A.; Waldner, A.; Manganotti, P.; et al. Quantification of Upper Limb Motor Recovery and EEG Power Changes after Robot-Assisted Bilateral Arm Training in Chronic Stroke Patients: A Prospective Pilot Study. Neural Plast. 2018, 2018, 1–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsieh, Y.W.; Wu, C.Y.; Liao, W.W.; Lin, K.C.; Wu, K.Y.; Lee, C.Y. Effects of Treatment Intensity in Upper Limb Robot-Assisted Therapy for Chronic Stroke: A Pilot Randomized Controlled Trial. Neurorehabilit. Neural Repair 2011, 25, 503–511. [Google Scholar] [CrossRef] [PubMed]
- Van Dokkum, L.; Ward, T.; Laffont, I. Brain computer interfaces for neurorehabilitation— Its current status as a rehabilitation strategy post-stroke. Ann. Phys. Rehabil. Med. 2015, 58, 3–8. [Google Scholar] [CrossRef] [Green Version]
- Carino-Escobar, R.I.; Carrillo-Mora, P.; Valdés-Cristerna, R.; Rodriguez-Barragan, M.A.; Hernandez-Arenas, C.; Quinzaños-Fresnedo, J.; Galicia-Alvarado, M.A.; Cantillo-Negrete, J. Longitudinal Analysis of Stroke Patients’ Brain Rhythms during an Intervention with a Brain-Computer Interface. Neural Plast. 2019, 2019, 7084618. [Google Scholar] [CrossRef] [PubMed]
- Vahdat, S.; Darainy, M.; Milner, T.E.; Ostry, D.J. Functionally Specific Changes in Resting-State Sensorimotor Networks after Motor Learning. J. Neurosci. 2011, 31, 16907–16915. [Google Scholar] [CrossRef] [Green Version]
- Askim, T.; Indredavik, B.; Vangberg, T.; Håberg, A. Motor Network Changes Associated With Successful Motor Skill Relearning After Acute Ischemic Stroke: A Longitudinal Functional Magnetic Resonance Imaging Study. Neurorehabilit. Neural Repair 2009, 23, 295–304. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Liu, H.; Wang, L. Relationship between functional connectivity and motor function assessment in stroke patients with hemiplegia: A resting-state functional MRI study. Neuroradiology 2016, 58, 503–511. [Google Scholar] [CrossRef]
- Urbin, M.A.; Hong, X.; Lang, C.E.; Carter, A.R. Resting-State Functional Connectivity and Its Association With Multiple Domains of Upper-Extremity Function in Chronic Stroke. Neurorehabilit. Neural Repair 2014, 28, 761–769. [Google Scholar] [CrossRef] [Green Version]
- Wu, J.; Srinivasan, R.; Kaur, A.; Cramer, S.C. Resting-state cortical connectivity predicts motor skill acquisition. NeuroImage 2014, 91, 84–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Westlake, K.P.; Nagarajan, S.S. Functional Connectivity in Relation to Motor Performance and Recovery After Stroke. Front. Syst. Neurosci. 2011, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, L.; Zhang, J.N.; Zhang, Y.; Yan, R.; Liu, H.; Qiu, M.G. Conditional Granger Causality Analysis of Effective Connectivity during Motor Imagery and Motor Execution in Stroke Patients. Biomed Res. Int. 2016, 2016, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, L.; Zhang, H.; Hui, M.; Long, Z.; Jin, Z.; Liu, Y.; Yao, L. Motor execution and motor imagery: A comparison of functional connectivity patterns based on graph theory. Neuroscience 2014, 261, 184–194. [Google Scholar] [CrossRef] [PubMed]
- Bajaj, S.; Butler, A.J.; Drake, D.; Dhamala, M. Brain effective connectivity during motor-imagery and execution following stroke and rehabilitation. NeuroImage Clin. 2015, 8, 572–582. [Google Scholar] [CrossRef] [Green Version]
- Baccalá, L.A.; Sameshima, K. Partial directed coherence: A new concept in neural structure determination. Biol. Cybern. 2001, 84, 463–474. [Google Scholar] [CrossRef]
- Britz, J.; Ville, D.V.D.; Michel, C.M. BOLD correlates of EEG topography reveal rapid resting-state network dynamics. NeuroImage 2010, 52, 1162–1170. [Google Scholar] [CrossRef]
- Brookes, M.J.; Woolrich, M.; Luckhoo, H.; Price, D.; Hale, J.R.; Stephenson, M.C.; Barnes, G.R.; Smith, S.M.; Morris, P.G. Investigating the electrophysiological basis of resting state networks using magnetoencephalography. Proc. Natl. Acad. Sci. USA 2011, 108, 16783–16788. [Google Scholar] [CrossRef] [Green Version]
- Lindenberg, R.; Zhu, L.L.; Rüber, T.; Schlaug, G. Predicting functional motor potential in chronic stroke patients using diffusion tensor imaging. Hum. Brain Mapp. 2012, 33, 1040–1051. [Google Scholar] [CrossRef] [Green Version]
- Song, J.; Nair, V.A.; Young, B.M.; Walton, L.M.; Nigogosyan, Z.; Remsik, A.; Tyler, M.E.; Farrar-Edwards, D.; Caldera, K.E.; Sattin, J.A.; et al. DTI measures track and predict motor function outcomes in stroke rehabilitation utilizing BCI technology. Front. Hum. Neurosci. 2015, 9, 195. [Google Scholar] [CrossRef] [Green Version]
- Werring, D.J.; Toosy, A.T.; Clark, C.A.; Parker, G.J.; Barker, G.J.; Miller, D.H.; Thompson, A.J. Diffusion tensor imaging can detect and quantify corticospinal tract degeneration after stroke. J. Neurol. Neurosurg. Psychiatry 2000, 69, 269–272. [Google Scholar] [CrossRef] [Green Version]
- Kierońska, S.; Sokal, P.; Dura, M.; Jabłońska, M.; Rudaś, M.; Jabłońska, R. Tractography-Based Analysis of Morphological and Anatomical Characteristics of the Uncinate Fasciculus in Human Brains. Brain Sci. 2020, 10, 709. [Google Scholar] [CrossRef] [PubMed]
- Borkowski, K.; Krzyżak, A.T. The generalized Stejskal-Tanner equation for non-uniform magnetic field gradients. J. Magn. Reson. 2018, 296, 23–28. [Google Scholar] [CrossRef] [PubMed]
- Rudrapatna, U.; Parker, G.D.; Roberts, J.; Jones, D.K. A comparative study of gradient nonlinearity correction strategies for processing diffusion data obtained with ultra-strong gradient MRI scanners. Magn. Reson. Med. 2021, 85, 1104–1113. [Google Scholar] [CrossRef]
- Draganski, B.; May, A. Training-induced structural changes in the adult human brain. Behav. Brain Res. 2008, 192, 137–142. [Google Scholar] [CrossRef] [PubMed]
- Young, B.M.; Stamm, J.M.; Song, J.; Remsik, A.B.; Nair, V.A.; Tyler, M.E.; Edwards, D.F.; Caldera, K.; Sattin, J.A.; Williams, J.C.; et al. Brain–Computer Interface Training after Stroke Affects Patterns of Brain–Behavior Relationships in Corticospinal Motor Fibers. Front. Hum. Neurosci. 2016, 10, 457. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Stroke | FMA (Max Score: 66) | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Age | Onset | Lesion | Stroke | ||||||
| No. | Range | Gender | (Years) | Side | Lesion Location | Type | Pre | Post | Six Month |
| S1 | 45–49 | M | 1 | R | MFG, SFG, precentral, | I | 19 | 34 | 28 |
| supramarginal, SMA | |||||||||
| S2 | 65–69 | M | 8 | L | insula, putamen, IFG, | H | 22 | 27 | 32 |
| temporal pole | |||||||||
| S3 | 65–69 | M | 1 | R | insula, ITG, IOG, | H | 13 | 16 | 27 |
| putamen | |||||||||
| S4 | 60–64 | M | 3 | R | insula, putamen, IFG | I | 16 | 14 | 18 |
| rolandic operculum | |||||||||
| S5 | 45–49 | M | 0.7 | R | ITG, MTG, STG, MOG, | H | 17 | 25 | 25 |
| angular, supramarginal | |||||||||
| S6 | 60–64 | M | 11 | L | PLIC, putamen, | I | 22 | 24 | 24 |
| insula, postcentral, SFG | |||||||||
| S7 | 55–59 | M | 6 | R | insula, IFG | I | 13 | 23 | 20 |
| rolandic operculum | |||||||||
| S8 | 40–44 | M | 5 | R | insula, rolandic operculum, IFG, | H | 15 | 17 | 16 |
| STG, putamen, temporal pole | |||||||||
| S9 | 50–54 | F | 3 | L | insula, rolandic operculum, | H | 34 | 34 | 37 |
| putamen | |||||||||
| S10 | 40–44 | M | 3 | R | insula, MTG, STG, temporal pole, | H | 17 | 20 | 20 |
| putamen, rolandic operculum | |||||||||
| S11 | 55–59 | M | 5 | L | insula, IFG, putamen | H | 28 | 33 | 24 |
| S12 | 50–54 | M | 1 | L | putamen, caudate nucleus | I | 24 | 22 | 22 |
| S13 | 55–59 | M | 7 | R | putamen, temporal pole, IFG, | I | 20 | 25 | 21 |
| insula, rolandic operculum | |||||||||
| S14 | 45–49 | M | 1 | R | insula, putamen | H | 34 | 37 | 35 |
| mean ± std | 21 ± 6.7 | 25 ± 7 | 25 ± 6 | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yuan, K.; Chen, C.; Wang, X.; Chu, W.C.-w.; Tong, R.K.-y. BCI Training Effects on Chronic Stroke Correlate with Functional Reorganization in Motor-Related Regions: A Concurrent EEG and fMRI Study. Brain Sci. 2021, 11, 56. https://doi.org/10.3390/brainsci11010056
Yuan K, Chen C, Wang X, Chu WC-w, Tong RK-y. BCI Training Effects on Chronic Stroke Correlate with Functional Reorganization in Motor-Related Regions: A Concurrent EEG and fMRI Study. Brain Sciences. 2021; 11(1):56. https://doi.org/10.3390/brainsci11010056
Chicago/Turabian StyleYuan, Kai, Cheng Chen, Xin Wang, Winnie Chiu-wing Chu, and Raymond Kai-yu Tong. 2021. "BCI Training Effects on Chronic Stroke Correlate with Functional Reorganization in Motor-Related Regions: A Concurrent EEG and fMRI Study" Brain Sciences 11, no. 1: 56. https://doi.org/10.3390/brainsci11010056