Neutrophil-to-Lymphocyte, Platelet-to-Lymphocyte and Monocyte-to-Lymphocyte Ratio in Bipolar Disorder

 ,
,  , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample
2.2. Assessments and Procedures
2.3. Statistical Analysis
3. Results
3.1. General Characteristics of the Sample
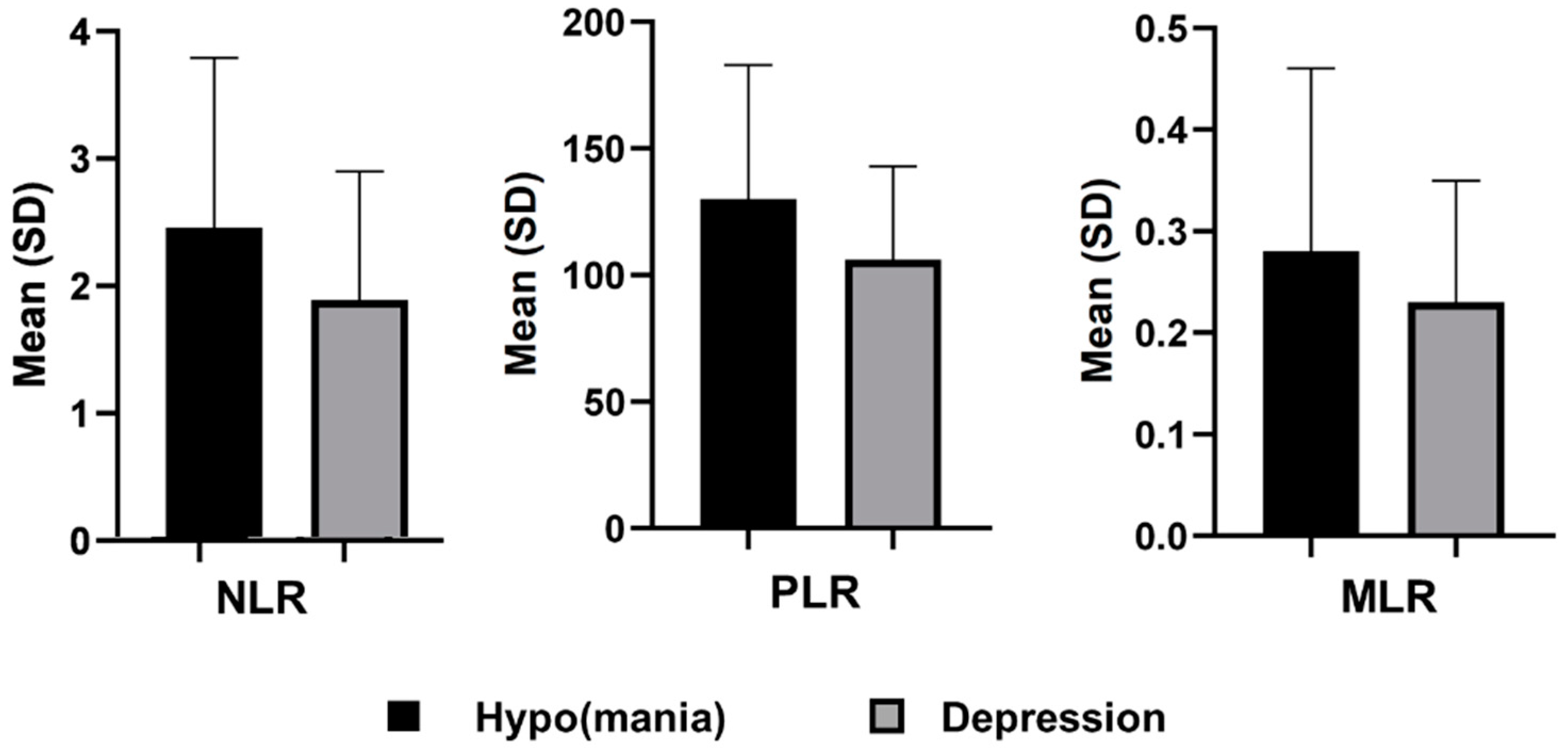
3.2. Complete Blood Count and Inflammatory Ratios: Differences between Major Depressive and (Hypo)manic Episode
3.3. Independent Predictors of (Hypo)manic Episodes
4. Discussion
4.1. Strengths and Limitations
4.2. Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Silva Ribeiro, J.; Pereira, D.; Salagre, E.; Coroa, M.; Santos Oliveira, P.; Santos, V.; Madeira, N.; Grande, I.; Vieta, E. Risk calculators in bipolar disorder: A systematic review. Brain Sci. 2020, 10, 525. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®); American Psychiatric Pub: Washington, DC, USA, 2013. [Google Scholar]
- Sigitova, E.; Fišar, Z.; Hroudová, J.; Cikánková, T.; Raboch, J. Biological hypotheses and biomarkers of bipolar disorder. Psychiatry Clin. Neurosci. 2017, 71, 77–103. [Google Scholar]
- Benedetti, F.; Aggio, V.; Pratesi, M.L.; Greco, G.; Furlan, R. Neuroinflammation in bipolar depression. Front. Psychiatry 2020, 11, 71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kowalczyk, M.; Szemraj, J.; Bliźniewska, K.; Maes, M.; Berk, M.; Su, K.P.; Gałecki, P. An immune gate of depression—Early neuroimmune development in the formation of the underlying depressive disorder. Pharmacol. Rep. 2019, 71, 1299–1307. [Google Scholar] [CrossRef] [PubMed]
- Maes, M.; Berk, M.; Goehler, L.; Song, C.; Anderson, G.; Gałecki, P.; Leonard, B. Depression and sickness behavior are janus-faced responses to shared inflammatory pathways. BMC Med. 2012, 10, 66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Najjar, S.; Pearlman, D.M.; Alper, K.; Najjar, A.; Devinsky, O. Neuroinflammation and psychiatric illness. J. Neuroinflamm. 2013, 10, 43. [Google Scholar]
- Rosenblat, J.D. Targeting the immune system in the treatment of bipolar disorder. Psychopharmacology 2019, 236, 2909–2921. [Google Scholar] [CrossRef]
- Fusar-Poli, L.; Surace, T.; Vanella, A.; Meo, V.; Patania, F.; Furnari, R.; Signorelli, M.S.; Aguglia, E. The effect of adjunctive nutraceuticals in bipolar disorder: A systematic review of randomized placebo-controlled trials. J. Affect. Disord. 2019, 252, 334–349. [Google Scholar] [CrossRef]
- Ashton, M.M.; Kavanagh, B.E.; Marx, W.; Berk, M.; Sarris, J.; Ng, C.H.; Hopwood, M.; Williams, L.J.; Dean, O.M. A systematic review of nutraceuticals for the treatment of bipolar disorder: Une revue systématique des nutraceutiques pour le traitement du trouble bipolaire. Can. J. Psychiatry 2020. [Google Scholar] [CrossRef]
- Misiak, B.; Bartoli, F.; Carrà, G.; Małecka, M.; Samochowiec, J.; Jarosz, K.; Banik, A.; Stańczykiewicz, B. Chemokine alterations in bipolar disorder: A systematic review and meta-analysis. BrainBehav. Immun. 2020, 88, 870–877. [Google Scholar] [CrossRef]
- Brietzke, E.; Kauer-Sant’Anna, M.; Teixeira, A.L.; Kapczinski, F. Abnormalities in serum chemokine levels in euthymic patients with bipolar disorder. BrainBehav. Immun. 2009, 23, 1079–1082. [Google Scholar] [CrossRef] [PubMed]
- Sayana, P.; Colpo, G.D.; Simoes, L.R.; Giridharan, V.V.; Teixeira, A.L.; Quevedo, J.; Barichello, T. A systematic review of evidence for the role of inflammatory biomarkers in bipolar patients. J. Psychiatr. Res. 2017, 92, 160–182. [Google Scholar] [CrossRef] [PubMed]
- Haarman, B.C.B.; Riemersma-Van der Lek, R.F.; de Groot, J.C.; Ruhé, H.G.E.; Klein, H.C.; Zandstra, T.E.; Burger, H.; Schoevers, R.A.; de Vries, E.F.; Drexhage, H.A. Neuroinflammation in bipolar disorder–a [11c]-(r)-pk11195 positron emission tomography study. BrainBehav. Immun. 2014, 40, 219–225. [Google Scholar] [CrossRef] [PubMed]
- Rao, J.S.; Harry, G.J.; Rapoport, S.I.; Kim, H.-W. Increased excitotoxicity and neuroinflammatory markers in postmortem frontal cortex from bipolar disorder patients. Mol. Psychiatry 2010, 15, 384–392. [Google Scholar] [CrossRef]
- Zulfic, Z.; Weickert, C.S.; Weickert, T.W.; Liu, D.; Myles, N.; Galletly, C. Neutrophil–lymphocyte ratio–a simple, accessible measure of inflammation, morbidity and prognosis in psychiatric disorders? Australas. Psychiatry 2020, 28, 454–458. [Google Scholar] [CrossRef]
- Çakır, U.; Can Tuman, T.; Yıldırım, O. Increased neutrophil/lymphoctye ratio in patients with bipolar disorder: A preliminary study. Psychiatr. Danub. 2015, 27, 180–184. [Google Scholar]
- Mert, D.G.; Terzi, H. Mean platelet volume in bipolar disorder: The search for an ideal biomarker. Neuropsychiatr. Dis. Treat. 2016, 12, 2057–2062. [Google Scholar] [CrossRef] [Green Version]
- Mayda, H.; Ahsen, A.; Bağcioğlu, E.; Öztürk, A.; Bahçeci, B.; Soyucok, E.; Başpinar, E.; Ulu, M.S. Effect of increased neutrophil-to-lymphocyte ratio (NLR) and decreased mean platelet volume (MPV) values on inflammation in acute mania. Nöro Psikiyatr. Arşivi 2016, 53, 317. [Google Scholar] [CrossRef] [Green Version]
- Kalelioglu, T.; Akkus, M.; Karamustafalioglu, N.; Genc, A.; Genc, E.S.; Cansiz, A.; Emul, M. Neutrophil-lymphocyte and platelet-lymphocyte ratios as inflammation markers for bipolar disorder. Psychiatry Res. 2015, 228, 925–927. [Google Scholar] [CrossRef]
- Sağlam Aykut, D.; Civil Arslan, F.; Özkorumak Karagüzel, E.; Aral, G.; Karakullukçu, S. The relationship between neutrophil-lymphocyte, platelet–lymphocyte ratio and cognitive functions in bipolar disorder. Nord. J. Psychiatry 2018, 72, 119–123. [Google Scholar] [CrossRef]
- Aguglia, A.; Amerio, A.; Asaro, P.; Caprino, M.; Conigliaro, C.; Giacomini, G.; Parisi, V.M.; Trabucco, A.; Amore, M.; Serafini, G. High-lethality of suicide attempts associated with platelet to lymphocyte ratio and mean platelet volume in psychiatric inpatient setting. World J. Biol. Psychiatry 2020, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Ekinci, O.; Ekinci, A. The connections among suicidal behavior, lipid profile and low-grade inflammation in patients with major depressive disorder: A specific relationship with the neutrophil-to-lymphocyte ratio. Nord. J. Psychiatry 2017, 71, 574–580. [Google Scholar] [CrossRef] [PubMed]
- Serafini, G.; Parisi, V.M.; Aguglia, A.; Amerio, A.; Sampogna, G.; Fiorillo, A.; Pompili, M.; Amore, M. A specific inflammatory profile underlying suicide risk? Systematic review of the main literature findings. Int. J. Environ. Res. Public Health 2020, 17, 2393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mazza, M.G.; Lucchi, S.; Tringali, A.G.M.; Rossetti, A.; Botti, E.R.; Clerici, M. Neutrophil/lymphocyte ratio and platelet/lymphocyte ratio in mood disorders: A meta-analysis. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2018, 84, 229–236. [Google Scholar] [CrossRef]
- Özdin, S.; Sarisoy, G.; Böke, Ö. A comparison of the neutrophil-lymphocyte, platelet-lymphocyte and monocyte-lymphocyte ratios in schizophrenia and bipolar disorder patients–a retrospective file review. Nord. J. Psychiatry 2017, 71, 509–512. [Google Scholar] [CrossRef]
- Mazza, M.G.; Tringali, A.G.M.; Rossetti, A.; Botti, R.E.; Clerici, M. Cross-sectional study of neutrophil-lymphocyte, platelet-lymphocyte and monocyte-lymphocyte ratios in mood disorders. Gen. Psychiatry 2019, 58, 7–12. [Google Scholar] [CrossRef]
- Rowland, T.; Perry, B.I.; Upthegrove, R.; Barnes, N.; Chatterjee, J.; Gallacher, D.; Marwaha, S. Neurotrophins, cytokines, oxidative stress mediators and mood state in bipolar disorder: Systematic review and meta-analyses. Br. J. Psychiatry 2018, 213, 514–525. [Google Scholar] [CrossRef] [Green Version]
- Brietzke, E.; Stertz, L.; Fernandes, B.S.; Kauer-Sant’Anna, M.; Mascarenhas, M.; Vargas, A.E.; Chies, J.A.; Kapczinski, F. Comparison of cytokine levels in depressed, manic and euthymic patients with bipolar disorder. J. Affect. Disord. 2009, 116, 214–217. [Google Scholar] [CrossRef]
- Kim, Y.-K.; Jung, H.-G.; Myint, A.-M.; Kim, H.; Park, S.-H. Imbalance between pro-inflammatory and anti-inflammatory cytokines in bipolar disorder. J. Affect. Disord. 2007, 104, 91–95. [Google Scholar] [CrossRef]
- Guloksuz, S.; Cetin, E.A.; Cetin, T.; Deniz, G.; Oral, E.T.; Nutt, D.J. Cytokine levels in euthymic bipolar patients. J. Affect. Disord. 2010, 126, 458–462. [Google Scholar] [CrossRef]
- van den Ameele, S.; van Diermen, L.; Staels, W.; Coppens, V.; Dumont, G.; Sabbe, B.; Morrens, M. The effect of mood-stabilizing drugs on cytokine levels in bipolar disorder: A systematic review. J. Affect. Disord. 2016, 203, 364–373. [Google Scholar] [CrossRef] [PubMed]
- Boufidou, F.; Nikolaou, C.; Alevizos, B.; Liappas, I.A.; Christodoulou, G.N. Cytokine production in bipolar affective disorder patients under lithium treatment. J. Affect. Disord. 2004, 82, 309–313. [Google Scholar] [CrossRef] [PubMed]
- Chou, Y.-H.; Hsieh, W.-C.; Chen, L.-C.; Lirng, J.-F.; Wang, S.-J. Association between the serotonin transporter and cytokines: Implications for the pathophysiology of bipolar disorder. J. Affect. Disord. 2016, 191, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Barbosa, I.G.; Bauer, M.E.; Machado-Vieira, R.; Teixeira, A.L. Cytokines in bipolar disorder: Paving the way for neuroprogression. Neural Plast. 2014, 2014, 360481. [Google Scholar] [CrossRef] [PubMed]
- Herr, N.; Bode, C.; Duerschmied, D. The effects of serotonin in immune cells. Front. Cardiovasc. Med. 2017, 4, 48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dietrich-Muszalska, A.; Wachowicz, B. Platelet haemostatic function in psychiatric disorders: Effects of antidepressants and antipsychotic drugs. World J. Biol. Psychiatry 2017, 18, 564–574. [Google Scholar] [CrossRef]
- Mann, J.J.; Arango, V.; Underwood, M.D. Serotonin and suicidal behavior. Ann. N. Y. Acad. Sci. 1990, 600, 476–484. [Google Scholar] [CrossRef]
- Spreux-Varoquaux, O.; Alvarez, J.; Berlin, I.; Batista, G.; Despierre, P.; Gilton, A.; Cremniter, D. Differential abnormalities in plasma 5-hiaa and platelet serotonin concentrations in violent suicide attempters relationships with impulsivity and depression. Life Sci. 2001, 69, 647–657. [Google Scholar] [CrossRef]
- Giurgiuca, A.; Schipor, S.; Caragheorgheopol, A.; Crasan, A.; Postolache, E.; Tudose, C.; Prelipceanu, D.; Cozman, D. Platelet serotonin as biomarker for assessing suicidal behaviour in patients with bipolar I disorder. Acta Endocrinol. (Bucharest) 2016, 12, 275–281. [Google Scholar] [CrossRef]
- Zahorec, R. Ratio of neutrophil to lymphocyte counts-rapid and simple parameter of systemic inflammation and stress in critically ill. Bratisl. Lek. Listy 2001, 102, 5–14. [Google Scholar]
- Anderson, G.; Maes, M. Bipolar disorder: Role of immune-inflammatory cytokines, oxidative and nitrosative stress and tryptophan catabolites. Curr. Psychiatry Rep. 2015, 17, 8. [Google Scholar] [CrossRef]
- Kim, Y.-K.; Na, K.-S.; Myint, A.-M.; Leonard, B.E. The role of pro-inflammatory cytokines in neuroinflammation, neurogenesis and the neuroendocrine system in major depression. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2016, 64, 277–284. [Google Scholar] [CrossRef] [PubMed]
- Dantzer, R.; O’Connor, J.C.; Freund, G.G.; Johnson, R.W.; Kelley, K.W. From inflammation to sickness and depression: When the immune system subjugates the brain. Nat. Rev. Neurosci. 2008, 9, 46–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brietzke, E.; Mansur, R.B.; Soczynska, J.; Powell, A.M.; McIntyre, R.S. A theoretical framework informing research about the role of stress in the pathophysiology of bipolar disorder. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2012, 39, 1–8. [Google Scholar] [CrossRef]
- Pfaffenseller, B.; Fries, G.R.; Wollenhaupt-Aguiar, B.; Colpo, G.D.; Stertz, L.; Panizzutti, B.; Magalhaes, P.V.; Kapczinski, F. Neurotrophins, inflammation and oxidative stress as illness activity biomarkers in bipolar disorder. Expert Rev. Neurother. 2013, 13, 827–842. [Google Scholar] [CrossRef] [PubMed]
- Beumer, W.; Gibney, S.M.; Drexhage, R.C.; Pont-Lezica, L.; Doorduin, J.; Klein, H.C.; Steiner, J.; Connor, T.J.; Harkin, A.; Versnel, M.A. The immune theory of psychiatric diseases: A key role for activated microglia and circulating monocytes. J. Leukoc. Biol. 2012, 92, 959–975. [Google Scholar] [CrossRef]
- Bustan, Y.; Drapisz, A.; Dor, D.H.B.; Avrahami, M.; Schwartz-Lifshitz, M.; Weizman, A.; Barzilay, R. Elevated neutrophil to lymphocyte ratio in non-affective psychotic adolescent inpatients: Evidence for early association between inflammation and psychosis. Psychiatry Res. 2018, 262, 149–153. [Google Scholar] [CrossRef] [PubMed]
- Jacomb, I.; Stanton, C.; Vasudevan, R.; Powell, H.; O’Donnell, M.; Lenroot, R.; Bruggemann, J.; Balzan, R.; Galletly, C.; Liu, D. C-reactive protein: Higher during acute psychotic episodes and related to cortical thickness in schizophrenia and healthy controls. Front. Immunol. 2018, 9, 2230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gao, S.-Q.; Huang, L.-D.; Dai, R.-J.; Chen, D.-D.; Hu, W.-J.; Shan, Y.-F. Neutrophil-lymphocyte ratio: A controversial marker in predicting crohn’s disease severity. Int. J. Clin. Exp. Pathol. 2015, 8, 14779–14785. [Google Scholar]
- Kasama, T.; Miwa, Y.; Isozaki, T.; Odai, T.; Adachi, M.; Kunkel, S.L. Neutrophil-derived cytokines: Potential therapeutic targets in inflammation. Curr. Drug Targ. Inflamm. Allergy 2005, 4, 273–279. [Google Scholar] [CrossRef]
- Gibson, P.H.; Croal, B.L.; Cuthbertson, B.H.; Small, G.R.; Ifezulike, A.I.; Gibson, G.; Jeffrey, R.R.; Buchan, K.G.; El-Shafei, H.; Hillis, G.S. Preoperative neutrophil-lymphocyte ratio and outcome from coronary artery bypass grafting. Am. Heart J. 2007, 154, 995–1002. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Socio-Demographic Characteristics (N = 294) | |
| Gender (female), N (%) | 157 (53.4) |
| Age (years), mean ± SD | 51.57 ± 13.64 |
| Education level, mean ± SD | 11.85 ± 2.05 |
| Marital status, N (%) | |
| Single | 145 (49.4) |
| Married | 75 (25.5) |
| Divorced | 51 (17.3) |
| Widowed | 23 (7.8) |
| Working status, employed N (%) | 95 (32.3) |
| Illness phase, N (%) | |
| (Hypo)manic episode | 143 (48.6) |
| Major depressive episode | 151 (51.4) |
| Pharmacological Treatment (N = 236) | |
| Antidepressants, N (%) | 98 (41.5) |
| Mood stabilizers, N (%) | |
| Valproate | 103 (43.6) |
| Lithium | 91 (38.6) |
| Others | 61 (25.8) |
| Antipsychotics, N (%) | 202 (85.6) |
| Typical | 45 (19.1) |
| Atypical | 182 (77.1) |
| Long-acting injection | 9 (3.8) |
| Benzodiazepines, N (%) | 175 (74.2) |
| Number of medications, mean ± SD | 3.81 ± 1.22 |
| Mean ± SD | (Hypo)manic Episode (N = 143) | Major Depressive Episode (N = 151) | t | p | Cohen’s d |
|---|---|---|---|---|---|
| Neutrophils | 4.87 ± 1.89 | 4.37 ± 1.56 | 2.462 | 0.014 * | 0.29 |
| Lymphocytes | 2.20 ± 0.78 | 2.37 ± 0.70 | −1.872 | 0.062 | 0.23 |
| Monocytes | 0.58 ± 0.34 | 0.53 ± 0.20 | 1.763 | 0.079 | 0.18 |
| Eosinophils | 0.21 ± 0.14 | 0.21 ± 0.13 | −0.052 | 0.959 | 0 |
| Basophils | 0.34 ± 0.02 | 0.40 ± 0.03 | −1.753 | 0.081 | 2.35 |
| Platelets | 261.25 ± 68.80 | 234.73 ± 58.97 | 3.554 | <0.001 * | 0.41 |
| Neutrophil-to-lymphocyte ratio (NLR) | 2.46 ± 1.33 | 1.89 ± 1.01 | 3.850 | <0.001 * | 0.48 |
| Platelet-to-lymphocyte ratio (PLR) | 130.13 ± 52.84 | 106.05 ± 36.79 | 4.554 | <0.001 * | 0.53 |
| Monocyte-to-lymphocyte ratio (MLR) | 0.28 ± 0.18 | 0.23 ± 0.12 | 2.664 | 0.008 * | 0.33 |
| Red blood cell | 4.68 ± 0.60 | 4.58 ± 0.54 | 1.506 | 0.133 | 0.17 |
| Hemoglobin | 135.93 ± 17.47 | 134.60 ± 15.71 | 0.686 | 0.493 | 0.08 |
| Hematocrit | 41.10 ± 4.54 | 40.72 ± 4.34 | 0.727 | 0.468 | 0.08 |
| Mean corpuscular volume | 88.34 ± 7.00 | 89.37 ± 7.62 | −1.208 | 0.228 | 0.14 |
| Mean corpuscular hemoglobin | 29.17 ± 2.72 | 29.53 ± 2.86 | −1.096 | 0.274 | 0.13 |
| Mean corpuscular hemoglobin concentration | 329.99 ± 12.14 | 330.17 ± 10.49 | −0.136 | 0.892 | 0.02 |
| Red blood cell distribution width_coefficient of variation | 13.84 ± 1.32 | 14.02 ± 1.60 | −1.052 | 0.294 | 0.12 |
| Variables | T | E.S. | Wald | p | Exp(B) (95% CI) |
|---|---|---|---|---|---|
| Platelet-to-lymphocyte ratio | 0.019 | 0.01 | 4.292 | 0.028 | 1.12 (1.05–1.24) |
| Neutrophil-to-lymphocyte ratio | −0.52 | 0.43 | 1.450 | 0.229 | 0.59 (0.26–1.38) |
| Monocyte-to-lymphocyte ratio | 1.63 | 1.01 | 2.581 | 0.108 | 5.1 (0.699–37.33) |
| Platelets | −0.001 | 0.005 | 0.101 | 0.750 | 1.00 (0.99–1.01) |
| Neutrophils | 0.33 | 0.23 | 1.938 | 0.164 | 1.39 (0.87–2.20) |
| Constant | −2.65 | 0.60 | 19.721 | <0.001 | 0.071 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fusar-Poli, L.; Natale, A.; Amerio, A.; Cimpoesu, P.; Grimaldi Filioli, P.; Aguglia, E.; Amore, M.; Serafini, G.; Aguglia, A. Neutrophil-to-Lymphocyte, Platelet-to-Lymphocyte and Monocyte-to-Lymphocyte Ratio in Bipolar Disorder. Brain Sci. 2021, 11, 58. https://doi.org/10.3390/brainsci11010058
Fusar-Poli L, Natale A, Amerio A, Cimpoesu P, Grimaldi Filioli P, Aguglia E, Amore M, Serafini G, Aguglia A. Neutrophil-to-Lymphocyte, Platelet-to-Lymphocyte and Monocyte-to-Lymphocyte Ratio in Bipolar Disorder. Brain Sciences. 2021; 11(1):58. https://doi.org/10.3390/brainsci11010058
Chicago/Turabian StyleFusar-Poli, Laura, Antimo Natale, Andrea Amerio, Patriciu Cimpoesu, Pietro Grimaldi Filioli, Eugenio Aguglia, Mario Amore, Gianluca Serafini, and Andrea Aguglia. 2021. "Neutrophil-to-Lymphocyte, Platelet-to-Lymphocyte and Monocyte-to-Lymphocyte Ratio in Bipolar Disorder" Brain Sciences 11, no. 1: 58. https://doi.org/10.3390/brainsci11010058