
Abstract
Neurologic manifestations of COVID-19 include anosmia, ageusia, encephalopathy, agitation, confusion, ischemic strokes, Guillain–Barré syndrome, seizures, and hemorrhagic encephalitis. Although mechanisms of central nervous system (CNS) injury are likely diverse, direct viral invasion of the CNS has been demonstrated in case reports. Neurotropism of human coronaviruses (HCoVs) is therefore of great interest in the context of the COVID-19 pandemic. Here we present an autopsy-proven case of fatal human coronavirus (HCoV)-OC43 encephalitis in an infant with aplastic thymus and chronic T-cell lymphopenia. Clinicians should remain alert to the possibility of direct CNS invasion by human coronaviruses, including the novel pandemic SARS-CoV-2.
Similar content being viewed by others


Introduction
The COVID-19 pandemic, caused by SARS-CoV-2, has claimed over 500,000 lives and resulted in numerous cases of lasting neurologic injury in survivors. Though the principal clinical signs and symptoms are respiratory, neurologic findings in COVID-19 patients include anosmia, ageusia, encephalopathy, agitation, confusion, and ischemic strokes. (Natoli et al. 2020) Mechanisms underlying these features may be non-specific and multifactorial (e.g., hypoxia related to respiratory failure, critical illness encephalopathy, circulating cytokines, coagulopathy, inflammatory involvement of brain blood vessels, or the effect or withdrawal of medications). (Natoli et al. 2020) The potential for immune-mediated pathogenicity targeting brain tissue is illustrated by cases of Guillain–Barré syndrome. (Natoli et al. 2020) Direct central nervous system (CNS) invasion was suggested a case of necro-hemorrhagic encephalitis. (Poyiadji et al. 2020) SARS-CoV-2 nucleic acid has been detected in the cerebrospinal fluid (CSF) of COVID-19 patients with seizures and encephalitis. (Moriguchi et al. 2020; Zhou et al. 2020) Given the novelty and explosive spread of COVID-19, anticipating its neurologic complications is critical.
Neurotropism of other human coronaviruses (HCoVs), including SARS-CoV-1, middle eastern respiratory syndrome (MERS)-CoV, and seasonal HCoVs, has been described but is likely under-recognized. (Desforges et al. 2019) Here we present a case of fatal HCoV-OC43 encephalitis in an immunocompromised infant, illustrating the neuroinvasive potential of coronaviruses, with possible analogy to SARS-CoV-2.
Case
A 10 month old boy with multiple co-morbidities (Di-George syndrome phenotype–negative for 22q11 deletion, micrognatia, pharyngeal web, hypocalcemia, hypothyroidism, Dandy-Walker malformation, and left facial paralysis) was admitted to the pediatric intensive care unit (PICU) with respiratory failure, requiring intubation, and ventilatory support. His past medical and surgical history were significant for patent ductus arteriosus repair, bilateral hernia repair, appendectomy, submandibular gland duct ligation, and Nissen fundoplication. He had chronic T cell lymphopenia (absolute lymphocyte count 3.5 × 109/L on admission, with prior enumeration of lymphocyte subtypes showing 1% T cells, 30% NK cells, and 65% B cells). He had multiple prior admissions for respiratory illnesses.
He was initially treated empirically with piperacillin-tazobactam and tobramycin, with subsequent adjustment of the antibiotic regimen, first to linezolid, then to trimethoprim/sulfamethoxazole, based on culture results from endotracheal tube aspirate, which grew methicillin-resistant Staphylococcus aureus and Stenotrophomonas maltophila. A nasopharyngeal swab was positive for HCoV-OC43 RNA by multiplex RT-PCR.
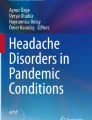
On day 5 of admission, he developed seizures, fluctuating level of consciousness, and bulging fontanelle. Anticonvulsant therapy was initiated with phenobarbital. Magnetic resonance imaging (MRI) of the brain showed patchy T2 hyperintensity and focal cystic change within the thalami, suggesting encephalitis, lacunar infarcts, or an incidental finding in Di-George syndrome (Schmitt et al. 2014) (Fig. 1). A lumbar puncture was performed, showing 37 leukocytes (40% monocytes, 40% neutrophils, and 20% lymphocytes), protein 0.79 g/L, and glucose 3.0 mmol/L. Microbiologic analysis of the CSF was negative for Gram stain, bacterial growth, fungal stain and culture, cryptococcal antigen, negative by PCR for enterovirus, parechovirus, herpes simplex viruses (HSV)-1 and 2, varicella zoster virus (VZV), cytomegalovirus, and JC virus. The CSF PCR was negative for HCoV-OC43. Rare, questionable acid-fast bacilli (AFB)-like organisms were seen; however, these were felt to be contaminants because a mycobacterial culture was negative after 12 weeks of incubation.
By day 36 of admission, the patient continued to have seizures, abnormal movements, severe brainstem dysfunction, and was comatose. Life-sustaining therapy was withdrawn with agreement from the family.
On autopsy, multisystem disease was identified: bilateral focal bronchopneumonia, mediastinal lymph node enlargement, myocardial edema, and focal myocarditis. Consistent with his clinical phenotype, the following extra-CNS congenital abnormalities were noted: aplastic thymus and absence of the thyroid gland. Numerous structural congenital abnormalities were noted on post-mortem examination of the central nervous system: reduction in fresh brain weight, bilateral reduction in deep cerebral white matter, reduced thickness of corpus callosum, bilateral olfactory aplasia with absence of olfactory bulbs and tracts, hydrocephalus of lateral and third ventricles with abnormal T-shaped configuration, retrocerebellar cyst communicating with enlarged fourth ventricle, superior displacement of cerebellar vermis, and bilateral compressive distortion of cerebellar hemispheres. In addition, acute pathologic findings included meningoencephalitis (involving cerebrum, cerebellum, brainstem, and spinomedullary junction); hypoxic-ischemic encephalopathy with subacute microinfarctions in white matter adjacent to right putamen, right posterior thalamus, and left amygdala; and moderate to marked edema. Further microscopic description included marked loss of neurons in the cortex, diencephalon, and basal ganglia. In the hippocampus, there was near complete loss of pyramidal CA1 neurons, approximately 50% loss in the subiculum, parahippocampal gyrus, and adjacent entorhinal cortex, and approximately 25% loss in the dentate gyrus. With respect to pathologic findings related to the meningoencephalitis, perivascular mononuclear infiltrates and microglial activation were seen throughout the CNS (cortex, basal ganglia, diencephalon, midbrain, pons, medulla, spinomedullary junction, and cerebellum). In the pons and midbrain and medulla, mononuclear infiltrates were associated with diffuse infiltration of surrounding tissue (meningitis), diffuse microglial activation with microglial nodules, and marked astrogliosis. In the cerebellum, myelin ovoids were seen in white matter, representing axonal damage. On electron microscopy, viral core-like structures within Purkinje cells of the cerebellar vermis were present. Microbiology studies of the tip of the right temporal lobe were positive for HCoV-OC43 RNA (Luminex® Molecular Diagnostics Respiratory Virus Panel (RVP) nucleic acid amplification assay with suspension microarray detection). Brain tissue was negative for bacterial culture, acid fast bacilli and mycobacterial culture, negative by PCR for HSV-1 and -2, VZV, enterovirus, parechovirus, influenza, and negative for other respiratory viruses on the Luminex® RVP (respiratory syncytial virus, HCoV-229E, HCoV-NL63, and HCoV-HKU1, parainfluenza virus, human metapneumovirus, and adenovirus).
Discussion
HCoV-OC43 is usually associated with upper respiratory tract infection but may infect brain tissue. In vitro, HCoV-OC43 replicates efficiently in primary neuronal cell cultures. (Arbour et al. 1999; Jacomy et al. 2006) In murine models, HCoV-OC43 invades the CNS when inoculated intranasally, (St-Jean et al. 2004) causes acute encephalitis with neuronal necrosis and apoptosis, (Jacomy et al. 2006) and leads to persistent neurologic disabilities. (Jacomy et al. 2006; Butler et al. 2006; Jacomy and Talbot 2003) Three previous cases of HCoV-OC43 neuroinvasive disease in humans have been reported, to our knowledge: (1) HCoV-OC43 was detected in the CSF and nasopharyngeal secretions in a child with demyelinating CNS disease; (Yeh et al. 2004) (2) co-infection with HCoV-OC43 and HCoV-229E was documented in a 3-year-old girl with lower respiratory tract infection and acute flaccid paralysis; (Turgay et al. 2015) and (3) HCoV-OC43 was detected from a brain biopsy sample of an 11-month-old boy with severe combined immunodeficiency and viral encephalitis. (Morfopoulou et al. 2016) Like our case, this boy was of similar age, had an immunocompromising condition, and had negative results on conventional PCR testing of the CSF. (Morfopoulou et al. 2016).
Other animal and human coronaviruses target the CNS. (Desforges et al. 2019) Transgenic mice expressing the human angiotensin-converting enzyme 2 (hACE2) receptor recapitulate the pulmonary pathology seen in humans with COVID-19 and are susceptible to CNS invasion and neuronal injury by the closely related SARS-CoV-1. (Natoli et al. 2020) Neurologic manifestations are frequently observed in COVID-19 patients, (Natoli et al. 2020) and SARS-CoV-2 has been detected in the CSF of at least two patients with COVID-19 and neurologic disease. (Moriguchi et al. 2020; Zhou et al. 2020) Taken together, these observations suggest that neuroinvasive properties are common to multiple coronavirus species. Given these similarities, insights from our case report may have relevance for the current COVID-19 pandemic. (Natoli et al. 2020)
On the other hand, molecular characteristics of SARS-CoV-2 and HCoV-OC43 may imply differences in their neuroinvasive potential. The coronavirus spike glycoprotein is a key determinant of cell entry and tissue tropism. (Hulswit et al. 2016) Although their genetic sequences can be readily aligned, HCoV-OC43 and SARS-CoV-2 have little similarity in the spike protein. Whereas HCoV-OC43 binds to 9-O-acetylated sialic acids, (Hulswit et al. 2019) SARS-CoV-2 uses hACE2 as its cellular receptor. (Li et al. 2003) Receptor distribution has important implications for neurotropism: hACE2 is abundant on epithelial cells of the lung and small intestine, as well as vascular endothelial cells in multiple organs, including the CNS. (Hamming et al. 2004) The spike glycoprotein is a critical determinant of neurovirulence. Compared with wild-type HCoV-OC43, a virus with two point mutations in the spike glycoprotein (H183R and Y241H) was more neuroinvasive in mice and caused more cell death in murine and human neuronal cells. (Meessen-Pinard et al. 2017) A transgenic mouse expressing hACE2 was susceptible to neuroinvasion by SARS-CoV. (Netland et al. 2008) A recent study identified key genomic features that differentiate SARS-CoV-2 from less pathogenic coronaviruses, including HCoV-OC43. (Gussow et al. 2020) SARS-CoV-2 exhibits distinct inserts in the spike glycoprotein and signals in the nucleocapsid protein that enhance the nuclear localization of the virus. (Gussow et al. 2020) Taken together, these studies suggest that molecular differences in the spike glycoprotein and other viral proteins may impact the neuroinvasive potential of SARS-CoV-2, relative to HCoV-OC43.
Host factors may affect susceptibility to coronavirus neurologic disease, including adaptive immune responses. Our patient had an aplastic thymus, with chronic T cell lymphopenia. Similarly, lower lymphocyte count is a risk factor for severe disease and mortality in COVID-19, (Henry 2020) and lower CD4 + T-lymphocyte count increased the risk of hospitalization among patients living with HIV. (Childs et al. 2020).
In summary, our case report demonstrates the neuroinvasive potential of HCoV-OC43, which should alert clinicians to the possibility of direct CNS invasion by human coronaviruses, including the novel pandemic SARS-CoV-2.

Magnetic resonance imaging of brain abnormalities in an immunocompromised infant with human coronavirus OC43 encephalitis. T1-weighted (a and c) and T2-weighted (b and d) transverse images of adjacent brain sections show two focal cystic lesions present medially in the left thalamus, measuring 4 and 6 mm in diameter (white arrows). Findings may reflect encephalitis, areas of lacunar infarction, or alternatively, can be an incidental finding in a patient with Di-George syndrome (Schmitt et al. 2014)
References
Natoli S, Oliveira V, Calabresi P, Maia LF, Pisani A (2020) Does SARS-Cov-2 invade the brain? Translational lessons from animal models. Eur J Neurol.
Poyiadji N, Shahin G, Noujaim D, Stone M, Patel S, Griffith B (2020) COVID-19-associated acute hemorrhagic necrotizing encephalopathy: CT and MRI features. Radiology. 201187.
Moriguchi T, Harii N, Goto J et al (2020) A first case of meningitis/encephalitis associated with SARS-Coronavirus-2. Int J Infect Dis 94:55–58
Zhou L, Zhang M, Wang J, Gao J (2020) Sars-Cov-2: Underestimated damage to nervous system. Travel Med Infect Dis. 101642.
Desforges M, Le Coupanec A, Dubeau P, et al (2019) Human coronaviruses and other respiratory viruses: Underestimated opportunistic pathogens of the central nervous system? Viruses. 12(1).
Schmitt JE, Yi JJ, Roalf DR (2014) Incidental radiologic findings in the 22q11.2 deletion syndrome. AJNR Am J Neuroradiol 35(11):2186–2191
Arbour N, Cote G, Lachance C, Tardieu M, Cashman NR, Talbot PJ (1999) Acute and persistent infection of human neural cell lines by human coronavirus OC43. J Virol 73(4):3338–3350
Jacomy H, Fragoso G, Almazan G, Mushynski WE, Talbot PJ (2006) Human coronavirus OC43 infection induces chronic encephalitis leading to disabilities in BALB/C mice. Virology 349(2):335–346
St-Jean JR, Jacomy H, Desforges M, Vabret A, Freymuth F, Talbot PJ (2004) Human respiratory coronavirus OC43: Genetic stability and neuroinvasion. J Virol 78(16):8824–8834
Butler N, Pewe L, Trandem K, Perlman S (2006) Murine encephalitis caused by HCoV-OC43, a human coronavirus with broad species specificity, is partly immune-mediated. Virology 347(2):410–421
Jacomy H, Talbot PJ (2003) Vacuolating encephalitis in mice infected by human coronavirus OC43. Virology 315(1):20–33
Yeh EA, Collins A, Cohen ME, Duffner PK, Faden H (2004) Detection of coronavirus in the central nervous system of a child with acute disseminated encephalomyelitis. Pediatrics 113(1 Pt 1):e73-76
Turgay C, Emine T, Ozlem K, Muhammet SP, Haydar AT (2015) A rare cause of acute flaccid paralysis: Human coronaviruses. J Pediatr Neurosci 10(3):280–281
Morfopoulou S, Brown JR, Davies EG et al (2016) Human coronavirus OC43 associated with fatal encephalitis. N Engl J Med 375(5):497–498
Hulswit RJ, de Haan CA, Bosch BJ (2016) Coronavirus spike protein and tropism changes. Adv Virus Res 96:29–57
Hulswit RJG, Lang Y, Bakkers MJG et al (2019) Human coronaviruses OC43 and HKU1 bind to 9-O-acetylated sialic acids via a conserved receptor-binding site in spike protein domain A. Proc Natl Acad Sci U S A 116(7):2681–2690
Li W, Moore MJ, Vasilieva N et al (2003) Angiotensin-converting enzyme 2 is a functional receptor for the SARS coronavirus. Nature 426(6965):450–454
Hamming I, Timens W, Bulthuis ML, Lely AT, Navis G, van Goor H (2004) Tissue distribution of ACE2 protein, the functional receptor for SARS coronavirus. A first step in understanding SARS pathogenesis. J Pathol. 203(2):631–637
Meessen-Pinard M, Le Coupanec A, Desforges M, Talbot PJ (2017) Pivotal role of receptor-interacting protein kinase 1 and mixed lineage kinase domain-like in neuronal cell death induced by the human neuroinvasive coronavirus OC43. J Virol. 91(1).
Netland J, Meyerholz DK, Moore S, Cassell M, Perlman S (2008) Severe acute respiratory syndrome coronavirus infection causes neuronal death in the absence of encephalitis in mice transgenic for human ACE2. J Virol 82(15):7264–7275
Gussow AB, Auslander N, Faure G, Wolf YI, Zhang F, Koonin EV (2020) Genomic determinants of pathogenicity in SARS-CoV-2 and other human coronaviruses. Proc Natl Acad Sci U S A 117(26):15193–15199
Henry BM (2020) COVID-19, ECMO, and lymphopenia: A word of caution. Lancet Respir Med 8(4):e24
Childs K, Post FA, Norcross C, et al (2020) Hospitalized patients with COVID-19 and HIV: A case series. Clin Infect Dis.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Kasereka, M.C., Hawkes, M.T. Neuroinvasive potential of human coronavirus OC43: case report of fatal encephalitis in an immunocompromised host. J. Neurovirol. 27, 340–344 (2021). https://doi.org/10.1007/s13365-020-00926-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13365-020-00926-0