
Abstract
There are few epidemiological studies on the relationships between trace element exposure and depression in the elderly Chinese population. We studied the levels of strontium (Sr), manganese (Mn), vanadium (V), barium (Ba), aluminum (Al), titanium (Ti), arsenic (As) and selenium (Se) in whole blood, and the relationships between trace element exposure and depressive symptoms in elderly Chinese individuals in a community. Data was obtained from the baseline investigation of the Health of Elderly and Environment Risk Factor Cohort, established in Lu'an municipality, Anhui Province, China, from June to September 2016. The levels of eight trace elements were determined by inductively coupled plasma mass spectrometry (ICP-MS), reflecting individuals’ exposure levels. The geriatric depression scale (GDS-30) was applied to screen depression in the elderly cohort. Binary logistic regression was used to analyze the associations between trace elements and depressive symptoms. All analyses were stratified by sex. Results show that among of 954 elderly participants, 27.13%, had depressive symptoms according to the GDS-30. The detection rate of Al was 91.70%, the detection rate of Ti was 89.55%, and the detection rate of other six mineral elements was 94.12–94.31%. High concentrations of Sr and Ba were found to be risk factors for depressive symptoms. Sr and Ba tertiles were related to an increased risk of depressive symptoms, with odds ratios (ORs) of 1.84 and 2.15 for the highest tertiles, respectively. When stratified by sex, increased whole blood levels of Sr and Ba were associated with depressive symptoms in women, but not in men.
Similar content being viewed by others

Introduction
Depression is a common disease worldwide, and World Health Organization (WHO) data indicate that more than 300 million people worldwide are affected (WHO 2017). Among population 65 and older, the prevalence of major depression in lifetime was 1.0–38.6% (Guerra et al. 2016b). Depression in the elderly individuals is a serious public health problem, as it is associated with severe disability, a high disease burden, high medical costs and decreased life expectancy (WHO 2014). Intervention studies in elderly volunteers in Mexico reported a reduction in the cost of disability (Salomon et al. 2012). The 2013 China National Health and Pensions Tracking Survey showed that the prevalence of depressive symptoms in elderly people increased from 3.86% in 1999 to 26.8% in 2013 (Chen et al. 1999; Yang et al. 2017). Elderly individuals with depression comorbid with chronic diseases have a substantial effect on the public health system (Moussavi et al. 2007). Although there are treatment options for depression, a considerable proportion of people cannot achieve remission (Mauskopf et al. 2009). Hence, it is necessary to discuss the risk factors and preventive measures. An increasing number of researchers are now studying biological factors that affect depression, and increasing attention has been given to the role of trace elements.
Environmental pollution has become an increasingly serious problem in China. Metals and some trace elements are the main environmental pollutants (Wu et al. 2018). Trace elements are ubiquitous in environmental media (Abuduwailil et al. 2015; Bian et al. 2015; Li et al. 2014). The main routes of human exposure to trace elements are ingestion of contaminated food, absorption through the skin and exposure during medical interventions. There have been a large number of studies demonstrating widespread exposure to trace elements in the population (Diyabalanage et al. 2017; Liu et al. 2020). High metal levels were found in plastic and paper/wood products (Cui et al. 2015; Aboel Dahab et al. 2016). Elderly individuals exposed to more to trace elements, as they have higher rates of exposure to equipment and medicines containing trace elements in the hospital than younger people, this may also lead to an increase in the accumulation of certain trace elements. Even though the concentrations of trace elements in the environment are very low, long-term exposure can cause accumulation in the body and substantial harm to the health (Feng et al. 2015). Trace elements are needed for healthy growth and development of physiological processes in the human body. Some trace elements play crucial role of physiologically active cells, and an imbalance can cause various diseases (Falah et al. 2017; Noor et al. 2011). Most of these necessary trace elements are known to alter the risk of depression in humans, but the results of population-based epidemiologic studies are limited or controversial.
It is reported that the levels of Sr in the cerebral cortexes of patients with severe depression and patients with two-way affective disorder were very low, and the concentrations of Sr, Mn, Al and Se in the cortex of suicide patients were altered (Dean 2019). Researchers have found that Al is related to the etiologies of mental illnesses, such as Alzheimer's disease and schizophrenia (Al-Fartusie et al. 2019). A study of American Indian seniors reported that urine As levels were not related to neuropsychological function (Carroll et al. 2017), which is inconsistent with the results of other studies. A Chinese case–control study showed that the contents of mercury (Hg), cadmium (Cd), lead (Pb) and chromium (Cr) in the blood of patients in the non-depression group were significantly higher than those in the non-depressive group (Guan 2016). In China, most studies have been small sample controlled studies or have assessed the relationship between common trace elements and depression in adolescents and adults. However, research on the relationship between trace elements and senile depression has been limited in China.
On the basis of data from the Health of Elderly and Environment Risk Factor Cohort in Lu'an, Anhui, the present study included 954 elderly Chinese individuals. Our primary goal was to quantify the levels of exposure to trace elements in the elderly population. Our secondary goal was to assess associations between exposures to trace elements and depressive symptoms in the elderly population.
Experimental
Participants
Data was obtained from the baseline survey of the Cohort Study on Controllable Factors of Elderly Health and Environment, which was conducted from June to September 2016 in Lu'an city, Anhui Province. The cohort was jointly established by the School of Public Health of Anhui Medical University and the local Center for Disease Control and Prevention (CDC). Using the method of stratified cluster sampling, the first step was to randomly select two counties in Lu'an city. Subsequently, a community was randomly selected from each county. Finally, in each community, senior citizens aged 60 years and above were selected to participate in the survey. The inclusion criteria were as follows: (1) aged 60 years or older; (2) living in the local area for more than 6 months; and (3) able to actively cooperate, understand and complete the questionnaire. Participants were recruited by the CDC and community hospitals. Telephone appointments with the participants were made one day prior. Those who met the requirements were required to participate in a face-to-face survey and undergo a relevant medical examination at the local hospital, which took approximately for about 2–3 h.
As shown in supplemental figure S1, 1080 elderly people agreed to and finished the questionnaire survey in communities in Lu'an city, Anhui Province, China. In total, 72 participants were missing whole blood samples, 54 participants did not provide complete basic information, and a total of 954 participants were included. This study was approved by the Medical Ethics Committee of Anhui Medical University. All participants or their legal representatives signed written consent forms to participate in the surveys.
Questionnaire survey
A total of 954 participants completed the interview and provided a sufficient sample of whole blood. The survey was conducted using a internally developed questionnaire to assess health and exposure to environmental factors in the elderly cohort. The following data were collected: a. demographic characteristics: age, sex, education level, marital status, etc.; b. lifestyle: characteristics: smoking status, drinking, eating habits, etc.; and chronic medical history: at least one disease diagnosed by the county level and above medical institutions, including hypertension, diabetes, cancer and stroke, etc.
Depression assessment
The Geriatric Depression Scale (GDS-30) was used to screen for depression in the elderly. The GDS-30 was compiled by Brank et al. in 1982. This study used the Chinese version of the GDS-30 (Jakobsson et al. 2010) to measure relevant feelings of the subjects over the past week. The scale has a total of 30 items, with each item receiving a score of 0 or 1. A score of 0 to 10 was considered normal, and 11 to 30 was considered depression.
Sample collection and detection of trace elements
Subjects fasted the night before the test, and healthcare workers in the hospital used anticoagulation vacuum blood collection tubes to collect early morning fasting venous blood. After blood collection, 2 mL of blood was placed into a prepared EP tube, and the EP tube was marked with a number and placed in a freezer at − 80 °C for storage. Sr, Mn, vanadium (V), barium (Ba), Al, titanium (Ti), arsenic (As) and Se concentration in whole blood by inductively coupled plasma mass spectrometry (ICP-MS) (PerkinElmer NexION 350X, Shelton, CT, USA).
Two days before the experiment, all laboratorial materials were thoroughly cleaned with 2% HNO3. The frozen blood samples were removed from the − 80 °C freezer and placed in a refrigerator at − 20 °C. The blood samples were thawed slowly in a 4 ℃ refrigerator the night before. One milliliter of whole blood was placed 50 ml metal-free PP tube; then, 24 mL of 0.05% Triton X-100 and 2% tetramethylammonium hydroxide (TMAH) mixed reagent were added to dilute the sample. The sample was subjected to ultrasound-assisted digestion for at least 1 h and then ICP-MS analysis 3 times. Whole blood trace element L-3 (Norway SERO) was used to evaluate the stability of the instrument. Kinetic energy discrimination (KED) mode was selected for the experimental detection of all the elements. The following was the ICP-MS NexION 350X daily working conditions (Gu et al. 2020): Ar nebulizer gas flow, 0.90 L/min (optimized daily); auxiliary gas, 1.2; plasma gas, 15; RF power, 1100; measurement units, Cps (counts per second); detector mode, dual; curve type simple, linear; auto lens, on; detector mode, KED; Blank subtraction, blank subtraction; sample units, μg/L; sweeps/reading, 20; readings/replicate, 1; replicates, 3; and dwell time, 50 ms. The limits of detection (LODs) for Sr, Mn, V, Ba, Al, Ti, As and Se were 0.0275 μg/L, 0.9652 μg/L, 0.1803 μg/L, 0.4025 μg/L, 0.7867 μg/L, 0.0475 μg/L, 0.0125 μg/L and 0.3175 μg/L, respectively. The background value of the blank was deducted from the final experimental results. Sample values below the (LOD) were assigned a value equal to the LOD/\(\sqrt {2}\).
Statistical analysis
The general demographic characteristics were considered variables, and Chi-square tests were used to compare the differences in demographic characteristics between the depressed elderly population and the normal elderly population. According to the Kolmogorov–Smirnov normality test, the concentration of mineral elements in whole blood is non-normally distributed, so it is described by the median of the interquartile range and compared by the Mann–Whitney U tests. The mineral element concentration was divided into tertiles, with the lowest tertile as a reference. Binary logistic regression was used to analyze the relationship between mineral element concentration and depression risk. Due to a high correlation among eight trace elements, each trace element was individually included in the regression model. First, we used a binary logistic regression model to examine the relationship between the tertiles of mineral element concentrations and the two endpoints in the total sample. Furthermore, after adjustment for multiple variables, such as age, gender, education level, income, marital status, living situation, drinking status, clitocybin, sleep, body mass index (BMI) and self-assessed of health status, binary logistic regression models were used to evaluate the relationships between trace element levels and the risk of depressive symptoms. Moreover, analyses of the associations of trace elements with depressive symptoms stratified by sex were carried out using binary logistic regression models with adjustments for potential confounders.
Double data entry was performed using EpiData 3.0 software, and logic checks and consistency checks were performed. All statistical analyses were carried out in the Statistical Package for the Social Sciences (SPSS), version 23.0. All reported p-values were bilateral, with a p-value < 0.05 as the difference was considered statistically significant.
Result and discussion
We assessed the levels of trace elements in the elderly Chinese population and to clarify the relationships between exposure levels of trace elements and the risk of depression. We measured the concentrations of eight trace elements in whole blood samples from 954 participants and found that higher whole blood Sr and Ba levels were associated with an increased risk of depression in elderly individuals. The main findings are as follows. First, the detection rates of the eight trace elements were high and the exposure levels in participants with depressive symptoms higher than those non-depressed participants in Lu'an city, Anhui Province, China (Table 1, Table S1). Second, the higher the concentrations of Ba and Sr were, the greater the risk of depression in the elderly population was (Table 2). In addition, there was a high prevalence of depression, in females, and the association between exposure to trace elements and depression was stronger in females than in males (Fig. 1).

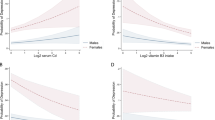
Logistic regression analysis of tertile trace elements and depressive symptoms. The odds ratios (ORs) and 95% confidence intervals (CIs) were presented for each higher tertile (Q3) compared with the lowest quartile (Q1) among male (438) and female (516) elderly with depression. Models were adjusted for age, gender, educational level, income, marital status, living situation, drinking status, clitocybine, sleep at night, BMI, self-assessment of health status. P trend is the Pvalue for trend across the lowest tertile (Q1) to the highest tertile (Q3)
Basic demographic characteristics and depression status
The characteristics stratified by depression status are shown in Table 3. Of the 954 participants, the prevalence of depression (GDS-30 ≥ 10) was 27.30%. Among the depressed participants, 45.91% were elderly males, and 54.09% were elderly females. There were significant differences between depressed elderly and non-depressed elderly individuals in sex, educational level, living situation, income, marital status, drinking status, diet, sleep, BMI and self-assessed of health status. Compared with the group of elderly individuals without depressive symptoms, those with depressive symptoms were more likely to be non-married, be lonely, have a lower education level, have a lower family income, receive less sleep, be obese, report dissatisfaction with self-assessed health status, be female, be vegetarian and be nondrinkers.
In this study, the prevalence of depression was 27.30%, which was higher than previously reported in China (Zhang et al. 2019; Xu et al. 2019). In people aged 65 and older, the prevalence of major depression in their lifetime was 1.0–38.6% (Guerra, M. et al. 2016a). Depression was ranked as the single largest contributor to non-fatal health loss by the WHO. Therefore, the potential risk factors for depressive symptoms deserve attention.
Distribution of whole blood trace elements
The concentrations of Ba, Ti, Se, Ti, As, Mn, V and Al in the whole blood samples of 954 elderly participants are presented in Table 1. The detection rate of aluminum was 91.70%, the detection rate of titanium was 89.55%, and the detection rates of the other six mineral elements were 94.12–94.31%. The highest median concentration was Se, at 89.33 μg/L, followed by Al, at 61.41 μg/L; the lowest median concentration was Ti, at 0.08 μg/L. The median concentrations of the remaining five trace elements (Ba, Mn, Sr, As and V) were 43.26 μg/L, 26.77 μg/L, 22. 38 μg/L, 1.83 μg/L and 0.61 μg/L, respectively.
Sr is an essential trace element in the human body. The 25th to 75th percentile of Sr was 17.96–28.70 μg/L, which was lower than that in normal people (approximately 38.1 μg/L) (Cheng et al. 2014), but was basically consistent with whole blood levels in general population in China (Ding et al. 2015) (18.24–32.0 μg/L) and general populations in other regions abroad (Meyer et al. 2018) (16.0–27.1 μg/L). Ba is a nonessential trace element in the human body, and different studies have reported inconsistent whole blood Ba levels. The blood Ba level was 0.64 μg/L in Queensland (Tanvir et al. 2020). Our results showed that the Ba concentration in whole blood samples of 954 elderly people in Lu'an city was 32.74–60.83 μg/L, which was higher than that of the general population (< 0.45 μg/L) (Ding et al. 2015). There have been a large number of studies demonstrating widespread exposure to trace elements in the population (Diyabalanage et al. 2017; Liu et al. 2020). High metal levels found in plastic and paper/wood products (Cui et al. 2015; Aboel Dahab et al. 2016). The sources of elderly people are mostly drug capsules and medical supplies.
Trace elements in depressed and normal population status
The results are shown in Table S1. The whole blood concentrations of Sr, Ba and Al in depressed participants were significantly higher than those in non-depressed participants (p < 0.05). The contents of As and Se were significantly lower than those non-depressed participants. There was no significant difference in the concentrations of Mn, V and Ti between depressed and non-depressed symptoms participants.
Correlation analysis of trace elements
Correlations between any two of the eight trace elements were analyzed by Spearman's rank correlation coefficient, and there were significant correlations with each other (p < 0.05). The results are given in Table S2.
The associations between the quartiles of the eight trace elements in whole blood and depression are shown in Table 2. Binary logistic regression analysis revealed that increased concentrations of Sr (Q2: OR: 1.80, 95% CI: 1.23−2.64; Q3: OR: 2.82, 95% CI: 1.95−4.08), Ba (Q2: OR: 1.51, 95% CI: 1.02−2.23; Q3: OR: 3.43, 95% CI: 2.37−4.95) and Al (Q3: OR: 1.63, 95% CI: 1.56−2.31) in whole blood were related to a high risk of depression (p < 0.01). The p values for the trends (p trend) were < 0.001, < 0.001 and 0.005 for Sr, Ba and Al, respectively. After adjustment for multiple variables, such as age, sex, educational level, income, marital status, living situation, alcohol consumption status, diet, sleep, BMI and self-assessed health status, significant relationships between whole blood Sr and Ba were still observed; however, this was not the case for Al. Increased concentrations of Se (Q2: OR: 0.61, 95% CI: 0.43−0.85; Q3: OR: 0.38, 95% CI: 0.26−0.54), As (Q3: OR: 0.63, 95% CI: 0.44−0.90), Ti (Q2: OR: 0.42, 95% CI: 0.29−0.61) were also related to reduce risk of depression (p < 0.05). The p-trend for Se and As was < 0.001 and 0.010, respectively. After adjustment for multiple potential factors, their correlations disappeared.
In our study, strong relationships were found between exposure to high levels of Sr and Ba and depression. Shika’s (Thithunguyen et al. 2019) cross-sectional study on low mineral intake and depression in elderly Japanese women showed that intakes of trace elements, such as potassium (K), magnesium (Mg), iron (Fe), zinc (Zn) and copper (Cu), were not associated with the prevalence of depression. To our knowledge, this is the first time that relationships between depression in elderly individuals in China and Sr and Ba have been reported.
The mechanism explaining the impact of trace elements on depressive symptoms is still unclear. The underlying mechanism of increased concentrations of whole blood Sr and Ba leading to an increased risk of depression in the elderly could be that Ba or Sr replaces Ca or Mg domain in the metabolic environment, such as in molecules like calmodulin, which activates the protein kinases (Fowler et al. 2009). Ba or Sr substitution will cause calcium channels to "compete" and enter a fast-burning state, leading to "overdrive" of the cholinergic and monoaminergic neuronal systems (Zamponi and Currie, 2013), affecting the associated pathway. In this way, Ba or Sr poisoning will overload the biological system through a free radical chain reaction mediated by oxidants, accelerating disease.
The passive outflow of K from the cell is competitively prevented by Ba, leading to intracellular K accumulation and extracellular hyperkalemia (Pandit et al. 2010; Spencer and Schaumburg, 2000). During the Ba poisoning process (Yi Chang et al. 2016), sodium and potassium ion pumps and Ca channels are affected, which alters the membrane depolarization, potentially causing the release of glutamic acid. In addition, Ba may also replace the Mg-binding domain of glutamine synthetase, leading to the accumulation of neurotoxic glutamate (Zuo et al. 2018).
Ba and Sr induce endogenous S-proteoglycan depletion, which blocks the binding of 5-HT to the 5-HT receptor, and pathogenic destruction may also lead to the inhibition of intercellular communication with adhesion molecules (Oliveira et al. 2020; Cowell et al. 2020). In addition, blocking the binding of cell surface proteoglycans to superoxide dismutase can due to increased oxidative stress produced by superoxide (Cowell et al. 2020). Many studies have shown that in the pathogenesis of depression, 5-HT intake is disturbed and oxidative stress generated by superoxide is increased (Matchkov et al. 2015; Sakr et al. 2015).
Sex differences in connection of trace elements with depression
There were differences in some trace element levels (Sr, Ba and Se) between males with and without depressive symptoms (p < 0.01). Among female, with the exception of Se, the whole blood trace elements (Sr, Ba and Al) were significantly lower (p < 0.01) in participants with depressive symptoms, than in those without such symptoms (Table S3).
The links between trace elements and depression were examined in males and females (Fig. 1). Figure 1 shows the relationships between trace elements after adjusting for confounding factors and depression. In elderly females, the increased concentrations of Sr (Q3: OR: 1.98, 95% CI: 1.03−3.83) and Ba (Q3: OR: 2.96, 95% CI: 1.52−5.78) were related to depression (p < 0.05), with a strong dose–response relationship (p < 0.05). However, no obvious association was observed in men.
Interestingly, significant sex differences were found in our study. Globally, the prevalence of women aged 55–74 is over 7.5%, and that of men is over 5.5% (WHO 2017). We found that the prevalence of depression among elderly women (30.5%) was higher than that among elderly men (23.1%), in accordance with results of studies in the Europe (Horackova et al. 2019). Mainly in the female population, high levels of trace elements (Sr and Ba) were positively correlated with depression, but these results were not observed in men. Neural structure and nerve function may be factors connected with depression, and sex differences are important factors that affect clinical manifestations and depression control (Parker et al. 2014; Shim et al. 2011). Among these factors, a sex difference in the serotonin system may have an important impact on the pathophysiology of depression (Kraus et al., 2017). The genetic contribution of serotonin transport in depression patients is sex-specific (Chang et al. 2017). The role of the serotonin system may be more pronounced in women than in men (Mattina et al. 2019). In summary, the sex difference in the serotonin system and the associations between trace elements and the serotonin system may explain the sex differences. However, the sex differences in the associations between trace elements and depression and their underlying mechanisms still need further exploration, as current research is limited.
This investigation has several strengths. First, the Elderly Health and Environment Risk Factor Cohort included only elderly people who were 60 years old or older and had sufficient sample material. Second, this study reported for the first time the relationships between Ba and Sr and depression in elderly individuals. Furthermore, we also controlled for many confounding variables, such as sex, age, education level, income, marital status, alcohol consumption status, diet, BMI, sleep and elderly self-health assessment score. Additionally, sex was used as an effect modifier. Our research has several disadvantages. Owing to the cross-sectional nature of our study, we could clarify only the link between exposure to trace elements and depression, but causal evidence cannot be elucidated. Another disadvantage is that our study used the Geriatric Depression Scale (GDS-30) to assess depression, not a clinical diagnosis. Different definitions of depression may limit the comparison of the prevalence of depression in different study populations. Finally, this study did not evaluate the levels of trace elements in the urine and diet of this population.
Conclusion
Elderly people are extensively exposed to environmental trace element pollutants in Lu'an, Anhui Province. The concentration of Ba and Sr exposure in depression participants was higher than that in non-depression participants. This suggests that an underlying source of exposure is medication in elderly Chinese individuals. We notice significant sex-specific discrepancy in the associations between trace elements and depression in elderly Chinese individuals. The relationship appeared to be the strongest in elderly women with high trace element concentrations and depression.
References
Aboel Dahab A, Elhag DE, Ahmed AB, Al-Obaid HA (2016) Determination of elemental toxicity migration limits, bioaccessibility and risk assessment of essential childcare products. Environ Sci Pollut Res Int 23(4):3406–3413. https://doi.org/10.1007/s11356-015-5594-0
Abuduwailil J, Zhaoyong Z, Fengqing J (2015) Evaluation of the pollution and human health risks posed by heavy metals in the atmospheric dust in Ebinur Basin in Northwest China. Environ Sci Pollut Res Int 22(18):14018–14031. https://doi.org/10.1007/s11356-015-4625-1
Al-Fartusie FS, Mohssan SN (2017) Essential Trace Elements and Their Vital Roles in Human Body. Indian J Adv Chem Sci 5(3):127–136. https://doi.org/10.22607/IJACS.2017.503003
Al-Fartusie FS, Al-Bairmani HK, Al-Garawi ZS, Yousif AH (2019) Evaluation of some trace elements and vitamins in major depressive disorder patients: a case-control study. Biol Trace Elem Res 189(2):412–419. https://doi.org/10.1007/s12011-018-1507-7
Ali NM, Muhammad SIKMS, Aldabagh A (2011) Serum Levels of Copper Zinc Iron and Magnesium in Iraqi`s Patient with Chronic Hepatitis C. Karbala Journal of Medicine 2(10):1146–1150
Bian B, Zhou LJ, Li L, Lv L, Fan YM (2015) Risk assessment of heavy metals in air, water, vegetables, grains, and related soils irrigated with biogas slurry in Taihu Basin, China. Environ Sci Pollut Res Int 22(10):7794–7807. https://doi.org/10.1007/s11356-015-4292-2
Carroll CR, Noonan C, Garroutte EM, Navas-Acien A, Verney SP, Buchwald D (2017) Low-level inorganic arsenic exposure and neuropsychological functioning in American Indian elders. Environ Res 156:74–79. https://doi.org/10.1016/j.envres.2017.03.018
Chang Y, Lu CW, Lin TY, Huang SK, Wang SJ (2016) Baicalein a constituent of scutellaria baicalensis reduces glutamate release and protects neuronal cell against kainic acid-induced excitotoxicity in rats. Am J Chin Med 44(05):943–962. https://doi.org/10.1142/S0192415X1650052X
Chang CC, Chang HA, Fang WH, Chang TC, Huang SY (2017) Gender-specific association between serotonin transporter polymorphisms (5-HTTLPR and rs25531) and neuroticism, anxiety and depression in well-defined healthy Han Chinese. J Affect Disord 207:422–428. https://doi.org/10.1016/j.jad.2016.08.055
Chen R, Copeland JR, Wei L (1999) A meta-analysis of epidemiological studies in depression of older people in the People’s Republic of China. Int J Geriatr Psychiatr 14(10):821–830. https://doi.org/10.1002/(sici)1099-1166(199910)14:10%3c821::aid-gps21%3e3.0.co;2-0
Cheng Y, De-Ye L (2014) Study on strontium distribution in human blood and strontium species in human plasma. Chin J Anal Lab 033(001):96–99
Cowell W, Colicino E, Tanner E, Amarasiriwardena C, Andra SS, Bollati V et al (2020) Prenatal toxic metal mixture exposure and newborn telomere length: modification by maternal antioxidant intake. Environ Res 190:110009. https://doi.org/10.1016/j.envres.2020.110009
Cui XY, Li SW, Zhang SJ, Fan YY, Ma LQ (2015) Toxic metals in children’s toys and jewelry: coupling bioaccessibility with risk assessment. Environ Pollut 200:77–84. https://doi.org/10.1016/j.envpol.2015.01.035
De Oliveira M, Gianeti T, da Rocha F, Lisboa-Filho PN, Piacenti-Silva M (2020) A preliminary study of the concentration of metallic elements in the blood of patients with multiple sclerosis as measured by ICP-MS. Sci Rep 10(1):13112. https://doi.org/10.1038/s41598-020-69979-9
Dean B, Lam LQ, Scarr E, Duce JA (2019) Cortical biometals: changed levels in suicide and with mood disorders. J Affect Disord 243:539–544. https://doi.org/10.1016/j.jad.2018.09.026
Ding C, Pan Y, Zhang A, Zhu C, Liu D, Xu G et al (2015) Zhonghua lao dong wei sheng zhi ye bing za zhi = Zhonghua laodong weisheng zhiyebing zazhi =. Chin J Ind Hyg Occup Dis 33(12):894–899. https://doi.org/10.3760/cma.j.issn.1001-9391.2015.12.004
Diyabalanage S, Fonseka S, Dasanayake D, Chandrajith R (2017) Environmental exposures of trace elements assessed using keratinized matrices from patients with chronic kidney diseases of uncertain etiology (CKDu) in Sri Lanka. J Trace Elem Med Biol Organ Soc Miner Trace Elem (GMS) 39:62–70. https://doi.org/10.1016/j.jtemb.2016.08.0031
Feng W, He X, Chen M, Deng S, Qiu G, Li X et al (2015) Urinary metals and heart rate variability: a cross-sectional study of urban adults in Wuhan. China Environ Health Perspect 123(3):217–222. https://doi.org/10.1289/ehp.1307563
Fowler MR, Colotti G, Chiancone E, Higuchi Y, Seidler T, Smith GL (2009) Complex modulation of L-type Ca(2+) current inactivation by sorcin in isolated rabbit cardiomyocytes. Pflugers Arch Euro J Physiol 457(5):1049–1060. https://doi.org/10.1007/s00424-008-0575-5
Gu L, Yu J, Fan Y, Wang S, Yang L, Liu K et al (2020) The association between trace elements exposure and the cognition in the elderly in China. Biol Trace Elem Res. https://doi.org/10.1007/s12011-020-02154-3
Guan HL (2016) Correlation between blood heavy metal levels and depression after cerebral infarction and intervention measures. Cap Food Med 23(04):52–53
Guerra M, Prina AM, Ferri CP, Acosta D, Gallardo S, Huang Y et al (2016a) A comparative cross-cultural study of the prevalence of late life depression in low and middle income countries. J Affect Disord 190:362–368. https://doi.org/10.1016/j.jad.2015.09.004
Guerra M, Prina AM, Ferri CP, Acosta D, Gallardo S, Huang Y et al (2016b) A comparative cross-cultural study of the prevalence of late life depression in low and middle income countries. J Affect Disord 190:362–368. https://doi.org/10.1016/j.jad.2015.09.004
Horackova K, Kopecek M, Machů V, Kagstrom A, Aarsland D, Motlova LB et al (2019) Prevalence of late-life depression and gap in mental health service use across European regions. Euro Psychiatr J Assoc Euro Psychiatr 57:19–25. https://doi.org/10.1016/j.eurpsy.2018.12.002
Jakobsson HE, Jernberg C, Andersson AF, Sjölund-Karlsson M, Jansson JK, Engstrand L (2010) Short-term antibiotic treatment has differing long-term impacts on the human throat and gut microbiome. PLoS ONE 5(3):e9836. https://doi.org/10.1371/journal.pone.0009836
Kraus C, Castrén E, Kasper S, Lanzenberger R (2017) Serotonin and neuroplasticity-Links between molecular, functional and structural pathophysiology in depression. Neurosci Biobehav Rev 77:317–326. https://doi.org/10.1016/j.neubiorev.2017.03.007
Li Y, Wang H, Wang H, Yin F, Yang X, Hu Y (2014) Heavy metal pollution in vegetables grown in the vicinity of a multi-metal mining area in Gejiu, China: total concentrations, speciation analysis, and health risk. Environ Sci Pollut Res Int 21(21):12569–12582. https://doi.org/10.1007/s11356-014-3188-x
Liu Y, Yuan Y, Xiao Y, Li Y, Yu Y, Mo T et al (2020) Associations of plasma metal concentrations with the decline in kidney function: a longitudinal study of Chinese adults. Ecotoxicol Environ Saf 189:110006. https://doi.org/10.1016/j.ecoenv.2019.110006
Matchkov VV, Kravtsova VV, Wiborg O, Aalkjaer C, Bouzinova EV (2015) Chronic selective serotonin reuptake inhibition modulates endothelial dysfunction and oxidative state in rat chronic mild stress model of depression. Am J Physiol Regul Integr Comp Physiol 309(8):R814–R823. https://doi.org/10.1152/ajpregu.00337.2014
Mattina GF, Van Lieshout RJ, Steiner M (2019) Inflammation, depression and cardiovascular disease in women: the role of the immune system across critical reproductive events. Ther Adv Cardiovasc Dis 13:1753944719851950. https://doi.org/10.1177/1753944719851950Guerra
Mauskopf JA, Simon GE, Kalsekar A, Nimsch C, Dunayevich E, Cameron A (2009) Nonresponse, partial response, and failure to achieve remission: humanistic and cost burden in major depressive disorder. Depression Anxiety 26(1):83–97. https://doi.org/10.1002/da.20505
Meyer S, Markova M, Pohl G, Marschall TA, Pivovarova O, Pfeiffer A et al (2018) Development, validation and application of an ICP-MS/MS method to quantify minerals and (ultra-)trace elements in human serum. J Trace Elem Med Biol Organ Soc Miner Trace Elem (GMS) 49:157–163. https://doi.org/10.1016/j.jtemb.2018.05.012
Moussavi S, Chatterji S, Verdes E, Tandon A, Patel V, Ustun B (2007) Depression, chronic diseases, and decrements in health: results from the World Health Surveys. Lancet (London, England) 370(9590):851–858. https://doi.org/10.1016/S0140-6736(07)61415-9
Pandit JJ, Collyer J, Buckler KJ (2010) “Hypoxic ventilatory decline” in the intracellular Ca2+ response to sustained is ocapnic hypoxia in carotid body glomus cells. Adv Exp Ental Med Biol 669:209–212. https://doi.org/10.1007/978-1-4419-5692-7_42
Parker G, Fletcher K, Paterson A, Anderson J, Hong M (2014) Gender differences in depression severity and symptoms across depressive sub-types. J Affect Disord 167:351–357. https://doi.org/10.1016/j.jad.2014.06.018
Sakr HF, Abbas AM, Elsamanoudy AZ, Ghoneim FM (2015) Effect of fluoxetine and resveratrol on testicular functions and oxidative stress in a rat model of chronic mild stress-induced depression. J Physiol Pharmacol Off J Pol Physiol Soc 66(4):515–527
Salomon JA, Carvalho N, Gutiérrez-Delgado C, Orozco R, Mancuso A, Hogan DR et al (2012) Intervention strategies to reduce the burden of non-communicable diseases in Mexico: cost effectiveness analysis. BMJ (Clin Res ed) 344:e355. https://doi.org/10.1136/bmj.e355
Shim RS, Baltrus P, Ye J, Rust G (2011) Prevalence, treatment, and control of depressive symptoms in the United States: results from the National Health and Nutrition Examination Survey (NHANES), 2005–2008. J Am Board Family Med JABFM 24(1):33–38. https://doi.org/10.3122/jabfm.2011.01.100121
Spencer PS, Schaumburg HH (eds) (2000) Experimental and clinical neurotoxicology, 2nd edn. Oxford University Press, Oxford
Tanvir EM, Whitfield KM, Ng JC, Shaw PN (2020) Development and validation of an ICP-MS method and its application to determine multiple trace elements in small volumes of whole blood and plasma. J Anal Toxicol. https://doi.org/10.1093/jat/bkaa033
Thithunguyen T, Miyagi S, Tsujiguchi H, Kambayashi Y, Hara A, Nakamura H et al (2019) Association between Lower intake of minerals and depressive symptoms among elderly Japanese women but not men: findings from Shika study. Nutrients 11(2):389. https://doi.org/10.3390/nu11020389
WHO (2014) Global health estimates 2014 summary tables. http://www.who.int/healthinfo/globalburdendisease/estimates/en/index2.html
WHO (2017) Depression and other common mental disorders. Global health estimates; WHO: Geneva, Switzerland, 2017; Available online: http://apps.who.int/iris/bitstream/handle/10665/254610/WHO-MSD-MER-2017.2-eng.pdf;jsessionid=7666696F2B865494E1DDFB4C5132EF81
WHO (2017) Depression fact sheet. http://www.who.int/mediacentre/factsheets/fs369/en/
Wu W, Jiang S, Zhao Q, Zhang K, Wei X, Zhou T et al (2018) Environmental exposure to metals and the risk of hypertension: a cross-sectional study in China. Environ Pollut (Barking, Essex : 1987) 233:670–678
Xu T, Jiao J, Zhu C, Li F, Guo X, Li J et al (2019) Prevalence and potential associated factors of depression among Chinese older inpatients. J Nutr Health Aging 23(10):997–1003. https://doi.org/10.1007/s12603-019-1270-2
Yang Z, Chen R, Hu X, Ren XH (2017) Factors that related to the depressive symptoms among elderly in urban and rural areas of China. Zhonghua liu xing bing xue za zhi = Zhonghua liu xing bing xue za zhi 38(8):1088–1093
Zamponi GW, Currie KP (2013) Regulation of Ca(V)2 calcium channels by G protein coupled receptors. Biochem Biophys Acta 1828(7):1629–1643. https://doi.org/10.1016/j.bbamem.2012.10.004
Zhang N, Shi GP, Wang Y, Chu XF, Wang ZD, Shi JM et al (2019) Depressive symptoms are associated with incident frailty in a Chinese population: the Rugao Longevity and aging study. Aging Clin Exp Res. https://doi.org/10.1007/s40520-019-01409-x
Zuo W, Nie L, Baskaran R, Kumar A, Liu Z (2018) Characterization and improved properties of Glutamine synthetase from Providencia vermicola by site-directed mutagenesis. Sci Rep 8(1):15640. https://doi.org/10.1038/s41598-018-34022-5
Acknowledgements
We thank all participants in this study. The authors are grateful to all people who contributed to this study, including the Lu’an Center for Disease Control and Prevention, Cheng bei Township Health Center and Bei shi community health service center. This work was supported by the National Key R&D Program of China (2016YFC1305900), the National Natural Science Foundation of China (81872662,82073558) and the Grants for Major Projects on College Leading Talent Team Introduced of Anhui (0303011224).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Lv, J., Li, Yl., Ren, Wq. et al. Increased depression risk for elderly women with high blood levels of strontium and barium. Environ Chem Lett 19, 1787–1796 (2021). https://doi.org/10.1007/s10311-020-01146-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10311-020-01146-y