
Abstract
Purpose Individual psychosocial factors are crucial in the return to work (RTW) process of workers with musculoskeletal disorders (MSDs) and common mental disorders (CMDs). However, the quality and validity of the questionnaires used to measure these factors have rarely been investigated. The present systematic search and literature review aims at identifying, categorizing, and evaluating the questionnaires (measurement tools) used to measure individual psychosocial factors related to the perception of the personal condition and motivation to RTW that are predictive of successful RTW among workers with MSDs or CMDs. Methods Through a systematic search on PubMed, Web of Science, and PsycINFO library databases and grey literature, we identified the individual psychosocial factors predictive of successful RTW among these workers. Then, we retrieved the questionnaires used to measure these factors. Finally, we searched for articles validating these questionnaires to describe them exhaustively from a psychometric and practical point of view. Results: The review included 76 studies from an initial pool of 2263 articles. Three common significant predictors of RTW after MSDs and CMDs emerged (i.e., RTW expectations, RTW self-efficacy, and work ability), two significant predictors of RTW after MSDs only (i.e., work involvement and the self-perceived connection between health and job), and two significant predictors of RTW after CMDs only (i.e., optimism and pessimism). We analyzed 30 questionnaires, including eight multiple-item scales and 22 single-item measures. Based on their psychometric and practical properties, we evaluated one of the eight multiple-item scales as questionable and five as excellent. Conclusions: With some exceptions (i.e., self-efficacy), the tools used to measure individual psychosocial factors show moderate to considerable room for improvement.
Similar content being viewed by others

Introduction
Musculoskeletal disorders (MSDs, such as low back pain) and common mental disorders (CMDs, such as depression) represent prominent causes of sickness absence and work disability worldwide [1]. An average of 6% of the working-age population in OECD countries have disability benefits as their primary income, and in some countries, this percentage doubles [2]. MSDs and CMDs account for 42% of the Years Lived with Disability (YLD) globally, with 21% each [3]. The employment rate of people with disabilities in OECD countries is on average 40% lower than that for the general population, and the unemployment rate is twice the overall level [2]. Work is crucial for people with disabilities, also because it promotes mental and physical recovery, functional abilities, and social participation [4]. In summary, MSDs and CMDs place hefty economic, social, and personal burdens on society.
It is therefore necessary to promote the return to work (RTW) of people with these disorders. To this end, there is well-established literature investigating the factors that facilitate and hinder the RTW. The RTW is regarded as a multidimensional process influenced mainly by psychosocial determinants (e.g., RTW expectations and job strain) and macrosystem variables (e.g., the healthcare and workplace systems) and, to a much lesser extent, by traditional medical indicators (e.g., symptom severity and prognosis) [5]. Reviews have highlighted that two categories of psychosocial factors are particularly relevant yet understudied for the RTW. The first category includes the organizational psychosocial factors associated with the genesis of strain, whereas the second includes individual psychosocial factors related to the perception of the personal condition and motivation to RTW [6,7,8]. A serious limitation of the study of psychosocial factors is the considerable heterogeneity in the definition and measurement of the psychosocial predictors among different studies [7, 9]. This limitation is associated with a lack of sufficiently validated measurement tools [7, 9]. Ultimately, this situation means that researchers and clinicians face a fragmented and inconsistent scientific literature when planning to measure individual and organizational psychosocial factors for a new study, clinical purposes, or international comparisons. It is therefore urgent to start identifying which psychosocial factors are relevant to the RTW process and how they are measured in order to identify both the pros and cons of existing measurement tools and gaps in the literature.
The present systematic search and literature review aims at identifying, categorizing, and evaluating the questionnaires used to measure the individual psychosocial factors related to the perception of the personal condition and motivation to RTW (e.g., RTW self-efficacy and RTW motivation, hereinafter referred to as “individual psychosocial factors”) that are predictive of RTW among workers with MSDs or CMDs. To this end, it is necessary first to identify the individual psychosocial factors predictive of successful RTW and then to review questionnaires in terms of their psychometric properties and practical information useful for clinicians. The same type of review, but concerning organizational work-related psychosocial factors predictive of RTW, has been conducted, and the results have been published elsewhere [10].
Methods
We adopted a two-phase search strategy. The first phase involved identifying the individual psychosocial factors predictive of successful RTW among workers with MSDs or CMDs and the related questionnaires used. In this review we considered two primary indicators of success in returning to work: (a) the probability of being back at work at the time of study follow-up, or (b) the time to return to the workplace, meaning the duration of work absence since the first day of absence due to the MSD or CMD. The review included both studies examining RTW as a single event and studies examining sustainable RTW (i.e., RTW for a minimum number of days). The second phase involved a search for articles that validated the questionnaire in order to describe them exhaustively from a psychometric and practical point of view.
Identification of the Individual Psychosocial Factors
Search Strategy
A systematic literature search was conducted in PubMed, PsycInfo, and Web of Science databases from January 1998 to January 2018 (20 years). We also performed a complementary search of non-indexed literature (Google Scholar) and identified additional articles from the bibliographic references in relevant articles. Four groups of keywords, combined by the Boolean operator and, were used. These groups were (i) outcome of interest (e.g., return to work or work participation or work reintegration), (ii) the work status (e.g., sickness or absence or off-work or disability or rehabilitation), (iii) psychosocial factors (e.g., work-ability or self-efficacy or expectation or motivation), and (iv) study type (e.g., longitudinal or prospective or wave study). A further group was added, combined with the Boolean operator and not, to exclude samples not of interest (e.g., stroke or brain injury or sclerosis or child).
Articles were selected if they met the following inclusion criteria: (1) they were prospective cohort studies; (2) study subjects had an MSD or a CMD or, for mixed population studies, at least two thirds (≥ 67%) of the study sample consisted of people suffering from an MSD and/or a CMD; (3) study subjects were workers on sick leave at the time of data collection (i.e., baseline), or if that was not the case, the condition of those not on sick leave or not employed was controlled for in the analyses; (4) the studies analyzed one of the two indicators of success in returning to work previously defined; (5) one or more individual psychosocial factors measured and tested as predictors of the outcome in multivariate regressions controlling for at least age and sex/gender; and (6) studies were written in English or French. The exclusion criteria were as follows: (1) articles were literature reviews, case studies, qualitative studies, or cross-sectional studies; and (2) study subjects were sick-listed workers with unspecified work disability.
Articles were selected first based on the title and abstract, then based on the full text. The article selection based on title and abstract was performed by three trained reviewers, PhD or Master’s students. Two additional independent reviewers (the first two authors) double-checked approximately 30% of the references. In case of discrepancy, an agreement was reached through discussion based on the information available in the title and abstract. The selection based on the full text was performed by one researcher (the first author). If the inclusion of an article was uncertain, another researcher (the second author) read the full text to reach a joint decision. When disagreement occurred after these two readings, a third researcher (last author) was consulted to reach full agreement.
Data Extraction
For each study selected, we gathered information about the individual psychosocial factors considered. We listed the population in which they were tested (i.e., MSD, CMD, or mixed), the crude and adjusted effects, and the type of outcomes. From this information, adopting the “best-evidence synthesis procedure” [11], we classified the individual factors as having a “limited”, “moderate”, “strong”, “insufficient”, or “inconsistent” level of evidence of their ability to predict RTW in the two populations considered separately. The level of evidence was attributed counting the number of multivariate effects tested that were statistically significant (p < 0.05) with a positive relationship with the outcome, statistically significant with a negative relationship with the outcome, and not statistically significant. At first, factors were scrutinized for consistency of the effects, that is, if the significant effects were in the same positive or negative direction. A factor was labeled as inconsistent if the ratio of significant positive effects to total (positive and negative) significant effects was between 0.45 and 0.65. If the factor was consistent, we determined the level of evidence supporting its predictivity based on X, where X equalled the ratio of significant positive (or negative) effects to total significant and non-significant effects. The rules were adapted from Gragnano et al. [7].
The level of evidence was classified as (o) insufficient, when X < 0.60; (i) limited, when only one significant effect (positive or negative) was found, or 0.60 ≤ X < 0.65; (ii) moderate, when only two significant effects in the same direction were found, or 0.65 ≤ X < 0.80; or (iii) strong, when 0.80 ≤ X ≤ 1.00.
We evaluated the number of effects separately for MSDs and CMDs. The effect tested in a sample consisting of both MSDs and CMDs was counted both in the evaluation of MSDs and that of CMDs. To be considered in the second step of identification of the measurement tools, a factor had to have a level of evidence classified at least as “moderate” for MSDs or CMDs.
It should be noted that the classifiers “insufficient”, “limited,” “moderate”, and “strong” did not pertain to the effect size of each factor. These classifiers represented the quantity (number of studies) and consistency (negative or positive relationship) of the effects (statistically significant and not) of each factor on the RTW success.
Identification and Description of the Measurement Tools
Search Strategy
For each factor predictive of RTW with at least a moderate level of evidence, we considered the studies that reported a multivariate statistically significant effect of that factor. For all these studies, we listed the tools used to measure the factor. For all the extracted questionnaires, we searched in the references and PubMed, PsycInfo, and Web of Science databases for articles validating the tools. From all these articles, we collected psychometric properties and practical information useful for clinicians.
We considered the following psychometric characteristics: (i) predictive validity; (ii) face validity; (iii) construct validity; (iv) internal consistency; (v) convergent validity; and (vi) test–retest reliability. All the measurement tools had predictive validity, as it was a requirement for inclusion in the list of tools. We reported information about the crude and adjusted effects detected with that tool. Face validity was estimated through qualitative inspection of the items used to measure a specific factor/concept in the measurement tool. Construct validity was evaluated positively if a factor analysis of the structure of the measure was found to exist. Internal consistency was evaluated positively if Cronbach’s alphas ranged between 0.70 and 0.95. Convergent validity was evaluated by significant and positive correlations with theoretically similar concepts. Test–retest reliability was rated positively when repeated testing of the same condition yielded comparable results (correlation coefficients higher than 0.60) [12].
The practical characteristics considered were (i) time required to complete the questionnaire, (ii) difficulties for the clinician in calculating the final score, (iii) fee or training needed for administering the questionnaire and interpreting the scores, and (iv) availability of the measurement tool. More specifically, the time required to complete the questionnaire was favorably rated if questionnaires had fewer than eight items. The final score was considered easy to calculate if it only required summing the items’ scores. The final score was considered difficult to obtain when a more complex formula was needed or when reversed items were present. The absence of a fee to pay and of training to follow on use of the measurement tool was evaluated positively. Instrument availability was evaluated positively if an English version of the measurement tool was easily available.
Based on how many psychometric and practical criteria the measurement tool met, we adopted rules for the evaluation (Table 1). Psychometric properties were evaluated for multiple-item scales. Therefore, single-item measures did not undergo a summary evaluation.
Results
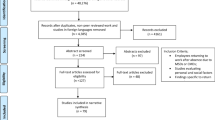
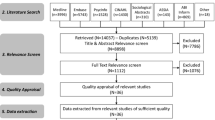
Figure 1 shows the results of the search strategy. In this study, we considered the individual psychosocial factors predictive of RTW. Villotti et al. published a similar review for organizational psychosocial factors [10]. The selection procedure in our study yielded 76 studies investigating individual psychosocial factors among people with an MSD and/or a CMD.

Results of the search strategy. The same publication can investigate both individual and organizational factors; therefore, the sum of the publications on individual and organizational factors is higher than the number of publications that met eligibility criteria
Among the individual psychosocial variables examined in these 76 studies, three were common significant predictors of RTW after MSDs and CMDs, two were significant predictors of RTW after MSDs only, and two others were significant predictors of RTW after CMDs only. Table 2 reports these predictors along with the references. We found a total of 35 effects for MSDs and 19 for CMDs. With regards to MSDs, RTW expectations, RTW self-efficacy, and work ability emerged as strong predictors of RTW, whereas work involvement and the self-perceived connection between health and job emerged as limited predictors. Apart from the self-perceived connection between health and job, these predictors were facilitators of the RTW process. With regards to CMDs, RTW self-efficacy was the only strong predictor of RTW, RTW expectations was a moderate predictor, and work ability, optimism, and pessimism were limited predictors of RTW. Apart from pessimism, these predictors were facilitators of the RTW process.
RTW Expectations
RTW expectations refers to the worker’s expectations of how difficult/likely/long the process of employment resumption will be. RTW expectations are a strong predictor of RTW after MSDs and a moderate one after CMDs (Table 2). The less difficult, more likely, or shorter the RTW process is expected to be, the more frequently this positive expectation will materialize. Table 3 describes the tools with predictive validity used to measure RTW expectations, along with their summary evaluation. Only one scale composed of more than one item was used. This scale was the Work-Related Recovery Expectations Questionnaire, whichwas used in three studies [13,14,15]. Following the rules for the summary evaluation of measurement tools, this questionnaire was evaluated as questionable because it met two out of six and three out of four psychometric and practical criteria, respectively. Nineteen single-item measures assessed RTW expectations [16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35]. No summary evaluation was performed of these tools because the psychometric criteria were not applicable. These single-item measures of RTW expectations can be classified as single-item measures with and without a time reference. The first group was subdivided into single-item measures with a time frame in terms of months (six measurement tools [16, 17, 28,29,30,31,32]) or in terms of weeks (three measurement tools [33,34,35]). The second group was subdivided into single-item measures that ask the respondents to estimate their confidence in the RTW (one measurement tool [18]), work ability (four measurement tools [19,20,21,22]), or the time they will take to RTW (five measurement tools [23,24,25,26,27]). Tables 4 and 5 (Online resources 1 and 2) report the psychometric and practical characteristics of the tools used to measure RTW expectations. Table 6 (Online resource 3) reports detailed information about the tools’ predictive validity.
RTW Self-efficacy
RTW self-efficacy indicates the belief the workers have in their ability to complete the RTW process successfully and to overcome possible obstacles during the RTW process. With four significant effects for MSDs and three for CMDs, RTW self-efficacy is a strong predictor of RTW after both MSDs and CMDs (Table 2). More specifically, a higher RTW self-efficacy is a facilitator of the RTW process. Table 3 describes the five scales with predictive validity used to measure RTW self-efficacy, along with their summary evaluation. The Self-efficacy for Return to Work Questionnaire [17, 36, 37] was evaluated as good. It did not meet two psychometric (i.e., construct validity and test–retest reliability) and two practical (i.e., length—8 items, and final score computation—not clearly defined) criteria. The other four scales were evaluated as excellent.
The Return-to-Work Self-Efficacy Scale [38, 39] failed to meet only one psychometric criterion (i.e., test–retest reliability) and one practical criterion (i.e., length; it consists of ten items). The Return-to-work Self-Efficacy Questionnaire [40,41,42,43,44,45] and the Return-to-Work Self-Efficacy Scale-19 [46] met all the psychometric criteria but did not meet two practical criteria (i.e., length and final score computation—some basic calculations needed to be made). Finally, the Return-to-Work Obstacles and Self-Efficacy Scale [ ROSES, 47] did not meet one psychometric (i.e., convergent validity) and two practical criteria (i.e., length—46 items, and final score computation). The length of ROSES is due, not only to the inclusion of two concepts at the same time (i.e., barriers to return to work and self-efficacy to overcome these RTW barriers), but also to the inclusion of 10 conceptual subscales (e.g., job demands). Tables 4 and 5 (Online resources 1 and 2) report the psychometric and practical characteristics of the tools used to measure RTW self-efficacy. Table 6 (Online resource 3) reports detailed information about the tools’ predictive validity.
Work Ability
In this context, work ability refers to the worker’s evaluation of his/her personal work capability in light of his/her health condition and the work demands. Work ability is a strong predictor of RTW after MSDs and a limited one after CMDs (Table 2). Increased work ability facilitates the return to work. Table 3 describes the measurement tools with predictive validity used to measure work ability, along with their summary evaluation. Two scales—Graded Reduced Work Scale [48, 49] and the Work Ability Index [50]—and three single-item measures were used. The Graded Reduced Work Ability Scale and the Work Ability Index were evaluated as good and excellent, respectively. Of the six psychometric criteria considered, the Graded Reduced Work Ability Scale scored four; there was no evidence of convergent and test–retest validity. The Work Ability Index scored five because a two-factor solution seemed to perform better than the hypothesized one-factor model [51]. Of the four practical criteria considered, the Graded Reduced Work Ability scale scored three; final score computation was not clearly defined, whereas the Work Ability Index scored two because of the length and of a complex final score computation. One single-item measure, the Single-Item WAI question [32, 52,53,54], consisted of one item from the Work Ability Index [50]. Unlike all the other single-item measures considered in this review, for the Single-Item WAI question, one study was found that compared the performance on the single item with that on the full scale, suggesting that the single item may be a good alternative to the full scale [55]. For this reason, the Single-Item WAI question is also reported in Table 4 (Online resource 1), even if a final score was not computed. The Single-Item WAI question asks the respondent to rate the current work ability compared to the best possible work ability. The other two single-item instruments asked how much the work ability is reduced by the “back disorders” [33] or at this “current moment in time” [25]. Tables 4 and 5 (Online resources 1 and 2) report the psychometric and practical characteristics of the tools used to measure work ability. Table 6 (Online resource 3) reports detailed information about the tools’ predictive validity.
Discussion
This review aimed at identifying and assessing the questionnaires used to measure individual psychosocial factors predictive of RTW among workers with MSDs or CMDs. We thus detected the individual psychosocial factors predictive of RTW. To our knowledge, this is the first work examining all the individual psychosocial predictors of RTW. A comparable review has been conducted, but it considered the measurement tools for only one individual psychosocial predictor of RTW (i.e., RTW expectations) [11, 12]. Our review identified three individual psychosocial factors that consistently predicted RTW among workers with MSDs or CMDs, that is, RTW self-efficacy, RTW expectations, and work ability. These three factors were all strong predictors of RTW after MSDs. However, only RTW self-efficacy was a strong predictor of RTW after CMDs. RTW expectations was a moderate predictor of RTW after CMDs and work ability was a limited predictor. These same factors have been identified as predictors of RTW for other diseases as well [7].
The studies included in the review show that more longitudinal studies have been conducted among workers with MSDs than CMDs. RTW expectations and work ability have been extensively studied, with 23 and 11 studies, respectively. Altogether, the other factors have been investigated in ten studies, with work involvement, self-perceived connection between health and job, optimism, and pessimism considered in only one study. In summary, 30 questionnaires about the three individual psychosocial factors with at least a moderate level of evidence of predictivity were analyzed. Of these instruments, only eight were multi-item scales; the 22 remaining tools were single-item measures for which it was impossible to provide a summary evaluation. Of the eight multi-item scales, only one was evaluated as questionable and five were evaluated as excellent.
RTW Self-efficacy
Self-efficacy is a very well-known and studied construct in the psychological field. This longstanding tradition is reflected in the high quality of the measurement tools analyzed in this review. Given the strong theoretical foundation of the construct and the quality of the instrument available, more studies should investigate the role of RTW self-efficacy in the RTW process. We retrieved only seven studies (two with the same sample) investigating RTW self-efficacy as a predictor of RTW among workers with MSDs or CMDs, a relatively low number compared to the 24 studies retrieved for RTW expectations.
Among the five questionnaires retrieved in this review that are used to measure RTW self-efficacy, four were evaluated as excellent. The Return-to-Work Self-Efficacy Scale [38, 39] was characterized by a balance in the number of practical and psychometric criteria met by the tool. However, if one is more interested in the psychometric properties, the Return-to-Work Self-Efficacy Questionnaire [40,41,42,43,44,45] and the Return-to-Work Self-Efficacy Scale-19 [46] met all the psychometric criteria. It is worth noting that these last two scales share eight items. Alternatively, the Return-to-Work Obstacles and Self-Efficacy Scale (ROSES) [47] assesses, on 10 conceptual dimensions, potential RTW barriers perceived by workers (46 items), and then measures the self-efficacy in overcoming them. This questionnaire is especially suitable for clinical purposes to evaluate more salient barriers such as difficult relationships with RTW stakeholders (e.g., manager, colleagues) or apprehensions regarding cognitive difficulties.
RTW Expectations
RTW expectations is the most studied factors among the four identified. This abundance of studies is partly due to how this factor is measured. Nineteen single-item measures were used, and only one scale. All these single items provided some predictive validity, as shown in Table 6 (Online resource 3), and they are short and easy to administer; therefore, RTW expectations can be measured in virtually every study at no cost. While this promotes extensive study of the factor and facilitates its evaluation in the clinical setting, we believe it also increases the risk of “HARKing”, in its form called “Suppress Loser Hypothesis” [56]. That is, the hypothesis of a significant effect of RTW expectations is not reported when results falsify it.
Moreover, none of the studies evaluated the reliability of the single-item measures. Even if it is commonly believed that single-item reliability cannot be estimated, this is not necessarily true [57, 58] and in fact should be estimated for RTW expectations, given the widespread adoption of single-item measures. However, estimating single-item reliability requires the presence of a validated scale consisting of more than one item. This step should be the first to be followed for the “RTW expectations” factor because the only scale proposed (i.e., Work-Related Recovery Expectations Questionnaire [13,14,15]) had some psychometric limitations, as shown in Table 4 (Online resource 1). A detailed discussion about the formulation of single items used to measure RTW expectations can be found in a dedicated review [59].
Work Ability
In studies examining RTW from a psychosocial perspective, work ability is consistently defined as the worker’s evaluation of his/her personal work capability in light of his/her health condition and the work demands. However, having examined the entire body of scientific literature, it is evident that the concept of work ability has several different meanings [60]. This plurality of meanings explains why some readers may be disoriented by the adopted definition of work ability. A systematic scoping review analyzed this and the other definitions of work ability [60].
The ambiguous nature of the concept work ability is reflected, to some extent, in the two scales used to measure it that we retrieved in this review, the Work Ability Index and the Graded Reduced Work Ability Scale. The Work Ability Index, evaluated in this review as an excellent questionnaire, is very popular, especially in Europe. It was developed by members of the Finnish Institute of Occupational Health (FIOH) [50] and translated into more than 20 languages. The tool was supposed to be unidimensional, but data from different countries supported a factor solution with two dimensions [51]. Radkiewicz et al. [51] defined these two factors as the “objective” and “subjective” components of work ability. Commenting further on their results, we suggest that the two factors are the consequence of the mixing of two different conceptualizations of work ability. The “objective” factor reflects a biomedical conceptualization in which the physical impairments/diseases linearly determine work (dis)ability. The “subjective” factor closely reflects the definition of work ability that we adopted, i.e., work ability as the result of the interaction between the individual’s mental and physical health and the work demands [60]. This situation is not ideal since the Work Ability Index has only one final score. By considering the scores for the two factors separately, it would be more apparent which one of the two definitions is more useful in different contexts.
In this sense, the Single Item WAI question [32, 52,53,54] uses only one item of the Work Ability Index, the one with the highest factor loading on the “subjective” factor; it is, therefore, a precise measure of the “subjective” conceptualization of work ability. Moreover, the single item WAI question is the only single-item measure among all those retrieved in this review that has been validated. This validation was obtained by comparing performance on the single item with that on the full version of the Work Ability Index and represents a procedure that should be adopted more often when using single-item measures.
The Graded Reduced Work Ability Scale, evaluated in this review as a good measurement tool, presented a one-factor structure, but no factor loadings were reported in the article, and the variance explained by the single factor was 51% of the total variance [61]. Even in this scale, different conceptualizations of work ability are apparent if one examines the items. Beyond the personal evaluation of work capability in light of the health condition and the work demands, the Graded Reduced Work Ability Scale has items measuring other dimensions. These dimensions are the perceived work ability to perform “other work” (item 1), the perceived functional limitation due to the health complaint (item 3), the perceived severity of the health complaint (item 4), the perceived effect of the work activity on health (item 5), and a generic evaluation of other health complaints (item 6). It is worth noting that the predictive validity of the Graded Reduced Work Ability Scale was tested in only one study [61] but with discriminant analysis. The other study using the Graded Reduced Work Ability Scale [49] analyzed only three of the six items (reduced ability to work, the belief that work will aggravate the condition, and other complaints) as single items.
The Work Ability Index and the Graded Reduced Work Ability Scale were designed for practical purposes. These scales try to capture many facets of work ability in order to be as predictive as possible. This legitimate approach leaves room for psychometric improvements to be made to both scales.
Strengths and Limitations
Other reviews have already investigated the measurement of RTW [62, 63], but this review is the first to examine the individual psychosocial predictors of RTW. The primary aim of the review was to identify and evaluate the questionnaires used to measure individual psychosocial factors predictive of RTW among workers with MSDs or CMDs. Pursuing this specific aim had two significant consequences. First, it was necessary to identify the predictive factors of RTW even though this was not the primary aim. For this reason, we did not focus our efforts on a meta-analysis of the effects of all the retrieved factors, which would have been the most reliable method for identifying the significant factors. Instead, we relied on a more resource-efficient approach: the “best-evidence synthesis procedure” [11]. We counted the significant and non-significant effects retrieved and determined the predictivity of the factor if the ratio between significant and non-significant effects was higher than a coefficient chosen a priori. While this may be a limitation of the present review, the procedure has already been successfully adopted in other reviews [6, 7, 64], and it is appropriate, given the primary aim of the review.
Second, substantial evidence in support of predictivity can be generated only when the predictors temporally precede the outcome. Therefore, we limited our inclusion criteria to prospective cohort studies. This criterion limited the number of studies and measurement tools we considered for all the individual psychosocial factors because many have been studied only in cross-sectional studies. More longitudinal studies are needed for individual psychosocial factors predictive of RTW among workers with CMDs. Other measurement tools with good psychometric and practical properties may exist but, because their predictive validity has not been tested longitudinally, they were not included in this review. While this may be considered a limitation of the present review, it also providesgreater confidence that the selected tools have predictive ability.
Another limitation of this review is the restriction on the type of psychosocial predictors and RTW outcomes we considered. As explained in the introduction, we focused on individual psychosocial factors related to the perception of the personal condition and motivation to RTW. Thus, other important psychosocial factors were not considered. Nevertheless, we acknowledge the relevance of age and gender because in phase 1—Identification of the individual psychosocial factors, we required the included studies to control for these two variables. Regarding the RTW outcomes, we considered the probability of being back at work at the time of study follow-up and the time to return to the workplace. There are other outcomes of the RTW process that have been used in the literature (e.g., number of days of absence during the observation time [65]). The studies that used these other RTW outcomes were not included in this review. Therefore, other sound measurement tools may not be included in this review because they were tested only against other RTW outcomes. Regardless, we believe that we identified most of the measurement tools used in the RTW literature, as the two definitions of RTW outcome we chose are those most frequently adopted in the studies investigating RTW specifically [63, 66].
Conclusions
Promoting RTW after the onset of physical or mental disability has become crucial for the economy, society, and life of people in all industrialized countries. Despite the traditional importance of medical factors in the RTW process, individual psychosocial factors have been increasingly studied and considered crucial to the process. Today, it is recognized that these factors should be considered during the early phases of the RTW process. Our review provided a classification of the tools measuring individual psychosocial factors that have been used in the scientific literature and showing predictive validity among workers with MSDs and CMDs. The psychometric and practical characteristics of the measurement tools were identified, reported, and discussed in this study. We also proposed suggestions for improving the measurement of all the significant predictive factors based on the identified limitations of the measurement tools available. The list of measurement tools proposed can promote the use of high-quality existing instruments in new studies rather than the often-adopted practice of creating new questionnaires from scratch. Similarly, having a reference list of measurement tools can support the translation of high-quality instruments into new languages and their validation in new cultures.
Finally, we believe that the review results will be useful and valuable not only for researchers and clinicians working on work disability, but also for policymakers involved in developing RTW policies.
References
James SL, Abate D, Abate KH, Abay SM, Abbafati C, Abbasi N, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 Diseases and Injuries for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392:1789–858.
OECD. Sickness, disability and work: breaking the barriers. Paris: OECD Publishing; 2010.
Vigo D, Thornicroft G, Atun R. Estimating the true global burden of mental illness. Lancet Psychiatry. 2016;3:171–8.
Waddell G, Burton AK. Is work good for your health and well-being? London: TSO (The Stationery Office); 2006.
Costa-Black KM, Feuerstein M, Loisel P. Work disability models: past and present. In: Loisel P, Anema JR, editors. Handbook of work disability. New York, NY: Springer; 2013. p. 71–93.
Steenstra IA, Munhall C, Irvin E, Oranye N, Passmore S, Van Eerd D, et al. Systematic review of prognostic factors for return to work in workers with sub acute and chronic low back pain. J Occup Rehabil. 2017;27:369–81.
Gragnano A, Negrini A, Miglioretti M, Corbière M. Common psychosocial factors predicting return to work after common mental disorders, cardiovascular diseases, and cancers: a review of reviews supporting a cross-disease approach. J Occup Rehabil. 2018;28:215–31.
Loisel P, Anema JR. Handbook of work disability. New York: Springer; 2013.
Main CJ, Shaw WS. Conceptual, methodological, and measurement challenges in addressing return to work in workers with musculoskeletal disorders. In: Schultz IZ, Gatchel R, editors. Handbook of return to work: from research to practice. New York: Springer; 2016. p. 423–38.
Villotti P, Gragnano A, Larivière C, Negrini A, Dionne CE, Corbière M. Tools appraisal of organizational factors associated with return-to-work in workers on sick leave due to musculoskeletal and common mental disorders: a systematic search and review. J Occup Rehabil. 2020. https://doi.org/10.1007/s10926-020-09902-1.
Slavin RE. Best evidence synthesis: an intelligent alternative to meta-analysis. J Clin Epidemiol. 1995;48:9–18.
Corbiere M, Fraccaroli F. La conception, la validation, la traduction et l’adaptation transculturelle d’outils de mesure : Exemples dans le domaine de la santé mentale Conception, validation and transcultural adaptation for measurement tools: examples in the mental health field. In: Corbière M, Larivière N, editors. Méthodes qualitatives, quantitatives et mixtes dans la recherche en sciences humaines, sociales et de la santé. 2nd ed. Quebec: Presses de l’Université du Québec (PUQ); 2020. p. 781–841.
Gross DP, Battié MC. Work-related recovery expectations and the prognosis of chronic low back pain within a workers’ compensation setting. J Occup Environ Med. 2005a;47:428–33.
Gross DP, Battié MC. Recovery expectations predict recovery in workers with back pain but not other musculoskeletal conditions. J Spinal Disord Technol. 2010;23:451–6.
Gross DP, Battié MC. Functional capacity evaluation performance does not predict sustained return to work in claimants with chronic back pain. J Occup Rehabil. 2005b;15:285–94.
Carriere JS, Thibault P, Sullivan MJL. The mediating role of recovery expectancies on the relation between depression and return-to-work. J Occup Rehabil. 2015;25:348–56.
Dionne CE, Bourbonnais R, Fremont P, Rossignol M, Stock SR, Larocque I. A clinical return-to-work rule for patients with back pain. Can Med Assoc J. 2005;172:1559–67.
Opsahl J, Eriksen HR, Tveito TH. Do expectancies of return to work and job satisfaction predict actual return to work in workers with long lasting LBP? BMC Musculoskelet Disord. 2016;17:481.
Nielsen MBD, Madsen IEH, Bultmann U, Christensen U, Diderichsen F, Rugulies R. Predictors of return to work in employees sick-listed with mental health problems: findings from a longitudinal study. Eur J Public Health. 2011;21:806–11.
Heymans MW, de Vet HCW, Knol DL, Bongers PM, Koes BW, van Mechelen W. Workers’ beliefs and expectations affect return to work over 12 months. J Occup Rehabil. 2006;16:685–95.
Heijbel B, Josephson M, Jensen I, Stark S, Vingård E. Return to work expectation predicts work in chronic musculoskeletal and behavioral health disorders: prospective study with clinical implications. J Occup Rehabil. 2006;16:173–84.
Lindell O, Johansson S-E, Strender L-E. Predictors of stable return-to-work in non-acute, non-specific spinal pain: low total prior sick-listing, high self prediction and young age. A two-year prospective cohort study. BMC Fam Pract. 2010;11:53.
Aasdahl L, Pape K, Jensen C, Vasseljen O, Braathen T, Johnsen R, et al. Associations between the Readiness for Return to Work Scale and return to work: a prospective study. J Occup Rehabil. 2018;28:97–106.
Richter J, Blatter B, Heinrich J, de Vroome E, Anema J. Prognostic factors for disability claim duration due to musculoskeletal symptoms among self-employed persons. BMC Public Health. 2011;11:945.
Sampere M, Gimeno D, Serra C, Plana M, López JC, Martínez JM, et al. Return to work expectations of workers on long-term non-work-related sick leave. J Occup Rehabil. 2012;22:15–26.
Nieuwenhuijsen K, Verbeek JH, de Boer AG, Blonk RW, van Dijk FJ. Predicting the duration of sickness absence for patients with common mental disorders in occupational health care. Scand J Work Environ Health. 2006;32:67–74.
Steenstra IA, Koopman FS, Knol DL, Kat E, Bongers PM, de Vet HCW, et al. Prognostic factors for duration of sick leave due to low-back pain in dutch health care professionals. J Occup Rehabil. 2005;15:591–605.
Turner JA, Franklin G, Fulton-Kehoe D, Sheppard L, Wickizer TM, Wu R, et al. Worker recovery expectations and fear-avoidance predict work disability in a population-based workers’ compensation back pain sample. Spine. 2006;31:682–9.
Turner JA, Franklin G, Fulton-Kehoe D, Sheppard L, Wickizer TM, Wu R, et al. Early predictors of chronic work disability associated with carpal tunnel syndrome: a longitudinal workers’ compensation cohort study. Am J Ind Med. 2007;50:489–500.
Du Bois M, Szpalski M, Donceel P. Patients at risk for long-term sick leave because of low back pain. Spine J. 2009;9:350–9.
Du Bois M, Donceel P. A screening questionnaire to predict no return to work within 3 months for low back pain claimants. Eur Spine J. 2008;17:380–5.
Wåhlin C, Ekberg K, Persson J, Bernfort L, Oberg B. Association between clinical and work-related interventions and return-to-work for patients with musculoskeletal or mental disorders. J Rehabil Med. 2012;44:355–62.
Reiso H, Nygård JF, Jørgensen GS, Holanger R, Soldal D, Bruusgaard D. Back to work: predictors of return to work among patients with back disorders certified as sick. Spine. 2003;28:1468–73.
Reme SE, Hagen EM, Eriksen HR. Expectations, perceptions, and physiotherapy predict prolonged sick leave in subacute low back pain. BMC Musculoskelet Disord. 2009;10:139.
Løvvik C, Shaw W, Øverland S, Reme SE. Expectations and illness perceptions as predictors of benefit recipiency among workers with common mental disorders: secondary analysis from a randomised controlled trial. BMJ Open. 2014;4:1–9.
Richard S, Dionne CE, Nouwen A. Self-efficacy and health locus of control: relationship to occupational disability among workers with back pain. J Occup Rehabil. 2011;21:421–30.
Dionne CE, Bourbonnais R, Frémont P, Rossignol M, Stock SR, Nouwen A, et al. Determinants of “return to work in good health” among workers with back pain who consult in primary care settings: a 2-year prospective study. Eur Spine J. 2007;16:641–55.
Brouwer S, Amick BC, Lee H, Franche R-L, Hogg-Johnson S. The predictive validity of the Return-to-Work Self-Efficacy Scale for return-to-work outcomes in claimants with musculoskeletal disorders. J Occup Rehabil. 2015;25:725–32.
Brouwer S, Franche R-L, Hogg-Johnson S, Lee H, Krause N, Shaw WS. Return-to-work self-efficacy: development and validation of a scale in claimants with musculoskeletal disorders. J Occup Rehabil. 2011;21:244–58.
Lagerveld SE, Blonk RWB, Brenninkmeijer V, Schaufeli WB. Return to work among employees with mental health problems: development and validation of a self-efficacy questionnaire. Work Stress. 2010;24:359–75.
Lagerveld SE, Brenninkmeijer V, Blonk RWBB, Twisk J, Schaufeli WB. Predictive value of work-related self-efficacy change on RTW for employees with common mental disorders. Occup Environ Med. 2017;74:381–3.
Nieuwenhuijsen K, Noordik E, van Dijk FJH, van der Klink JJ. Return to work perceptions and actual return to work in workers with common mental disorders. J Occup Rehabil. 2013;23:290–9.
Volker D, Zijlstra-Vlasveld MC, Brouwers EPM, van Lomwel AGC, van der Feltz-Cornelis CM. return-to-work self-efficacy and actual return to work among long-term sick-listed employees. J Occup Rehabil. 2015;25:423–31.
Huijs JJJM, Koppes LLJ, Taris TW, Blonk RWB. Differences in predictors of return to work among long-term sick-listed employees with different self-reported reasons for sick leave. J Occup Rehabil. 2012;22:301–11.
Huijs JJJM, Koppes LLJ, Taris TW, Blonk RWB. Work characteristics and return to work in long-term sick-listed employees with depressive symptoms. J Occup Rehabil. 2017;27:612–22.
Shaw WS, Reme SE, Linton SJ, Huang Y-H, Pransky G. 3rd place, PREMUS best paper competition: development of the return-to-work self-efficacy (RTWSE-19) questionnaire—psychometric properties and predictive validity. Scand J Work Environ Health. 2011;37:109–19.
Corbière M, Negrini A, Durand M-J, St-Arnaud L, Briand C, Fassier J-B, et al. Development of the Return-to-Work Obstacles and Self-Efficacy Scale (ROSES) and validation with workers suffering from a common mental disorder or musculoskeletal disorder. J Occup Rehabil. 2017;27:329–41.
Haldorsen EMH, Kronholm K, Skouen JS, Ursin H. Predictors for outcome of a multi-modal cognitive behavioural treatment program for low back pain patients—a 12-month follow-up study. Eur J Pain. 1998;2:293–307.
Hagen EM, Svensen E, Eriksen HR. Predictors and modifiers of treatment effect influencing sick leave in subacute low back pain patients. Spine. 2005;30:2717–23.
Ilmarinen J. The Work Ability Index (WAI). Occup Med. 2007;57:160–160.
Radkiewicz P, Widerszal-Bazyl M. Psychometric properties of Work Ability Index in the light of comparative survey study. Int Congr Ser. 2005;1280:304–9.
Netterstrøm B, Eller NH, Borritz M. Prognostic factors of returning to work after sick leave due to work-related common mental disorders: a one- and three-year follow-up study. Biomed Res Int. 2015;2015:1–7.
Kuijer PPFM, Gouttebarge V, Wind H, van Duivenbooden C, Sluiter JK, Frings-Dresen MHW. Prognostic value of self-reported work ability and performance-based lifting tests for sustainable return to work among construction workers. Scand J Work Environ Heal. 2012;38:600–3.
van der Giezen AM, Bouter LM, Nijhuis FJN. Prediction of return-to-work of low back pain patients sicklisted for 3–4 months. Pain. 2000;87:285–94.
Ahlstrom L, Grimby-Ekman A, Hagberg M, Dellve L. The work ability index and single-item question: associations with sick leave, symptoms, and health—a prospective study of women on long-term sick leave. Scand J Work Environ Heal. 2010;36:404–12.
Kerr NL. HARKing: hypothesizing after the results are known. Personal Soc Psychol Rev. 1998;2:196–217.
Wanous JP, Hudy MJ. Single-Item reliability: a replication and extension. Organ Res Methods. 2001;4:361–75.
Zijlmans EAO, van der Ark LA, Tijmstra J, Sijtsma K. Methods for estimating item-score reliability. Appl Psychol Meas. 2018;42:553–70.
Young AE, Besen E, Choi YS. The importance, measurement and practical implications of worker’s expectations for return to work. Disabil Rehabil. 2015;37:1808–16.
Lederer V, Loisel P, Rivard M, Champagne F. Exploring the diversity of conceptualizations of work (dis)ability: a scoping review of published definitions. J Occup Rehabil. 2014;24:242–67.
Haldorsen EMH, Indahl A, Ursin H. Patients with low back pain not returning to work—a 12-month follow-up study. Spine. 1998;23:1202–7.
Biering K, Hjollund NH, Lund T. Methods in measuring return to work: a comparison of measures of return to work following treatment of coronary heart disease. J Occup Rehabil. 2013;23:400–5.
Wasiak R, Young AE, Roessler RT, McPherson KM, van Poppel MNM, Anema JR. Measuring return to work. J Occup Rehabil. 2007;17:766–81.
Detaille SI, Heerkens YF, Engels JA, van der Gulden JW, van Dijk FJ. Common prognostic factors of work disability among employees with a chronic somatic disease: a systematic review of cohort studies. Scand J Work Environ Health. 2009;35:261–81.
Truchon M, Schmouth MÈ, Côté D, Fillion L, Rossignol M, Durand MJ. Absenteeism screening questionnaire (ASQ): a new tool for predicting long-term absenteeism among workers with low back pain. J Occup Rehabil. 2012;22:27–50.
Steenstra IA, Lee H, de Vroome EMM, Busse JW, Hogg-Johnson SJ. Comparing current definitions of return to work: a measurement approach. J Occup Rehabil. 2012;22:394–400.
Anema JR, Schellart AJM, Cassidy JD, Loisel P, Veerman TJ, van der Beek AJ. Can cross country differences in return-to-work after chronic occupational back pain be explained? An exploratory analysis on disability policies in a six country cohort study. J Occup Rehabil. 2009;19:419–26.
Jensen AGC. A two-year follow-up on a program theory of return to work intervention. Work. 2013;44:165–75.
Ekberg K, Wahlin C, Persson J, Bernfort L, Oberg B. Early and late return to work after sick leave: predictors in a cohort of sick-listed individuals with common mental disorders. J Occup Rehabil. 2015;25:627–37.
Brouwer S, Reneman MF, Bültmann U, van der Klink JJL, Groothoff JW. A prospective study of return to work across health conditions: perceived work attitude, self-efficacy and perceived social support. J Occup Rehabil. 2010;20:104–12.
Kronström K, Karlsson H, Nabi H, Oksanen T, Salo P, Sjösten N, et al. Optimism and pessimism as predictors of work disability with a diagnosis of depression: a prospective cohort study of onset and recovery. J Affect Disord. 2011;130:294–9.
Gross DP, Battié MC. Factors influencing results of functional capacity evaluations in workers’ compensation claimants with low back pain. Phys Ther. 2005c;85:315–22.
Funding
Open access funding provided by Università degli Studi di Milano - Bicocca within the CRUI-CARE Agreement.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Gragnano, A., Villotti, P., Larivière, C. et al. A Systematic Search and Review of Questionnaires Measuring Individual psychosocial Factors Predicting Return to Work After Musculoskeletal and Common Mental Disorders. J Occup Rehabil 31, 491–511 (2021). https://doi.org/10.1007/s10926-020-09935-6
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10926-020-09935-6