



Adolescence is a phase of life in which considerable physical changes occur that may interfere with the development of body image(1). It is also during this period that life habits are established, generating long-term health consequences(2). In addition, it is possible to identify the presence of environmental and behavioural risk factors that threaten the health and quality of life of adolescents, such as unhealthy eating behaviours and practices and, consequently, body dissatisfaction (BD)(1).
BD is defined by the perception of wanting a different body, that is, it is represented by the perceived difference between the real and the idealised body, as well as a person’s negative thoughts and feelings about their body(Reference Grogan3). Currently, the presence of BD represented by the desire to lose weight has been growing, especially in female adolescents(Reference Grogan3–Reference Regnier, Le Bihan and Tichit6). According to a study, female adolescents between 12 and 15 years of age have higher BD values when compared with women of all ages(Reference Izydorczyk and Sitnik-Warchulska7), and the prevalence of BD varies from 44·9 to 71·7 % according to the population investigated and the instrument applied(Reference Dion, Hains and Vachon4,Reference Felden, Claumann and Sacomori5,Reference Chagas, Ferreira and Hartmann8–Reference Petroski, Pelegrini and Glaner15) .
The evidence that investigates the aetiology of BD reinforces its multifactorial and complex character, in which sociocultural pressures, the ideal of thin beauty, dietary practices, unhealthy behaviours for weight control, teasing and negative comments regarding weight or body, especially when performed by the family, seem to be the main risk factors for this condition(Reference Regnier, Le Bihan and Tichit6,Reference Abdalla, Buffarini and Weber16–Reference Terhoeven, Nikendei and Bärnighausen19) . In girls, the negative comments and teasing about their bodies made by their parents pass on the ideal of thin beauty, which is often unattainable and, consequently, has an impact on BD(Reference Abdalla, Buffarini and Weber16–Reference Philippi and Leme18). According to a study, in adolescents, the feeling that their parents considered them fatter than the ideal negatively influenced the perception of their own body, increasing BD throughout adolescence, as well as the chances of making weight loss attempts(Reference Abdalla, Buffarini and Weber16). In another survey, BD was present in approximately three-quarters (73·0 %) of girls who reported suffering weight-related teasing by the family(Reference Leme and Philippi20). In addition, parents’ incentive to control weight or body shape has already been identified as a strong predictor of BD(Reference Helfert and Warschburger21). However, most studies that investigate parents’ behaviours and the pressures related to weight do not individually assess the influence of parents(Reference Abdalla, Buffarini and Weber16,Reference Philippi and Leme18) .
Risk behaviours for eating disorders, unhealthy behaviours for weight control, dieting and eating restrictions are some of the factors in which BD acts as a predictor(Reference Terhoeven, Nikendei and Bärnighausen19,Reference Duarte, Palombo and Solis-Cordero22,Reference Neumark-Sztainer, Bauer and Friend23) , which can cause negative health consequences for adolescents(Reference Berg and Larsson24–Reference Perkins and Brausch26). Among the negative health consequences caused by these behaviours, suicidal ideation stands out, as well as the high rates of morbidity and mortality(Reference Perkins and Brausch26–Reference Guest, Bilgin and Pearce28), highlighting the need to carry out studies and early screening in adolescents, both in BD and in cited behaviours.
Some studies that investigated BD in female adolescents were identified, analysing the associations with parental(Reference Abdalla, Buffarini and Weber16,Reference Philippi and Leme18) and personal aspects in weight control practices(Reference Dion, Blackburn and Auclair11,Reference Abdalla, Buffarini and Weber16,Reference Philippi and Leme18,Reference Frank, Claumann and Felden29) . However, few studies have evaluated the behaviours related to the weight of the father and the mother, individually(Reference Neumark-Sztainer, Bauer and Friend23,Reference Keery, Boutelle and Van Den Berg30,Reference Rodgers and Chabrol31) . Given this context, the present study aimed to identify BD – constituted by the desire to lose weight – and possible associations with parental and personal aspects related to body shape and practices for weight control and loss in female adolescents from public schools in Caxias do Sul/Rio Grande do Sul (RS), Brazil.
Methods
Study design and population
This is an epidemiological observational study with a cross-sectional, school-based design. The study population consisted of female adolescents, enrolled in the 8th and 9th grades of elementary school in public schools in the urban area of the city of Caxias do Sul/RS, Brazil. This study is part of the project called ‘Health risk behaviors in elementary school adolescents in Caxias do Sul, RS’, the main objective of which is to identify and evaluate the health risk behaviours of students.
Sample characteristics
During the investigation period, the urban area of the city of Caxias do Sul/RS had thirty-nine state and sixty-one municipal schools that included primary education for the final years, in which there were 8924 students enrolled, representing 83·0 % of all students in 8th- and 9th-grade classes(32).
Sampling was carried out by clusters in two stages, with a probability proportional to the size of the clusters. Initially, the schools were divided according to the fourteen administrative regions of the urban area of the municipality. In order to reach the sample number, in the first stage, the average number of students per class was considered; thus, eighty classes were included. According to the number of classes in each school, thirty-one public schools were systematically drawn to enter the survey. In the second stage, the classes were chosen by simple drawing.
Female schoolchildren enrolled in classes of the 8th and 9th grades of elementary school in public schools belonging to the urban area of the city of Caxias do Sul/RS were included in the study. Adolescents who were on a diet for special conditions, pregnant women and nursing mothers were not included in the study. At the time of data analysis, those over the age of 19 years, who did not correctly complete the outcome assessment instrument and had a positive BD – desire to gain weight – were excluded from the study.
Data collection
Data collection took place between May and June 2016 carried out by the three research coordinators and by eleven academic volunteers from the Nutrition and Biomedicine courses, who were previously trained and supervised the application of a standardised questionnaire, pre-coded, pre-tested and self-administered, composed of questions prepared by the researchers themselves, based on the National School Health Survey (Pesquisa Nacional de Saúde do Escolar 2015)(1) and the Project Eating Among Teens(Reference Neumark-Sztainer, Wall and Larson33), as well as by questions regarding other instruments. The instrument used, as well as the logistics and field supervisors, was tested in a pilot study carried out in a municipal school in the city of São Leopoldo/RS.
Regarding demographic variables, the following were investigated: age (collected in full years and, later, categorised as: ≤13, 14, 15 and ≥16 years), skin colour (self-reported and categorised as white and non-white) and school year (collected as a dichotomous categorical variable in the 8th or 9th grade).
The socio-economic aspects included the mother’s schooling, obtained with the following question: ‘What level (degree) of education did your mother studied or study?’(1). Afterwards, the variable was categorised as follows: did not study and/or incomplete elementary school, complete elementary school and/or incomplete high school, complete high school and/or incomplete higher education and complete higher education and/or specialisations.
Nutritional status was assessed by means of BMI, calculated by the ratio between body mass (in kg) and height squared (in m) (kg/m2). The data required for the calculation, weight and height, were self-reported. According to studies(Reference Allison, Colby and Opoku-Acheampong34–Reference Strauss40), self-reported weight and height data for calculating BMI are in agreement with the measured values and can be used with adolescents. For the classification of BMI, according to WHO references for adolescents, the following categories were adopted: underweight (z-score < −2), eutrophy (z-score > −2 and z-score < +1), overweight (z-score > +1) and obesity (z-score > +2)(41).
To investigate the parents’ behaviours related to weight, the behaviours of the mother – or maternal figure – and father – or father figure – were individually researched. The girls answered the following questions: ‘My mother/father diets to lose weight or avoid gaining weight”, “My mother/father encourages me to eat healthy foods’, ‘My mother/father encourages me to diet to control weight’, ‘My mother/father talks about my weight’ and ‘My mother/father comments on other people’s weight’(Reference Neumark-Sztainer, Bauer and Friend23). The response options were assessed by frequency in: ‘never’, ‘rarely’, ‘sometimes’ and ‘always’. In addition, the adolescents were instructed to consider a maternal figure and father figure those who are responsible for them (stepmother/stepfather, grandmother/grandfather, aunt/uncle, others).
The student’s attitudes towards weight, the frequency of weighing, the use of diets for weight loss, as well as unhealthy eating behaviours for weight control were researched as variables of weight control practices. To investigate the adolescents’ attitudes towards weight, the following question was used: ‘Regarding your weight, you are currently trying to: lose weight, stay on the same weight, gain weight or I am not trying to do anything about my weight’. Subsequently, the variable was categorised as: nothing, maintaining weight, gaining weight and losing weight(1,Reference Chin, Laverty and Filippidis42) .
Regarding the frequency of weighing, the categorisation took place as follows: less than once a month, once a month, more than once a month/less than once a week and once a week or more. In addition, the practice of dieting last year was identified – any changes in the way of eating in order to lose weight are considered diet – presenting the following response options: never, 1–4 times during the last year, 5–10 times during the last year, more than 10 times during the last year and I am always on a diet (categorised as: never, 1–4 times a year and ≥5 times a year)(Reference Neumark-Sztainer, Wall and Larson33).
Regarding unhealthy eating behaviours for weight loss, the practice of not eating or eating very little food, skipping meals and following a high-protein, low-carbohydrate diet were investigated(Reference Neumark-Sztainer, Wall and Larson33). The answers obtained alternate in: no time, less than once a week, once a week or more.
Outcome
The BD was obtained through the silhouette scale validated for Portuguese by Conti & Latorre(Reference Conti and Latorre43) based on the proposal by Thompson & Gray(Reference Thompson and Gray44). The instrument allows the adolescent to identify, through figures, the current silhouette, considering the perception in relation to her own body at the time of the research, as well as the desired silhouette. The result of this scale consists of a scoring system (−8 to +8), the greater the difference, the greater the body discrepancy and, consequently, the more dissatisfied is the adolescent(Reference Scagliusi, Alvarenga and Polacow45). Thus, the BD was verified from values other than zero, with positive values expressing the desire to gain weight and negative values to lose weight.
In order to analyse and compare the data, in view of the objective of the study, schoolchildren with positive BD were excluded, that is, those who had a desire to gain weight. Therefore, the sample was divided between those with BD (desire to lose weight) and without BD.
Statistical analysis and justification of sample size
The sample size was calculated considering a prevalence of 70·0 % of BD – represented by the desire to lose weight – in female adolescents, with a margin of error of 4·0 %, significance level of 95·0 % and loss of 10·0 %, requiring 624 adolescents. The calculation was based on the study by Lawler & Nixon(Reference Lawler and Nixon13), which found a prevalence of BD, assessed by the scale of silhouettes of Thompson & Gray(Reference Thompson and Gray44), of 70·2 % in female adolescents aged 12–19 years. The calculation was performed using WinPepi 3.18 software.
Data entry was performed with double entry in the EpiData Program, version 3.1. For the analysis of the data, the program Statistical Package for the Social Sciences® (SPSS), version 18.0 was used. Initially, data consistency analyses were conducted, performing the validation to identify typing errors after every 100 typed questionnaires.
The sample consisted of 904 female students. At the time of data analysis, in order to minimise confounding factors, adolescents who were trying to gain weight were excluded, as well as those who were identified with positive BD. Thus, 685 students participated in the study, representing a sample reduction of 24·22 % to control confounding factors.
The sample description was presented by absolute and relative frequencies. To check the proportion between the independent variables and the BD, the bivariate analysis was performed using the χ 2 test. The crude analysis was applied to identify the crude prevalence ratios (PR) and respective 95 % CI, in order to demonstrate the effect of the sample characteristics on the BD.
Subsequently, multivariate analysis was performed, using Poisson regression with robust variation, using the backwards technique, in a hierarchical way by a pre-established conceptual model, in which, for the decision of the variables that constituted the model, the hierarchy between them was observed; thus, observing the characteristics of the variables, three blocks were created. Block I was composed of demographic and socio-economic variables: age, school year, self-reported skin colour and mother’s education. In block II, socio-cultural variables referring to the frequency of the father and mother’s behaviour related to weight were included. Block III comprised the variables of practices for adolescent weight control: relationship with weight, the frequency of weighing, dieting, going without eating or eating very little food, skipping meals and following a diet rich in protein and low in carbohydrates. In addition, the model was controlled with the nutritional status variable, BMI, being considered a possible confounding factor (Fig. 1).
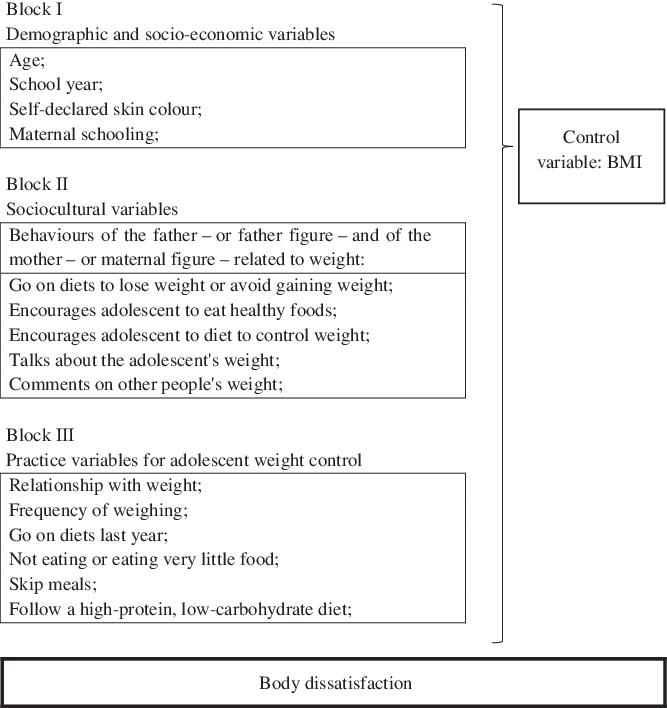
Fig. 1. Multivariate conceptual model for determining body dissatisfaction in female adolescents.
Thus, in the multivariate analysis, after the inclusion of variables that showed a significance of up to 20 % in the binary analysis, variables that reached up to 20 % of significance in the regression remained in the model, being considered possible confounding factors to follow the regression with the next block, with those that reached a significance level of 5 % (P ≤ 0·05) remaining in the final model. In addition, PR adjusted with 95 % CI was used as a measure of effect.
Ethical aspects
The recommendations established in Resolution 466/12 were fulfilled(46), obtaining approval by an Ethics in Research Committee, under opinion no. 1.379.794. Data collection was carried out only after the signing of the Free and Informed Consent Term, guaranteeing the interviewees total anonymity and the right to choose not to participate in the research or to abandon it at any time, without prejudice.
Results
The sample consisted of 685 female students from public schools in the municipality of Caxias do Sul/RS, of these 77·2 % had BD, characterised by the desire to lose weight. Most were 14 years old (47·0 %) and were in the 9th grade (51·5 %). As for skin colour, 71·1 % of the adolescents referred to themselves as white (Table 1).
Table 1. Description of demographic and socio-economic variables in relation to body dissatisfaction (BD) among adolescents/students in public schools in the city of Caxias do Sul/Rio Grande do Sul, 2016 (n 685)
(Prevalence ratios (PR) and 95 % confidence intervals)

n, Absolute frequency; n%, relative frequency; HE, higher education; HS, high school; ES, elementary school.
* χ 2 test for heterogeneity.
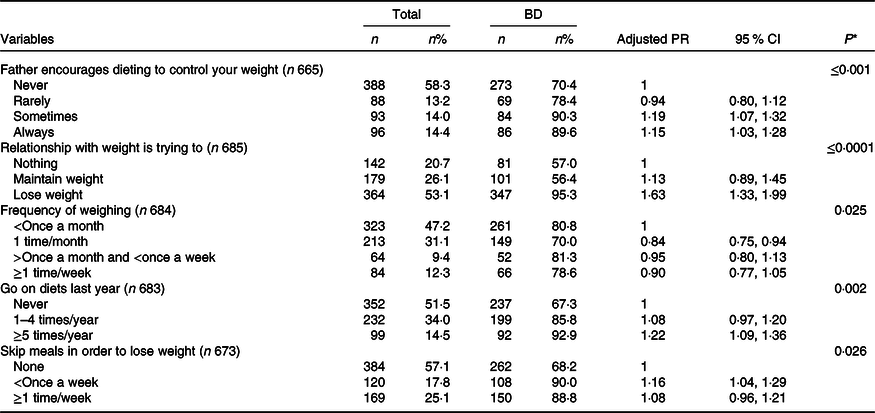
As for the father’s behaviour in relation to weight, 14·4 % reported that they were always encouraged to follow diets for weight control and 11·3 % reported that the father always talks about the adolescent’s weight (Table 2). With regard to the mother’s behaviours, 30·9 % of the students reported that sometimes the mother used diets to control and lose weight, 25·0 % said they always received an incentive to diet in order to control their weight and 23·3 % stated that the mother always talks about her daughter’s weight (Table 3). Regarding practices related to adolescent weight control, 53·1 % were trying to lose weight, 34·0 % went on a diet one to four times in the last year, 24·7 % were left without eating or ate very little food once a week or more and 25·1 % skipped meals once a week or more (Table 4).
Table 2. Description of behavioural variables related to father’s weight in relation to body dissatisfaction (BD) in adolescents/students from public schools in Caxias do Sul/Rio Grande do Sul, 2016 (n 685)
(Prevalence ratios (PR) and 95 % confidence intervals)
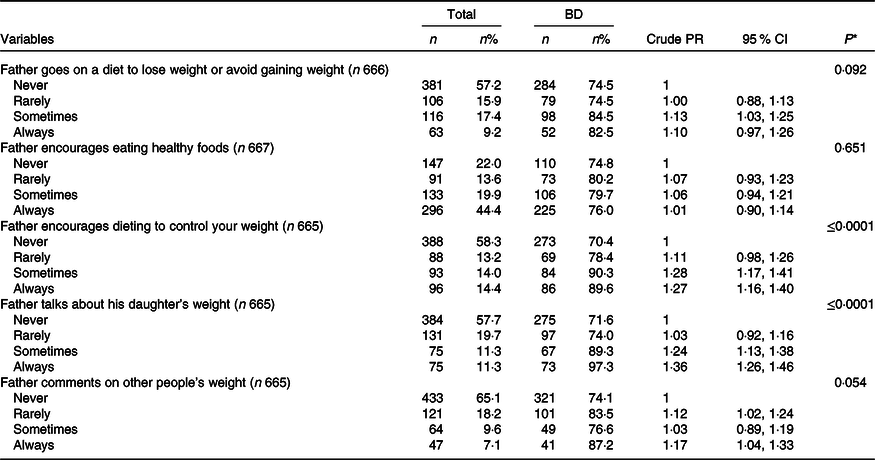
n, Absolute frequency; n%, relative frequency.
* χ 2 test for heterogeneity.
Table 3. Description of behavioural variables related to mother’s weight in relation to body dissatisfaction (BD) in adolescents/students from public schools in Caxias do Sul/Rio Grande do Sul, 2016 (n 685)
(Prevalence ratios (PR) and 95 % confidence intervals)
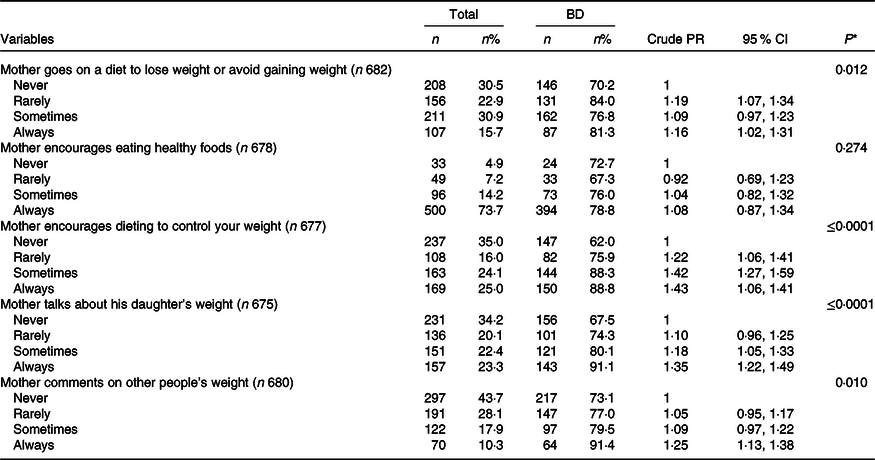
n, Absolute frequency; n%, relative frequency.
* χ 2 test for heterogeneity.
Table 4. Description of weight control practice variables in relation to body dissatisfaction (BD) in female adolescents/students from public schools in the city of Caxias do Sul/Rio Grande do Sul, 2016 (n 685)
(Prevalence ratios (PR) and 95 % confidence intervals)
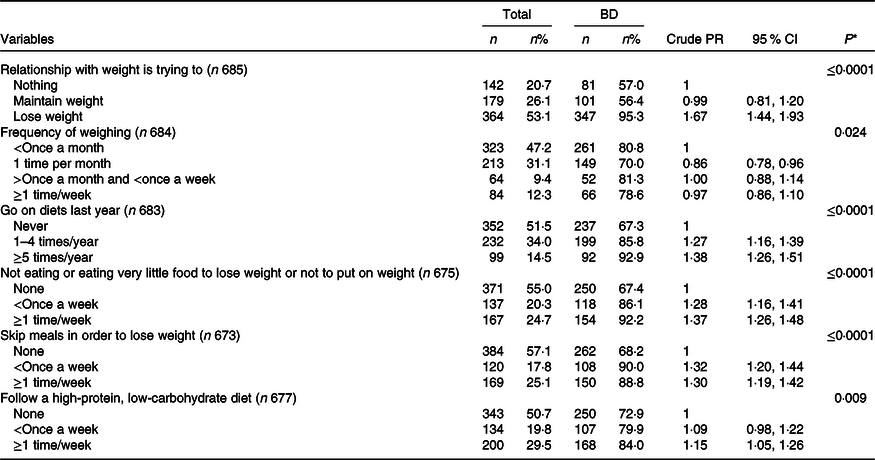
n, Absolute frequency; n%, relative frequency.
* χ 2 test for heterogeneity.
Table 5 describes data on nutritional status, showing that the majority of the sample had eutrophy (72·1 %), followed by overweight (21·9 %) and obesity (4·9 %). A positive association was identified between BD and nutritional status (P ≤ 0·0001). Compared with participants with normal weight, overweight and obese adolescents were 29·0 % (PR 1·29; 95 % CI 1·19, 1·40; P ≤ 0·0001) and 41·0 % more likely to have BD (PR 1·41; 95 % CI 1·32, 1·49; P ≤ 0·0001), respectively.
Table 5. Description of the nutritional status variable in relation to body dissatisfaction (BD) among adolescents/students in public schools in the city of Caxias do Sul/Rio Grande do Sul, 2016 (n 685)
(Prevalence ratios (PR) and 95 % confidence intervals)

n, Absolute frequency; n%, relative frequency.
* χ 2 test for heterogeneity.
Regarding the outcome, there was no significant association with demographic and socio-economic variables. However, schoolchildren aged ≥16 years had a higher prevalence of BD (88·2 %), when compared with younger ones (P = 0·083). In addition, referring to the school year (P = 0·071), adolescents in the 9th grade were identified with a high prevalence of BD (80·2 %) (Table 1). Regarding the father’s weight-related behaviours, in cases where the father encouraged her to go on a diet to control his weight sometimes (90·3 %) (P ≤ 0·0001) and talked about his daughter’s weight always (97·3 %) (P ≤ 0·0001), girls had a higher prevalence of the outcome, compared with those who reported that these behaviours never occurred (Table 2). As for the mother’s weight-related behaviours, the mother always: encouraged her daughter to go on a diet to control her weight (P ≤ 0·0001), commented on her daughter’s weight (P ≤ 0·0001) and other people’s weight (P = 0·010), and had a high prevalence of BD (88·8, 91·1 and 91·4 %, respectively) (Table 3), compared with the young women who never mentioned this.
In Table 4, regarding the practices for weight control of the schoolchildren, there is a high prevalence of the outcome in young women who were trying to lose weight (95·3 %) (P ≤ 0·0001), were on a diet five times or more per year (92·9 %) (P ≤ 0·0001) and in those who, once a week or more, did not eat or ate very little food (92·2 %) (P ≤ 0·0001) and skipped meals (88·8 %) (P ≤ 0·0001).
In the final model of the multivariate analysis, there was statistical significance with the variables: father encouraged his daughter to go on a diet in order to control weight, relationship with weight, frequency of weighing, dieting last year and skipping meals for weight control or loss. The results showed that the students whom the father encouraged to go on a diet in order to control their weight sometimes (PR 1·19; 95 % CI 1·07, 1·32; Pp ≤ 0·001) and always (PR 1·15; 95 % CI 1·03, 1·28; P ≤ 0·001) were 19·0 and 15·0 % more likely to have BD, respectively, when compared with those who reported that this never occurred. Still, trying to lose weight increased the chance of presenting the outcome by 63·0 % (PR 1·63; 95 % CI 1·33, 1·99; P ≤ 0·0001). Regarding the frequency of weighing, the adolescents who performed this practice once a month were 16·0 % less likely to have BD (PR 0·84; 95 % CI 0·75, 0·94; P = 0·025) compared with those weighing less than once a month. The use of diets to lose weight or not to gain weight, when performed five times or more in the last year, increased the probability of presenting the outcome by 22·0 % (PR 1·22; 95 % CI 1·09, 1·36; P = 0·002), compared with those who did not use this practice. Finally, skipping meals less than once a week increased the chance of having BD by 16·0 % (PR 1·16; 95 % CI 1·04, 1·29; P = 0·026) in relation to school-children who never skipped meals (Table 6).
Table 6. Description of the variables that made up the final model in the multivariate regression analysis in relation to body dissatisfaction (BD) in female adolescents/students from public schools in the city of Caxias do Sul/Rio Grande do Sul, 2016 (n 685)
(Prevalence ratios (PR) and 95 % confidence intervals)
n, Absolute frequency; n%, relative frequency.
* Final model of multivariate regression.
Discussion
The present study aimed to identify BD – constituted by the desire to lose weight – and associations with parental and personal aspects related to body shape and practices for weight control and loss in female adolescents, in which there was a high prevalence of BD represented by the desire to lose weight. Among girls, the father’s incentive to go on a diet to control his weight, as well as variables of adolescent weight control practices, such as trying to lose weight, the frequency of weighing, dieting and not eating or eating a lot little food, was associated with the outcome. It is noteworthy that at the national level, studies investigating parental aspects related to weight control and loss in relation to BD represented by the desire to lose weight were not identified.
This research found a high prevalence of BD among the schoolchildren investigated, showing the desire for weight loss and thinness. Corroborating with our findings, approximate values have been reported by international studies carried out in high-income countries in which the prevalence of BD, characterised by the desire to lose weight, in female adolescents, varies between 50·5 and 71·2 %(Reference Dion, Hains and Vachon4,Reference Dion, Blackburn and Auclair11–Reference Lawler and Nixon13) . Still, compared with the prevalence of BD identified in low-middle-income countries (26·6–61·8 %)(Reference Al Sabbah, Vereecken and Elgar47–Reference Roy, Ganguly and Roy50), there is a high prevalence of BD in the girls investigated in this study. However, when compared with the prevalence observed at national and regional level, there is a need to pay attention to BD in the investigated population. It is known that the prevalence of females at national level is high, constituted by the desire to lose weight or to have a smaller silhouette, ranging from 32·2 to 71·7 %(Reference Felden, Claumann and Sacomori5,Reference Chagas, Ferreira and Hartmann8–Reference Corseuil, Pelegrini and Beck10,Reference Leal, Philippi and Alvarenga14,Reference Petroski, Pelegrini and Glaner15,Reference Pinho, Brito and Silva51) , among which stands out the high prevalence identified in the south of the country (52·5–71·7 %)(Reference Felden, Claumann and Sacomori5,Reference Chagas, Ferreira and Hartmann8,Reference Corseuil, Pelegrini and Beck10) , reinforcing the findings of the present study.
According to the data in the literature, it is understood that BD varies from the beginning to the end of adolescence(Reference Duarte, Palombo and Solis-Cordero22); in addition, it has a positive association with age(Reference Berg and Larsson24) and, in turn, is more frequent in adolescents aged 15 years or more(Reference Dion, Blackburn and Auclair11,Reference Abdalla, Buffarini and Weber16,Reference Duarte, Palombo and Solis-Cordero22,Reference Berg and Larsson24) . BD is not only a predictor of important clinical complications, mainly psychiatric, but it is also associated with risk behaviours for eating disorders(Reference Terhoeven, Nikendei and Bärnighausen19,Reference Duarte, Palombo and Solis-Cordero22,Reference Sharpe, Griffiths and Choo52) , which have already been associated with anxiety and mood disorders, self-mutilation and increased risk of suicide(Reference Keski-Rahkonen and Mustelin25,Reference Perkins and Brausch26) , showing the importance of paying attention to the health of students in this age group, also due to the high prevalence identified in this study.
Based on the results demonstrated, the father’s incentive to go on diets to control his weight increased the likelihood of having BD. Sociocultural factors, such as parental comments about weight and incentives for weight control, are strong predictors for BD(Reference Abdalla, Buffarini and Weber16–Reference Philippi and Leme18). Corroborating our findings, according to a study carried out in Brazil(Reference Guimarães, Perez and Dunker17), in female adolescents the father’s incentive to go on a diet, aiming at weight loss, increased the chances of having BD by six times. However, the difficulty in talking to the father was also associated with BD in girls(Reference Al Sabbah, Vereecken and Elgar47). Furthermore, it has been found that the father’s incentive for his daughter to go on a diet is associated with the use of unhealthy behaviours for weight control, and although often the father has the best of intentions, this conversation can cause unintended harmful consequences for the health of adolescents(Reference Neumark-Sztainer, Bauer and Friend23). Thus, it is believed that the encouragement of the father figure to go on diets and the difficulty of talking to the father are factors associated with BD in female adolescents, highlighting the importance of the father figure.
With regard to attitudes towards weight, trying to lose weight increased the likelihood of having the outcome. It is known that weight loss attempts are significantly greater among individuals with BD(Reference Matias, Silva and Duca53,Reference Mchiza, Parker and Makoae54) , in addition to, at the age of 18 years, increasing the chances of having BD and wanting a thinner figure about two times(Reference Dion, Blackburn and Auclair11). Thus, the importance of evaluating unhealthy behaviours for control and weight loss practiced by adolescents is reinforced, as they are frequently used by young people with BD(Reference Leal, Philippi and Alvarenga14,Reference Duarte, Palombo and Solis-Cordero22) and are associated with lower chances of maintaining a healthy weight, both in adolescence and in adult life(Reference Larson, Chen and Wall55).
The frequency of weighing establishes a social comparison, which can generate concern about the appearance and intention of changing weight and, consequently, cause psychological losses such as BD(Reference Hosseini and Padhy56,Reference Kachani57) . According to a study, the most frequent body verification behaviours are positively associated with BD(Reference Stefano, Hudson and Whisenhunt58). In our findings, participants with BD demonstrated avoidance of carrying out weighing. However, in some cases, individuals with BD avoid weighing, as they start to avoid situations that can lead to body checking or generate social comparisons(Reference Kachani57). In addition, it can be concluded that the avoidance of body verification, identified through the frequency of weighing, possibly occurred due to the non-verification of other methods of body verification, knowing that obsession with verification often occurs in certain parts of the body(Reference Kachani57,Reference Cheah, Hazmi and Chang59) .
Observing the results regarding the practice of dieting last year, a positive association with BD was identified. Strengthening our findings, according to data in the literature, the practice of dieting to lose weight – including dietary restrictions – is often associated with obsession with thinness and BD(Reference Terhoeven, Nikendei and Bärnighausen19,Reference Contreras, Morán and Frez60) . Thus, individuals with BD are more likely to follow diets for weight control(Reference Sharpe, Griffiths and Choo52), which tends to increase throughout adolescence(Reference Berg and Larsson24). In addition, it is known that a considerable proportion of adolescents adopt a diet with restricted food considered to be at risk(Reference Contreras, Morán and Frez60), which, together with BD, has negative consequences for the adolescent’s health(Reference Berg and Larsson24). Still, unhealthy eating behaviours for weight loss are often identified in young people with BD(Reference Frank, Claumann and Felden29,Reference Tebar, Gil and Scarabottolo61) , demonstrating a preference for energetic restriction and not for the nutritional quality of the diet(Reference Frank, Claumann and Felden29), reinforcing the need to study and address this issue with female students.
Regarding unhealthy eating behaviours for weight loss, analysing the results observed in this study, it was identified that the practice of skipping meals in order to lose weight sometimes increased the probability of presenting BD. According to a study, adolescents with BD were more likely to perform unhealthy behaviours for weight control, such as skipping meals(Reference Leal, Philippi and Alvarenga14), which is common among girls(Reference Dion, Blackburn and Auclair11,Reference Leal, Philippi and Alvarenga14) . Goals incompatible with current weight are considered a strong predictor of unhealthy weight management behaviours in adolescents with BD(Reference Roy and Gauvin62). Thus, it is possible that BD is a risk factor for the appearance of unhealthy eating behaviours in the young women investigated.
As limitations of this research, the reverse causality bias stands out, as it is a cross-sectional study. The monitoring of these students would be interesting, in order to identify the long-term consequences of dietary factors and practices. As for self-reported data on weight and height for calculating BMI, it is important to note that, although the use of self-reported data is validated for adolescents(Reference Allison, Colby and Opoku-Acheampong34–Reference Strauss40), studies reported that there may be an under-report between girls(Reference Marangoni, Machado and Passos39) and overweight and obese individuals(Reference Allison, Colby and Opoku-Acheampong34,Reference Marangoni, Machado and Passos39) , which may have influenced the results. Still, a possible memory bias is also being considered, due to the long questionnaire, which may have confused students, in addition to the homogeneity of the sample, which is composed only of students from the public school system. However, studies at national and regional levels that analyse and discuss family and personal aspects of weight loss and control in female students are limited.
However, as potentials of this research, the sampling process and the scope of included public schools are highlighted, in addition to the data collected, consisting of a wide and diversified amount of relevant information. The care and control with data manipulation is evidenced, minimising typing errors, as well as the training of all research participants who worked on data collection, increasing the veracity of the information and results presented in this study. It is noteworthy that, at the national level, no studies were identified that investigated BD constituted by the desire to lose weight and the relationship with parental aspects for weight control and loss. Positively, in addition to presenting the prevalence of BD, represented by the desire to lose weight, characterising adolescents in public schools in the city, this study presents the family and personal aspects for control and weight loss associated with the outcome, individually evaluating the effects of the father and the mother, which can be used for the development of strategies aimed at the health of this population.
Thus, the high prevalence of BD, together with the associated factors verified in this study, reinforces the need for strategies to identify this condition early, enabling the appropriate treatment and prevention of health complications, such as eating disorders and nutritional deficit.
Acknowledgements
R. S. D’O. had a CAPES (“Coordenação de Aperfeiçoamento de Pessoal de Nível Superior”) master’s degree grant. The authors are grateful to the study participants, the “Prefeitura Municipal de Caxias do Sul, Brasil” and all school members involved during during data collection.
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
T. D. and R. L. H. contributed substantially to the conception, design and acquisition of data. R. S. D., C. C., E. C. and M. L. O. G. participated in the study design, data analysis, interpretation of results, preparation, writing and final review of the article. All authors participated in the formulation of the research question, carried out a critical evaluation of the article and the content, approved the final version and agreed on responsibility for all aspects of the work.
The authors declare that there are no conflicts of interest.







