Mental Health and Quality of Life of Women One Year after Maternal Near-Miss in Low and Middle-Income Countries: The Case of Zanzibar, Tanzania

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
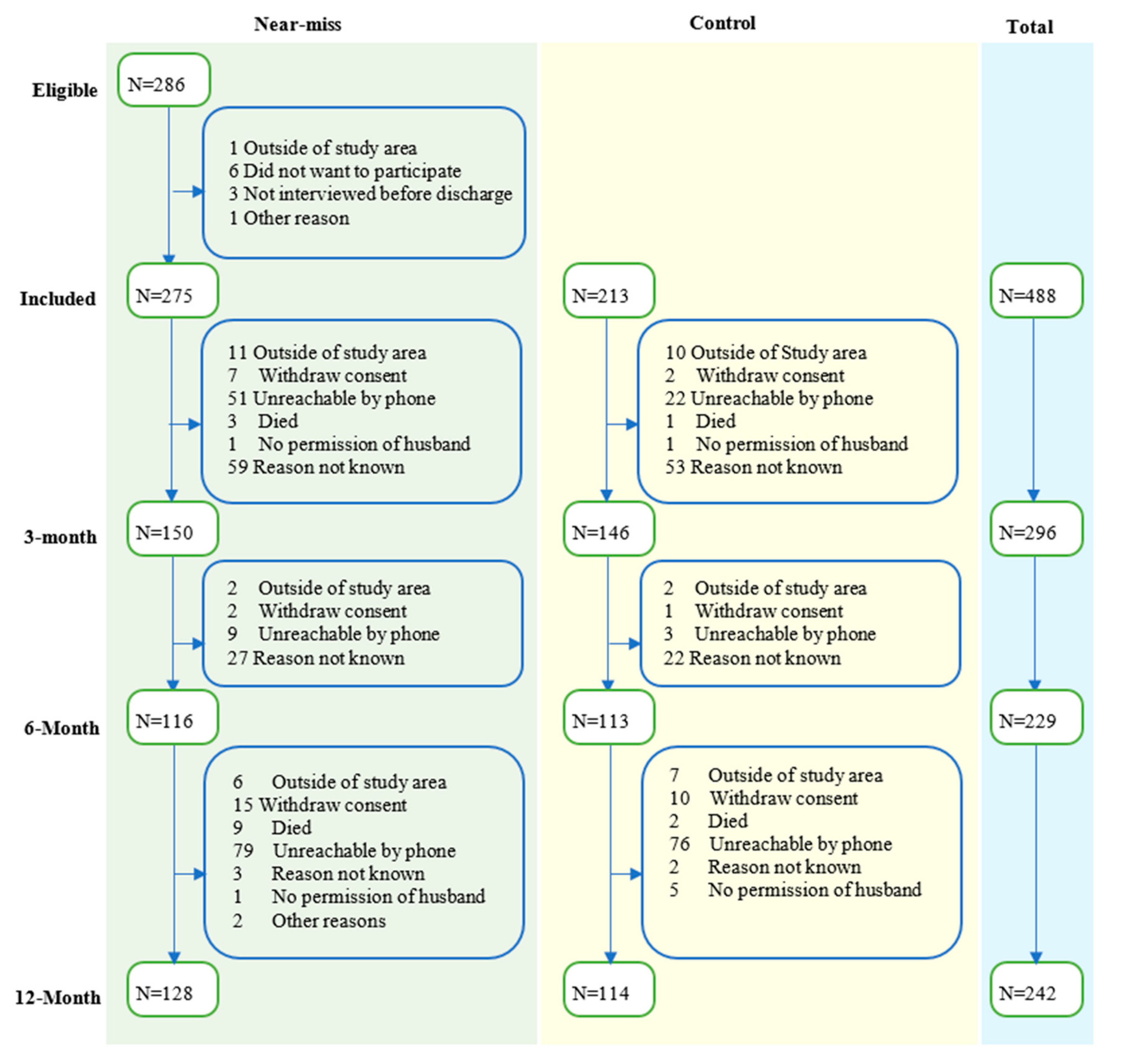
2.1. Study Design, Data Sources, and Population
2.2. Outcome Variables
2.3. Risk Factors
2.4. Missing Data
2.5. Statistical Analysis
2.6. Medical Ethical Considerations
3. Results
3.1. Mental Health Problems and QoL over Time
3.2. Association of Risk Factors with Mental Health Problems and QoL
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Geller, S.E.; Koch, A.R.; Garland, C.E.; MacDonald, E.J.; Storey, F.; Lawton, B. A global view of severe maternal morbidity: Moving beyond maternal mortality. Reprod. Health 2018, 15, 98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prual, A.; Bouvier-Colle, M.H.; de Bernis, L.; Breart, G. Severe maternal morbidity from direct obstetric causes in West Africa: Incidence and case fatality rates. Bull. World Health Organ. 2000, 78, 593–602. [Google Scholar] [PubMed]
- Norhayati, M.N.; Surianti, S.; Nik Hazlina, N.H. Metasynthesis: Experiences of Women with Severe Maternal Morbidity and Their Perception of the Quality of Health Care. PLoS ONE 2015, 10, e0130452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tunçalp, Ö.; Hindin, M.J.; Adu-Bonsaffoh, K.; Adanu, R. Listening to Women’s Voices: The Quality of Care of Women Experiencing Severe Maternal Morbidity, in Accra, Ghana. PLoS ONE 2012, 7, e44536. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Furuta, M.; Sandall, J.; Cooper, D.; Bick, D. The relationship between severe maternal morbidity and psychological health symptoms at 6–8 weeks postpartum: A prospective cohort study in one English maternity unit. BMC Pregnancy Childbirth 2014, 14, 133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Angelini, C.R.; Pacagnella, R.C.; Parpinelli, M.A.; Silveira, C.; Andreucci, C.B.; Ferreira, E.C.; Santos, J.P.; Zanardi, D.M.; Souza, R.T.; Cecatti, J.G. Post-Traumatic Stress Disorder and severe maternal morbidity: Is there an association? Clinics (Sao Paulo) 2018, 73, e309. [Google Scholar] [CrossRef] [PubMed]
- Assarag, B.; Dujardin, B.; Essolbi, A.; Cherkaoui, I.; De Brouwere, V. Consequences of severe obstetric complications on women‘s health in Morocco: Please, listen to me! Trop. Med. Int. Health TM IH 2015, 20, 1406–1414. [Google Scholar] [CrossRef] [Green Version]
- Filippi, V.; Goufodji, S.; Sismanidis, C.; Kanhonou, L.; Fottrell, E.; Ronsmans, C.; Alihonou, E.; Patel, V. Effects of severe obstetric complications on women’s health and infant mortality in Benin. Trop. Med. Int. Health 2010, 15, 733–742. [Google Scholar] [CrossRef] [Green Version]
- Filippi, V.; Ganaba, R.; Baggaley, R.F.; Marshall, T.; Storeng, K.T.; Sombié, I.; Ouattara, F.; Ouedraogo, T.; Akoum, M.; Meda, N.J.T.L. Health of women after severe obstetric complications in Burkina Faso: A longitudinal study. Lancet 2007, 370, 1329–1337. [Google Scholar] [CrossRef]
- Norhayati, M.N.; Nik Hazlina, N.H.; Aniza, A.A.; Asrenee, A.R. Severe Maternal Morbidity and Postpartum Depressive Symptomatology: A Prospective Double Cohort Comparison Study. Res. Nurs. Health 2016, 39, 415–425. [Google Scholar] [CrossRef]
- Adewuya, A.O.; Ologun, Y.A.; Ibigbami, O.S. Post-traumatic stress disorder after childbirth in Nigerian women: Prevalence and risk factors. BJOG Int. J. Obstet. Gynaecol. 2006, 113, 284–288. [Google Scholar] [CrossRef] [PubMed]
- Soma-Pillay, P.; Makin, J.D.; Pattinson, R.C. Quality of life 1 year after a maternal near-miss event. Int. J. Gynaecol. Obstet. Off. Organ Int. Fed. Gynaecol. Obstet. 2018, 141, 133–138. [Google Scholar] [CrossRef] [PubMed]
- Angelini, C.R.; Pacagnella, R.C.; Parpinelli, M.A.; Silveira, C.; Andreucci, C.B.; Ferreira, E.C.; Santos, J.P.; Zanardi, D.M.; Souza, R.T.; Sousa, M.H.; et al. Quality of Life after an Episode of Severe Maternal Morbidity: Evidence from a Cohort Study in Brazil. BioMed Res. Int. 2018, 2018, 9348647. [Google Scholar] [CrossRef] [PubMed]
- Herklots, T.; van Acht, L.; Khamis, R.S.; Meguid, T.; Franx, A.; Jacod, B. Validity of WHO’s near-miss approach in a high maternal mortality setting. PLoS ONE 2019, 14, e0217135. [Google Scholar] [CrossRef] [Green Version]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Smith Fawzi, M.C.; Ngakongwa, F.; Liu, Y.; Rutayuga, T.; Siril, H.; Somba, M.; Kaaya, S.F. Validating the Patient Health Questionnaire-9 (PHQ-9) for screening of depression in Tanzania. Neurol. Psychiatry Brain Res. 2019, 31, 9–14. [Google Scholar] [CrossRef]
- Mollica, R.F.; Caspi-Yavin, Y.; Bollini, P.; Truong, T.; Tor, S.; Lavelle, J. The Harvard Trauma Questionnaire. Validating a cross-cultural instrument for measuring torture, trauma, and posttraumatic stress disorder in Indochinese refugees. J. Nerv. Ment. Dis. 1992, 180, 111–116. [Google Scholar] [CrossRef]
- de Fouchier, C.; Blanchet, A.; Hopkins, W.; Bui, E.; Ait-Aoudia, M.; Jehel, L. Validation of a French adaptation of the Harvard Trauma Questionnaire among torture survivors from sub-Saharan African countries. Eur. J. Psychotraumatol. 2012, 3, 19225. [Google Scholar] [CrossRef]
- Housen, T.; Lenglet, A.; Ariti, C.; Ara, S.; Shah, S.; Dar, M.; Hussain, A.; Paul, A.; Wagay, Z.; Viney, K.; et al. Validation of mental health screening instruments in the Kashmir Valley, India. Transcult Psychiatry 2018, 55, 361–383. [Google Scholar] [CrossRef]
- The WHOQOL Group. Development of the World Health Organization WHOQOL-BREF quality of life assessment. Psychol. Med. 1998, 28, 551–558. [Google Scholar] [CrossRef] [Green Version]
- The World Bank, D.W. Questionnaire Translation. Available online: https://dimewiki.worldbank.org/wiki/Questionnaire_Translation (accessed on 23 October 2020).
- World Health Organization. Programme on Mental Health: WHOQOL User Manual, 2012 Revision; World Health Organization: Geneva, Switzerland, 1998. [Google Scholar]
- Twisk, J.; de Boer, M.; de Vente, W.; Heymans, M. Multiple imputation of missing values was not necessary before performing a longitudinal mixed-model analysis. J. Clin. Epidemiol. 2013, 66, 1022–1028. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing; R Core Team: Vienna, Austria, 2013. [Google Scholar]
- World Health Organization. Depression and Other Common Mental Disorders: Global Health Estimates; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Monteiro, N. Addressing mental illness in Africa: Global health challenges and local opportunities. Community Psychol. Glob. Perspect. 2015, 1, 78–95. [Google Scholar] [CrossRef]
- Schwartz, C.E.; Sprangers, M.A.G. Response Shift. In Encyclopedia of Quality of Life and Well-Being Research; Michalos, A.C., Ed.; Springer: Dordrecht, The Netherlands, 2014; pp. 5542–5547. [Google Scholar] [CrossRef]
- Wang, H.H.; Wu, S.Z.; Liu, Y.Y. Association between social support and health outcomes: A meta-analysis. Kaohsiung J. Med. Sci. 2003, 19, 345–351. [Google Scholar] [CrossRef] [Green Version]
- Helgeson, V.S. Social support and quality of life. Qual. Life Res. Int. J. Qual. Life Asp. Treat. Care Rehabil. 2003, 12 (Suppl. 1), 25–31. [Google Scholar] [CrossRef]
- Herklots, T.; Van Acht, L.; Meguid, T.; Franx, A.; Jacod, B. Severe maternal morbidity in Zanzibar’s referral hospital: Measuring the impact of in-hospital care. PLoS ONE 2017, 12, e0181470. [Google Scholar] [CrossRef]
- Kristiansen, M.; Sheikh, A. Understanding faith considerations when caring for bereaved Muslims. J. R. Soc. Med. 2012, 105, 513–517. [Google Scholar] [CrossRef] [Green Version]
- Flaherty, J.A.; Gaviria, F.M.; Pathak, D.; Mitchell, T.; Wintrob, R.; Richman, J.A.; Birz, S. Developing Instruments for Cross-Cultural Psychiatric Research. J. Nerv. Ment. Dis. 1988, 176, 260–263. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Category | MNM (N = 275) | Control (N = 213) | Total (N = 488) | p-Value § |
|---|---|---|---|---|---|
| Age | Mean (SD) | 29.1 (6.0) | 28.3 (5.6) | 28.8 (5.9) | 0.080 |
| Marital Status | Married | 201 (91.0) | 184 (92.9) | 385 (91.9) | 0.459 |
| Unmarried | 20 (9.0) | 14 (7.1) | 34 (8.1) | ||
| Residence | Rural | 32 (29.9) | 23 (34.3) | 55 (31.6) | 0.476 |
| Urban | 33 (30.8) | 15 (22.4) | 48 (27.6) | ||
| Mixed | 42 (39.3) | 29 (43.3) | 71 (40.8) | ||
| Education | Primary or less | 90 (42.1) | 57 (29.2) | 147 (35.9) | 0.007 * |
| Secondary or more | 124 (57.9) | 138 (70.8) | 262 (64.1) | ||
| Employment | Employed | 30 (13.9) | 34 (17.3) | 64 (15.5) | 0.269 |
| Housewife | 121 (56.0) | 98 (49.7) | 219 (53.0) | ||
| Self-employed | 58 (26.9) | 52 (26.4) | 110 (26.6) | ||
| Others † | 7 (3.2) | 13 (6.6) | 20 (4.8) | ||
| Perceived Wealth | Average | 160 (76.2) | 168 (88.4) | 328 (82.0) | 0.001 * |
| Below average | 50 (23.8) | 22 (11.6) | 72 (18.0) | ||
| Gestational age | First trimester | 17 (9.4) | 19 (13.5) | 36 (11.2) | 0.272 |
| Second trimester | 12 (6.7) | 5 (3.5) | 17 (5.3) | ||
| Third trimester | 151 (83.9) | 117 (83.0) | 268 (83.5) | ||
| Mode of termination of pregnancy | Vaginal delivery | 74 (28.1) | 60 (28.8) | 134 (28.4) | 0.827 |
| Cesarean section | 146 (56.1) | 116 (55.8) | 262 (55.4) | ||
| Early pregnancy loss | 37 (14.1) | 25 (12.0) | 62 (13.2) | ||
| Still pregnant at discharge | 7 (2.7) | 7 (3.4) | 14 (3.0) | ||
| Parity | 1 | 100 (38.6) | 113 (53.3) | 213 (45.2) | 0.002 * |
| 2–4 | 105 (40.5) | 74 (34.9) | 179 (38.0) | ||
| >4 | 54 (20.8) | 25 (11.8) | 79 (16.8) | ||
| History of cesarean section | Yes | 40 (27.8) | 18 (19.6) | 58 (24.6) | 0.153 |
| No | 104 (72.2) | 74 (80.4) | 178 (75.4) | ||
| Pregnancy outcome | Livebirth | 73 (42.9) | 125 (74.0) | 198 (58.4) | <0.001 * |
| Early pregnancy loss | 26 (15.3) | 21 (12.4) | 47 (13.9) | ||
| Perinatal loss | 71 (41.8) | 23 (13.6) | 94 (27.7) |
| 3 Months | 6 Months | 12 Months | Total | ||||
|---|---|---|---|---|---|---|---|
| MNM | Controls | MNM | Controls | MNM | Controls | ||
| Mental Health-Median (IQR) | |||||||
| PHQ-9 Score | 1.0 (0.0–3.0) | 1.0 (0.0–2.0) | 1.0 (0.0–2.0) | 1.0 (0.0–2.0) | 1.0 (0.0–3.0) | 1.0 (0.0–2.0) | 1.0 (0.0–2.0) |
| HTQ Score | 1.0 (1.0–1.1) | 1.0 (1.0–1.1) | 1.0 (1.0–1.1) | 1.0 (1.0–1.1) | 1.0 (1.0–1.1) | 1.0 (1.0–1.1) | 1.0 (1.0–1.1) |
| WHOQOL-BREEF Domain Scores-Median (IQR) | |||||||
| Physical | 85.7 (71.4–96.4) | 89.3 (78.6–100.0) | 92.9 (78.6–96.4) | 92.9 (78.6–100.0) | 92.9 (89.3–100.0) | 96.4 (89.3–100.0) | 92.9 (82.1–100.0) |
| Psychological | 95.8 (79.2–100.0) | 95.8 (79.2–100.0) | 95.8 (91.7–100.0) | 100.0 (83.3–100.0) | 100.0 (95.8–100.0) | 100.0 (95.8–100.0) | 100.0 (91.7–100.0) |
| Social | 75.0 (58.3–100.0) | 83.3 (58.3–100.0) | 100.0 (75.0–100.0) | 100.0 (58.3–100.0) | 100.0 (91.7–100.0) | 100.0 (93.8–100.0) | 100.0 (66.7–100.0) |
| Environmental | 87.5 (75.8–93.8) | 87.5 (75.0–93.8) | 90.6 (84.4–93.8) | 90.6 (78.1–93.8) | 93.8 (87.5–93.8) | 93.8 (90.6–96.9) | 90.6 (84.4–93.8) |
| Variable | EXP (Estimate) | 95% CI | p-Value | |
|---|---|---|---|---|
| Lower | Upper | |||
| Intercept | 5.03 | 2.67 | 9.49 | 0.000 |
| Time after discharge from hospital | 1.00 | 0.96 | 1.03 | 0.888 |
| MNM status × time after discharge | 1.01 | 0.96 | 1.06 | 0.705 |
| MNM status (near-miss women) | 1.05 | 0.79 | 1.38 | 0.750 |
| Pregnancy outcome (Early pregnancy loss) | 0.91 | 0.66 | 1.26 | 0.582 |
| Pregnancy outcome (Perinatal loss) | 1.30 | 1.01 | 1.67 | 0.041 |
| Intercurrent illness of mother (yes) | 1.42 | 1.15 | 1.75 | 0.001 |
| Social support scale | 0.95 | 0.93 | 0.97 | 0.000 |
| Negative Binomial | Zero-Inflated | |||||||
|---|---|---|---|---|---|---|---|---|
| EXP (Estimate) | 95% CI | p-Value | EXP (Estimate) | 95% CI | p-Value | |||
| Lower | Upper | Lower | Upper | |||||
| Physical Domain of Quality of Life | ||||||||
| (Intercept) | 77..89 | 45.18 | 134.30 | 0.000 | 0.00 | 0.00 | 0.01 | 0.000 |
| Time after discharge from hospital | 1.00 | 0.98 | 1.03 | 0.888 | 1.01 | 0.95 | 1.09 | 0.696 |
| MNM status (near-miss women) | 1.21 | 1.01 | 1.45 | 0.038 | 0.62 | 0.34 | 1.11 | 0.107 |
| MNM status ×time after discharge | 0.95 | 0.92 | 0.99 | 0.007 | 1.00 | 0.90 | 1.10 | 0.955 |
| Intercurrent illness of mother (yes) | 1.11 | 0.96 | 1.29 | 0.152 | 0.41 | 0.24 | 0.70 | 0.001 |
| Social support scale | 0.93 | 0.92 | 0.95 | 0.000 | 1.31 | 1.16 | 1.48 | 0.000 |
| Mode of delivery (Early pregnancy loss) | 1.01 | 0.82 | 1.25 | 0.892 | 1.39 | 0.73 | 2.67 | 0.317 |
| Mode of delivery (Cesarean section) | 0.89 | 0.76 | 1.03 | 0.120 | 1.96 | 1.21 | 3.19 | 0.006 |
| Age of the women | 1.01 | 1.00 | 1.03 | 0.029 | 0.96 | 0.93 | 1.00 | 0.063 |
| Psychological Domain of Quality of Life | ||||||||
| (Intercept) | 93.06 | 26.52 | 326.55 | 0.000 | 0.00 | 0.00 | 0.07 | 0.003 |
| Time after discharge from hospital | 1.00 | 0.92 | 1.08 | 0.978 | 0.93 | 0.80 | 1.08 | 0.339 |
| MNM status (near-miss women) | 1.42 | 0.80 | 2.51 | 0.228 | 0.58 | 0.21 | 1.62 | 0.301 |
| MNM status × time after discharge | 0.93 | 0.85 | 1.03 | 0.179 | 1.11 | 0.93 | 1.33 | 0.243 |
| Intercurrent illness of mother (yes) | 1.00 | 0.65 | 1.52 | 0.987 | 0.62 | 0.30 | 1.28 | 0.196 |
| History of C-Section (Only one) | 1.09 | 0.70 | 1.69 | 0.711 | 0.35 | 0.15 | 0.84 | 0.018 |
| History of C-Section (two or more) | 0.83 | 0.38 | 1.82 | 0.647 | 0.87 | 0.22 | 3.36 | 0.834 |
| Social support scale | 0.93 | 0.90 | 0.97 | 0.001 | 1.34 | 1.13 | 1.59 | 0.001 |
| Residence (Mixed) | 0.64 | 0.40 | 1.01 | 0.053 | 1.33 | 0.59 | 2.97 | 0.493 |
| Residence (Rural) | 0.84 | 0.55 | 1.29 | 0.423 | 0.69 | 0.30 | 1.59 | 0.390 |
| Employment (Housewife) | 1.05 | 0.64 | 1.73 | 0.841 | 1.67 | 0.67 | 4.13 | 0.269 |
| Employment (Self-employed) | 1.20 | 0.70 | 2.09 | 0.507 | 1.16 | 0.41 | 3.29 | 0.778 |
| Employment (Unemployed) d | 3.86 | 1.34 | 11.15 | 0.013 | 2.20 | 0.40 | 12.15 | 0.365 |
| Social Domain of Quality of Life | ||||||||
| (Intercept) | 66.71 | 49.82 | 89.31 | 0.000 | 0.00 | 0.00 | 0.01 | 0.000 |
| Time after discharge from hospital | 0.99 | 0.97 | 1.02 | 0.464 | 1.12 | 1.04 | 1.20 | 0.002 |
| MNM status (near-miss women) | 1.02 | 0.88 | 1.18 | 0.833 | 0.75 | 0.45 | 1.26 | 0.280 |
| MNM status × time after discharge | 0.98 | 0.95 | 1.01 | 0.180 | 0.98 | 0.89 | 1.08 | 0.689 |
| Pregnancy outcome (Early pregnancy loss) | 0.88 | 0.74 | 1.03 | 0.113 | 1.24 | 0.72 | 2.15 | 0.438 |
| Pregnancy outcome (Perinatal loss) | 1.00 | 0.87 | 1.15 | 0.991 | 1.62 | 1.03 | 2.54 | 0.035 |
| Education (Secondary or more) | 0.92 | 0.82 | 1.03 | 0.152 | 1.39 | 0.94 | 2.06 | 0.096 |
| Social support scale | 0.98 | 0.97 | 0.99 | 0.000 | 1.21 | 1.14 | 1.29 | 0.000 |
| Environmental Domain of Quality of Life | ||||||||
| (Intercept) | 229.64 | 166.83 | 316.10 | 0.000 | 0.00 | 0.00 | 0.02 | 0.001 |
| Time after discharge from hospital | 0.97 | 0.95 | 0.99 | 0.001 | 1.03 | 0.94 | 1.14 | 0.482 |
| MNM status (near-miss women) | 1.02 | 0.90 | 1.17 | 0.737 | 0.92 | 0.41 | 2.11 | 0.851 |
| MNM status × time after discharge | 1.01 | 0.99 | 1.03 | 0.432 | 0.87 | 0.74 | 1.02 | 0.085 |
| Intercurrent illness of mother (yes) | 1.17 | 1.05 | 1.30 | 0.004 | 0.60 | 0.27 | 1.32 | 0.205 |
| Social support scale | 0.91 | 0.90 | 0.92 | 0.000 | 1.24 | 1.04 | 1.47 | 0.014 |
| Education (Secondary or more) | 0.94 | 0.84 | 1.04 | 0.216 | 2.36 | 1.12 | 5.00 | 0.024 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alemu, S.; Herklots, T.; Almansa, J.; Mbarouk, S.; Sulkers, E.; Stekelenburg, J.; de Zeeuw, J.; Jacod, B.; Biesma, R. Mental Health and Quality of Life of Women One Year after Maternal Near-Miss in Low and Middle-Income Countries: The Case of Zanzibar, Tanzania. Int. J. Environ. Res. Public Health 2020, 17, 9034. https://doi.org/10.3390/ijerph17239034
Alemu S, Herklots T, Almansa J, Mbarouk S, Sulkers E, Stekelenburg J, de Zeeuw J, Jacod B, Biesma R. Mental Health and Quality of Life of Women One Year after Maternal Near-Miss in Low and Middle-Income Countries: The Case of Zanzibar, Tanzania. International Journal of Environmental Research and Public Health. 2020; 17(23):9034. https://doi.org/10.3390/ijerph17239034
Chicago/Turabian StyleAlemu, Sisay, Tanneke Herklots, Josue Almansa, Shadya Mbarouk, Esther Sulkers, Jelle Stekelenburg, Janine de Zeeuw, Benoit Jacod, and Regien Biesma. 2020. "Mental Health and Quality of Life of Women One Year after Maternal Near-Miss in Low and Middle-Income Countries: The Case of Zanzibar, Tanzania" International Journal of Environmental Research and Public Health 17, no. 23: 9034. https://doi.org/10.3390/ijerph17239034