Consumption of a Beverage Containing Aspartame and Acesulfame K for Two Weeks Does Not Adversely Influence Glucose Metabolism in Adult Males and Females: A Randomized Crossover Study



Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Approval and Registration
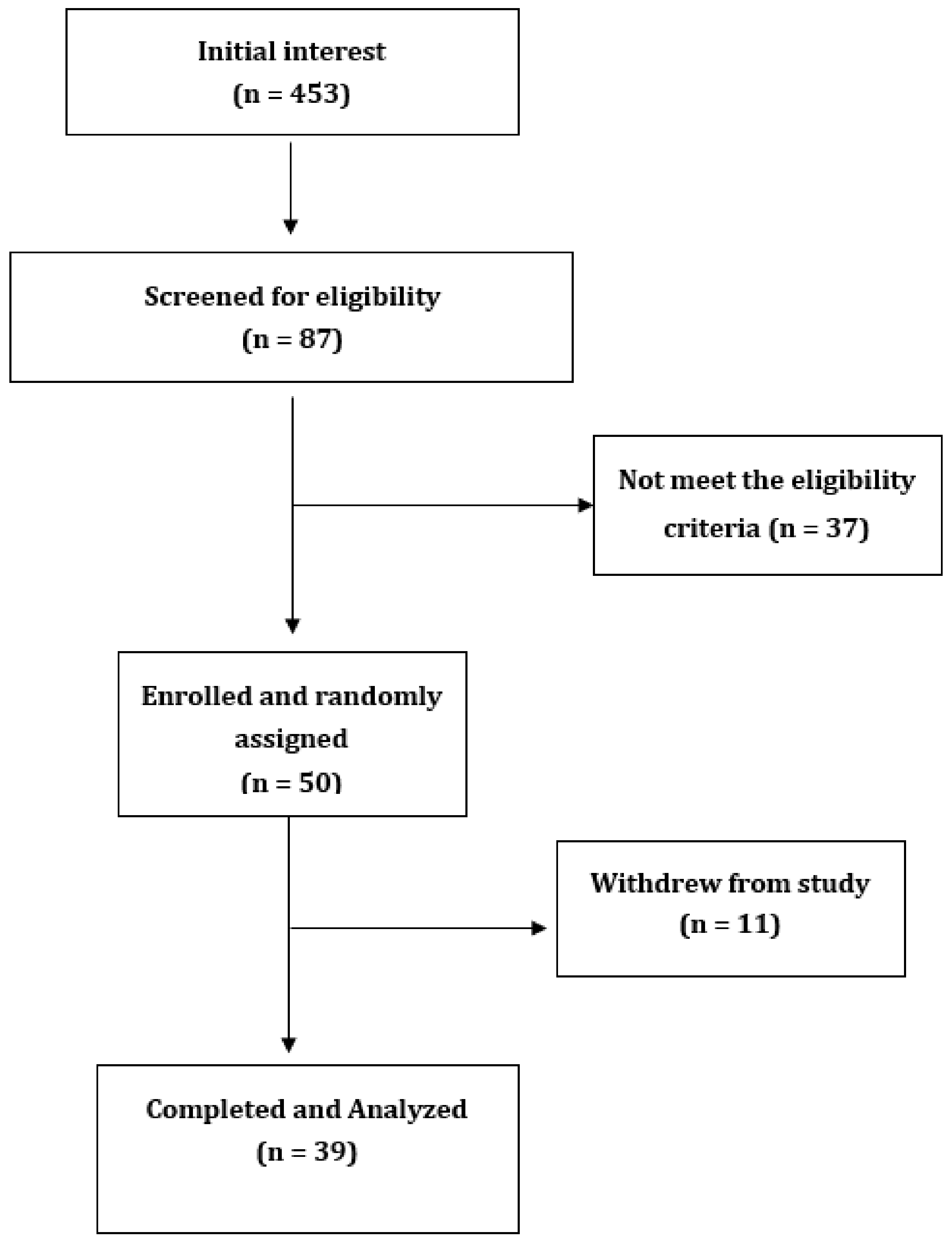
2.2. Study Participants
2.3. Study Design
2.4. Measurements during Intervention
2.5. Glucose Monitoring during Intervention
2.6. Statistical Analysis
3. Results
3.1. Participant Characteristics
3.2. Fasting Glucose, Fasting Insulin, and Area under Curve for Glucose and Insulin
3.3. Continuous Glucose Concentrations over 2 Weeks
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Saeedi, P.; Petersohn, I.; Salpea, P.; Malanda, B.; Karuranga, S.; Unwin, N.; Colagiuri, S.; Guariguata, L.; Motala, A.A.; Ogurtsova, K.; et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the international diabetes federation diabetes atlas, 9(th) edition. Diabetes Res. Clin. Pract. 2019, 157, 107843. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sylvetsky, A.C.; Rother, K.I. Trends in the consumption of low-calorie sweeteners. Physiol. Behav. 2016, 164, 446–450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piernas, C.; Ng, S.W.; Popkin, B. Trends in purchases and intake of foods and beverages containing caloric and low-calorie sweeteners over the last decade in the United States. Pediatric Obes. 2013, 8, 294–306. [Google Scholar] [CrossRef] [Green Version]
- Sylvetsky, A.C.; Welsh, J.A.; Brown, R.J.; Vos, M.B. Low-calorie sweetener consumption is increasing in the United States. Am. J. Clin. Nutr. 2012, 96, 640–646. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sylvetsky, A.C.; Jin, Y.; Clark, E.J.; Welsh, J.A.; Rother, K.I.; Talegawkar, S.A. Consumption of low-calorie sweeteners among children and adults in the United States. J. Acad. Nutr. Diet. 2017, 117, 441–448.e442. [Google Scholar] [CrossRef] [PubMed]
- Azad, M.B.; Abou-Setta, A.M.; Chauhan, B.F.; Rabbani, R.; Lys, J.; Copstein, L.; Mann, A.; Jeyaraman, M.M.; Reid, A.E.; Fiander, M.; et al. Nonnutritive sweeteners and cardiometabolic health: A systematic review and meta-analysis of randomized controlled trials and prospective cohort studies. CMAJ Can. Med. Assoc. J. 2017, 189, E929–E939. [Google Scholar] [CrossRef] [Green Version]
- Greenwood, D.C.; Threapleton, D.E.; Evans, C.E.; Cleghorn, C.L.; Nykjaer, C.; Woodhead, C.; Burley, V.J. Association between sugar-sweetened and artificially sweetened soft drinks and type 2 diabetes: Systematic review and dose-response meta-analysis of prospective studies. Br. J. Nutr. 2014, 112, 725–734. [Google Scholar] [CrossRef]
- Imamura, F.; O’Connor, L.; Ye, Z.; Mursu, J.; Hayashino, Y.; Bhupathiraju, S.N.; Forouhi, N.G. Consumption of sugar sweetened beverages, artificially sweetened beverages, and fruit juice and incidence of type 2 diabetes: Systematic review, meta-analysis, and estimation of population attributable fraction. BMJ 2015, 351, h3576. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.; Keogh, J.B.; Clifton, P.M. Non-nutritive sweeteners and glycaemic control. Curr. Atheroscler. Rep. 2019, 21, 49. [Google Scholar] [CrossRef]
- Nettleton, J.A.; Lutsey, P.L.; Wang, Y.; Lima, J.A.; Michos, E.D.; Jacobs, D.R., Jr. Diet soda intake and risk of incident metabolic syndrome and type 2 diabetes in the Multi-Ethnic Study of Atherosclerosis (MESA). Diabetes Care 2009, 32, 688–694. [Google Scholar] [CrossRef] [Green Version]
- Duffey, K.J.; Steffen, L.M.; van Horn, L.; Jacobs, D.R., Jr.; Popkin, B.M. Dietary patterns matter: Diet beverages and cardiometabolic risks in the longitudinal Coronary Artery Risk Development in Young Adults (CARDIA) Study. Am. J. Clin. Nutr. 2012, 95, 909–915. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lutsey, P.L.; Steffen, L.M.; Stevens, J. Dietary intake and the development of the metabolic syndrome: The atherosclerosis risk in communities study. Circulation 2008, 117, 754–761. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fowler, S.P.; Williams, K.; Resendez, R.G.; Hunt, K.J.; Hazuda, H.P.; Stern, M.P. Fueling the obesity epidemic? Artificially sweetened beverage use and long-term weight gain. Obes. Silver Spring Md. 2008, 16, 1894–1900. [Google Scholar] [CrossRef] [PubMed]
- Fowler, S.P.; Williams, K.; Hazuda, H.P. Diet soda intake is associated with long-term increases in waist circumference in a biethnic cohort of older adults: The San Antonio Longitudinal Study of Aging. J. Am. Geriatr. Soc. 2015, 63, 708–715. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moran, A.W.; Al-Rammahi, M.A.; Arora, D.K.; Batchelor, D.J.; Coulter, E.A.; Daly, K.; Ionescu, C.; Bravo, D.; Shirazi-Beechey, S.P. Expression of Na + /glucose co-transporter 1 (SGLT1) is enhanced by supplementation of the diet of weaning piglets with artificial sweeteners. Br. J. Nutr. 2010, 104, 637–646. [Google Scholar] [CrossRef] [Green Version]
- Meyer-Gerspach, A.C.; Wolnerhanssen, B.; Beglinger, C. Functional roles of low calorie sweeteners on gut function. Physiol. Behav. 2016, 164, 479–481. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Onakpoya, I.J.; Heneghan, C.J. Effect of the natural sweetener, steviol glycoside, on cardiovascular risk factors: A systematic review and meta-analysis of randomised clinical trials. Eur. J. Prev. Cardiol. 2015, 22, 1575–1587. [Google Scholar] [CrossRef]
- Romo-Romo, A.; Aguilar-Salinas, C.A.; Brito-Córdova, G.X.; Gómez Díaz, R.A.; Vilchis Valentín, D.; Almeda-Valdes, P. Effects of the non-nutritive sweeteners on glucose metabolism and appetite regulating hormones: Systematic review of observational prospective studies and clinical trials. PLoS ONE 2016, 11, e0161264. [Google Scholar] [CrossRef]
- Bonora, E.; Targher, G.; Alberiche, M.; Bonadonna, R.C.; Saggiani, F.; Zenere, M.B.; Monauni, T.; Muggeo, M. Homeostasis model assessment closely mirrors the glucose clamp technique in the assessment of insulin sensitivity: Studies in subjects with various degrees of glucose tolerance and insulin sensitivity. Diabetes Care 2000, 23, 57–63. [Google Scholar] [CrossRef] [Green Version]
- Stumvoll, M.; Mitrakou, A.; Pimenta, W.; Jenssen, T.; Yki-Järvinen, H.; Van Haeften, T.; Renn, W.; Gerich, J. Use of the oral glucose tolerance test to assess insulin release and insulin sensitivity. Diabetes Care 2000, 23, 295–301. [Google Scholar] [CrossRef] [Green Version]
- Matsuda, M.; DeFronzo, R.A. Insulin sensitivity indices obtained from oral glucose tolerance testing: Comparison with the euglycemic insulin clamp. Diabetes Care 1999, 22, 1462–1470. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, S.Y.; Friel, J.K.; MacKay, D.S. The effect of the artificial sweeteners on glucose metabolism in healthy adults: A randomized, double-blinded, crossover clinical trial. Appl. Physiol. Nutr. Metab. Physiol. Appl. Nutr. Et. Metab. 2020, 45, 606–612. [Google Scholar] [CrossRef] [PubMed]
- Romo-Romo, A.; Aguilar-Salinas, C.A.; López-Carrasco, M.G.; Guillén-Pineda, L.E.; Brito-Córdova, G.X.; Gómez-Díaz, R.A.; Gómez-Pérez, F.J.; Almeda-Valdes, P. Sucralose Consumption over 2 Weeks in Healthy Subjects Does Not Modify Fasting Plasma Concentrations of Appetite-Regulating Hormones: A Randomized Clinical Trial. J. Acad. Nutr. Diet. 2020, 120, 1295–1304. [Google Scholar] [CrossRef] [PubMed]
- Lertrit, A.; Srimachai, S.; Saetung, S.; Chanprasertyothin, S.; Chailurkit, L.O.; Areevut, C.; Katekao, P.; Ongphiphadhanakul, B.; Sriphrapradang, C. Effects of sucralose on insulin and glucagon-like peptide-1 secretion in healthy subjects: A randomized, double-blind, placebo-controlled trial. Nutr. Burbank Los Angeles Cty. Calif. 2018, 55, 125–130. [Google Scholar] [CrossRef]
- Tey, S.L.; Salleh, N.B.; Henry, C.J.; Forde, C.G. Effects of non-nutritive (artificial vs natural) sweeteners on 24-h glucose profiles. Eur. J. Clin. Nutr. 2017, 71, 1129–1132. [Google Scholar] [CrossRef]
- Suez, J.; Korem, T.; Zeevi, D.; Zilberman-Schapira, G.; Thaiss, C.A.; Maza, O.; Israeli, D.; Zmora, N.; Gilad, S.; Weinberger, A.; et al. Artificial sweeteners induce glucose intolerance by altering the gut microbiota. Nature 2014, 514, 181–186. [Google Scholar] [CrossRef]
- Palmnäs, M.S.; Cowan, T.E.; Bomhof, M.R.; Su, J.; Reimer, R.A.; Vogel, H.J.; Hittel, D.S.; Shearer, J. Low-dose aspartame consumption differentially affects gut microbiota-host metabolic interactions in the diet-induced obese rat. PLoS ONE 2014, 9, e109841. [Google Scholar] [CrossRef]
- Wang, Q.P.; Browman, D.; Herzog, H.; Neely, G.G. Non-nutritive sweeteners possess a bacteriostatic effect and alter gut microbiota in mice. PLoS ONE 2018, 13, e0199080. [Google Scholar] [CrossRef]
- David, L.A.; Maurice, C.F.; Carmody, R.N.; Gootenberg, D.B.; Button, J.E.; Wolfe, B.E.; Ling, A.V.; Devlin, A.S.; Varma, Y.; Fischbach, M.A.; et al. Diet rapidly and reproducibly alters the human gut microbiome. Nature 2014, 505, 559–563. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Sex (M/F) | 13/26 |
| Age (y) | 34.5 ± 17 |
| Height (m) | 1.7 ± 0.1 |
| Weight (kg) | 75.2, 34.8 |
| Body-mass index (BMI; kg/m2) | 26.1, 9.3 |
| BMI (kg/m2) | |
| Normal | 18 |
| Overweight | 8 |
| Obese | 13 |
| Smoking | |
| Yes | 1 |
| No | 38 |
| Alcohol intake | |
| 0–5/week | 30 |
| 6–10/week | 9 |
| Family diabetes history | |
| Yes | 9 |
| No | 30 |
| NGT (n)IFG/IGT (n) | 33/6 |
| Baseline fasting glucose (mmol/L) | 4.9 ± 0.7 |
| Baseline 2 h glucose (mmol/L) | 5.5 ± 1.6 |
| Variables | ASB | MW | |||||
|---|---|---|---|---|---|---|---|
| Baseline | After 2 Weeks | p Value | N | Baseline | After 2 Weeks | p Value | |
| Fasting glucose (mmol/L) | 4.91, 0.82 | 4.73, 0.72 | 0.65 *** | 35 | 4.98, 0.7 | 4.96, 0.7 | 0.79 *** |
| Fasting insulin (pmol/L) | 8.93, 10.1 | 9.49, 7.03 | 0.10 *** | 31 | 8.67, 9.27 | 8.95, 6.9 | 0.64 *** |
| HOMA-IR | 1.52, 2.22 | 1.86, 2.1 | 0.07 *** | 30 | 2.01, 1.94 | 1.90, 1.28 | 0.42 *** |
| Matsuda index | 5.71, 7.22 | 5.45, 4.97 | 0.32 ** | 30 | 4.67, 5.16 | 4.94, 4.19 | 0.47 ** |
| Glucose AUC | 13.54 ± 5.88 | 12.25 ± 2.99 | 0.14 * | 35 | 13.06, 3.73 | 12.84, 4.09 | 0.85 *** |
| Glucose iAUC | 2.27, 4.37 | 2.51, 3.67 | 0.09 *** | 35 | 3.21, 4.49 | 2.59, 3.84 | 0.45 *** |
| Insulin AUC | 91.9, 84.95 | 96.3, 84.3 | 0.35 ** | 30 | 105.1, 61.3 | 94.1, 98.6 | 0.62 *** |
| Insulin iAUC | 71.3, 52.2 | 76.7, 74.7 | 0.27 ** | 30 | 95.3, 45.2 | 78.7, 86.5 | 0.81 *** |
| Weight changes | 75.2, 34.2 | 75, 32.6 | 0.52 *** | 39 | 76.1, 34.2 | 76.1,33.4 | 0.69 *** |
| BMI changes | 26.2, 8.9 | 26.2, 9.4 | 0.65 ** | 39 | 25.9, 9.34 | 25.4, 9.06 | 0.47 ** |
| Variables | ASB | MW | Between-Group Comparison (after ASB vs. after MW) |
|---|---|---|---|
| Difference at Baseline vs. 2 Weeks | Difference at Baseline vs. 2 Weeks | p Value | |
| Fasting glucose (mmol/L) | −0.044, 0.8 | 0.145, 0.65 | 0.17 |
| Fasting insulin (pmol/L) | −0.94, 6.29 | −0.13, 4.58 | 0.34 |
| Glucose AUC | 0.63, 2.92 | 0.18, 2.82 | 0.31 |
| Glucose iAUC | 0.39, 3.88 | −0.10, 2.9 | 0.86 |
| Insulin AUC | −8.38 ± 35.6 | 3.44 ± 40.1 | 0.17 |
| Insulin iAUC | 3.44 ± 40.1 | 0.07 ± 32.05 | 0.47 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, Y.; Keogh, J.B.; Clifton, P.M. Consumption of a Beverage Containing Aspartame and Acesulfame K for Two Weeks Does Not Adversely Influence Glucose Metabolism in Adult Males and Females: A Randomized Crossover Study. Int. J. Environ. Res. Public Health 2020, 17, 9049. https://doi.org/10.3390/ijerph17239049
Kim Y, Keogh JB, Clifton PM. Consumption of a Beverage Containing Aspartame and Acesulfame K for Two Weeks Does Not Adversely Influence Glucose Metabolism in Adult Males and Females: A Randomized Crossover Study. International Journal of Environmental Research and Public Health. 2020; 17(23):9049. https://doi.org/10.3390/ijerph17239049
Chicago/Turabian StyleKim, Yoona, Jennifer B. Keogh, and Peter M. Clifton. 2020. "Consumption of a Beverage Containing Aspartame and Acesulfame K for Two Weeks Does Not Adversely Influence Glucose Metabolism in Adult Males and Females: A Randomized Crossover Study" International Journal of Environmental Research and Public Health 17, no. 23: 9049. https://doi.org/10.3390/ijerph17239049