COVID-19 in Switzerland and Liechtenstein: A Cross-Sectional Survey among Dentists’ Awareness, Protective Measures and Economic Effects


Abstract
:1. Introduction
2. Materials and Methods
2.1. Development and Calibration of the Questionnaire
2.2. Online Survey
2.3. Data Analysis
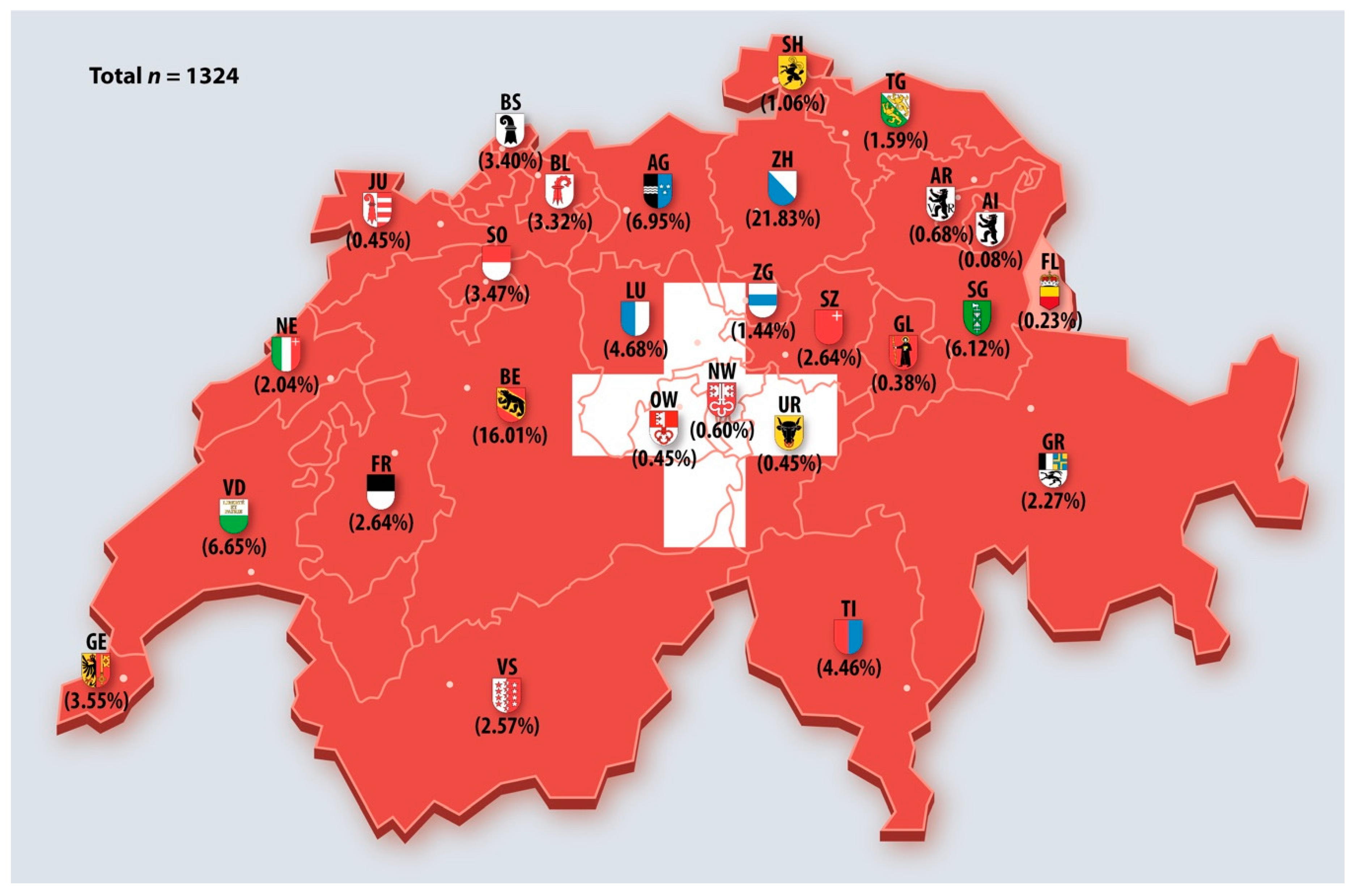
3. Results
4. Discussion
4.1. Awareness of COVID-19
4.2. Protective Measures
4.3. Economic Effects on Dental Practice
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| COVID-19 | Coronavirus Disease |
| SARS-CoV-2 | Severe Acute Respiratory Syndrome Coronavirus 2 |
| OF | Observed frequency |
| AG | Aargau |
| AI | Appenzell Innerhoden |
| AR | Appenzell Ausserrhoden |
| BE | Bern |
| BL | Basel-Landschaft |
| BS | Basel-Stadt |
| FL | Fürstentum (Principality of) Liechtenstein |
| FR | Fribourg |
| GE | Genève |
| GL | Glarus |
| GR | Graubünden |
| JU | Jura |
| LU | Luzern |
| NE | Neuchâtel |
| NW | Nidwalden |
| OW | Obwalden |
| SG | St. Gallen |
| SH | Schaffhausen |
| SO | Solothurn |
| SZ | Schwyz |
| TG | Thurgau |
| TI | Ticino |
| UR | Uri |
| VD | Vaud |
| VS | Valais |
| ZG | Zug |
| ZH | Zürich |
References
- World Health Organization. Rolling Updates on Coronavirus Disease (COVID-19). Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/interactive-timeline (accessed on 23 October 2020).
- World Health Organization. Coronavirus Disease (COVID-19) Weekly Epidemiological Update and Weekly Operational Update. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports (accessed on 23 October 2020).
- Swiss Federal Office of Public Health FOPH (Bundesamt für Gesundheit BAG der Schweizerischen Eidgenossenschaft). New Coronavirus: Situation in Switzerland. Available online: https://www.bag.admin.ch/bag/en/home/krankheiten/ausbrueche-epidemien-pandemien/aktuelle-ausbrueche-epidemien/novel-cov/situation-schweiz-und-international.html (accessed on 23 October 2020).
- Association of Cantonal Dentists of Switzerland (Vereinigung der Kantonszahnärztinnen und Kantonszahnärzte der Schweiz VKZS). Position Paper. Covid-19 Guidelines for the Operation of a Dental Practice during the Covid-19 Pandemic. Available online: https://www.sso.ch/fileadmin/upload_sso/0_Home/2_Newsrollbox/0_PDF/Covid-19-Positionspapier.pdf (accessed on 23 October 2020).
- Swiss Dental Association SSO & Association of Cantonal Dentists of Switzerland VZKS (Vereinigung der Kantonszahnärztinnen und Kantonszahnärzte der Schweiz VKZS). Position Paper. COVID-19-Communication—Frequently Asked Questions to Smart Restart. Available online: https://www.sso.ch/fileadmin/upload_sso/5_Newsletter/2020/Covid-19-Positionspapier3-7.pdf (accessed on 23 October 2020).
- European Centre for Disease Prevention and Control. Available online: https://www.ecdc.europa.eu/en/geographical-distribution-2019-ncov-cases (accessed on 24 June 2020).
- Alwan, N.A.; Burgess, R.A.; Ashworth, S.; Beale, R.; Bhadelia, N.; Bogaert, D.; Dowd, J.; Eckerle, I.; Goldman, L.R.; Greenhalgh, T.; et al. Scientific consensus on the COVID-19 pandemic: We need to act now. Lancet 2020, 396, e71–e72. [Google Scholar] [CrossRef]
- Cagetti, M.G.; Cairoli, J.L.; Senna, A. Guglielmo Campus COVID-19 Outbreak in North Italy: An Overview on Dentistry. A Questionnaire Survey. Int. J. Environ. Res. Pub. Health 2020, 17, 3835. [Google Scholar] [CrossRef] [PubMed]
- Guglielmo Campus; Diaz-Betancourt, M.; Cagetti, M.G.; Carvalho, J.C.; Carvalho, T.S.; Cortés-Martinicorena, J.F.; Deschner, J.; Douglas, G.V.A.; Giacaman, R.A.; Machiulskiene, V.; et al. Study Protocol for an Online Questionnaire Survey on Symptoms/Signs, Protective Measures, Level of Awareness and Perception Regarding COVID-19 Outbreak among Dentists. A Global Survey. Int. J. Environ. Res. Pub. Health 2020, 17, 5598. [Google Scholar] [CrossRef]
- Li, L.; Huang, T.; Wang, Y.; Wang, Z.; Liang, Y.; Huang, T.; Zhang, H.; Sun, W.; Wang, Y. COVID-19 patients’ clinical characteristics, discharge rate, and fatality rate of meta-analysis. J. Med. Virol. 2020, 92, 577–583. [Google Scholar] [CrossRef] [PubMed]
- Fragebogen zur Bewertung der epidemiologischen Situation von COVID-19 von Zahnärzten in der Schweiz. Available online: https://survey.sso.ch/covid/ (accessed on 2 December 2020).
- Swiss Federal Office of Public Health FOPH (Bundesamt für Gesundheit BAG der Schweizerischen Eidgenossenschaft). Statistiken Zahnärztinnen/Zahnärzte (Statistics dentists). Available online: https://www.bag.admin.ch/bag/de/home/zahlen-und-statistiken/statistiken-berufe-im-gesundheitswesen/statistiken-medizinalberufe1/statistiken-zahnaerztinnen-zahnaerzte.html (accessed on 23 October 2020).
- Office for Statistics of the Principality of Liechtenstein (Amt für Statistik, Fürstentum Liechtenstein). Available online: https://www.llv.li/files/as/jahrbuch-2019.pdf (accessed on 23 October 2020).
- Federal Council of the Swiss Confederation (Bundesrat der Schweizerischen Eigdenossenschaft). Federal Act on Research involving Human Beings. Human Research Act (HRA). Available online: https://www.admin.ch/opc/de/classified-compilation/20061313/index.html (accessed on 23 October 2020).
- Volgenant, C.M.C.; De Soet, J.J. Cross-transmission in the Dental Office: Does This Make You Ill? Curr. Oral Health Rep. 2018, 5, 221–228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kamate, S.K.; Sharma, S.; Thakar, S.; Srivastava, D.; Sengupta, K.; Hadi, A.J.; Chaudhary, A.; Joshi, R.; Dhanker, K. Assessing Knowledge, Attitudes and Practices of dental practitioners regarding the COVID-19 pandemic: A multinational study. Dent. Med. Probl. 2020, 57, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Federal Statistics Office of the Swiss Confederation (Bundesamt für Statistik der Schweizerischen Eidgenossenschaft). Available online: https://www.bfs.admin.ch/bfs/de/home/statistiken/kataloge-datenbanken/publikationen/uebersichtsdarstellungen/statistik-schweizer-staedte.html (accessed on 23 October 2020).
- Stangvaltaite-Mouhat, L.; Uhlen, M.-M.; Skudutyte-Rysstad, R.; Hovden, E.A.S.; Shabestari, M.; Ansteinsson, V.E. Dental Health Services Response to COVID-19 in Norway. Int. J. Environ. Res. Pub. Health 2020, 17, 5843. [Google Scholar] [CrossRef] [PubMed]
- Tysiąc-Miśta, M.; Dziedzic, A. The Attitudes and Professional Approaches of Dental Practitioners during the COVID-19 Outbreak in Poland: A Cross-Sectional Survey. Int. J. Environ. Res. Pub. Health 2020, 17, 4703. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Zhou, Y.; Liu, X.; Tan, J. Health services provision of 48 public tertiary dental hospitals during the COVID-19 epidemic in China. Clin. Oral Investig. 2020, 24, 1861–1864. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolf, T.G.; Seeberger, G.K.; Callaway, A.; Briseño-Marroquín, B.; Rusca, P.; Frank, M.; Otterbach, E.-J. Is liberal independent dental practice in danger? Assessing forms of dental practice in the European Regional Organization (ERO) zone of the FDI World Dental Federation. Quintessence Int. 2018, 26, 313–324. [Google Scholar]
- Guglielmo Campus; Rusca, P.; Amrhein, C.; Meier, A.; Zeyer, O.; Wolf, T.G. Career Prospects of Young Dentists in Switzerland. Int. J. Environ. Res. Pub. Health 2020, 17, 4310. [Google Scholar] [CrossRef]
- Wolf, T.G.; Wagner, R.F.; Zeyer, O.; Ilhan, D.; Crnić, T.; Otterbach, E.-J. Guglielmo Campus Expectations Regarding Dental Practice: A Cross-Sectional Survey of European Dental Students. Int. J. Environ. Res. Pub. Health 2020, 17, 7296. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Symptoms/Signs | Low Prevalence Area | Middle Prevalence Area | High Prevalence Area | Total | ||||
|---|---|---|---|---|---|---|---|---|
| OF | % | OF | % | OF | % | n | % | |
| Fever | 3 | 0.23 | 4 | 0.30 | 4 | 0.30 | 11 | 0.83 |
| Cramer’s V = 0.06 Fisher’s exact = 0.12 | ||||||||
| Cough | 8 | 0.60 | 3 | 0.23 | 5 | 0.38 | 16 | 1.21 |
| Cramer’s V = 0.06 Fisher’s exact = 0.08 | ||||||||
| Fatigue | 4 | 0.30 | 8 | 0.60 | 8 | 0.60 | 20 | 1.51 |
| Cramer’s V = 0.09 Fisher’s exact > 0.01 | ||||||||
| Breathing difficulties | 2 | 0.15 | 4 | 0.30 | 3 | 0.23 | 9 | 0.68 |
| Cramer’s V = 0.05 Fisher’s exact = 0.14 | ||||||||
| Nasal congestion | 3 | 0.23 | 1 | 0.08 | 3 | 0.23 | 7 | 0.53 |
| Cramer’s V = 0.06 Fisher’s exact = 0.09 | ||||||||
| COVID 19 | Normal Working | Working Additionally Measures | Only Emergencies | Stop Working for More than 2 Weeks | Practice Close Due to Economic Hardship | Practice Close (Positively Employee) | Practice Close (Positively Owner) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| OF | % | OF | % | OF | % | OF | % | OF | % | OF | % | OF | % | |
| Low prevalence | 11 | 1.81 | 328 | 54.04 | 105 | 17.30 | 126 | 20.76 | 19 | 3.13 | 1 | 0.16 | 17 | 2.80 |
| Middle prevalence | 9 | 1.75 | 250 | 48.64 | 98 | 19.07 | 119 | 23.15 | 15 | 2.92 | 3 | 0.58 | 20 | 3.89 |
| High prevalence | 6 | 3.09 | 75 | 38.66 | 48 | 24.74 | 35 | 18.04 | 8 | 4.12 | 2 | 1.03 | 20 | 10.31 |
| p-value | χ2(2) = 66.21 < 0.01 | χ2(2) = 48.33 < 0.01 | χ2(2) = 18.73 <0.01 | χ2(2) = 7.97 0.02 | χ2(2) = 36.66 < 0.01 | 0.09 | χ2(2) = 61.37 < 0.01 | |||||||
| COVID 19 Prevalence | Workload < 10% | Workload < 30% | Workload 60% | Normal Workload (100%) | ||||
|---|---|---|---|---|---|---|---|---|
| OF | % | OF | % | OF | % | OF | % | |
| Low prevalence | 428 | 46.37 | 106 | 54.92 | 23 | 46.00 | 49 | 32.03 |
| Middle prevalence | 379 | 41.06 | 71 | 36.79 | 18 | 36.00 | 9 | 18.00 |
| High prevalence | 116 | 12.57 | 16 | 8.29 | 51 | 33.33 | 53 | 34.64 |
| p-value | χ2(2) = 297.82 < 0.01 | χ2(2) = 496.71 < 0.01 | χ2(2) = 37.84 < 0.01 | χ2(2) = 8.11 0.02 | ||||
| COVID 19 | Small | Medium-Small | Medium-Large | Large | ||||
|---|---|---|---|---|---|---|---|---|
| OF | % | OF | % | OF | % | OF | % | |
| Low prevalence | 41 | 6.73 | 121 | 19.87 | 62 | 10.18 | 385 | 63.22 |
| Middle prevalence | 17 | 3.26 | 146 | 28.02 | 69 | 13.24 | 289 | 55.47 |
| High prevalence | -- | -- | -- | -- | 59 | 30.41 | 135 | 69.59 |
| p-value | χ2(2) = 23.12 < 0.01 | χ2(2) = 1.75 0.19 | χ2(2) = 16.04 < 0.01 | χ2(2) = 4.82 0.09 | ||||
| Use of Face Filter (FFP2/FFP3) | Disposable Visor | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| COVID 19 | Area | No | Yes | No | Yes | ||||
| OF | % | OF | % | OF | % | OF | % | ||
| Low prevalence | Small | 34 | 58.62 | 24 | 41.38 | 39 | 95.12 | 2 | 4.88 |
| Medium-small | 143 | 53.56 | 124 | 46.44 | 108 | 89.26 | 13 | 10.74 | |
| Medium-large | 88 | 46.32 | 102 | 53.68 | 54 | 87.10 | 8 | 12.90 | |
| Large | 363 | 44.87 | 446 | 55.13 | 330 | 85.71 | 55 | 14.29 | |
| p-value | χ2(3) = 12.69 p < 0.01 | χ2(3) = 3.52 p = 0.32 | |||||||
| Middle Prevalence | Small | 25 | 60.98 | 16 | 39.02 | 12 | 70.59 | 5 | 29.41 |
| Medium-small | 77 | 63.64 | 44 | 36.36 | 113 | 77.40 | 33 | 22.60 | |
| Medium-large | 29 | 46.77 | 33 | 53.23 | 59 | 85.51 | 10 | 14.49 | |
| Large | 185 | 48.05 | 200 | 51.95 | 249 | 86.16 | 40 | 13.84 | |
| p-value | χ2(3) = 10.97 p = 0.01 | χ2(3) = 54.73 p < 0.01 | |||||||
| High Prevalence | Small | 9 | 52.94 | 8 | 47.06 | -- | -- | -- | -- |
| Medium-small | 66 | 45.21 | 80 | 54.79 | -- | -- | -- | -- | |
| Medium-large | 38 | 55.07 | 31 | 44.93 | 47 | 79.66 | 12 | 20.34 | |
| Large | 143 | 49.48 | 146 | 50.52 | 114 | 84.44 | 21 | 15.56 | |
| p-value | χ2(3) = 1.99 p = 0.57 | χ2(1) = 0.37 p = 0.54 | |||||||
| COVID-19 Prevalence Area | Variables | OR (SE) | p-Value | 95% CI |
|---|---|---|---|---|
| Low Prevalence | Base Outcome | |||
| Middle Prevalence | Area by size | 0.90 (0.06) | 0.08 | 0.79–1.01 |
| Work during lockdown | 1.02 (0.02) | 0.45 | 0.97–1.07 | |
| Presence of symptoms | 1.37 (0.40) | 0.27 | 0.78–2.42 | |
| Use of face filter (FFP2/FFP3) | 1.11 (0.13) | 0.403 | 0.87–1.41 | |
| Disposable visor | 1.32 (0.23) | 0.78 | 0.69–1.65 | |
| High Prevalence | Area by size | 1.80 (0.22) | <0.01 | 1.41–2.29 |
| Work during lockdown | 1.17 (0.03) | <0.01 | 1.11–1.23 | |
| Presence of symptoms | 2.91 (0.88) | <0.01 | 1.61–5.26 | |
| Use of face filter (FFP2/FFP3) | 2.55 (0.48) | <0.01 | 1.77–3.68 | |
| Disposable visor | 1.15 (0.28) | 0.54 | 0.72–1.85 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wolf, T.G.; Zeyer, O.; Campus, G. COVID-19 in Switzerland and Liechtenstein: A Cross-Sectional Survey among Dentists’ Awareness, Protective Measures and Economic Effects. Int. J. Environ. Res. Public Health 2020, 17, 9051. https://doi.org/10.3390/ijerph17239051
Wolf TG, Zeyer O, Campus G. COVID-19 in Switzerland and Liechtenstein: A Cross-Sectional Survey among Dentists’ Awareness, Protective Measures and Economic Effects. International Journal of Environmental Research and Public Health. 2020; 17(23):9051. https://doi.org/10.3390/ijerph17239051
Chicago/Turabian StyleWolf, Thomas Gerhard, Oliver Zeyer, and Guglielmo Campus. 2020. "COVID-19 in Switzerland and Liechtenstein: A Cross-Sectional Survey among Dentists’ Awareness, Protective Measures and Economic Effects" International Journal of Environmental Research and Public Health 17, no. 23: 9051. https://doi.org/10.3390/ijerph17239051