Synergy Effect of Combined Near and Mid-Infrared Fibre Spectroscopy for Diagnostics of Abdominal Cancer

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Collection
2.2. Sample Preparation
2.3. Spectroscopic Measurements
2.4. Histopathological Evaluation
2.5. Data Analysis
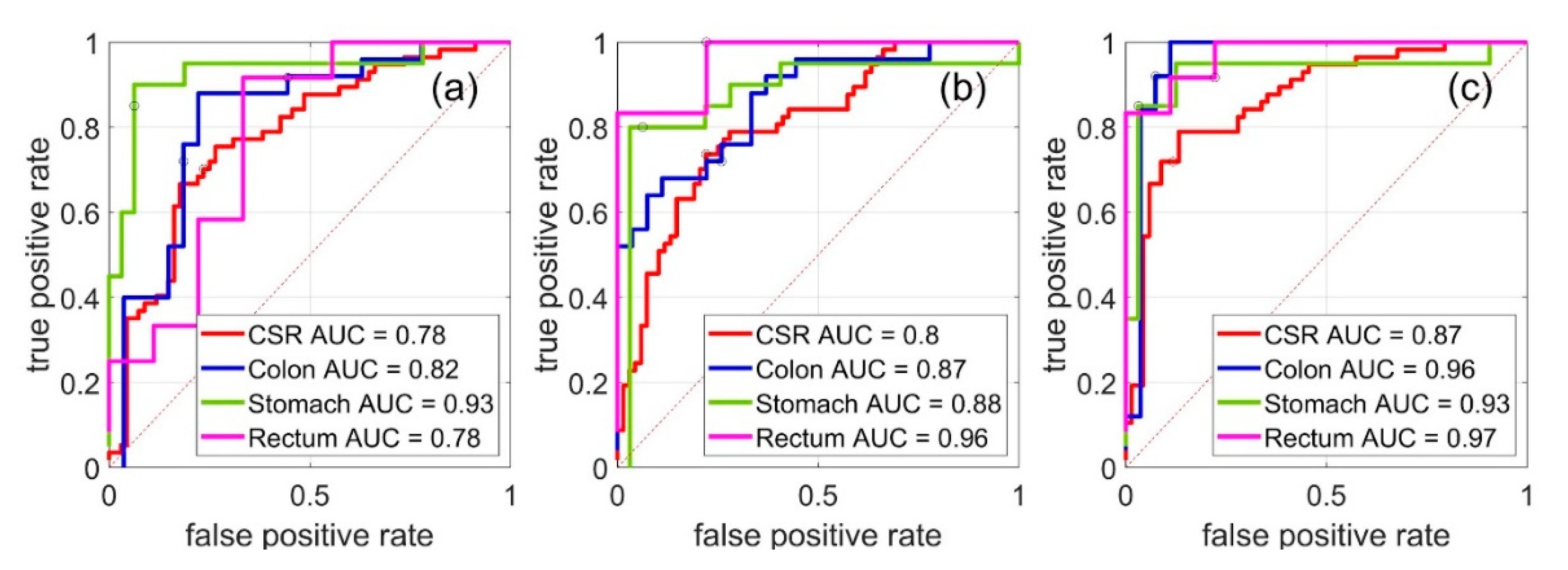
2.6. Models Ranking Using ROC-Curves
3. Results and Discussion
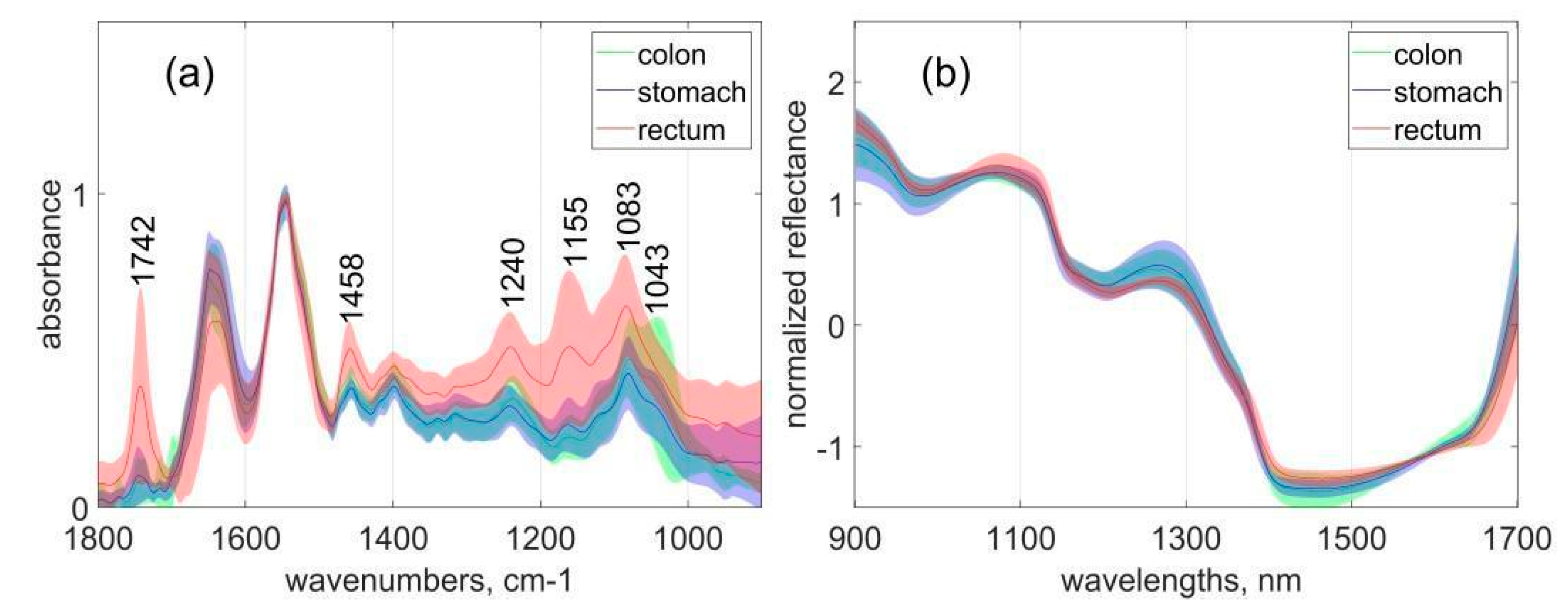
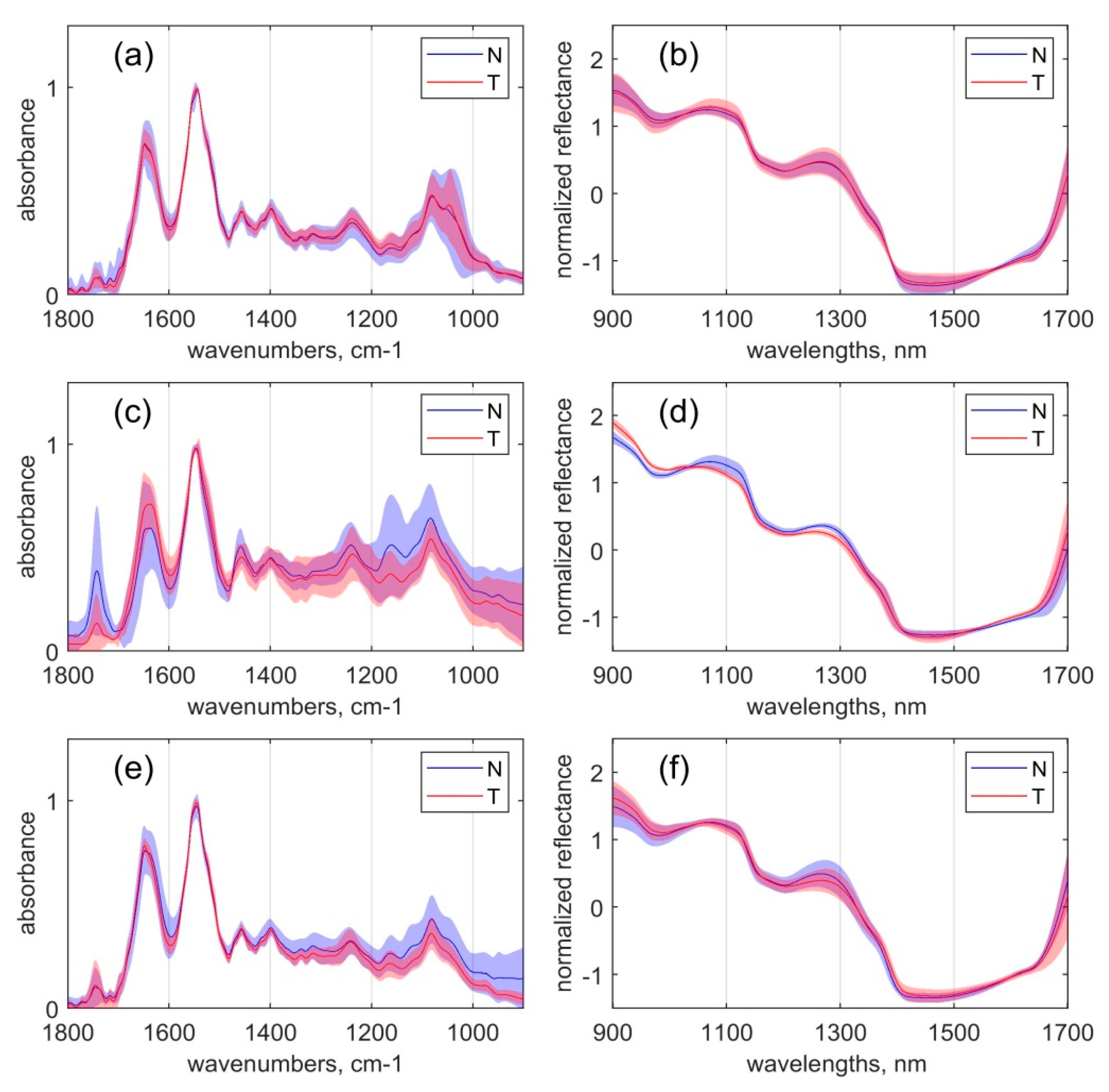
3.1. Spectral Analysis
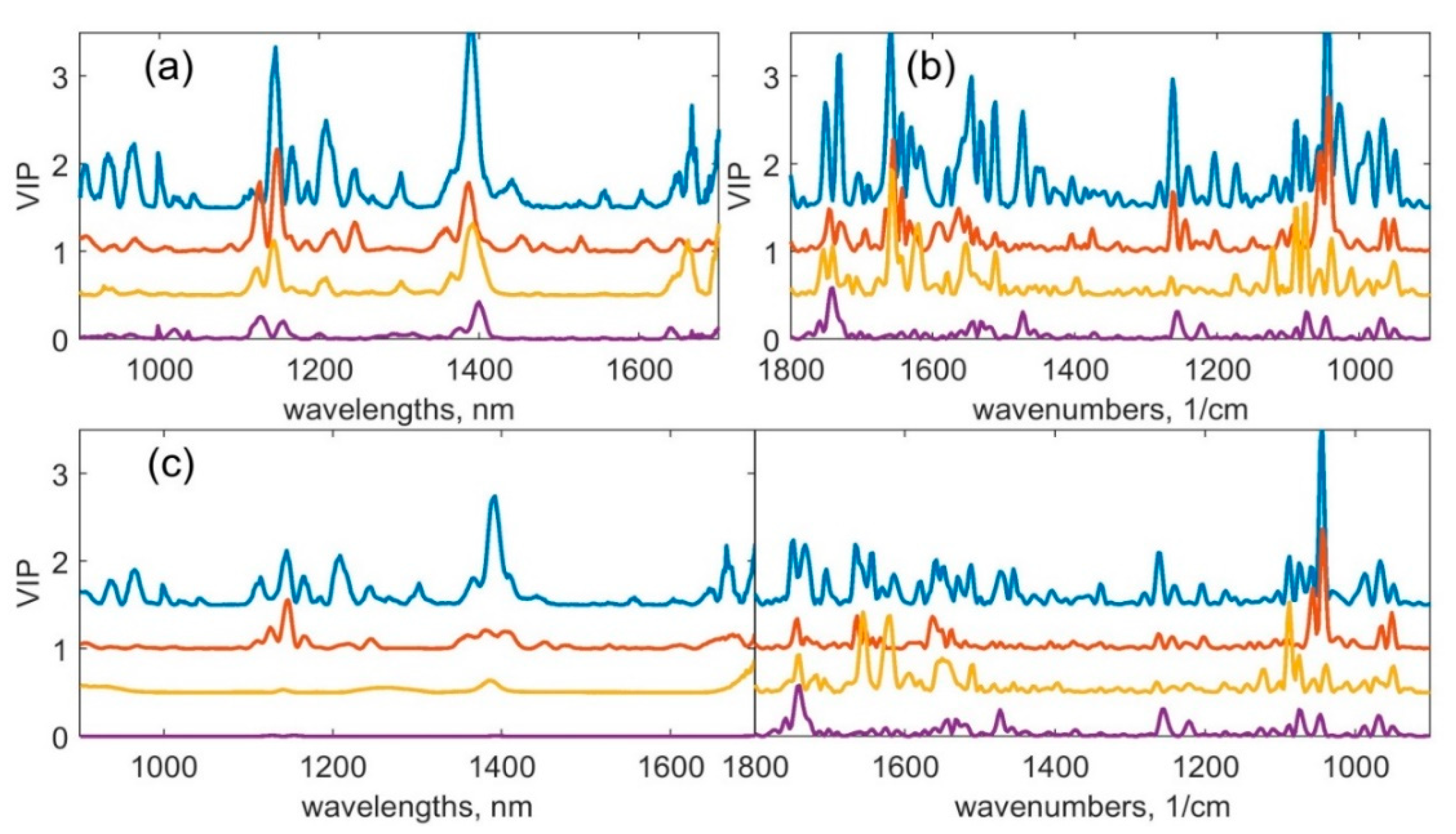
3.2. Multivariate Analysis
4. Conclusions and Outlook
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Roser, M.; Ritchie, H. Cancer. 2015. Available online: https://ourworldindata.org/cancer (accessed on 19 October 2020).
- John, S.; Broggio, J. Cancer Survival in England-Adults Diagnosed. 2019. Available online: https://www.nuffieldtrust.org.uk/resource/cancer-survival-rates (accessed on 19 October 2020).
- Senkus, E.; Kyriakides, S.; Ohno, S.; Penault-Llorca, F.; Poortmans, P.; Rutgers, E.; Zackrisson, S.; Cardoso, F. Primary breast cancer: ESMO Clinical Practice. Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2015, 26, 8–30. [Google Scholar] [CrossRef] [PubMed]
- Hijazi, Y.; Gondal, U.; Aziz, O. A systematic review of prehabilitation programs in abdominal cancer surgery. Int. J. Surg. 2017, 39, 156–162. [Google Scholar] [CrossRef] [PubMed]
- Hiller, J.G.; Perry, N.J.; Poulogiannis, G.; Riedel, B.; Sloan, E.K. Perioperative events influence cancer recurrence risk after surgery. Nat. Rev. Clin. Oncol. 2018, 15, 205–218. [Google Scholar] [CrossRef]
- Krafft, C.; Dochow, S.; Latka, I.; Dietzek, B.; Popp, J. Diagnosis and screening of cancer tissues by fiber-optic probe Raman spectroscopy. Biomed. Spectrosc. Imaging 2012, 1, 39–55. [Google Scholar] [CrossRef]
- Flusberg, B.A.; Cocker, E.D.; Piyawattanametha, W.; Jung, J.C.; Cheung, E.L.M.; Schnitzer, M.J. Fiber-optic fluorescence imaging. Nat. Methods 2005, 2, 941–950. [Google Scholar] [CrossRef] [PubMed]
- Tu, Q.; Chang, C. Diagnostic applications of Raman spectroscopy. Nanomedicine 2012, 8, 545–558. [Google Scholar] [CrossRef]
- Bird, B.; Miljković, M.; Remiszewski, S.; Akalin, A.; Kon, M.; Diem, M. Infrared spectral histopathology (SHP): A novel diagnostic tool for the accurate classification of lung cancer. Lab. Investig. 2012, 92, 1358–1373. [Google Scholar] [CrossRef] [Green Version]
- Brozek-Pluska, B.; Dziki, A.; Abramczyk, H. Virtual spectral histopathology of colon cancer - biomedical applications of Raman spectroscopy and imaging. J. Mol. Liq. 2020, 303, 112676. [Google Scholar] [CrossRef]
- Hui, R.; O’Sullivan, M. Fiber Optic Measurement Techniques; Elsevier Academic Press: Burlington, MA, USA, 2009. [Google Scholar]
- Arimoto, H.; Egawa, M.; Yamada, Y. Depth profile of diffuse reflectance near-infrared spectroscopy for measurement of water content in skin. Skin Res. Technol. 2005, 11, 27–35. [Google Scholar] [CrossRef]
- Moreau, F.; Yang, R.; Nambiar, V.; Demchuk, A.M.; Dunn, J.F. Near-infrared measurements of brain oxygenation in stroke. Neurophotonics 2016, 3, 031403. [Google Scholar] [CrossRef] [Green Version]
- Kondepati, V.R.; Heise, H.M.; Backhaus, J. Recent applications of near-infrared spectroscopy in cancer diagnosis and therapy. Anal. Bioanal. Chem. 2008, 390, 125. [Google Scholar] [CrossRef] [PubMed]
- Bogomolov, A.; Zabarylo, U.; Kirsanov, D.; Belikova, V.; Ageev, V.; Usenov, I.; Galyanin, V.; Minet, O.; Sakharova, T.; Danielyan, G.; et al. Development and Testing of an LED-Based Near-Infrared Sensor for Human Kidney Tumor Diagnostics. Sensors 2017, 17, 1914. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakudo, A. Near-infrared spectroscopy for medical applications: Current status and future perspectives. Clin. Chim. Acta 2016, 455, 181–188. [Google Scholar] [CrossRef] [PubMed]
- Yi, W.-e.; Cui, D.-s.; Li, Z.; Wu, L.-l.; Shen, A.-g.; Hu, J.-m. Gastric cancer differentiation using Fourier transform near-infrared spectroscopy with unsupervised pattern recognition. Spectrochim. Acta Part A Mol. Biomol. Spectrosc. 2013, 101, 127–131. [Google Scholar] [CrossRef] [PubMed]
- Kondepati, V.R.; Keese, M.; Mueller, R. Bernd Christoph Manegold, Juergen Backhaus. Application of near-infrared spectroscopy for the diagnosis of colorectal cancer in resected human tissue specimens. Vib. Spectrosc. 2007, 44, 236–242. [Google Scholar] [CrossRef]
- Ferrari, M.; Mottola, L.; Quaresima, V. Principles, Techniques, and Limitations of Near Infrared Spectroscopy. Can. J. Appl. Physiol. 2004, 29, 463–487. [Google Scholar] [CrossRef] [Green Version]
- Guardia, M.d.l. Vibrational Spectroscopy. In Comprehensive Analytical Chemistry; Guardia, M.d.l., Garrigues, S., Eds.; Elsevier: Amsterdam, The Netherlands, 2013; Volume 60, pp. 101–122. [Google Scholar]
- Morros, J.; Garrigues, S.; Guardia, M.d.l. Vibrational spectroscopy provides a green tool for multi-component analysis. TrAC Trends Anal. Chem. 2010, 29, 578–591. [Google Scholar] [CrossRef]
- Baker, M.J.; Trevisan, J.; Bassan, P.; Bhargava, R.; Butler, H.J.; Dorling, K.M.; Fielden, P.R.; Fogarty, S.W.; Fullwood, N.J.; Heys, K.A.; et al. Using Fourier Transform IR Spectroscopy to Analyze Biological Materials. Nat. Protoc. 2014, 9, 1771–1791. [Google Scholar] [CrossRef] [Green Version]
- Minnes, R.; Nissinmann, M.; Maizels, Y.; Gerlitz, G.; Katzir, A.; Raichlin, Y. Using Attenuated Total Reflection–Fourier Transform Infra-Red (ATR-FTIR) spectroscopy to distinguish between melanoma cells with a different metastatic potential. Sci. Rep. 2017, 7, 4381. [Google Scholar] [CrossRef]
- Bunaciu, A.A.; Fleschin, S.; Aboul-enein, H.Y. Cancer diagnosis by ftir spectrophotometry. Rev. Roum. Chim. 2015, 60, 415–426. [Google Scholar]
- Li, G.; Thomson, M.; Dicarlo, E.; Xu, Y.; Nestor, B.; Bostrom, M.P.G.; Camacho, N.P. A chemometric analysis for evaluation of early-stage cartilage degradation by infrared fiber-optic probe spectroscopy. Appl. Spectrosc. 2005, 59, 1527–1533. [Google Scholar] [CrossRef] [PubMed]
- Sablinskas, V.; Velicka, M.; Pucetaite, M.; Urboniene, V.; Ceponkus, J.; Bandzeviciute, R.; Jankevicius, F.; Sakharova, T.; Bibikova, O.; Steiner, G. In situ detection of cancerous kidney tissue by means of fiber ATR-FTIR spectroscopy. Imaging Manip. Anal. Biomol. Cells Tissues XVI 2018, 10497, 1049713. [Google Scholar] [CrossRef]
- Finlayson, D.; Rinaldi, C.; Baker, M.J. Is Infrared Spectroscopy Ready for the Clinic? Anal. Chem. 2019, 91, 12117–12128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Varma, V.K.; Kajdacsy-Balla, A.; Akkina, S.K.; Setty, S.; Walsh, M.J. A label-free approach by infrared spectroscopic imaging for interrogating the biochemistry of diabetic nephropathy progression. Kidney Int. 2016, 89, 1153–1159. [Google Scholar] [CrossRef] [Green Version]
- Sreedhar, H.; Carns, M.; Aren, K.; Nazeer, S.S.; Walsh, M.J.; Varga, J. Label-free spectroscopic imaging of the skin characterizes biochemical changes associated with systemic sclerosis. Vib. Spectrosc. 2020, 109, 103102. [Google Scholar] [CrossRef]
- Ami, D.; Mereghetti, P.; Foli, A.; Tasaki, M.; Milani, P.; Nuvolone, M.; Palladini, G.; Merlini, G.; Lavatelli, F.; Natalello, A. ATR-FTIR Spectroscopy Supported by Multivariate Analysis for the Characterization of Adipose Tissue Aspirates from Patients Affected by Systemic Amyloidosis. Anal. Chem. 2019, 91, 2894–2900. [Google Scholar] [CrossRef]
- Tunnell, J.W.; Desjardins, A.E.; Galindo, L.; Georgakoudi, I.; McGee, S.A.; Mirkovic, J.; Mueller, M.G.; Nazemi, J.; Nguyen, F.T.; Wax, A.; et al. Instrumentation for Multi-Modal Spectroscopic Diagnosis of Epithelial Dysplasia. Technol. Cancer Res. Treat. 2003, 2, 505–514. [Google Scholar] [CrossRef]
- Volynskaya, Z.; Haka, A.S.; Bechtel, K.L.; Fitzmaurice, M.; Shenk, R.; Wang, N.; Nazemi, J.; Dasari, R.R.; Feld, M.S. Diagnosing Breast Cancer Using Diffuse Reflectance Spectroscopy and Intrinsic Fluorescence Spectroscopy. J. Biomed. Opt. 2008, 13, 024012. [Google Scholar] [CrossRef]
- Bogomolov, A.; Belikova, V.; Zabarylo, U.J.; Bibikova, O.; Usenov, I.; Sakharova, T.; Krause, H.; Minet, O.; Feliksberger, E.; Artyushenko, V. Synergy Effect of Combining Fluorescence and Mid Infrared Fiber Spectroscopy for Kidney Tumor Diagnostics. Sensors 2017, 17, 2548. [Google Scholar] [CrossRef] [Green Version]
- Chang, S.K.; Mirabal, Y.N.; Atkinson, E.N.; Cox, D.; Malpica, A.; Follen, M.; Richards-Kortum, R.J. Combined Reflectance and Fluorescence Spectroscopy for In Vivo Detection of Cervical pre-Cancer. J. Biomed. Opt. 2005, 10, 024031. [Google Scholar] [CrossRef]
- Ehlen, L.; Zabarylo, U.J.; Speichinger, F.; Bogomolov, A.; Belikova, V.; Bibikova, O.; Artyushenko, V.; Minet, O.; Beyer, K.; Kreis, M.E.; et al. Synergy of Fluorescence and Near-Infrared Spectroscopy in Detection of Colorectal Cancer. J. Surg. Res. 2019, 242, 349–356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pieszczek, L.; Daszykowski, M. Improvement of recyclable plastic waste detection—A novel strategy for the construction of rigorous classifiers based on the hyperspectral images. Chemom. Intell. Lab. Syst. 2009, 187, 28–40. [Google Scholar] [CrossRef]
- Lee, L.C.; Liong, C.Y.; Jemain, A.A. Partial least squares-discriminant analysis (PLS-DA) for classification of high-dimensional (HD) data: A review of contemporary practice strategies and knowledge gaps. Analyst 2018, 143, 3526–3539. [Google Scholar] [CrossRef] [PubMed]
- Andersen, C.M.; Bro, R. Variable selection in regression—A tutorial. J. Chemom. Spec. Issue Herman Wold Medal Win. 2010, 24, 728–737. [Google Scholar] [CrossRef]
- Wong, T.-T. Performance evaluation of classification algorithms by k-fold and leave-one-out cross validation. Pattern Recognit. 2015, 48, 2839–2846. [Google Scholar] [CrossRef]
- Petersen, D.; Naveed, P.; Ragheb, A.; Niedieker, D.; El-Mashtoly, S.F.; Brechmann, T.; Kötting, C.; Schmiegel, W.H.; Freier, E.; Pox, C.; et al. Raman fiber-optical method for colon cancer detection: Cross-validation and outlier identification approach. Spectrochim. Acta Part A Mol. Biomol. Spectrosc. 2017, 181, 270–275. [Google Scholar] [CrossRef]
- Krakowska, B.; Custers, D.; Deconinck, E.; Daszykowski, M. The Monte Carlo validation framework for the discriminant partial least squares model extended with variable selection methods applied to authenticity studies of Viagra® based on chromatographic impurity profiles. Analyst 2016, 141, 1060–1070. [Google Scholar] [CrossRef]
- Pieszczek, L.; Czarnik-Matusewicz, H.; Daszykowski, M. Identification of ground meat species using near-infrared spectroscopy and class modeling techniques–Aspects of optimization and validation using a one-class classification model. Meat Sci. 2018, 139, 15–24. [Google Scholar] [CrossRef]
- Rinnan, Å.; Berg, F.; Engelsen, S. Review of the Most Common pre-Processing Techniques for Near-Infrared Spectra. TrAC Trends Anal. Chem. 2009, 28, 1201–1222. [Google Scholar] [CrossRef]
- Fawcett, T. An introduction to ROC analysis. Pattern Recognit. Lett. 2006, 27, 861–874. [Google Scholar] [CrossRef]
- Casal, H.L.; Mantsch, H.H. Polymorphic phase behaviour of phospholipid membranes studied by infrared spectroscopy. Biochim. Biophys. Acta (BBA)-Rev. Biomembr. 1984, 779, 381–401. [Google Scholar] [CrossRef]
- Arrondo, J.L.R.; Goñi, F.M. Infrared studies of protein-induced perturbation of lipids in lipoproteins and membranes. Chem. Phys. Lipids 1998, 96, 53–68. [Google Scholar] [CrossRef] [Green Version]
- Dong, L.; Sun, X.; Chao, Z.; Zhang, S.; Zheng, J.; Gurung, R.; Du, J.; Shi, J.; Xu, Y.; Zhang, Y.; et al. Evaluation of FTIR spectroscopy as diagnostic tool for colorectal cancer using spectral analysis. Spectrochim. Acta Part A Mol. Biomol. Spectrosc. 2014, 122, 288–294. [Google Scholar] [CrossRef] [PubMed]
- Simonova, D.; Karamancheva, I. Application of Fourier Transform Infrared Spectroscopy for Tumor Diagnosis. Biotechnol. Biotechnol. Equip. 2013, 27, 4200–4207. [Google Scholar] [CrossRef]
- Talari, A.C.S.; Martinez, M.A.G.; Movasaghi, Z.; Rehman, S.; Rehman, I.U. Advances in Fourier transform infrared (FTIR) spectroscopy of biological tissues. Appl. Spectrosc. Rev. 2017, 52, 456–506. [Google Scholar] [CrossRef]
- Takahashi, S.; Satomi, A.; Yano, K.; Kawase, H.; Tanimizu, T.; Tuji, Y.; Murakami, S.; Hirayama, R. Estimation of glycogen levels in human colorectal cancer tissue: Relationship with cell cycle and tumor outgrowth. J. Gastroenterol. 1999, 34, 474–480. [Google Scholar] [CrossRef]
- Kondepati, V.R.; Oszinda, T.; Heise, H.M.; Luig, K.; Mueller, R.; Schroeder, O.; Keese, M.; Backhaus, J. CH-overtone regions as diagnostic markers for near-infrared spectroscopic diagnosis of primary cancers in human pancreas and colorectal tissue. Anal. Bioanal. Chem. 2007, 387, 1633–1641. [Google Scholar] [CrossRef]
- Yano, K.; Sakamoto, Y.; Hirosawa, N.; Tonooka, S.; Katayama, H.; Kumaido, K.; Satomi, A. Applications of Fourier transform infrared spectroscopy, Fourier transform infrared microscopy and near-infrared spectroscopy to cancer research. Spectroscopy 2003, 17, 315–321. [Google Scholar] [CrossRef] [Green Version]
- Chen, H.; Lin, Z.; Wu, H.; Wang, L.; Wu, T.; Tan, C. Diagnosis of colorectal cancer by near-infrared optical fiber spectroscopy and random forest. Spectrochim. Acta Part A Mol. Biomol. Spectrosc. 2015, 135, 185–191. [Google Scholar] [CrossRef]
- Wan, Q.-S.; Wang, T.; Zhang, K.-H. Biomedical optical spectroscopy for the early diagnosis of gastrointestinal neoplasms. Tumor Biol. 2017, 39. [Google Scholar] [CrossRef] [Green Version]
- Li, Q.; Hao, C.; Kang, X.; Zhang, J.; Sun, X.; Wang, W.; Zeng, H. Colorectal Cancer and Colitis Diagnosis Using Fourier Transform Infrared Spectroscopy and an Improved K-Nearest-Neighbour Classifier. Sensors 2017, 17, 2739. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, S.C.; Lee, S.J.; Namkung, H.; Chung, H.; Han, S.-H.; Yoon, M.-Y.; Park, J.-J.; Lee, J.-H.; Oh, C.-H.; Woo, Y.-A. Feasibility study for diagnosis of stomach adenoma and cancer using IR spectroscopy. Vib. Spectrosc. 2007, 44, 279–285. [Google Scholar] [CrossRef]
- Lee, S.; Kim, K.; Lee, H.; Jun, C.-H.; Chung, H.; Park, J.-J. Improving the classification accuracy for IR spectroscopic diagnosis of stomach and colon malignancy using non-linear spectral feature extraction methods. Analyst 2013, 138, 4076–4082. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, H.; Yang, S.; Kong, J.; Dong, A.; Yu, S. Obtaining information about protein secondary structures in aqueous solution using Fourier transform IR spectroscopy. Nat. Protoc. 2015, 10, 382–396. [Google Scholar] [CrossRef] [PubMed]
- Fabian, H.; Lasch, P.; Naumann, D. Analysis of biofluids in aqueous environment based on mid-infrared spectroscopy. J. Biomed. Opt. 2005, 10, 031103. [Google Scholar] [CrossRef] [PubMed]
- Zohdi, V.; Whelan, D.R.; Wood, B.R.; Pearson, J.T.; Bambery, K.R.; Black, M.J. Importance of Tissue Preparation Methods in FTIR Micro-Spectroscopical Analysis of Biological Tissues: ‘Traps for New Users’. PLoS ONE 2015, 10, e0116491. [Google Scholar] [CrossRef] [Green Version]
- Dybas, J.; Marzec, K.M.; Pacia, M.Z.; Kochan, K.; Czamara, K.; Chrabaszcz, K.; Staniszewska-Slezak, e.; Malek, K.; Baranska, M.; Kaczor, A. Raman spectroscopy as a sensitive probe of soft tissue composition—Imaging of cross-sections of various organs vs. single spectra of tissue homogenates. TrAC Trends Anal. Chem. 2016, 85C, 117–127. [Google Scholar] [CrossRef]
- Barroso, E.M.; Smits, R.W.H.; Bakker Schut, T.C.; ten Hove, I.; Hardillo, J.A.; Wolvius, E.B.; Baatenburg de Jong, R.J.; Koljenović, S.; Puppels, G.J. Discrimination between Oral Cancer and Healthy Tissue Based on Water Content Determined by Raman Spectroscopy. Anal. Chem. 2015, 87, 2419–2426. [Google Scholar] [CrossRef]
- Ralbovsky, N.M.; Lednev, I.K. Raman spectroscopy and chemometrics: A potential universal method for diagnosing cancer. Spectrochim. Acta Part A Mol. Biomol. Spectrosc. 2019, 219, 463–487. [Google Scholar] [CrossRef]
- Cugmas, B.; Bürmen, M.; Bregar, M.; Pernuš, F.; Likar, B. Pressure-induced near infrared spectra response as a valuable source of information for soft tissue classification. J. Biomed. Opt. 2013, 18, 047002. [Google Scholar] [CrossRef] [Green Version]
- Kukreti, S.; Cerussi, A.; Tromberg, B.; Gratton, E. Intrinsic tumor biomarkers revealed by novel double-differential spectroscopic analysis of near-infrared spectra. J. Biomed. Opt. 2007, 12, 020509. [Google Scholar] [CrossRef] [PubMed]
- Pasquini, C. Near infrared spectroscopy: A mature analytical technique with new perspectives—A review. Anal. Chim. Acta 2018, 1026, 8–36. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Organ | Number of Patients | Number of Samples | Cancer in Tumour Sample (Confirmed) | Absence of Cancer in Normal Sample (Confirmed) |
|---|---|---|---|---|
| Stomach | 19 | 38 (19N, 19T) | 9 (T)/19 (T) | 15 (N)/19 (N) |
| Colon | 10 | 20 (10N, 10T) | 9 (T)/10 (T) | 10 (N)/10 (N) |
| Rectum | 6 | 12 (6N, 6T) | 6 (T)/6 (T) | 6 (N)/6 (N) |
| # | Method | LV 1 | Pre-processing | Calibration 5 | Cross-Validation (Leave-One-Out) | Cross-Validation (Monte Carlo) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| %Se 2 | %Sp 3 | %Ac 4 | %Se 2 | %Sp 3 | %Ac 4 | %Se 2 | %Sp 3 | %Ac 4 | ||||
| Colon, Stomach, Rectum (CSR) samples set | ||||||||||||
| 1 | NIR | 5 | 2D, SNV | 84 | 84 | 84 | 70 | 76 | 74 | 64 | 78 | 72 |
| 2 | MIR | 5 | 2D, SNV | 82 | 81 | 82 | 74 | 78 | 76 | 70 | 70 | 70 |
| 3 | Combination | 5 | 2D, SNV | 2D, SNV | 91 | 94 | 93 | 72 | 90 | 82 | 68 | 86 | 78 |
| Colon samples set | ||||||||||||
| 4 | NIR | 5 | 2D | 92 | 89 | 90 | 72 | 81 | 77 | 62 | 74 | 69 |
| -* | 4 | 2D, SNV | 80 | 81 | 81 | 64 | 74 | 69 | 61 | 75 | 68 | |
| 5 | MIR | 5 | 2D, SNV | 96 | 96 | 96 | 72 | 78 | 75 | 78 | 83 | 80 |
| 6 | Combination | 5 | 2D, SNV | 2D, SNV | 100 | 96 | 98 | 92 | 93 | 92 | 84 | 96 | 90 |
| Stomach samples set | ||||||||||||
| 7 | NIR | 5 | 2D | 90 | 94 | 92 | 85 | 94 | 90 | 84 | 92 | 89 |
| -* | 5 | SNV | 75 | 94 | 87 | 60 | 81 | 73 | 61 | 82 | 74 | |
| 8 | MIR | 5 | 2D, SNV | 90 | 97 | 94 | 80 | 94 | 88 | 78 | 92 | 87 |
| 9 | Combination | 5 | SNV | 2D, SNV | 95 | 100 | 98 | 85 | 97 | 92 | 75 | 97 | 88 |
| Rectum samples set | ||||||||||||
| 10 | NIR | 5 | 2D | 100 | 100 | 100 | 92 | 67 | 81 | 87 | 58 | 75 |
| 11 | MIR | 5 | 2D | 100 | 100 | 100 | 92 | 78 | 86 | 94 | 81 | 89 |
| 12 | Combination | 5 | 2D | 2D | 100 | 100 | 100 | 92 | 89 | 90 | 96 | 83 | 90 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hocotz, T.; Bibikova, O.; Belikova, V.; Bogomolov, A.; Usenov, I.; Pieszczek, L.; Sakharova, T.; Minet, O.; Feliksberger, E.; Artyushenko, V.; et al. Synergy Effect of Combined Near and Mid-Infrared Fibre Spectroscopy for Diagnostics of Abdominal Cancer. Sensors 2020, 20, 6706. https://doi.org/10.3390/s20226706
Hocotz T, Bibikova O, Belikova V, Bogomolov A, Usenov I, Pieszczek L, Sakharova T, Minet O, Feliksberger E, Artyushenko V, et al. Synergy Effect of Combined Near and Mid-Infrared Fibre Spectroscopy for Diagnostics of Abdominal Cancer. Sensors. 2020; 20(22):6706. https://doi.org/10.3390/s20226706
Chicago/Turabian StyleHocotz, Thaddäus, Olga Bibikova, Valeria Belikova, Andrey Bogomolov, Iskander Usenov, Lukasz Pieszczek, Tatiana Sakharova, Olaf Minet, Elena Feliksberger, Viacheslav Artyushenko, and et al. 2020. "Synergy Effect of Combined Near and Mid-Infrared Fibre Spectroscopy for Diagnostics of Abdominal Cancer" Sensors 20, no. 22: 6706. https://doi.org/10.3390/s20226706