
Abstract
NETosis is a program for formation of neutrophil extracellular traps (NETs), which consist of modified chromatin decorated with bactericidal proteins from granules and cytoplasm. Various pathogens, antibodies and immune complexes, cytokines, microcrystals, and other physiological stimuli can cause NETosis. Induction of NETosis depends on reactive oxygen species (ROS), the main source of which is NADPH oxidase. Activation of NADPH oxidase depends on increase in the concentration of Ca2+ in the cytoplasm and in some cases on the generation of ROS in mitochondria. NETosis includes release of the granule components into the cytosol, modification of histones leading to chromatin decondensation, destruction of the nuclear envelope, as well as formation of pores in the plasma membrane. In this review, basic mechanisms of NETosis, as well as its role in the pathogenesis of some diseases including COVID-19 are discussed.
Similar content being viewed by others

INTRODUCTION
Neutrophils are the largest population of myeloid leukocytes, which normally comprise 50-70% of all white blood cells. Neutrophils differentiate in the bone marrow from hematopoietic stem cells and, after full maturation, enter the bloodstream. Neutrophils circulate in the bloodstream for no more than 72 h, thereupon, they either return to the bone marrow to be phagocytosed by resident macrophages, or undergo apoptosis in peripheral tissues, where they are also phagocytized. When the host organism is infected, neutrophils immediately migrate from the bloodstream to the site of infection providing a “first line” of defense against pathogens.
Being “professional” phagocytes, neutrophils contain a huge amount of antimicrobial “weaponry” in their granules that allows them to destroy pathogens in the process of phagocytosis. Bactericidal enzymes can be also released from the cells during degranulation. Activation of NADPH oxidase leads to mass generation of reactive oxygen species (ROS), which are involved in the destruction of pathogens both inside the phagosomes and outside the cells. Finally, there is another antimicrobial mechanism representing the release of neutrophil extracellular traps (NETs), which consist of modified chromatin “decorated” with bactericidal proteins from granules and cytoplasm. This phenomenon was first described in the work of Takei and co-workers [1] and subsequently characterized in detail in the laboratory of Arturo Zychlinsky [2]. Since it was initially shown that NET formation is accompanied by the cell death, this process was called NETosis [3].
Formation of NETs can be activated by various pathogens, such as bacteria, fungi, protozoa, viruses, as well as bacterial cell wall components – lipopolysaccharides (LPS). NETosis can be induced by antibodies and immune complexes, cytokines and chemokines (IL-8, TNF), microcrystals, and other physiological stimuli [4-8]. In order to induce NETosis in in vitro experiments, phorbol esters (in particular, phorbol-12-myristate-13-acetate, PMA), which mimic the action of diacylglycerol activating protein kinase C, as well as calcium (ionomycin, A23187) and potassium (nigericin) ionophores are often used.
Currently, two fundamentally different forms of NETosis have been described: classical or suicidal NETosis, which leads to the cell death, and vital NETosis, in which the cell retains not only viability, but also many of its effector functions (see below).
Classical NETosis is a special form of programmed cell death (PCD), which is characterized by the release of granule components into the cytosol, as well as chromatin decondensation associated with histone modification. At the same time, many features characteristic of other forms of PCD (apoptosis, necroptosis, pyroptosis, autophagy, secondary necrosis) are also inherent in NETosis. During NETosis, like in apoptosis, coordinated changes in the nucleus and in the cytoplasm occur, although the nature of the changes is different, and NETosis, unlike apoptosis, does not require activation of caspases. Unlike apoptosis, NETosis (as the other forms of PCD) is accompanied by disturbance of insulating properties of the plasma membrane, and the mechanisms of permeabilization are similar for NETosis, pyroptosis, and necroptosis. The signaling mechanisms of NETosis may include activation of phosphoinositide-3-kinase (PI3K) [9], which also controls the autophagy induction, but assembly of autophagosomes is not required for NETosis [10]. The pathways leading to NETosis and necroptosis can be especially closely intertwined [11-13]. For a long time, it was believed that mitochondria do not play a significant role in the functioning of neutrophils, since their content in these cells is low, energy supply is supported by glycolysis, and NADPH oxidase is the main source of ROS. Subsequently, however, it turned out that mitochondria are involved in the transmission of signals that determine main responses of the neutrophils to pathogens [14]. It was found that mitochondrial ROS are involved in the activation of NADPH oxidase and in the induction of NETosis caused by various stimuli [15, 16].
NETs formation has also been shown in other types of immune cells – eosinophils and mast cells [17], basophils [18], monocytes [19], and macrophages [20]. Interestingly, decondensed chromatin is not only used by animals for protection from pathogens, but also by unicellular eukaryotes [21], as well as plants [22]. Thus, it can be assumed that the use of chromatin to protect the host against pathogens arose quite early in the course of evolution of eukaryotes.
In recent years, data has accumulated on the role of NETosis in a wide range of pathologies associated with inflammatory processes. This led to a surge in publications about NETosis. Almost 3,000 publications on this topic can be found in the PubMed database, of which about a third appears in 2018-2020. Such intensive studies resulted in significant advances in understanding the nature of NETosis, but at the same time have led to the accumulation of data that contradict each other. In this review, we attempted to consider basic concepts of the mechanisms of NETosis, which determine its place among other forms of PCD. In addition, we briefly discuss the role of NETosis in pathogenesis of certain diseases.
MECHANISMS OF NETs FORMATION
Participation of ROS produced by NADPH oxidase and mitochondria in the induction of NETosis. As was shown in the first classical studies of A. Zychlinsky and co-workers [23], NETosis caused by Staphilococcus aureus or PMA depended on ROS produced by NADPH oxidase. Interestingly, addition of exogenous ROS to the neutrophils from patients with chronic granulomatous disease (CGD), for which absence of NADPH oxidase was typical, promoted NET formation [23]. The main mechanism of NADPH oxidase activation is associated with phosphorylation of its subunits by protein kinase C (PKC), which leads to the assembly of the active enzyme on the membrane [24]. Other kinases c-Raf, MEK, Akt, and ERK, together with PKC contributed to activation of NADPH oxidase during NETosis caused by Helicobacter pylori [25]. NETosis induced by the parasite Entamoeba histolytica was also dependent on activation of the c-Raf-MEK-ERK kinase cascade, but PKC was not involved [26]. Interestingly, the c-Raf-MEK-ERK signaling cascade, as well as PKC stimulates expression of Mcl-1, the main anti-apoptotic protein of neutrophils [25]. Apparently, induction of NETosis can be associated with suppression of apoptosis, which enhances the overall antimicrobial effect.
The main mechanisms of NADPH oxidase activation during NETosis are probably not so much different from those that provide an oxidative burst of neutrophils in response to pathogens and other stimuli. We found in the course of investigation of activation of NADPH oxidase by the peptide chemoattractant N-formylmethionyl-leucyl-phenylalanine (fMLP), which caused oxidative burst and degranulation but not NETosis, that mitochondria played an important role in these processes. Mitochondria-targeted antioxidant SkQ1 in submicromolar concentrations prevented activation of NADPH oxidase induced by fMLP but not by PMA [15]. Mitochondrial ROS (mtROS) stimulated NADPH oxidase with participation of PKC, but the primary target of their action remained unknown. This may be the PKC itself, which has two redox-sensitive sulfur-zinc clusters in the diacylglycerol-binding domain. In addition, some members of the Src kinase family (in particular, Lyn kinase), which stimulate PKC via phosphorylation of its tyrosine residues, are activated by ROS [27]. Another redox-sensitive mechanism of NADPH oxidase activation in neutrophils is based on the ROS-dependent association of the disulfide isomerase protein with the p47phox subunit, which leads to its translocation to the membrane with subsequent assembly of NADPH oxidase [28].
Activation of NADPH oxidase by mtROS was first demonstrated by Dikalov and co-workers [29] in endothelial cells. They showed that mitochondria-targeted antioxidant MitoTEMPO and expression of mitochondrial superoxide dismutase SOD2 prevented NADPH oxidase activation caused by the hormone angiotensin II, which stimulated hypertension. Subsequent studies showed that mtROS in the endothelium stimulated only one of the four isoforms of NADPH oxidase – NOX2 [30], and this isoform was typical for neutrophils. In neutrophils, the NADPH oxidase activation by myxotiazole, an inhibitor of complex III of the respiratory chain, which stimulated production of mtROS, was described [31]. In our study [15], an increase in mtROS and activation of NADPH oxidase was caused by a signal from the G-protein-coupled fMLP receptor, which initiated the release of Ca2+ from intracellular reticulum, as well as Ca2+-independent activation of PI3K. Both of these signaling pathways are apparently important for the receptor-mediated activation of NADPH oxidase in neutrophils [27].
The Ca2+-dependent generation of mtROS could serve as a predominant source of ROS in the case of NETosis induction by Ca2+ ionophores (A23187 or ionomycin) [32] and some other stimuli [33, 34]. These observations promote the concept of two different mechanisms of NETosis, one of which is independent of NADPH oxidase (see, the review [5]). However, mtROS can contribute to the initiation of NETosis due to stimulation of NADPH oxidase. For example, as was shown in our recent work [16], NETosis induced by A23187 was inhibited both by the mitochondria-targeted antioxidant SkQ1 and specific NADPH oxidase inhibitors. At the same time, we also showed that in neutrophils isolated from the blood of patients with X-linked CGD formation of NETs in response to A23187 depended on the enhanced generation of mtROS without participation of NADPH oxidase [16]. We suggest that in the NADPH oxidase-deficient neutrophils, mtROS are formed with increased intensity due to excessive accumulation of Ca2+ [35] and this is enough to trigger NETosis. The uncontrolled influx of Ca2+ into the cytoplasm of CGD neutrophils is apparently due to the lack of electrogenic function of NADPH oxidase and membrane depolarization upon activation [36].
Our studies demonstrated that generation of mtROS caused by both fMLP and A23187 depended on opening of the non-selective mitochondrial permeability transition pore (mPTP) [16]. This phenomenon went unnoticed for a long time, probably due to the fact that the most well-known mPTP inhibitor cyclosporin A (CsA) was also an inhibitor of cytoplasmic phosphatase calcineurin involved in the transmission of numerous Ca2+-dependent signals [37]. In our study, we used the mPTP inhibitors sangliferin A and bongkrekic acid, which did not affect calcineurin. Interestingly, fMLP did not cause significant decrease in the mitochondrial membrane potential and mitochondrial swelling characteristic of the prolonged opening of mPTP. We assume that this short-term increase in cytoplasmic Ca2+ caused by fMLP induced temporal reversible pore opening. This mPTP opening mode has been described both in isolated mitochondria [37] and in cell models [38]. Signalling function of the mPTP opening and associated production of mtROS have been previously described in the endothelial cells [30] and in neutrophils treated with mixotiazole [31].
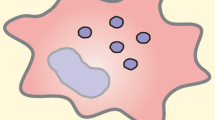
NETosis caused by A23187 was also dependent on the opening of mPTP [16]. In this case, electron microscopy revealed a significant swelling of mitochondria, which was accompanied by chromatin decondensation and destruction of the nuclear envelope (Fig. 1).

Electron microscopy of neutrophils in the early stages of NETosis. a, b) Intact human neutrophil; c and d) neutrophil stimulated with 2 µM A23187 for 30 min. Chromatin decondensation, characteristic of NETosis, and swelling of mitochondria were observed simultaneously indicating opening of the non-selective mitochondrial pore, mPTP. Scale bars: 2 µm (a, c) and 500 nm (b, d) [16].
It can be assumed that the significant increase in cytoplasmic Ca2+ induced by A23187 caused a prolonged opening of the pore. Ca2+-dependent opening of the mPTP stimulated formation of mtROS, while mPTP inhibitors prevented their accumulation [16]. The direct cause of excessive formation of mtROS was probably related to the release of the main components of antioxidant defense, such as NADPH [38] and reduced glutathione [16] from mitochondria. Along with Ca2+, oxidative stress is an effective inducer of the mPTP opening [37]. It is possible that the ROS formed by NADPH oxidase penetrate the cell, thus stimulating opening of the mPTP and creating an amplification loop leading to NETosis (Fig. 2).

Scheme illustrating the mechanisms of NETosis induced by various stimuli. NETosis caused by the calcium ionophore A23187 starts with the mobilization of Ca2+ from the endoplasmic reticulum (ER), which leads to the activation of CRAC channels located in the cytoplasmic membrane, and the entry of extracellular Ca2+ into the cytoplasm. In addition, A23187 catalyzes the transfer of Ca2+ through the plasma membrane into the cytoplasm. Subsequent accumulation of Ca2+ in the mitochondrial matrix leads to the activation of non-selective mitochondrial pores (mPTP) and the formation of mitochondrial reactive oxygen species (mtROS). Along with Ca2 + overload, oxidative stress is also an inducer of the mPTP. mtROS released from the mitochondria into the cytosol activate NADPH oxidase apparently with the participation of protein kinase C (PKC). PKC can be activated with the phorbol ester (PMA), which induces NADPH oxidase and NETosis independently of mtROS and the mPTP. NADPH oxidase can be also activated by a chemoattractant N-formylmethionyl-leucyl-phenylalanine (fMLP), which by binding to a specific receptor activates phospholipase C (PLC) to stimulate the formation of diacylglycerol (DAG) and inositol triphosphate (IP3) from the phosphatidylinositol 4,5-bisphosphate. The activation of NADPH oxidase in this case depends on mtROS and on the opening of mPTP. For reasons not fully understood, fMLP does not induce NETosis [16]. (Color version of the figure is available in online version of the article and can be accessed at: https://www.springer.com/journal/10541)
Opening of the mitochondrial pore has long been considered as one of the steps in the apoptosis program [39]. Initially, it was assumed that the mPTP opening resulted in swelling of the matrix, rupture of the outer mitochondrial membrane, and exit of proapoptotic proteins (in particular, cytochrome c) from the intermembrane space into the cytoplasm. Later, this hypothesis was modified taking into account the data on the release of cytochrome c through protein pores in the membrane. It was assumed that opening of the mPTP promotes change in the morphology of the inner membrane and release of cytochrome c from the space inside the cristae [40]. The details of this mechanism remain unclear, but there is no doubt that specific pore inhibitors prevent apoptosis in various models. The mPTP opening is also involved in the induction of necrotic death. In particular, mPTP opening contributes to the necrosis induced by ischemia/reperfusion of the heart, and its critical role has been confirmed by the protective effect of the pore inhibitors [41]. These data allow us to place NETosis induced by calcium ionophores into the family of mPTP-dependent PCD mechanisms. The mtROS-dependent activation of NADPH oxidase during NETosis, which is often referred to as “NADPH oxidase-independent”, indicates that it seems more accurate to call it “mitochondria-dependent NETosis”.
MECHANISMS OF NETosis
An important event in NETosis is the release of some proteins from granules into the cytosol. Azurophil granules contain the protein complex “azurosome”, which includes eight types of proteins, three of them are highly homologous serine proteases – neutrophilic elastase (NE), cathepsin G and azurocidin, and also myeloperoxidase (MPO), an enzyme that produces hypochlorite anion using chlorine and hydrogen peroxide as substrates. It was shown that ROS cause dissociation of azurosomes, which led to the release of serine proteases and MPO from the granules into the cytosol [42]. Serine proteases (primarily, NE) break down cytoskeletal elements contributing to realization of NETosis [43]. Subsequently, they migrate to the nucleus, where they break down the lamin and histones contributing to the chromatin decondensation and destruction of the nuclear envelope. MPO plays an important role in dissociation of the azurosome and release of the proteases from the granules [42, 44]. Interestingly, enzymatic activity of MPO is not required at this stage. It is likely that this heme-containing protein serves as an intracellular hydrogen peroxide receptor. However, MPO activity is required for NETosis, since hypochlorite anion stimulates activity of neutrophil elastase [42]. It is worth noting that the ROS-dependent release of proteins from the granules during NETosis is in many ways similar to the ROS-dependent permeabilization of lysosomes and release of cathepsins from them, which is typical for many variants of necrosis [45].
Additionally, peptidyl-arginine deaminase 4 (PAD4) is transferred from the cytoplasm into the nucleus to catalyze citrullination of histones, which leads to chromatin decondensation. Inhibition of PAD4 prevented chromatin decondensation and NETosis caused by Ca2+ ionophores or Shigella flexneri, and neutrophils isolated from the PAD4 knockout mice did not form NETs in response to PMA [46]. Peptidyl-arginine deaminases are Ca2+-binding proteins and their activity is stimulated by Ca2+. On the other hand, PAD4 is activated and causes histone citrullination in response to the addition of hydrogen peroxide [46]. Moreover, LPS-related citrullination of histones and NETosis depend on the intactness of microtubules [47]. Apparently, combination of all these factors is necessary for activation of PAD4. Along with citrullination, histones can also undergo acetylation during NETosis, but its role in this process is still poorly understood [5]. Chromatin decondensation, as well as proteolytic damage of the nuclear lamina leads to the destruction of the nuclear envelope, and release of chromatin into the cytoplasm. Recently, it has been shown that NETosis can occur due to the activation of cyclin-dependent kinases (CDKs), which facilitate entry into the cell cycle [48]. It is possible that parts of the mitosis apparatus, such as lamina phosphorylation and centrosomes separation are used to destroy nuclear envelope during NETosis.
At the final stage of NETosis, pores are formed in the plasma membrane and chromatin is released into the environment with NETs formation. Proteins released from the granules are strongly bound to the decondensed chromatin due to electrostatic interaction. The pores that allow this giant complex to pass through are formed by the gasdermin D protein (GSDMD), which also forms pores in the macrophage membrane during pyroptosis. Unlike pyroptosis, where GSDMD is activated through the cleavage by caspase-1 and -4/5 (caspase-11, in mice), during NETosis it is cleaved and activated mainly by neutrophil elastase [49, 50]. Activation of GSDMD probably leads to the formation of pores not only in the plasmalemma, but also in the nuclear membrane [51]. Caspase-dependent activation of GSDMD in neutrophils can also occur as a result of noncanonical activation of the inflammasome [51], but the role of this mechanism in NETosis requires further investigations. Gasdermin E, related to GSDMD, is activated by caspase-3 leading to permeabilization of mitochondria and promotion of apoptosis, as well as secondary necrosis [52, 53]. Another pore-forming protein MLKL (not related to gasdermins) is activated by RIP kinases during necroptosis. Activation of MLKL in neutrophils can also lead to the release of NETs [11-13].
Physiological modulation of NETosis. Under physiological conditions, the ratio of CO2/HCO3– concentrations, pH, and O2 content can modulate NETosis. Under moderately alkaline conditions and at reduced CO2/HCO3– ratio, the level of NETosis caused by PMA, Ca2+ ionophore, uric acid microcrystals, or LPS was increased [54]. An increase of pH in neutrophil cytoplasm caused a raise in the concentration of Ca2+ and enhanced production of ROS by both NADPH oxidase and mitochondria [55]. A decrease of pH in the medium causes inhibition of NETosis, possibly due to inhibition of glycolysis [56]. In addition, at low pH, probability of the mPTP opening is sharply reduced [37], which could lower production of mtROS [16]. It is assumed that pH dependence of NETosis leads to the fact that it is maximally activated on the periphery of inflammatory lesion protecting the tissue from pathogens, while in the center of the lesion, which is characterized by low pH, NETosis is weakened and does not enhance tissue damage [54]. Information on the effect of hypoxia on NETosis is controversial. From the one hand, knockout of Hif-1α (the main transcription factor regulating adaptation to hypoxia) suppressed NETosis, while pharmacological stabilization of Hif-1α stimulated it [57]. On the other hand, NETosis induced by PMA (but not S. aureus) decreased with hypoxia, and this effect was not dependent on Hif-1α [58]. In addition to the composition of the medium, NETosis depends on its osmolarity, therefore, the hypertonic medium suppressed ROS production and NETosis. The ROS level in this case was critical, since the addition of hydrogen peroxide restored NETosis [59].
Cytokines and inflammatory mediators play an important role in the activation of NETosis, while at the same time some anti-inflammatory substances can cause the opposite effect. Thus, prostaglandin E2, which plays an important role in resolving inflammation, inhibits NETosis due to increase in the intracellular content of cyclic AMP [60, 61]. Activated C protein (a serine proteinase with anti-thrombotic and anti-inflammatory effects) can also inhibit NETosis by binding to a specific receptor (EPCR) or by interacting with protease-activated receptor 3 (PAR3) and CD11b/CD18 integrins (Mac-1). Interestingly, the same activated C protein can cleave histones that are part of NETs [62]. It has been shown that NETosis is suppressed by the important anti-inflammatory cytokine IL-10 [63]. Peptides that effectively suppress NETs formation have been found in the cord blood. The most common peptide is called the “neonatal NETs inhibitory factor” (nNIF). This peptide selectively inhibited NETosis without affecting phagocytosis and other neutrophil functions. Its intravenous administration protected mice from systemic inflammation caused by LPS and from microbial sepsis [64].
Pathogenic microorganisms have a wide range of tools that interfere with the microbicidal action of NETs [65]. Many microorganisms produce lytic enzymes (primarily, endonucleases) that destroy NETs. Bacteria, such as Pseudomonas aeruginosa, Mycobacterium tuberculosis, as well as fungi of the Aspergillus genus produce protective and masking extracellular envelops. In the case of P. aeruginosa, coating with sialic acids induces production of IL-10, which suppresses NETosis. The same mechanism appears to be used by the human immunodeficiency virus (HIV-1). HIV-1 virions stimulate production of IL-10 by dendritic cells, which protects the virus from the lytic action of NETs enzymes [63]. Hepatitis B virus (HBV) inhibits NETosis by suppressing production of ROS in neutrophils using the HBE envelope protein and HBC core protein [66].
VITAL NET RELEASE
Along with the suicidal NETosis described above, there are also mechanisms of DNA release, when neutrophils retain their viability and natural effector functions (for a review, see [6]). The term “vital NETosis” was used to describe these processes. However, the Cell Death Nomenclature Committee in 2018 [67] did not recommend to use the term NETosis for processes not associated with cell death. The vital release of chromatin was first described in a system where neutrophils were present together with platelets activated by LPS via TLR4 [68]. NETosis, in this case, occurred much faster than when induced by PMA, and the role of NADPH oxidase and ROS was not studied. Unfortunately, this interesting model, which has obvious physiological significance, has not been investigated further. A similar vital release of chromatin was observed in vivo when the skin was infected with gram-positive bacteria [69]. Induction of NETosis in this case required opsonization of bacteria, interaction with TLR2, and activation of the complement system. Interestingly, after NETosis, nuclear-free neutrophils were capable for chemotaxis and phagocytosis of bacteria.
Massive and very fast release of mitochondrial DNA (mtDNA) without loss of viability was observed in eosinophils and neutrophils primed with pro-inflammatory cytokines IL-5/IFN-γ or GM-CSF, respectively, and stimulated with LPS [70, 71]. In both types of granulocytes, this process was dependent on the activity of NADPH oxidase. A similar phenomenon was observed in the case of basophils [18]. Recently, the vital mtDNA release was discovered in B and T lymphocytes, as well as in natural killer cells (NK cells) in response to oligodeoxynucleotides [72]. Unlike granulocytes, the release of mtDNA from lymphocytes was not dependent on NADPH oxidase. The question of the functional role of extracellular mtDNA remains open. Low content of mitochondria in neutrophils and, especially, in eosinophils makes formation of the functional NETs extremely unlikely. In the case of lymphocytes, extracellular mtDNA did not contain lytic enzymes and most likely performed a signaling function. In particular, mtDNA stimulated expression and secretion of the type I interferons by peripheral blood mononuclear cells [72]. It should be noted that extracellular mtDNA (usually, oxidized) is found in the blood at a wide range of pathologies including systemic lupus erythematosus, an autoimmune disease in the pathogenesis of which NETosis plays an important role [33].
THE ROLE OF NETosis IN HOST DEFENCE AND PATHOLOGY
In the first studies on NETosis, physiological protective role of this phenomenon was suggested. In particular, structures similar to NETs were found in the contents of the appendix [2]. Later, NETs were found in numerous organs and tissues [6], however, the question of its protective effect remains open. NETosis is observed in foci of infections and, apparently, slows down the spread of pathogens. Thus, it has been shown that NETs in the staphylococcal skin infections inhibits penetration of the pathogens into the bloodstream [69]. Mice that are not capable of NETosis due to knockout of the PAD4 gene suffered more significantly from necrotic fasciitis caused by the group A Streptococcus pyogenes [46]. Undoubtedly, excessive formation of NETs associated with both increased NETosis and defects in the mechanisms for their elimination can lead to inflammatory and autoimmune pathologies, as well as to vascular or duct occlusion.
NETosis on the surface of epithelium. Microorganisms constantly attack epithelial barriers inducing formation of NETs on the surface of eyes, oral mucosa, and skin. Therefore, formation of NETs and their degradation must be strictly regulated to avoid inflammation in these tissues. A number of diseases have been described in which NETs play both antimicrobial and pathogenetic role.
On the surface of the eye cornea, NETosis is involved in the protection against both bacterial and fungal infections. In patients with severe NETosis, fungal keratitis progressed much easier [73], while keratitis caused by clinical isolates of P. aeruginosa was exacerbated by NETosis in the mouse model [74]. In the case of sterile inflammation of the cornea during dry eye syndrome, NETs accumulation was also observed [75]. One of the reasons for NETosis could be the increased osmolarity of the lacrimal fluid washing the cornea in patients with dry eye syndrome [76]. Dry eye syndrome, which often occurs as a manifestation of the “graft versus host” reaction after bone marrow transplantation [77], and Sjogren’s autoimmune syndrome [78] are also characterized by accumulation of NETs in the lacrimal fluid. Interestingly, the mitochondria-targeted antioxidant SkQ1 (an acting component of the eye drops “Visomitin”) was proven to be highly effective in the treatment of dry eye syndrome of various etiologies [79]. It can be assumed that this effect of SkQ1 is partly related to the suppression of NETosis described in our study [16].
The role of NETosis in thrombosis. NETosis plays an important role in the pathogenesis of thrombosis of various origin [80, 81]. For example, in the model of stenosis of the inferior vein cava probability of thrombosis was significantly reduced in the PAD4 knockout mice [82]. The role of NETs in thrombosis involves interaction with endothelium and platelets, as well as capture of small blood clots. NETosis apparently underlies thrombosis associated with excessive innate immunity reactions (“immunothrombosis”) [83]. Immunothrombosis, presumably, is a protective reaction of the body against pathogens, facilitating their capture in a fibrin clot. In addition, small blood vessel thrombi can create compartments, where pathogens can be effectively destroyed. However, consequences of such reaction can be tragic. A recent large-scale clinical study revealed correlation between the level of NETosis and the severity of ischemic stroke and myocardial infarction [84]. NETosis can be activated by microcrystals of cholesterol and participate in the pathogenesis of atherosclerosis. Histones in the NETs cause TLR4-dependent activation of macrophages and release of cytokines that activate T-helper cells (Th17) [85, 86]. The inflammatory process in atherosclerotic plaques can be one of the causes of thrombosis [87]. Oncological diseases could be another cause of thrombosis, and NETosis is believed to be involved in this case [87]. On the other hand, therapeutic viral infection of tumors induces neutrophil-dependent intratumoral coagulation and death of cancer cells. However, it remains to be elucidated, whether this process is really caused by NETosis [88]. Thrombosis, which is characteristic of various viral infections, could be associated with excessive NETosis and appears to be involved in the pathogenesis of COVID-19 (see below).
In the pancreatic ducts, NETosis can be caused by microcrystals of calcium carbonate, which leads to blockage of the pancreatic duct and pancreatitis [89]. Such crystals cause NETosis in the bile ducts and in the gallbladder, which can lead to the formation of gallstones [90].
The role of NETosis in the development of pulmonary diseases. In the respiratory tract, NETosis contributes to the protection against infection by increasing viscosity of the mucus and by destruction of pathogens. However, many of pathogens (in particular, Streptococcus pneumoniae, Haemophilus influenzae) produce endonucleases that break down NETs and protect the bacteria (see review [91]). At the same time, NETosis contributes to the development of complications of the lungs infectious diseases, including acute respiratory distress syndrome (ARDS), chronic obstructive pulmonary disease (COPD), as well as bronchial asthma, etc. The recent clinical trial (conducted prior to the onset of the COVID-19 pandemic) showed correlation between the NETs content and severity of the community-acquired pneumonia [92]. Acute lung injury (ALI) and ARDS of various etiologies are accompanied by excessive NETosis (see review [93]). NETs in these pathologies may be involved in the damage of alveolar epithelium and endothelium. COPD, which is usually associated with smoking and air pollution, and severe “neutrophilic” asthma are also characterized by accumulation of NETs in the sputum and respiratory tract lavage [94]. Rhinovirus infection in patients with asthma significantly increased NETs content [95]. In asthma, formation of the chromatin-containing traps can also occur due to the death of eosinophils, which is similar to NETosis [96].
The severe acute respiratory infection COVID-19 (Coronavirus Disease-19), which broke out in December 2019 in the Chinese city of Wuhan and subsequently escalated into a pandemic, has affected up to now more than 15 million people from 250 countries. The disease was caused by a new coronavirus called SARS-CoV-2 (severe acute respiratory syndrome coronavirus2), and was accompanied by viral pneumonia often progressing to ARDS and multiple organ failure. Elevated levels of neutrophils in the blood indicate severity of the disease and poor prognosis [97]. Examination of the patients infected with SARS-CoV-2 revealed an increased level of NETosis markers (cell-free DNA, MPO-DNA complexes, and citrullinated histone H3) and the marker of cell death – lactate dehydrogenase [98]. Concentration of the cell-free DNA correlated with the content of neutrophils, C-reactive protein (marker of the acute phase of inflammation), and the D-dimer (marker of thrombosis). Serum from the patients with COVID-19 induced NETosis in the healthy donor blood in the in vitro system. One of the manifestations of COVID-19 is Kawasaki syndrome, vasculitis that occurs in children, which is accompanied by excessive NETosis [99]. NETosis in COVID-19 can be caused by epithelial and endothelial cells affected by the virus, by activated platelets, and by inflammatory cytokines. At the same time, excessive NETosis is involved in the development of the “cytokine storm” and thrombosis, which are main indicators of the severe course of COVID-19 [100].
NETosis and autoimmune diseases. Many NET components, in particular, double-stranded DNA, granule proteins, and histones, can stimulate production of antibodies and development of autoimmune diseases. For the first time, involvement of NETosis in pathogenesis of autoimmune diseases was studied in detail for systemic lupus erythematosus (see review [101]). A special form of granulocytes called “low density granulocytes” appears in the blood during this disease. These cells produce more inflammatory cytokines (including type I interferons) and are more involved NETotsis than the normal neutrophils. Their NETs contain more autoantigens and oxidized mitochondrial DNA [33], which makes them stronger immunostimulants. One of the peculiarities of low-density granulocytes is the increased production of mitochondrial ROS. Recently, it was shown that the mitochondria-targeted antioxidant MitoQ (similar in structure to SkQ1) suppressed NETs accumulation and pathological manifestations in the mouse model of systemic lupus erythematosus [102].
In rheumatoid arthritis (RA), the development of pathology correlated with accumulation of the NETosis markers, such as DNA-MPO complexes and antibodies against citrullinated histones [103, 104]. In addition, it was found that NETs engulfed by fibroblasts stimulated formation of the antibodies against citrullinated histones in the RA model [105]. Similar observations indicate involvement of NETosis in the autoimmune diseases, such as vasculitis associated with “anti-neutrophil antibodies” (AAV), antiphospholipid syndrome, multiple sclerosis, and psoriasis (see review [106]). Interestingly, in some diseases, NETosis can play an anti-inflammatory role. For example, during the gout attacks, NETosis induced by uric acid crystals is accompanied by the release of lytic enzymes that break down proinflammatory cytokines in the foci of inflammation. It is believed that NETosis in gout prevents development of the chronic disease [107].
THERAPY OF NETosis
Evidences for involvement of NETosis in various pathologies has led to intensive study and testing of various therapeutic approaches. One approach includes the use of drugs that prevent NETosis. It comprises anticytokine therapy aimed to prevent accumulation of neutrophils in the foci and their activation, as well as applying inhibitors of the components involved in NETosis program: NE, PAD4, and GSDMD. Another approach is based on the destroying of NETs or attenuating their damaging effects. Anticytokine therapy directed against IL-1β is widely used in various inflammatory and autoimmune diseases. One of its targets may be excessive NETosis. The recombinant anakinra protein, an IL-1β receptor antagonist, is currently undergoing clinical trials as a potential preparation to treat COVID-19 (https://clinicaltrials.gov: NCT04324021, NCT04330638, NCT02735707). Among the NETosis inhibitors, the trials of the NE inhibitors have been progressed the farthest. The first of these, sivelestat, was approved for treating ARDS in Japan and South Korea, but meta-analysis of the clinical data did not confirm its effectiveness [108]. New generation of NE inhibitors is currently only at the first stage of clinical trials. GSDMD and PAD4 inhibitors are at the preclinical stage of testing. Of great interest is the use of existing drugs for inhibition of NETosis. So, disulfiram, which is used to treat alcoholism, inhibits GSDMD activation and protects mice in the lethal LPS-induced sepsis model [109]. It should be noted that GSDMD is also a critical component of the pyroptosis program and the authors of the study attribute its effect to the prevention of macrophage pyroptosis. The in vitro experiments have shown that NETosis can be prevented by microtubule inhibitors [47]. This group of drugs includes colchicine, and the clinical trials testing efficacy of colchicine against COVID-19 are currently underway (https://clinicaltrials.gov: NCT04326790, NCT04328480, NCT04322565, NCT04322682).
Among the drugs aimed to destroy NETs, DNase I and anti-histone antibodies are the most studied. Recombinant DNase I has been successfully used in almost all models of pathologies associated with NETosis. In particular, introduction of DNase I significantly facilitates the course of ARDS [93] and COPD [94] in animal models. In patients with cystic fibrosis, DNase inhalation improved lung function, and neutrophil elastase facilitated sputum dissolution making it more accessible for DNase [110]. Clinical trials of actin-resistant DNase (PRX-110) go through the second phase and give encouraging results (https://clinicaltrials.gov: NCT02605590, NCT02722122). It is possible to hope that DNase will not only liquefy sputum, but will also interrupt the progression of ARDS, as was observed in animal experimental models.
Our experiments with the mitochondria-targeted antioxidant SkQ1 have shown its potential effectiveness against NETosis [16]. In the mouse model of systemic inflammatory syndrome, SkQ1 prevented lethal effect of the inflammatory cytokine TNF [111]. The antioxidant MitoQ, similar in structure to SkQ1, suppressed NETosis in the mouse model of systemic lupus erythematosus [102]. These results suggest, that drugs based on mitochondria-targeted antioxidants will be created soon in order to treat diseases associated with the excessive NETosis, and, in particular, to combat COVID-19.
CONCLUSION
The program for formation of neutrophil extracellular traps – NETosis – is being studied extensively, however, many questions regarding its mechanisms and physiological role remain open. First of all, this refers to the signaling mechanisms of the initiation of NETosis. In particular, the processes leading to chromatin modification and decondensation remain unclear. Targets for the mtROS action and details of the mtROS-dependent activation of NADPH oxidase have not yet been determined. Excessive NETosis has been suggested to play an important role in pathogenesis of many infectious, inflammatory, and autoimmune diseases, but there is no sufficient evidence to support this. A new impetus to study pathophysiological role of NETosis may be related to its putative role in the pathogenesis of COVID-19. The development of new drugs preventing NETosis, including mitochondria-targeted antioxidants, appears to be a promising area of pharmacological research.
Abbreviations
- ARDS:
-
acute respiratory distress syndrome
- CGD:
-
chronic granulomatous disease
- COPD:
-
chronic obstructive pulmonary disease
- GSDMD:
-
gasdermin D
- LPS:
-
lipopolysaccharide of the bacterial wall
- MPO:
-
myeloperoxidase
- mPTP:
-
nonselective mitochondrial permeability transition pore
- NE:
-
neutrophil elastase
- NETs:
-
Neutrophil Extracellular Traps
- PCD:
-
programmed cell death
- PKC:
-
protein kinase C
- PMA:
-
phorbol-12-myristate-13-acetate
- ROS:
-
reactive oxygen species
References
Takei, H., Araki, A., Watanabe, H., Ichinose, A., and Sendo, F. (1996) Rapid killing of human neutrophils by the potent activator phorbol 12-myristate 13-acetate (PMA) accompanied by changes different from typical apoptosis or necrosis, J. Leukoc. Biol., 59, 229-240, doi: https://doi.org/10.1002/jlb.59.2.229.
Brinkmann, V., Reichard, U., Goosmann, C., Fauler, B., Uhlemann, Y., et al. (2004) Neutrophil extracellular traps kill bacteria, Science, 303, 1532-1535, doi: https://doi.org/10.1126/science.1092385.
Steinberg, B. E., and Grinstein, S. (2007) Unconventional roles of the NADPH oxidase: signaling, ion homeostasis, and cell death, Sci. STKE, 379, pe11, doi: https://doi.org/10.1126/stke.3792007pe11.
Vorobjeva, N. V., and Pinegin, B. V. (2014) Neutrophil extracellular traps: mechanisms of formation and role in health and disease, Biochemistry (Moscow), 79, 1286-1296, doi: https://doi.org/10.1134/S0006297914120025.
Ravindran, M., Khan, M. A., and Palaniyar, N. (2019) Neutrophil extracellular trap formation: physiology, pathology, and pharmacology, Biomolecules, 9, 365, doi: https://doi.org/10.3390/biom9080365.
Yousefi, S., Simon, D., Stojkov, D., Karsonova, A., Karaulov, A., and Simon, H. U. (2020) In vivo evidence for extracellular DNA trap formation, Cell Death Dis., 11, 300, doi: https://doi.org/10.1038/s41419-020-2497-x.
Rada, B. (2017) Neutrophil extracellular traps and microcrystals, J. Immunol. Res., 2017, 2896380, doi: https://doi.org/10.1155/2017/2896380.
Pinegin, B., Vorobjeva, N., and Pinegin, V. (2015) Neutrophil extracellular traps and their role in the development of chronic inflammation and autoimmunity, Autoimmun. Rev., 14, 633-640, doi: https://doi.org/10.1016/j.autrev.2015.03.002.
Remijsen, Q., Vanden Berghe, T., Wirawan, E., Asselbergh, B., Parthoens, E., et al. (2011) Neutrophil extracellular trap cell death requires both autophagy and superoxide generation, Cell Res., 21, 290-304, doi: https://doi.org/10.1038/cr.2010.150.
Germic, N., Stojkov, D., Oberson, K., Yousefi, S., and Simon, H. U. (2017) Neither eosinophils nor neutrophils require ATG5-dependent autophagy for extracellular DNA trap formation, Immunology, 152, 517-525, doi: https://doi.org/10.1111/imm.12790.
Desai, J., Kumar, S. V., Mulay, S. R., Konrad, L., Romoli, S., et al. (2016) PMA and crystal-induced neutrophil extracellular trap formation involves RIPK1-RIPK3-MLKL signaling, Eur. J. Immunol., 46, 223-229, doi: https://doi.org/10.1002/eji.201545605.
Schreiber, A., Rousselle, A., Becker, J. U., von Mässenhausen, A., Linkermann, A., and Kettritz, R. (2017) Necroptosis controls NET generation and mediates complement activation, endothelial damage, and autoimmune vasculitis, Proc. Natl. Acad. Sci. USA, 114, E9618‐E9625, doi: https://doi.org/10.1073/pnas.1708247114.
D’Cruz, A. A., Speir, M., Bliss-Moreau, M., Dietrich, S., Wang, S., et al. (2018) The pseudokinase MLKL activates PAD4-dependent NET formation in necroptotic neutrophils, Sci. Signal., 11, eaao1716, doi: https://doi.org/10.1126/scisignal.aao1716.
Pinegin, B., Vorobjeva, N., Pashenkov, M., and Chernyak, B (2018) The role of mitochondrial ROS in antibacterial immunity, J. Cell. Physiol., 233, 3745-3754, doi: https://doi.org/10.1002/jcp.26117.
Vorobjeva, N., Prikhodko, A., Galkin, I., Pletjushkina, O., Zinovkin, R., et al. (2017) Mitochondrial reactive oxygen species are involved in chemoattractant-induced oxidative burst and degranulation of human neutrophils in vitro, Eur. J. Cell. Biol., 96, 254-265, doi: https://doi.org/10.1016/j.ejcb.2017.03.003.
Vorobjeva, N., Galkin, I., Pletjushkina, O., Golyshev, S., Zinovkin, R., et al. (2020) Mitochondrial permeability transition pore is involved in oxidative burst and NETosis of human neutrophils, Biochim. Biophys. Acta Mol. Basis. Dis., 1866, 165664, doi: https://doi.org/10.1016/j.bbadis.2020.165664.
Von Köckritz-Blickwede, M., Goldmann, O., Thulin, P., Heinemann, K., et al. (2008) Phagocytosis-independent antimicrobial activity of mast cells by means of extracellular trap formation, Blood, 111, 3070-3080, doi: https://doi.org/10.1182/blood-2007-07-104018.
Morshed, M., Hlushchuk, R., Simon, D., Walls, A. F., Obata-Ninomiya, K., et al. (2014) NADPH oxidase-independent formation of extracellular DNA traps by basophils, J. Immunol., 192, 5314-5323, doi: https://doi.org/10.4049/jimmunol.1303418.
Granger, V., Faille, D., Marani, V., Noël, B., Gallais, Y., et al. (2017) Human blood monocytes are able to form extracellular traps, J. Leukoc. Biol., 102, 775-781, doi: https://doi.org/10.1189/jlb.3MA0916-411R.
Chow, O. A., von Köckritz-Blickwede, M., Bright, A. T., Hensler, M. E., Zinkernagel, A. S., et al. (2010) Statins enhance formation of phagocyte extracellular traps. Statins enhance formation of phagocyte extracellular traps, Cell. Host Microbe, 8, 445-454, doi: https://doi.org/10.1016/j.chom.2010.10.005.
Zhang, X., Zhuchenko, O., Kuspa, A., and Soldati, T. (2016) Social amoebae trap and kill bacteria by casting DNA nets, Nat. Commun., 7, 10938, doi: https://doi.org/10.1038/ncomms10938.
Hawes, M., Allen, C., Turgeon, B. G., Curlango-Rivera, G., Minh Tran, T., Huskey, D. A., and Xiong, Z. (2016) Root border cells and their role in lant defense, Annu. Rev. Phytopathol., 54, 143-161, doi: https://doi.org/10.1146/annurev-phyto-080615-100140.
Fuchs, T. A., Abed, U., Goosmann, C., Hurwitz, R., Schulze, I., et al. (2007) Novel cell death program leads to neutrophil extracellular traps, J. Cell Biol., 176, 231-241, doi: https://doi.org/10.1083/jcb.200606027.
Lu, D. J., Furuya, W., and Grinstein, S. (1993) Involvement of multiple kinases in neutrophil activation, Blood Cells, 19, 343‐351.
Hakkim, A., Fuchs, T. A., Martinez, N. E., Hess, S., Prinz, H., Zychlinsky, A., and Waldmann, H. (2011) Activation of the Raf-MEK-ERK pathway is required for neutrophil extracellular trap formation, Nat. Chem. Biol., 7, 75-77, doi: https://doi.org/10.1038/nchembio.496.
Fonseca, Z., Díaz-Godínez, C., Mora, N., Alemán, O. R., Uribe-Querol, E., Carrero, J. C., and Rosales, C. (2018) Entamoeba histolytica induce signaling via Raf/MEK/ERK for neutrophil extracellular trap (NET) formation, Front. Cell. Infect. Microbiol., 8, 226, doi: https://doi.org/10.3389/fcimb.2018.00226.
Steinberg, S. F. (2015) Mechanisms for redox-regulation of protein kinase C, Front. Pharmacol., 6, 128, doi: https://doi.org/10.3389/fphar.2015.00128.
Trevelin, S. C., and Lopes, L. R. (2015) Protein disulfide isomerase and Nox: new partners in redox signaling, Curr. Pharm. Des., 21, 5951-5963, doi: https://doi.org/10.2174/1381612821666151029112523.
Dikalova, A. E., Bikineyeva, A. T., Budzyn, K., Nazarewicz, R. R., McCann, L., et al. (2010) Therapeutic targeting of mitochondrial superoxide in hypertension, Circ. Res., 107, 106-116, doi: https://doi.org/10.1161/CIRCRESAHA.109.214601.
Nazarewicz, R. R., Dikalova, A. E., Bikineyeva, A., and Dikalov, S. I. (2013) Nox2 as a potential target of mitochondrial superoxide and its role in endothelial oxidative stress, Am. J. Physiol. Heart Circ. Physiol., 305, H1131-1140, doi: https://doi.org/10.1152/ajpheart.00063.2013.
Kröller-Schön, S., Steven, S., Kossmann, S., Scholz, A., Daub, S., et al. (2014) Molecular mechanisms of the crosstalk between mitochondria and NADPH oxidase through reactive oxygen species-studies in white blood cells and in animal models, Antioxid. Redox Signal., 20, 247-266, doi: https://doi.org/10.1089/ars.2012.4953.
Douda, D. N., Khan, M. A., Grasemann, H., and Palaniyar, N. (2015) SK3 channel and mitochondrial ROS mediate NADPH oxidase-independent NETosis induced by calcium influx, Proc. Natl. Acad. Sci. USA, 112, 2817-2822, doi: https://doi.org/10.1073/pnas.1414055112.
Lood, C., Blanco, L. P., Purmalek, M. M., Carmona-Rivera, C., De Ravin, S. S., et al. (2016) Neutrophil extracellular traps enriched in oxidized mitochondrial DNA are interferogenic and contribute to lupus-like disease, Nat. Med., 22, 146-153, doi: https://doi.org/10.1038/nm.4027.
Kenny, E. F., Herzig, A., Krüger, R., Muth, A., Mondal, S., et al. (2017) Diverse stimuli engage different neutrophil extracellular trap pathways, Elife, 6, pii: e24437, doi: https://doi.org/10.7554/eLife.24437.
Vorobjeva, N. V., and Chernyak, B. V. (2020) NADPH oxidase modulates Ca2+-dependent formation of neutrophil extracellular traps, Vestn. Mosk. Univ. Ser. 16. Biol., 75 (in press).
Tintinger, G. R., Theron, A. J., Steel, H. C., and Anderson, R. (2001) Accelerated calcium influx and hyperactivation of neutrophils in chronic granulomatous disease, Clin. Exp. Immunol., 123, 254-263, doi: https://doi.org/10.1046/j.1365-2249.2001.01447.x.
Bernardi, P., Rasola, A., Forte, M., and Lippe, G. (2015) The mitochondrial permeability transition pore: channel formation by F-ATP synthase, integration in signal transduction, and role in pathophysiology, Physiol. Rev., 95, 1111‐1155, doi: https://doi.org/10.1152/physrev.00001.2015.
Dumas, J. F., Argaud, L., Cottet-Rousselle, C., Vial, G., Gonzalez, C., et al. (2009) Effect of transient and permanent permeability transition pore opening on NAD(P)H localization in intact cells, J. Biol. Chem., 284, 15117-15125, doi: https://doi.org/10.1074/jbc.M900926200.
Kroemer, G., Dallaporta, B., and Resche-Rigon, M. (1998) The mitochondrial death/life regulator in apoptosis and necrosis, Annu. Rev. Physiol., 60, 619-642, doi: https://doi.org/10.1146/annurev.physiol.60.1.619.
Scorrano, L., Ashiya, M., Buttle, K., Weiler, S., Oakes, S. A., Mannella, C. A., and Korsmeyer, S. J. (2002) A distinct pathway remodels mitochondrial cristae and mobilizes cytochrome c during apoptosis, Dev. Cell, 2, 55-67, doi: https://doi.org/10.1016/S1534-5807(01)00116-2.
Griffiths, E. J., and Halestrap, A. P. (1995) Mitochondrial non-specific pores remain closed during cardiac ischaemia, but open upon reperfusion, Biochem. J., 307, 93-98, doi: https://doi.org/10.1042/bj3070093.
Metzler, K. D., Goosmann, C., Lubojemska, A., Zychlinsky, A., and Papayannopoulos, V. (2014) A myeloperoxidase-containing complex regulates neutrophil elastase release and actin dynamics during NETosis, Cell. Rep., 8, 883-896, doi: https://doi.org/10.1016/j.celrep.2014.06.044.
Papayannopoulos, V., Metzler, K. D., Hakkim, A., and Zychlinsky, A. (2010) Neutrophil elastase and myeloperoxidase regulate the formation of neutrophil extracellular traps, J. Cell Biol., 191, 677-691, doi: https://doi.org/10.1083/jcb.201006052.
Metzler, K. D., Fuchs, T. A., Nauseef, W. M., Reumaux, D., Roesler, J., et al. (2011) Myeloperoxidase is required for neutrophil extracellular trap formation: implications for innate immunity, Blood, 117, 953-959, doi: https://doi.org/10.1182/blood-2010-06-290171.
Repnik, U., Hafner Česen, M., and Turk, B. (2014) Lysosomal membrane permeabilization in cell death: concepts and challenges, Mitochondrion, 19 Pt. A, 49-57, doi: https://doi.org/10.1016/j.mito.2014.06.006.
Li, P., Li, M., Lindberg, M. R., Kennett, M. J., Xiong, N., and Wang, Y. (2010) PAD4 is essential for antibacterial innate immunity mediated by neutrophil extracellular traps, J. Exp. Med., 207, 1853‐1862, doi: https://doi.org/10.1084/jem.20100239.
Neeli, I., Dwivedi, N., Khan, S., and Radic, M. (2009) Regulation of extracellular chromatin release from neutrophils, J. Innate Immun., 1, 194-201, doi: https://doi.org/10.1159/000206974.
Amulic, B., Knackstedt, S. L., Abu Abed, U., Deigendesch, N., Harbort, C. J., et al. (2017) Cell-cycle proteins control production of neutrophil extracellular traps, Dev. Cell, 43, 449-462.e5, doi: https://doi.org/10.1016/j.devcel.2017.10.013.
Kambara, H., Liu, F., Zhang, X., Liu, P., Bajrami, B., et al. (2018) Gasdermin D exerts anti-inflammatory effects by promoting neutrophil death, Cell Rep., 22, 2924-2936, doi: https://doi.org/10.1016/j.celrep.2018.02.067.
Sollberger, G., Choidas, A., Burn, G. L., Habenberger, P., Di Lucrezia, R., et al. (2018) Gasdermin D plays a vital role in the generation of neutrophil extracellular traps, Sci. Immunol., 3, eaar6689, doi: https://doi.org/10.1126/sciimmunol.aar6689.
Chen, K. W., Monteleone, M., Boucher, D., Sollberger, G., Ramnath, D., et al. (2018) Noncanonical inflammasome signaling elicits gasdermin D-dependent neutrophil extracellular traps, Sci. Immunol., 3, eaar6676, doi: https://doi.org/10.1126/sciimmunol.aar6676.
Rogers, C., Fernandes-Alnemri, T., Mayes, L., Alnemri, D., Cingolani, G., and Alnemri, E. S. (2017) Cleavage of DFNA5 by caspase-3 during apoptosis mediates progression to secondary necrotic/pyroptotic cell death, Nat. Commun., 8, 14128, doi: https://doi.org/10.1038/ncomms14128.
Rogers, C., Erkes, D. A., Nardone, A., Aplin, A. E., Fernandes-Alnemri, T., and Alnemri, E. S. (2019) Gasdermin pores permeabilize mitochondria to augment caspase-3 activation during apoptosis and inflammasome activation, Nat. Commun., 10, 1689, doi: https://doi.org/10.1038/s41467-019-09397-2.
Maueröder, C., Mahajan, A., Paulus, S., Gößwein, S., Hahn, J., et al. (2016) Ménage-à-Trois: the ratio of bicarbonate to CO2 and the pH regulate the capacity of neutrophils to form NETs, Front. Immunol., 7, 583, doi: https://doi.org/10.3389/fimmu.2016.00583.
Naah de Souza, C., Breda, L. C. D., Khan, M. A., de Almeida, S. R., Câmara, N. O. S., Sweezey, N., and Palaniyar, N. (2017) Alkaline pH promotes NADPH oxidase-independent neutrophil extracellular trap formation: a matter of mitochondrial reactive oxygen species generation and citrullination and cleavage of histone, Front. Immunol., 8, 1849, doi: https://doi.org/10.3389/fimmu.2017.01849.
Behnen, M., Möller, S., Brozek, A., Klinger, M., and Laskay, T. (2017) Extracellular acidification inhibits the ROS-dependent formation of neutrophil extracellular traps, Front. Immunol., 8, 184, doi: https://doi.org/10.3389/fimmu.2017.00184.
Lodge, K. M., Cowburn, A. S., Li, W., and Condliffe, A. M. (2020) The impact of hypoxia on neutrophil degranulation and consequences for the host, Int. J. Mol. Sci., 21, 1183, doi: https://doi.org/10.3390/ijms21041183.
Branitzki-Heinemann, K., Möllerherm, H., Völlger, L., Husein, D. M., de Buhr, N., Blodkamp, S., et al. (2016) Formation of neutrophil extracellular traps under low oxygen level, Front. Immunol., 7, 518, doi: https://doi.org/10.3389/fimmu.2016.00518.
Nadesalingam, A., Chen, J. H. K., Farahvash, A., and Khan, M. A. (2018) Hypertonic saline suppresses NADPH oxidase-dependent neutrophil extracellular trap formation and promotes apoptosis, Front. Immunol., 9, 359, doi: https://doi.org/10.3389/fimmu.2018.00359.
Domingo-Gonzalez, R., Martínez-Colón, G. J., Smith, A. J., Smith, C. K., et al. (2016) Inhibition of neutrophil extracellular trap formation after stem cell transplant by prostaglandin E2, Am. J. Respir. Crit. Care Med., 193, 186-197, doi: https://doi.org/10.1164/rccm.201501-0161OC.
Shishikura, K., Horiuchi, T., Sakata, N., Trinh, D. A., Shirakawa, R., Kimura, T., Asada, Y., and Horiuchi, H. (2016) Prostaglandin E2 inhibits neutrophil extracellular trap formation through production of cyclic AMP, Br. J. Pharmacol., 173, 319-331, doi: https://doi.org/10.1111/bph.13373.
Healy, L. D., Puy, C., Fernández, J. A., Mitrugno, A., Keshari, R. S., et al. (2017) Activated protein C inhibits neutrophil extracellular trap formation in vitro and activation in vivo, J. Biol. Chem., 292, 8616-8629, doi: https://doi.org/10.1074/jbc.M116.768309.
Saitoh, T., Komano, J., Saitoh, Y., Misawa, T., Takahama, M., Kozaki, T., et al. (2012) Neutrophil extracellular traps mediate a host defense response to human immunodeficiency virus-1, Cell Host Microbe, 12, 109-116, doi: https://doi.org/10.1016/j.chom.2012.05.015.
Yost, C. C., Schwertz, H., Cody, M. J., Wallace, J. A., Campbell, R. A., et al. (2016) Neonatal NET-inhibitory factor and related peptides inhibit neutrophil extracellular trap formation, J. Clin. Invest., 126, 3783-3798, doi: https://doi.org/10.1172/JCI83873.
Hahn, S., Giaglis, S., Chowdhury, C. S., Hösli, I., and Hasler, P. (2013) Modulation of neutrophil NETosis: interplay between infectious agents and underlying host physiology, Semin. Immunopathol., 35, 439‐453, doi: https://doi.org/10.1007/s00281-013-0380-x.
Hu, S., Liu, X., Gao, Y., Zhou, R., Wei, M., Dong, J., Yan, H., and Zhao, Y. (2019) Hepatitis B virus inhibits neutrophil extracellular trap release by modulating reactive oxygen species production and autophagy, J. Immunol., 202, 805-815, doi: https://doi.org/10.4049/jimmunol.1800871.
Galluzzi, L., Vitale, I., Aaronson, S. A., Abrams, J. M., Adam, D., et al. (2018) Molecular mechanisms of cell death: recommendations of the Nomenclature Committee on cell death 2018, Cell. Death Differ., 25, 486‐541, doi: https://doi.org/10.1038/s41418-017-0012-4.
Clark, S. R., Ma, A. C., Tavener, S. A., McDonald, B., Goodarzi, Z., et al. (2007) Platelet TLR4 activates neutrophil extracellular traps to ensnare bacteria in septic blood, Nat. Med., 13, 463-469, doi: https://doi.org/10.1038/nm1565.
Yipp, B. G., Petri, B., Salina, D., Jenne, C. N., Scott, B. N., et al. (2012) Infection-induced NETosis is a dynamic process involving neutrophil multitasking in vivo, Nat. Med., 18, 1386-1393, doi: https://doi.org/10.1038/nm.2847.
Yousefi, S., Gold, J. A., Andina, N., Lee, J. J., Kelly, A. M., et al. (2008) Catapult-like release of mitochondrial DNA by eosinophils contributes to antibacterial defense, Nat. Med., 14, 949-953, doi: https://doi.org/10.1038/nm.1855.
Yousefi, S., Mihalache, C., Kozlowski, E., Schmid, I., and Simon, H. U. (2009) Viable neutrophils release mitochondrial DNA to form neutrophil extracellular traps, Cell Death Dis., 16, 1438-1444, doi: https://doi.org/10.1038/cdd.2009.96.
Ingelsson, B., Söderberg, D., Strid, T., Söderberg, A., Bergh, A. C., et al. (2018) Lymphocytes eject interferogenic mitochondrial DNA webs in response to CpG and non-CpG oligodeoxynucleotides of class C, Proc. Natl. Acad. Sci. USA, 115, E478-E487, doi: https://doi.org/10.1073/pnas.1711950115.
Jin, X., Zhao, Y., Zhang, F., Wan, T., Fan, F., Xie, X., and Lin, Z. (2016) Neutrophil extracellular traps involvement in corneal fungal infection, Mol. Vis., 22, 944-952.
Shan, Q., Dwyer, M., Rahman, S., and Gadjeva, M. (2014) Distinct susceptibilities of corneal Pseudomonas aeruginosa clinical isolates to neutrophil extracellular trap-mediated immunity, Infect. Immun., 82, 4135-4143, doi: https://doi.org/10.1128/IAI.02169-14.
Sonawane, S., Khanolkar, V., Namavari, A., Chaudhary, S., Gandhi, S., et al. (2012) Ocular surface extracellular DNA and nuclease activity imbalance: a new paradigm for inflammation in dry eye disease, Invest. Ophthalmol. Vis. Sci., 53, 8253-8263, doi: https://doi.org/10.1167/iovs.12-10430.
Tibrewal, S., Ivanir, Y., Sarkar, J., Nayeb-Hashemi, N., Bouchard, C. S., Kim, E., and Jain, S. (2014) Hyperosmolar stress induces neutrophil extracellular trap formation: implications for dry eye disease, Invest. Ophthalmol. Vis. Sci., 55, 7961-7969, doi: https://doi.org/10.1167/iovs.14-15332.
An, S., Raju, I., Surenkhuu, B., Kwon, J. E., Gulati, S., Karaman, M., et al. (2019) Neutrophil extracellular traps (NETs) contribute to pathological changes of ocular graft-vs.-host disease (oGVHD) dry eye: Implications for novel biomarkers and therapeutic strategies, Ocul. Surf., 17, 589-614, doi: https://doi.org/10.1016/j.jtos.2019.03.010.
De Bont, C. M., Stokman, M. E. M., Faas, P., Thurlings, R. M., Boelens, W. C., Wright, H. L., and Pruijn, G. J. (2020) Autoantibodies to neutrophil extracellular traps represent a potential serological biomarker in rheumatoid arthritis, J. Autoimmun., 113, 102484, doi: https://doi.org/10.1016/j.jaut.2020.102484.
Brzheskiy, V. V., Efimova, E. L., Vorontsova, T. N., Alekseev, V. N., Gusarevich, O. G., et al. (2015) Results of a multicenter, randomized, double-masked, placebo-controlled clinical study of the efficacy and safety of visomitin eye drops in patients with dry eye syndrome, Adv. Ther., 32, 1263-1279, doi: https://doi.org/10.1007/s12325-015-0273-6.
Martinod, K., and Wagner, D. D. (2014) Thrombosis: tangled up in NETs, Blood, 123, 2768-2776, doi: https://doi.org/10.1182/blood-2013-10-463646.
Moschonas, I. C., and Tselepis, A. D. (2019) The pathway of neutrophil extracellular traps towards atherosclerosis and thrombosis, Atherosclerosis, 288, 9-16, doi: https://doi.org/10.1016/j.atherosclerosis.2019.06.919.
Martinod, K., Demers, M., Fuchs, T. A., Wong, S. L., Brill, A., Gallant, M., Hu, J., Wang, Y., and Wagner, D. D. (2013) Neutrophil histone modification by peptidylarginine deiminase 4 is critical for deep vein thrombosis in mice, Proc. Natl. Acad. Sci. USA, 110, 8674-8679, doi: https://doi.org/10.1073/pnas.1301059110.
Zucoloto, A. Z., and Jenne, C. N. (2019) Platelet-neutrophil interplay: insights into neutrophil extracellular trap (NET)-driven coagulation in infection, Front. Cardiovasc. Med., 6, 85, doi: https://doi.org/10.3389/fcvm.2019.00085.
Novotny, J., Oberdieck, P., Titova, A., Pelisek, J., Chandraratne, S., et al. (2020) Thrombus NET content is associated with clinical outcome in stroke and myocardial infarction, Neurology, 94, e2346-e2360, doi: https://doi.org/10.1212/WNL.0000000000009532.
Warnatsch, A., Ioannou, M., Wang, Q., and Papayannopoulos, V. (2015) Inflammation. Neutrophil extracellular traps license macrophages for cytokine production in atherosclerosis, Science, 349, 316-320, doi: https://doi.org/10.1126/science.aaa8064.
Tsourouktsoglou, T. D., Warnatsch, A., Ioannou, M., Hoving, D., Wang, Q., and Papayannopoulos, V. (2020) Histones, DNA, and citrullination promote neutrophil extracellular trap inflammation by regulating the localization and activation of TLR4, Cell Rep., 31, 107602, doi: https://doi.org/10.1016/j.celrep.2020.107602.
Snoderly, H. T., Boone, B. A., and Bennewitz, M. F. (2019) Neutrophil extracellular traps in breast cancer and beyond: current perspectives on NET stimuli, thrombosis and metastasis, and clinical utility for diagnosis and treatment, Breast Cancer Res., 21, 145, doi: https://doi.org/10.1186/s13058-019-1237-6.
Breitbach, C. J., De Silva, N. S., Falls, T. J., Aladl, U., Evgin, L., et al. (2011) Targeting tumor vasculature with an oncolytic virus, Mol. Ther., 19, 886-894, doi: https://doi.org/10.1038/mt.2011.26.
Leppkes, M., Maueroder, C., Hirth, S., Nowecki, S., Gunther, C., et al. (2016) Externalized decondensed neutrophil chromatin occludes pancreatic ducts and drives pancreatitis, Nat. Commun., 7, 10973, doi: https://doi.org/10.1038/ncomms10973.
Muñoz, L. E., Boeltz, S., Bilyy, R., Schauer, C., Mahajan, A., et al. (2019) Neutrophil extracellular traps initiate gallstone formation, Immunity, 51, 443-450.e4, doi: https://doi.org/10.1016/j.immuni.2019.07.002.
Twaddell, S. H., Baines, K. J., Grainge, C., and Gibson, P. G. (2019) The emerging role of neutrophil extracellular traps in respiratory disease, Chest, 156, 774‐782, doi: https://doi.org/10.1016/j.chest.2019.06.012.
Ebrahimi, F., Giaglis, S., Hahn, S., Blum, C. A., Baumgartner, C., et al. (2018) Markers of neutrophil extracellular traps predict adverse outcome in community-acquired pneumonia: secondary analysis of a randomised controlled trial, Eur. Respir. J., 51, 1701389, doi: https://doi.org/10.1183/13993003.01389-2017.
Vassallo, A., Wood, A. J., Subburayalu, J., Summers, C., and Chilvers, E. R. (2019) The counter-intuitive role of the neutrophil in the acute respiratory distress syndrome, Br. Med. Bull., 131, 43‐55, doi: https://doi.org/10.1093/bmb/ldz024.
Uddin, M., Watz, H., Malmgren, A., and Pedersen, F. (2019) NETopathic inflammation in chronic obstructive pulmonary disease and severe asthma, Front. Immunol., 10, 47, doi: https://doi.org/10.3389/fimmu.2019.00047.
Toussaint, M., Jackson, D. J., Swieboda, D., Guedan, A., Tsourouktsoglou, T. D., et al. (2017) Host DNA released by NETosis promotes rhinovirus-induced type-2 allergic asthma exacerbation, Nat. Med., 23, 681-691, doi: https://doi.org/10.1038/nm.4332.
Choi, Y., Pham, D., Lee, D.-H., Lee, S.-H., Kim, S.-H., and Park, H.-S. (2018) Biological function of eosinophil extracellular traps in patients with severe eosinophilic asthma, Exp. Mol. Med., 50, 104, doi: https://doi.org/10.1038/s12276-018-0136-8.
Mehta, P., McAuley, D. F., Brown, M., Sanchez, E., Tattersall, R. S., and Manson, J. J., HLH Across Speciality Collaboration, UK (2020) COVID-19: consider cytokine storm syndromes and immunosuppression, Lancet, 395, 1033-1034, doi: https://doi.org/10.1016/S0140-6736(20)30628-0.
Zuo, Y., Yalavarthi, S., Shi, H., Gockman, K., Zuo, M., et al. (2020) Neutrophil extracellular traps in COVID-19, JCI insight, 138999. Advance online publication, doi: https://doi.org/10.1172/jci.insight.138999.
Yoshida, Y., Takeshita, S., Kawamura, Y., Kanai, T., Tsujita, Y., and Nonoyama, S. (2020) Enhanced formation of neutrophil extracellular traps in Kawasaki disease, Pediatr. Res., 87, 998‐1004, doi: https://doi.org/10.1038/s41390-019-0710-3.
Barnes, B. J., Adrover, J. M., Baxter-Stoltzfus, A., Borczuk, A., Cools-Lartigue, J., et al. (2020) Targeting potential drivers of COVID-19: neutrophil extracellular traps, J. Exp. Med., 217, e20200652, doi: https://doi.org/10.1084/jem.20200652.
Gupta, S., and Kaplan, M. J. (2016) The role of neutrophils and NETosis in autoimmune and renal diseases, Nat. Rev. Nephrol., 12, 402-413, doi: https://doi.org/10.1038/nrneph.2016.71.
Fortner, K. A., Blanco, L. P., Buskiewicz, I., Huang, N., Gibson, P. C., et al. (2020) Targeting mitochondrial oxidative stress with MitoQ reduces NET formation and kidney disease in lupus-prone MRL-lpr mice, Lupus Sci. Med., 7, e000387, doi: https://doi.org/10.1136/lupus-2020-000387.
Khandpur, R., Carmona-Rivera, C., Vivekanandan-Giri, A., Gizinski, A., Yalavarthi, S., et al. (2013) NETs are a source of citrullinated autoantigens and stimulate inflammatory responses in rheumatoid arthritis, Sci. Transl. Med., 5, 178ra40, doi: https://doi.org/10.1126/scitranslmed.3005580.
Wang, W., Peng, W., and Ning, X. (2018) Increased levels of neutrophil extracellular trap remnants in the serum of patients with rheumatoid arthritis, Int. J. Rheum. Dis., 21, 415-421, doi: https://doi.org/10.1111/1756-185X.13226.
Carmona-Rivera, C., Carlucci, P. M., Moore, E., Lingampalli, N., Uchtenhagen, H., et al. (2017) Synovial fibroblast-neutrophil interactions promote pathogenic adaptive immunity in rheumatoid arthritis, Sci. Immunol., 2, eaag3358, doi: https://doi.org/10.1126/sciimmunol.aag3358.
Fousert, E., Toes, R., and Desai, J. (2020) Neutrophil extracellular traps (NETs) take the central stage in driving autoimmune responses, Cells, 9, 915, doi: https://doi.org/10.3390/cells9040915.
Schauer, C., Janko, C., Munoz, L. E., Zhao, Y., Kienhöfer, D., et al. (2014) Aggregated neutrophil extracellular traps limit inflammation by degrading cytokines and chemokines, Nat. Med., 20, 511-517, doi: https://doi.org/10.1038/nm.3547.
Tagami, T., Tosa, R., Omura, M., Fukushima, H., Kaneko, T., et al. (2014) Effect of a selective neutrophil elastase inhibitor on mortality and ventilator-free days in patients with increased extravascular lung water: a post hoc analysis of the PiCCO pulmonary edema study, J. Intensive Care, 2, 67, doi: https://doi.org/10.1186/s40560-014-0067-y.
Hu, J. J., Liu, X., Xia, S., Zhang, Z., Zhang, Y., et al. (2020) FDA-approved disulfiram inhibits pyroptosis by blocking gasdermin D pore formation, Nat. Immunol., 21, 736-745, doi: https://doi.org/10.1038/s41590-020-0669-6.
Papayannopoulos, V., Staab, D., and Zychlinsky, A. (2011) Neutrophil elastase enhances sputum solubilization in cystic fibrosis patients receiving DNase therapy, PLoS One, 6, e28526, doi: https://doi.org/10.1371/journal.pone.0028526.
Zakharova, V. V., Pletjushkina, O. Y., Galkin, I. I., Zinovkin, R. A., Chernyak, B. V., et al. (2017) Low concentration of uncouplers of oxidative phosphorylation decreases the TNF-induced endothelial permeability and lethality in mice, Biochim. Biophys. Acta. Mol. Basis Dis., 1863, 968-977, doi: https://doi.org/10.1016/j.bbadis.2017.01.024.
Acknowledgements
The authors are grateful to the co-workers O. Yu. Pletjushkina, I. I. Galkin, S. A. Golyshev, R. A. Zinovkin, and A. S. Prikhodko (Belozersky Institute of Physico-Chemical Biology, Lomonosov Moscow State University), who participated in the experimental studies on NETosis, degranulation, and oxidative burst in human neutrophils. We are grateful to Vladimir Petrovich Skulachev, who initiated our work in the field of mitochondriology, and congratulate our dear teacher on the 85th anniversary.
Funding
The work was supported by the Russian Foundation for Basic Research (project no. 17-00-00088).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
The authors declare no conflict of interest in financial or any other sphere. This article does not contain any studies with human participants or animals performed by any of the authors.
Rights and permissions
About this article

Cite this article
Vorobjeva, N.V., Chernyak, B.V. NETosis: Molecular Mechanisms, Role in Physiology and Pathology. Biochemistry Moscow 85, 1178–1190 (2020). https://doi.org/10.1134/S0006297920100065
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1134/S0006297920100065