Mechanism of Lithotripsy by Superpulse Thulium Fiber Laser and Its Clinical Efficiency

 , ,
, , 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:Featured Application
Abstract
1. Introduction
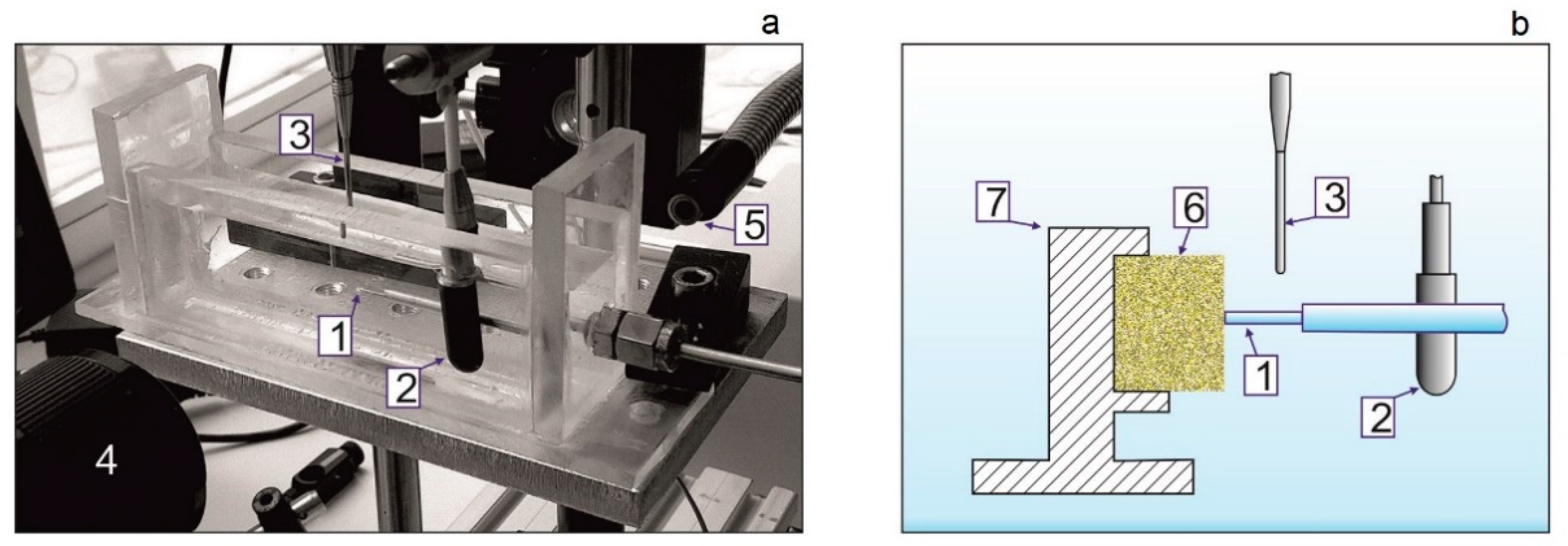
2. Materials and Methods
3. Results and Discussion
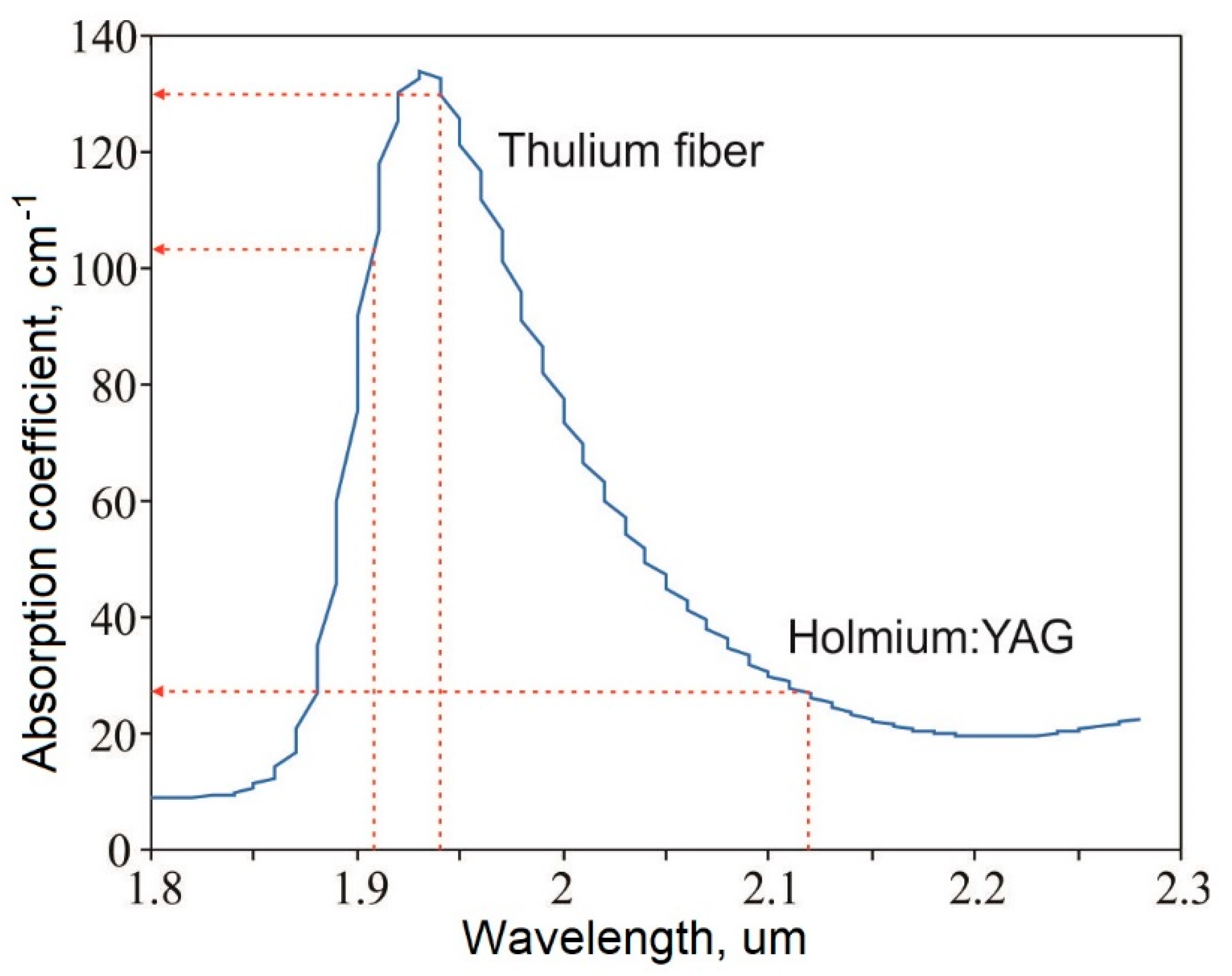
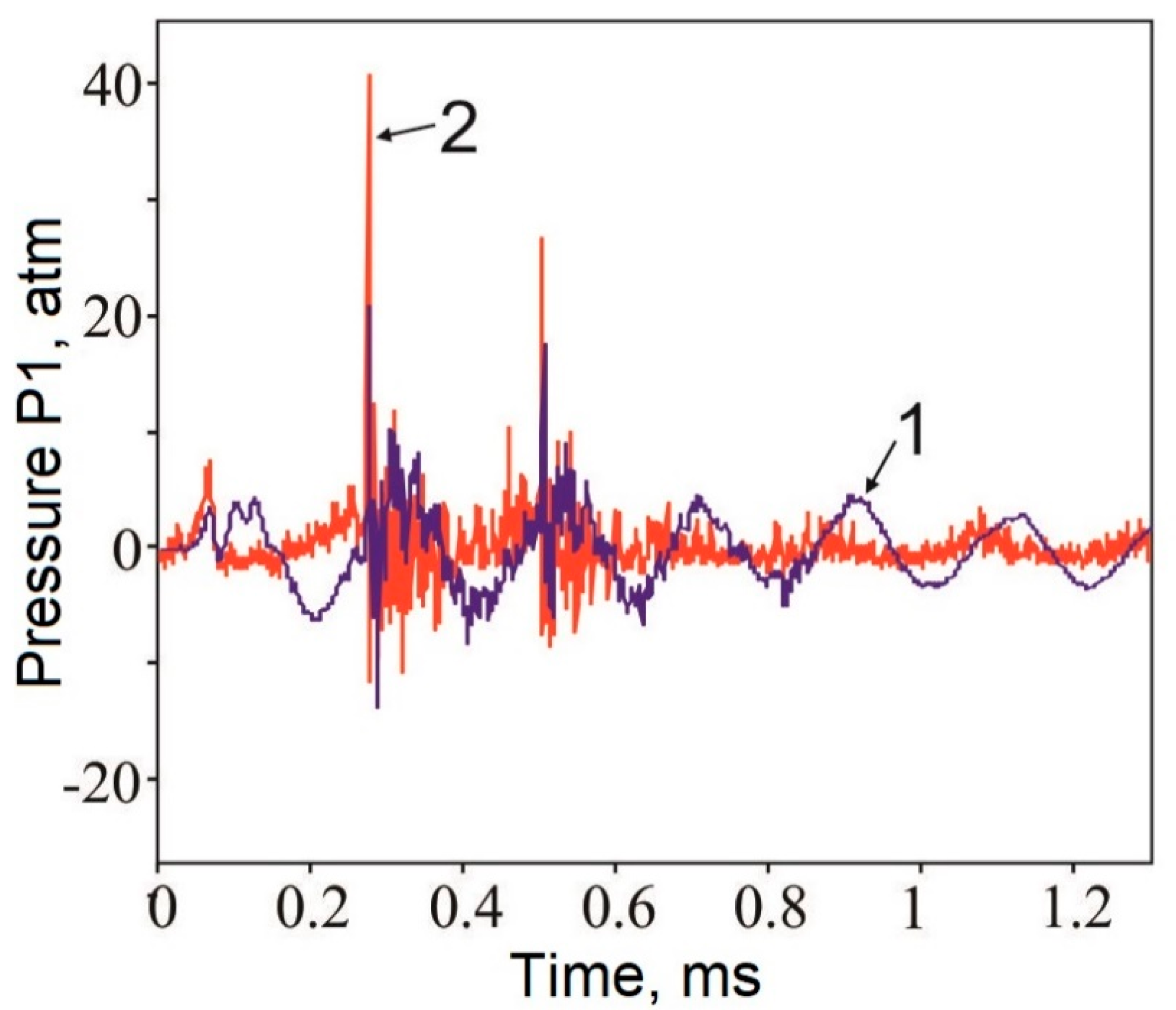
3.1. Optical and Acoustic Tests
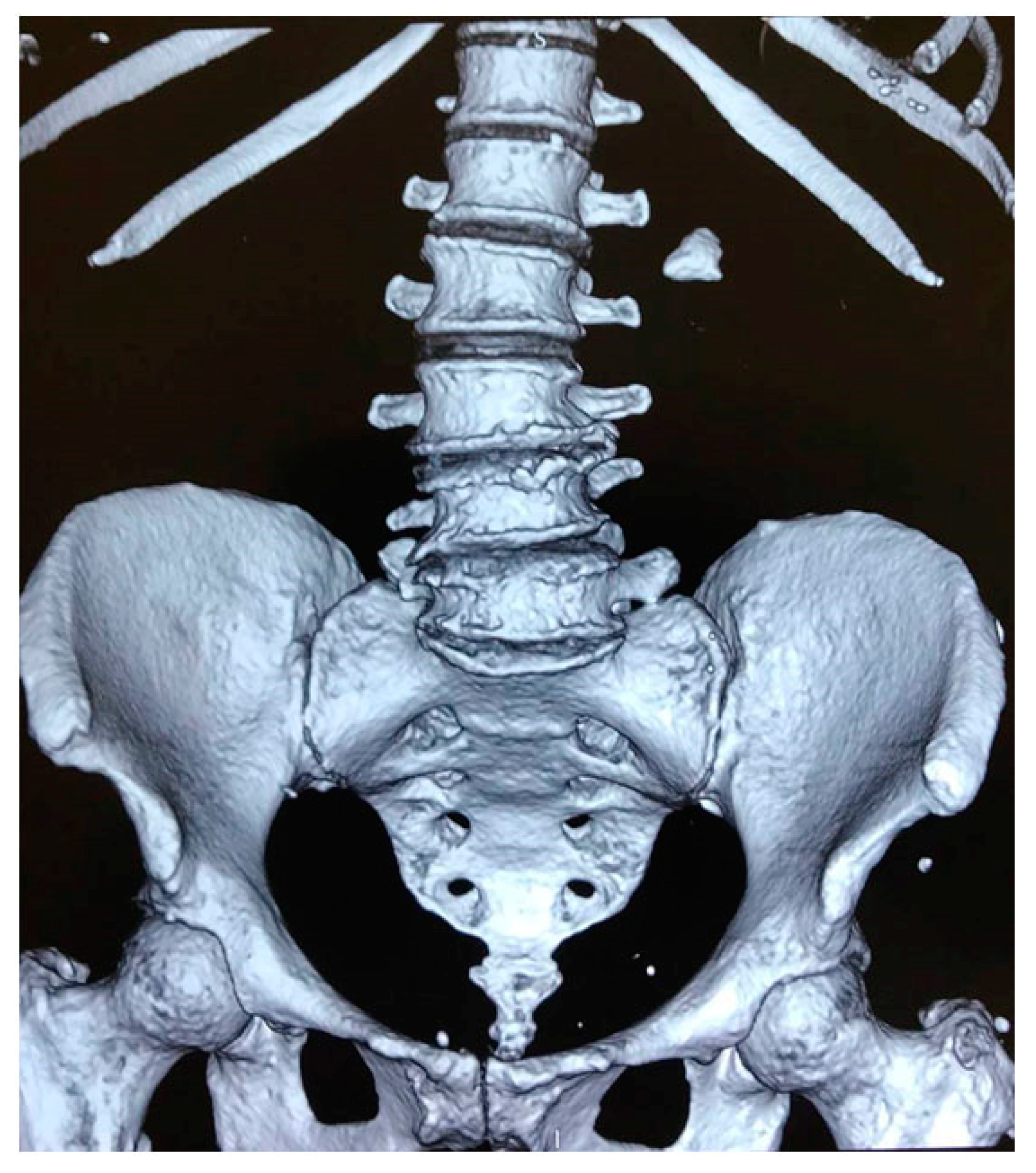
3.2. Clinical Case
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Papatsoris, A.G.; Kachrilas, S.; El Howairis, M.; Masood, J.; Buchholz, N.; Osther, P.J. Novel technologies in flexible ureterorenoscopy. Arab J. Urol. 2011, 9, 41–45. [Google Scholar] [CrossRef] [PubMed]
- Khalkhal, E.; Rezaei-Tavirani, M.; Zali, M.R.; Akbari, Z. The Evaluation of Laser Application in Surgery: A Review Article. J. Lasers Med. Sci. 2019, 10, S104–S111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Platonova, D.V.; Zamyatina, V.A.; Dymov, A.M.; Kovalenko, A.A.; Vinarov, A.Z.; Minaev, V.P. Laser lithotripsy. Urologiia 1999, 2015, 116–121. [Google Scholar]
- Welch, A.J.; Kang, H.W.; Lee, H.; Teichman, J.M. Calculus fragmentation in laser lithotripsy. Minerva Urol. Nefrol. 2004, 56, 49–63. [Google Scholar]
- Türk, C.; Skolarikos, A.; Neisius, A.; Petnk, A.; Seitz, C.; Thomas, K. Guidelines on Urolithiasis. European Association of Urology. Available online: https://uroweb.org/guideline/urolithiasis/ (accessed on 20 October 2020).
- Fried, N.M. Thulium fiber laser lithotripsy: An in vitro analysis of stone fragmentation using a modulated 110-watt Thulium fiber laser at 1.94 µm. Lasers Surg. Med. 2005, 37, 53–58. [Google Scholar] [CrossRef]
- Taratkin, M.; Laukhtina, E.; Singla, N.; Kozlov, V.; Abdusalamov, A.; Ali, S.; Gabdullina, S.; Alekseeva, T.; Enikeev, D. Temperature changes during laser lithotripsy with Ho:YAG laser and novel Tm-fiber laser: A comparative in-vitro study. World J. Urol. 2020, 1–6. [Google Scholar] [CrossRef]
- Hardy, L.A.; Vinnichenko, V.; Fried, N.M. High power holmium:YAG versus thulium fiber laser treatment of kidney stones in dusting mode: Ablation rate and fragment size studies. Lasers Surg. Med. 2019, 51, 522–530. [Google Scholar] [CrossRef]
- Ventimiglia, E.; Doizi, S.; Kovalenko, A.; Andreeva, V.; Traxer, O. Effect of temporal pulse shape on urinary stone phantom retropulsion rate and ablation efficiency using holmium:YAG and super-pulse thulium fibre lasers. BJU Int. 2020, 126, 159–167. [Google Scholar] [CrossRef]
- Andreeva, V.; Vinarov, A.; Yaroslavsky, I.; Kovalenko, A.; Vybornov, A.; Rapoport, L.; Enikeev, D.; Sorokin, N.; Dymov, A.; Tsarichenko, D.; et al. Preclinical comparison of superpulse thulium fiber laser and a holmium:YAG laser for lithotripsy. World J. Urol. 2020, 38, 497–503. [Google Scholar] [CrossRef]
- de La Floratos, R. Lasers in urology. BJU Int. 1999, 84, 204–211. [Google Scholar]
- Lee, J.; Gianduzzo, T.R.J. Advances in Laser Technology in Urology. Urol. Clin. N. Am. 2009, 36, 189–198. [Google Scholar] [CrossRef] [PubMed]
- Fried, N.M.; Irby, P.B. Advances in laser technology and fibre-optic delivery systems in lithotripsy. Nat. Rev. Urol. 2018, 15, 563–573. [Google Scholar] [CrossRef] [PubMed]
- Deng, R.; He, Y.; Qin, Y.; Chen, Q.; Chen, L. Measuring pure water absorption coefficient in the near-infrared spectrum (900–2500 nm). J. Remote Sens. 2012, 4619, 192–206. [Google Scholar]
- Enikeev, D.; Taratkin, M.; Klimov, R.; Alyaev, Y.; Rapoport, L.; Gazimiev, M.; Korolev, D.; Ali, S.; Akopyan, G.; Tsarichenko, D.; et al. Thulium-fiber laser for lithotripsy: First clinical experience in percutaneous nephrolithotomy. World J. Urol. 2020. [Google Scholar] [CrossRef]
- Rapoport, L.M.R.; Vinarov, A.Z.V.; Sorokin, N.I.S.; Dymov, A.M.D.; Enikeev, D.V.E.; Tsarichenko, D.G.T.; Lekarev, V.Y.L.; Klimov, R.E.K.; Andreeva, V.A.A.; Kovalenko, A.A.K. Experimental verification of thulium lithotripsy. Urologiia 2018, 5, 74–80. [Google Scholar] [CrossRef]
- Yusupov, V.I.; Konovalov, A.N.; Ul’yanov, V.A.; Bagratashvili, V.N. Generation of acoustic waves by cw laser radiation at the tip of an optical fiber in water. Acoust. Phys. 2016, 62, 537–544. [Google Scholar] [CrossRef]
- Enikeev, D.; Taratkin, M.; Klimov, R.; Inoyatov, J.; Azilgareeva, C.; Ali, S.; Korolev, D.; Corrales, M.; Traxer, O.; Glybochko, P. Superpulsed Thulium Fiber Laser for Stone Dusting: In Search of a Perfect Ablation Regimen—A Prospective Single-Center Study. J. Endourol. 2020. [Google Scholar] [CrossRef]
- Roggan, A.; Bindig, U.; Wäsche, W.; Zgoda, F.; Steiner, R.; Senz, R.; Helfmann, J.; Dörschel, K. Action Mechanisms of Laser Radiation in Biological Tissues. In Applied Laser Medicine; Springer: Berlin/Heidelberg, Germany, 2003; pp. 73–127. [Google Scholar]
- Kim, D.; Ye, M.; Grigoropoulos, C.P. Pulsed laser-induced ablation of absorbing liquids and acoustic-transient generation. Appl. Phys. A Mater. Sci. Process. 1998, 67, 169–181. [Google Scholar] [CrossRef]
- Skripov, V.P.; Sinitsyn, E.N.; Pavlov, P.A.; Ermakov, G.V.; Muratov, G.N.; Bulanov, N.V.; Baidakov, V.G. Thermophysical Properties of Liquids in the Metastable (Superheated) State; Gordon and Breach Science Publishers: New York, NY, USA, 1988. [Google Scholar]
- Yusupov, V.I.; Bulanov, V.V.; Chudnovskii, V.M.; Bagratashvili, V.N. Laser-induced hydrodynamics in water-saturated tissue: III. Optoacoustic effects. Laser Phys. 2014, 24, 015601. [Google Scholar] [CrossRef]
- Vogel, A.; Lauterborn, W.; Timm, R. Optical and acoustic investigations of the dynamics of laser-produced cavitation bubbles near a solid boundary. J. Fluid Mech. 1989, 206, 299–338. [Google Scholar] [CrossRef]
- Ohl, C.; Kurz, T.; Geisler, R.; Lindau, O.; Lauterborn, W. Bubble dynamics, shock waves and sonoluminescence. Philos. Trans. R. Soc. London. Ser. A Math. Phys. Eng. Sci. 1999, 357, 269–294. [Google Scholar] [CrossRef]
- Lindau, O.; Lauterborn, W. Cinematographic observation of the collapse and rebound of a laser-produced cavitation bubble near a wall. J. Fluid Mech. 2003, 479, 327–348. [Google Scholar] [CrossRef]
- Yusupov, V.I. Formation of Supercritical Water under Laser Radiation. Russ. J. Phys. Chem. B 2019, 13, 1245–1253. [Google Scholar] [CrossRef]
- Chan, K.F.; Pfefer, T.J.; Teichman, J.M.H.; Welch, A.J. A Perspective on Laser Lithotripsy: The Fragmentation Processes. J. Endourol. 2001, 15, 257–273. [Google Scholar] [CrossRef]
- Chan, K.F.; Vassar, G.J.; Pfefer, T.J.; Teichman, J.M.H.; Glickman, R.D.; Weintraub, S.T.; Welch, A.J. Holmium:YAG laser lithotripsy: A dominant photothermal ablative mechanism with chemical decomposition of urinary calculi. Lasers Surg. Med. 1999, 25, 22–37. [Google Scholar] [CrossRef]
- Gao, J.; Xue, J.-F.; Xu, M.; Gui, B.-S.; Wang, F.-X.; Ouyang, J.-M. Comparison of Physicochemical Properties of Nano- and Microsized Crystals in the Urine of Calcium Oxalate Stone Patients and Control Subjects. J. Nanomater. 2014, 2014, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Elhilali, M.M.; Badaan, S.; Ibrahim, A.; Andonian, S. Use of the Moses Technology to Improve Holmium Laser Lithotripsy Outcomes: A Preclinical Study. J. Endourol. 2017, 31, 598–604. [Google Scholar] [CrossRef]
- Rastopov, S.F.; Sukhodol’sky, A.T. Cluster nucleation in the process of CW laser induced thermocavitation. Phys. Lett. A 1990, 149, 229–232. [Google Scholar] [CrossRef]
- Padilla-Martinez, J.P.; Berrospe-Rodriguez, C.; Aguilar, G.; Ramirez-San-Juan, J.C.; Ramos-Garcia, R. Optic cavitation with CW lasers: A review. Phys. Fluids 2014, 26, 16–20. [Google Scholar] [CrossRef] [Green Version]
- Zhigarkov, V.S.; Yusupov, V.I.; Tsypina, S.I.; Bagratashvili, V.N. Hydrodynamic effects in laser cutting of biological tissue phantoms. Quantum Electron. 2017, 47, 942–948. [Google Scholar] [CrossRef]
- Yusupov, V.I.; Chudnovskii, V.M.; Bagratashvili, V.N. Laser-induced hydrodynamics in water-saturated biotissues: 2. Effect on delivery fiber. Laser Phys. 2011, 21, 1230–1234. [Google Scholar] [CrossRef]
- Thomsen, S.; Pearce, J.A. Thermal Damage and Rate Processes in Biologic Tissues. In Optical-Thermal Response of Laser-Irradiated Tissue; Springer: Dordrecht, The Netherlands, 2010; Volume 3, pp. 487–549. ISBN 9789048188307. [Google Scholar]
- Fried, N.M. Recent advances in infrared laser lithotripsy [Invited]. Biomed. Opt. Express 2018, 9, 4552. [Google Scholar] [CrossRef] [PubMed]







Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lekarev, V.; Dymov, A.; Vinarov, A.; Sorokin, N.; Minaev, V.; Minaev, N.; Tsypina, S.; Yusupov, V. Mechanism of Lithotripsy by Superpulse Thulium Fiber Laser and Its Clinical Efficiency. Appl. Sci. 2020, 10, 7480. https://doi.org/10.3390/app10217480
Lekarev V, Dymov A, Vinarov A, Sorokin N, Minaev V, Minaev N, Tsypina S, Yusupov V. Mechanism of Lithotripsy by Superpulse Thulium Fiber Laser and Its Clinical Efficiency. Applied Sciences. 2020; 10(21):7480. https://doi.org/10.3390/app10217480
Chicago/Turabian StyleLekarev, Vladimir, Alim Dymov, Andrey Vinarov, Nikolay Sorokin, Vladimir Minaev, Nikita Minaev, Svetlana Tsypina, and Vladimir Yusupov. 2020. "Mechanism of Lithotripsy by Superpulse Thulium Fiber Laser and Its Clinical Efficiency" Applied Sciences 10, no. 21: 7480. https://doi.org/10.3390/app10217480