Using Elastographic Ultrasound to Assess Plantar Tissue Stiffness after Walking at Different Speeds and Durations

 ,
, 

Abstract
:1. Introduction
2. Methods
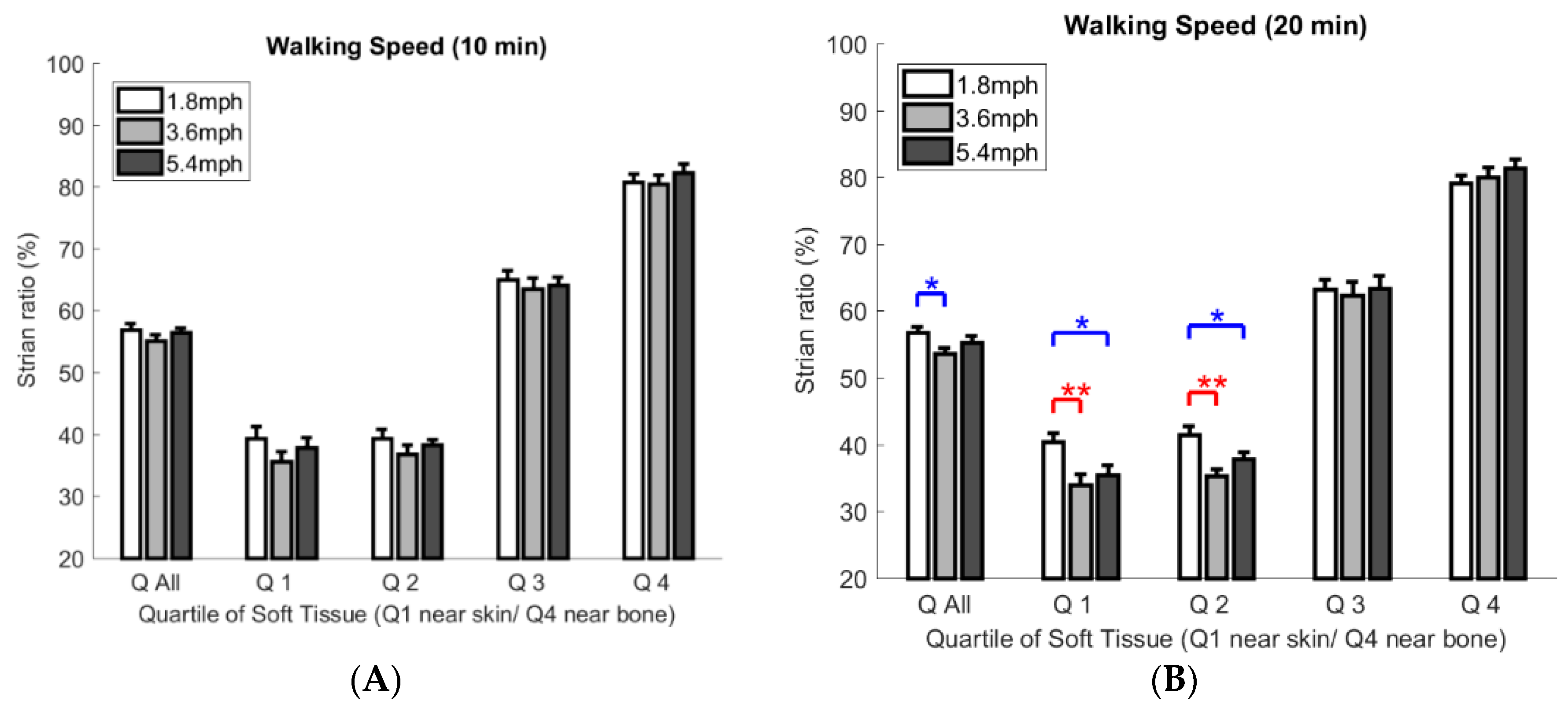
- First walking protocol: walking at 1.8 mph for 10 and 20 min (slow walking speed);
- Second walking protocol: walking at 3.6 mph for 10 and 20 min (moderate to fast walking speed);
- Third walking protocol: walking at 5.4 mph for 10 and 20 min (jogging speed).
2.1. Subjects
2.2. Experimental Procedures
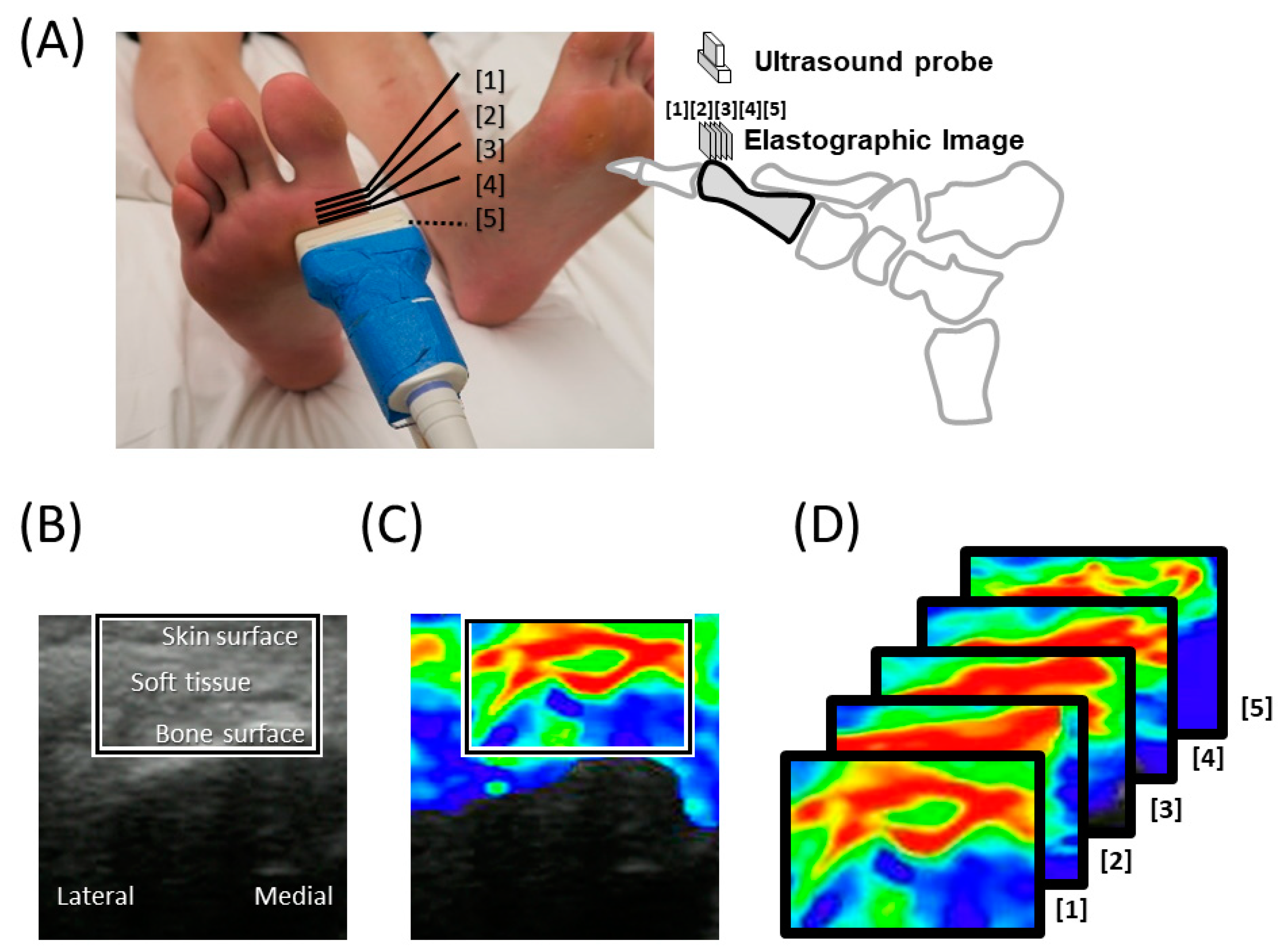
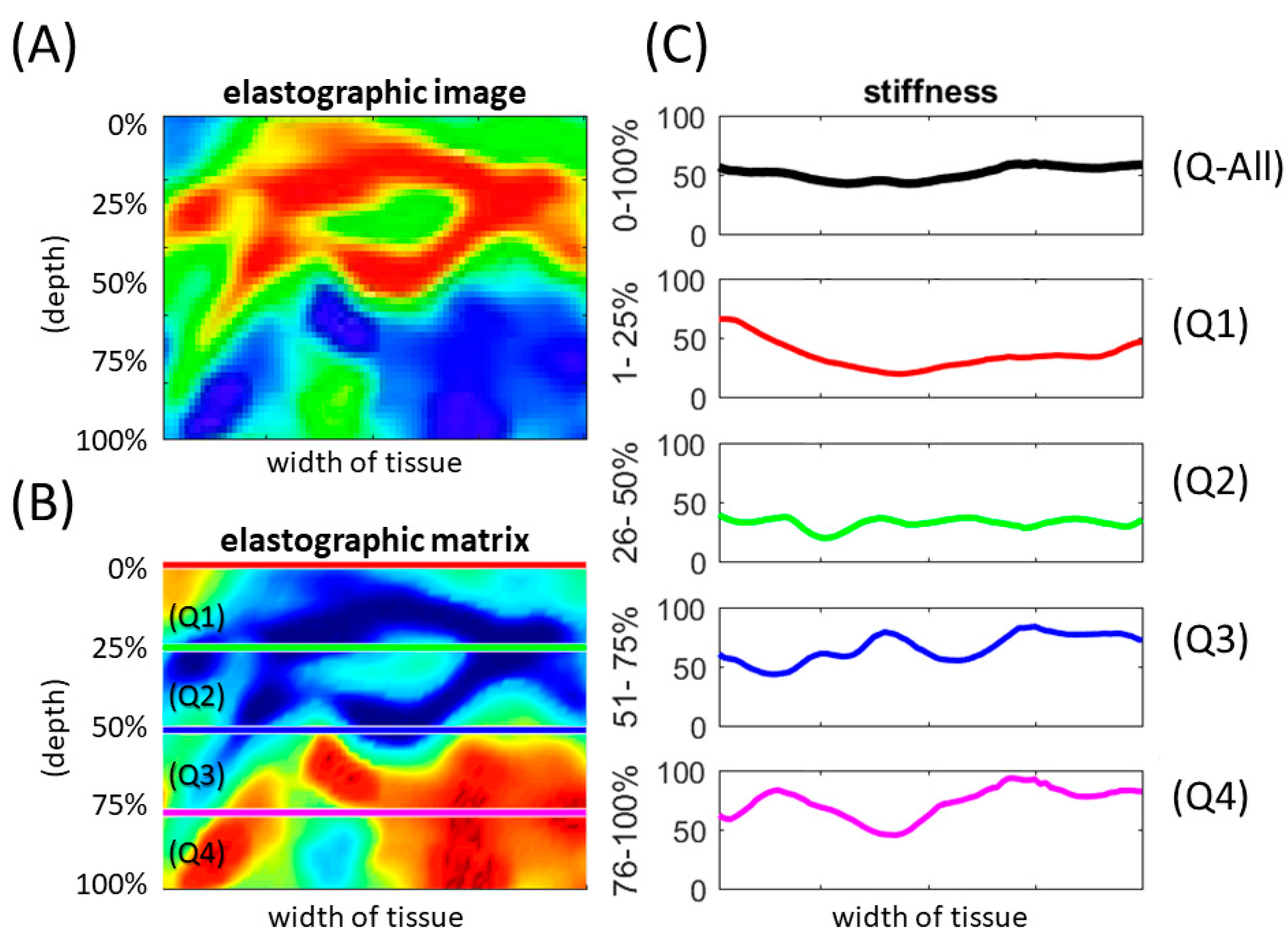
2.3. Plantar Tissue Mechanical Property
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Zhang, P.; Lu, J.; Jing, Y.; Tang, S.; Zhu, D.; Bi, Y. Global epidemiology of diabetic foot ulceration: A systematic review and meta-analysis (dagger). Ann. Med. 2017, 49, 106–116. [Google Scholar] [CrossRef] [PubMed]
- Walsh, J.W.; Hoffstad, O.J.; Sullivan, M.O.; Margolis, D.J. Association of diabetic foot ulcer and death in a population-based cohort from the United Kingdom. Diabet. Med. 2016, 33, 1493–1498. [Google Scholar] [CrossRef] [PubMed]
- Colberg, S.R.; Sigal, R.J.; Yardley, J.E.; Riddell, M.C.; Dunstan, D.W.; Dempsey, P.C.; Horton, E.S.; Castorino, K.; Tate, D.F. Physical Activity/Exercise and Diabetes: A Position Statement of the American Diabetes Association. Diabetes Care 2016, 39, 2065–2079. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boule, N.G.; Kenny, G.P.; Haddad, E.; Wells, G.A.; Sigal, R.J. Meta-analysis of the effect of structured exercise training on cardiorespiratory fitness in Type 2 diabetes mellitus. Diabetologia 2003, 46, 1071–1081. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, L.; Pei, J.H.; Kuang, J.; Chen, H.M.; Chen, Z.; Li, Z.W.; Yang, H.Z. Effect of lifestyle intervention in patients with type 2 diabetes: A meta-analysis. Metabolism 2015, 64, 338–347. [Google Scholar] [CrossRef]
- Hu, F.B.; Stampfer, M.J.; Solomon, C.; Liu, S.; Colditz, G.A.; Speizer, F.E.; Willett, W.C.; Manson, J.E. Physical activity and risk for cardiovascular events in diabetic women. Ann. Intern. Med. 2001, 134, 96–105. [Google Scholar] [CrossRef]
- Mak, A.F.; Zhang, M.; Tam, E.W. Biomechanics of pressure ulcer in body tissues interacting with external forces during locomotion. Annu. Rev. Biomed. Eng. 2010, 12, 29–53. [Google Scholar] [CrossRef] [Green Version]
- Patry, J.; Belley, R.; Cote, M.; Chateau-Degat, M.L. Plantar pressures, plantar forces, and their influence on the pathogenesis of diabetic foot ulcers: A review. J. Am. Podiatr. Med. Assoc. 2013, 103, 322–332. [Google Scholar] [CrossRef]
- Wu, F.L.; Wang, W.T.; Liao, F.; Elliott, J.; Jain, S.; Jan, Y.K. Effects of walking speeds and durations on plantar skin blood flow responses. Microvasc. Res. 2020, 128, 103936. [Google Scholar] [CrossRef]
- Liao, F.Y.; An, R.P.; Pu, F.; Burns, S.; Shen, S.; Jan, Y.K. Effect of Exercise on Risk Factors of Diabetic Foot Ulcers A Systematic Review and Meta-Analysis. Am. J. Phys. Med. Rehabil. 2019, 98, 103–116. [Google Scholar] [CrossRef]
- Bus, S.A.; van Deursen, R.W.; Armstrong, D.G.; Lewis, J.E.; Caravaggi, C.F.; Cavanagh, P.R. Footwear and offloading interventions to prevent and heal foot ulcers and reduce plantar pressure in patients with diabetes: A systematic review. Diabetes Metab. Res. Rev. 2016, 32 (Suppl. 1), 99–118. [Google Scholar] [CrossRef] [Green Version]
- Sacco, I.C.; Hamamoto, A.N.; Tonicelli, L.M.; Watari, R.; Ortega, N.R.; Sartor, C.D. Abnormalities of plantar pressure distribution in early, intermediate, and late stages of diabetic neuropathy. Gait Posture 2014, 40, 570–574. [Google Scholar] [CrossRef]
- Lung, C.W.; Wu, F.L.; Liao, F.; Pu, F.; Fan, Y.; Jan, Y.K. Emerging technologies for the prevention and management of diabetic foot ulcers. J. Tissue Viability 2020, 29, 61–68. [Google Scholar] [CrossRef]
- Klaesner, J.W.; Hastings, M.K.; Zou, D.; Lewis, C.; Mueller, M.J. Plantar tissue stiffness in patients with diabetes mellitus and peripheral neuropathy. Arch. Phys. Med. Rehabil. 2002, 83, 1796–1801. [Google Scholar] [CrossRef] [PubMed]
- Vorlander, C.; Wolff, J.; Saalabian, S.; Lienenluke, R.H.; Wahl, R.A. Real-time ultrasound elastography--a noninvasive diagnostic procedure for evaluating dominant thyroid nodules. Langenbecks Arch. Surg 2010, 395, 865–871. [Google Scholar] [CrossRef] [PubMed]
- Jan, Y.K.; Lung, C.W.; Cuaderes, E.; Rong, D.; Boyce, K. Effect of viscoelastic properties of plantar soft tissues on plantar pressures at the first metatarsal head in diabetics with peripheral neuropathy. Physiol. Meas. 2013, 34, 53–66. [Google Scholar] [CrossRef]
- Tajaddini, A.; Scoffone, H.M.; Botek, G.; Davis, B.L. Laser-induced auto-fluorescence (LIAF) as a method for assessing skin stiffness preceding diabetic ulcer formation. J. Biomech. 2007, 40, 736–741. [Google Scholar] [CrossRef]
- Gefen, A. Plantar soft tissue loading under the medial metatarsals in the standing diabetic foot. Med. Eng. Phys. 2003, 25, 491–499. [Google Scholar] [CrossRef]
- Williams, E.D.; Stebbins, M.J.; Cavanagh, P.R.; Haynor, D.R.; Chu, B.; Fassbind, M.J.; Isvilanonda, V.; Ledoux, W.R. A preliminary study of patient-specific mechanical properties of diabetic and healthy plantar soft tissue from gated magnetic resonance imaging. Proc. Inst. Mech Eng. H 2017, 231, 625–633. [Google Scholar] [CrossRef]
- Bohannon, R.W.; Williams Andrews, A. Normal walking speed: A descriptive meta-analysis. Physiotherapy 2011, 97, 182–189. [Google Scholar] [CrossRef]
- Wasadikar, A.P.; Jadhav, M.B.; Rote-Kaginalkar, V.J.; Wasadikar, P.P.; Jha, P.S. Differentiation of Solid Breast Masses into Benign and Malignant by Using Gray Scale Ultrasonography and Strain Elastography. J. Med. Sci. Clin. Res. 2017, 5, 31456–31463. [Google Scholar] [CrossRef]
- Tohno, E.; Umemoto, T.; Sasaki, K.; Morishima, I.; Ueno, E. Effect of adding screening ultrasonography to screening mammography on patient recall and cancer detection rates: A retrospective study in Japan. Eur. J. Radiol. 2013, 82, 1227–1230. [Google Scholar] [CrossRef] [PubMed]
- Wojtaszek-Nowicka, M.; Slowinska-Klencka, D.; Sporny, S.; Popowicz, B.; Kuzdak, K.; Pomorski, L.; Kaczka, K.; Sopinski, J.; Klencki, M. The efficiency of elastography in the diagnostics of follicular lesions and nodules with an unequivocal FNA result. Endokrynol. Pol. 2017, 68, 610–622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ophir, J.; Alam, S.K.; Garra, B.S.; Kallel, F.; Konofagou, E.E.; Krouskop, T.; Merritt, C.R.; Righetti, R.; Souchon, R.; Srinivasan, S.; et al. Elastography: Imaging the elastic properties of soft tissues with ultrasound. J. Med. Ultrason. 2002, 29, 155. [Google Scholar] [CrossRef]
- Havre, R.F.; Waage, J.E.R.; Mulabecirovic, A.; Gilja, O.H.; Nesje, L.B. Strain ratio as a quantification tool in strain imaging. Appl. Sci. 2018, 8, 1273. [Google Scholar] [CrossRef] [Green Version]
- Aznaveh, M.M.; Mirzaei, H.; Roshan, E.; Saraee, M. A new color based method for skin detection using RGB vector space. In Proceedings of the 2008 Conference on Human System Interactions, Krakow, Poland, 25–27 May 2008; pp. 932–935. [Google Scholar]
- Jan, Y.K.; Hou, X.; He, X.; Guo, C.; Jain, S.; Bleakney, A. Using elastographic ultrasound to assess the effect of cupping size of cupping therapy on stiffness of triceps muscle. Am. J. Phys. Med. Rehabil. 2020. [Google Scholar] [CrossRef]
- Sun, J.H.; Cheng, B.K.; Zheng, Y.P.; Huang, Y.P.; Leung, J.Y.; Cheing, G.L. Changes in the thickness and stiffness of plantar soft tissues in people with diabetic peripheral neuropathy. Arch. Phys. Med. Rehabil. 2011, 92, 1484–1489. [Google Scholar] [CrossRef]
- Mueller, M.J.; Maluf, K.S. Tissue adaptation to physical stress: A proposed “Physical Stress Theory” to guide physical therapist practice, education, and research. Phys. Ther. 2002, 82, 383–403. [Google Scholar] [CrossRef]
- Deprez, J.F.; Brusseau, E.; Fromageau, J.; Cloutier, G.; Basset, O. On the potential of ultrasound elastography for pressure ulcer early detection. Med. Phys. 2011, 38, 1943–1950. [Google Scholar] [CrossRef] [Green Version]
- Shoham, N.; Gefen, A. Deformations, mechanical strains and stresses across the different hierarchical scales in weight-bearing soft tissues. J. Tissue Viability 2012, 21, 39–46. [Google Scholar] [CrossRef]
- Jan, Y.K.; Liao, F.Y.; Cheing, G.L.Y.; Pu, F.; Ren, W.Y.; Choi, H.M.C. Differences in skin blood flow oscillations between the plantar and dorsal foot in people with diabetes mellitus and peripheral neuropathy. Microvasc. Res. 2019, 122, 45–51. [Google Scholar] [CrossRef]
- Jan, Y.K.; Shen, S.; Foreman, R.D.; Ennis, W.J. Skin blood flow response to locally applied mechanical and thermal stresses in the diabetic foot. Microvasc. Res. 2013, 89, 40–46. [Google Scholar] [CrossRef] [PubMed]
- Gennisson, J.L.; Baldeweck, T.; Tanter, M.; Catheline, S.; Fink, M.; Sandrin, L.; Cornillon, C.; Querleux, B. Assessment of elastic parameters of human skin using dynamic elastography. IEEE Trans. Ultrason. Ferroelectr. Freq. Control. 2004, 51, 980–989. [Google Scholar] [CrossRef]
- Kennedy, B.F.; Hillman, T.R.; McLaughlin, R.A.; Quirk, B.C.; Sampson, D.D. In vivo dynamic optical coherence elastography using a ring actuator. Opt. Express 2009, 17, 21762–21772. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Guan, G.; Reif, R.; Huang, Z.; Wang, R.K. Determining elastic properties of skin by measuring surface waves from an impulse mechanical stimulus using phase-sensitive optical coherence tomography. J. R. Soc. Interface 2012, 9, 831–841. [Google Scholar] [CrossRef]
- Fung, Y.C. Structure and stress-strain relationship of soft-tissues. Am. Zool. 1984, 24, 13–22. [Google Scholar] [CrossRef] [Green Version]
- Kottner, J.; Balzer, K.; Dassen, T.; Heinze, S. Pressure ulcers: A critical review of definitions and classifications. Ostomy Wound Manag. 2009, 55, 22–29. [Google Scholar]
- Daniel, R.K.; Priest, D.L.; Wheatley, D.C. Etiologic factors in pressure sores: An experimental model. Arch. Phys. Med. Rehabil. 1981, 62, 492–498. [Google Scholar]
- Federico, S.; Herzog, W. On the anisotropy and inhomogeneity of permeability in articular cartilage. Biomech. Model. Mechanobiol. 2008, 7, 367–378. [Google Scholar] [CrossRef]
- Schafer, G.; Dobos, G.; Lunnemann, L.; Blume-Peytavi, U.; Fischer, T.; Kottner, J. Using ultrasound elastography to monitor human soft tissue behaviour during prolonged loading: A clinical explorative study. J. Tissue Viability 2015, 24, 165–172. [Google Scholar] [CrossRef]
- Behforootan, S.; Chatzistergos, P.E.; Chockalingam, N.; Naemi, R. A Simulation of the Viscoelastic Behaviour of Heel Pad During Weight-Bearing Activities of Daily Living. Ann. Biomed. Eng. 2017, 45, 2750–2761. [Google Scholar] [CrossRef] [PubMed]
- Koo, S.; Park, M.S.; Chung, C.Y.; Yoon, J.S.; Park, C.; Lee, K.M. Effects of walking speed and slope on pedobarographic findings in young healthy adults. PLoS ONE 2019, 14, e0220073. [Google Scholar] [CrossRef]
- Rosenbaum, D.; Hautmann, S.; Gold, M.; Claes, L. Effects of walking speed on plantar pressure patterns and hindfoot angular motion. Gait Posture 1994, 2, 191–197. [Google Scholar] [CrossRef]
- Negishi, T.; Ito, K.; Kamono, A.; Lee, T.; Ogihara, N. Strain-rate dependence of viscous properties of the plantar soft tissue identified by a spherical indentation test. J. Mech. Behav. Biomed. Mater. 2019, 102, 103470. [Google Scholar] [CrossRef] [PubMed]
- Vawter, D.L.; Fung, Y.C.; West, J.B. Elasticity of excised dog lung parenchyma. J. Appl. Physiol. Respir. Env. Exerc. Physiol. 1978, 45, 261–269. [Google Scholar] [CrossRef]
- Behforootan, S.; Chatzistergos, P.E.; Chockalingam, N.; Healy, A.; Naemi, R. Localized pressure stimulation using turf-like structures can improve skin perfusion in the foot. Microcirculation 2019, 26, e12543. [Google Scholar] [CrossRef] [PubMed]
- Naemi, R.; Chatzistergos, P.E.; Chockalingam, N. A mathematical method for quantifying in vivo mechanical behaviour of heel pad under dynamic load. Med. Biol. Eng. Comput. 2016, 54, 341–350. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Duration | Level | Speed | One-Way | Fisher’s LSD | ||||
|---|---|---|---|---|---|---|---|---|
| ANOVA | Post Hoc | |||||||
| 1.8 mph (Mean ± SE) | 3.6 mph (Mean ± SE) | 5.4 mph (Mean ± SE) | p Value | 1.8 mph vs | 1.8 mph vs | 3.6 mph vs | ||
| 3.6 mph | 5.4 mph | 5.4 mph | ||||||
| 10 min | Q-All | 56.9 ± 1.0 | 55.1 ± 1.0 | 56.4 ± 0.8 | 0.363 | 0.170 | 0.696 | 0.321 |
| Q1 | 39.4 ± 1.8 | 35.6 ± 1.6 | 37.9 ± 1.6 | 0.293 | 0.123 | 0.556 | 0.331 | |
| Q2 | 39.4 ± 1.4 | 36.8 ± 1.4 | 38.3 ± 0.9 | 0.374 | 0.165 | 0.542 | 0.428 | |
| Q3 | 65.1 ± 1.3 | 63.5 ± 1.8 | 64.2 ± 1.2 | 0.741 | 0.444 | 0.663 | 0.740 | |
| Q4 | 80.8 ± 1.3 | 80.5 ± 1.4 | 82.3 ± 1.4 | 0.603 | 0.864 | 0.442 | 0.349 | |
| 20 min | Q-All | 56.8 ± 0.8 | 53.6 ± 0.9 | 55.3 ± 1.0 | 0.057 | 0.017 * | 0.251 | 0.191 |
| Q1 | 40.4 ± 1.3 | 34.0 ± 1.5 | 35.5 ±1.4 | 0.007 ** | 0.003 ** | 0.018 * | 0.449 | |
| Q2 | 41.4 ± 1.4 | 35.3 ± 1.0 | 37.9 ± 1.0 | 0.003 ** | 0.001 ** | 0.040 | 0.113 | |
| Q3 | 63.2 ± 1.4 | 62.3 ± 2.1 | 63.4 ± 1.8 | 0.901 | 0.732 | 0.931 | 0.668 | |
| Q4 | 79.2 ± 1.4 | 80.0 ± 1.5 | 81.4 ± 1.2 | 0.467 | 0.684 | 0.229 | 0.420 | |
| Duration | Paired t-Test | |||
|---|---|---|---|---|
| Speed | Layer | 10 min (Mean ± SE) | 20 min (Mean ± SE) | p Value |
| 1.8 mph | Q-All | 56.9 ± 1.0 | 56.8 ± 0.8 | 0.874 |
| Q1 | 39.4 ± 1.8 | 40.4 ± 1.3 | 0.283 | |
| Q2 | 39.4 ± 1.4 | 41.4 ± 1.4 | 0.149 | |
| Q3 | 65.1 ± 1.3 | 63.2 ± 1.4 | 0.191 | |
| Q4 | 80.8 ± 1.3 | 79.2 ± 1.0 | 0.139 | |
| 3.6 mph | Q-All | 55.1 ± 1.0 | 53.6 ± 0.9 | 0.053 |
| Q1 | 35.6 ± 1.6 | 34.0 ± 1.5 | 0.153 | |
| Q2 | 36.8 ± 1.4 | 35.3 ± 1.0 | 0.336 | |
| Q3 | 63.5 ± 1.8 | 62.3 ± 2.1 | 0.326 | |
| Q4 | 80.5 ± 1.4 | 80.0 ± 1.5 | 0.548 | |
| 5.4 mph | Q-All | 56.4 ± 0.8 | 55.3 ± 1.0 | 0.356 |
| Q1 | 37.9 ± 1.6 | 35.5 ± 1.4 | 0.051 | |
| Q2 | 38.3 ± 0.9 | 37.9 ± 1.0 | 0.814 | |
| Q3 | 64.2 ± 1.2 | 63.4 ± 1.8 | 0.699 | |
| Q4 | 82.3 ± 1.4 | 81.4 ± 1.2 | 0.585 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lung, C.-W.; Wu, F.-L.; Zhang, K.; Liau, B.-Y.; Townsend, R.; Jan, Y.-K. Using Elastographic Ultrasound to Assess Plantar Tissue Stiffness after Walking at Different Speeds and Durations. Appl. Sci. 2020, 10, 7498. https://doi.org/10.3390/app10217498
Lung C-W, Wu F-L, Zhang K, Liau B-Y, Townsend R, Jan Y-K. Using Elastographic Ultrasound to Assess Plantar Tissue Stiffness after Walking at Different Speeds and Durations. Applied Sciences. 2020; 10(21):7498. https://doi.org/10.3390/app10217498
Chicago/Turabian StyleLung, Chi-Wen, Fu-Lien Wu, Keying Zhang, Ben-Yi Liau, Runnell Townsend, and Yih-Kuen Jan. 2020. "Using Elastographic Ultrasound to Assess Plantar Tissue Stiffness after Walking at Different Speeds and Durations" Applied Sciences 10, no. 21: 7498. https://doi.org/10.3390/app10217498