Preclinical and Clinical Applications of Biomaterials in the Enhancement of Wound Healing in Oral Surgery: An Overview of the Available Reviews

 , and
, and
Abstract
:1. Introduction
2. Methods
2.1. Development of a Protocol
2.2. Defining the Focused Question
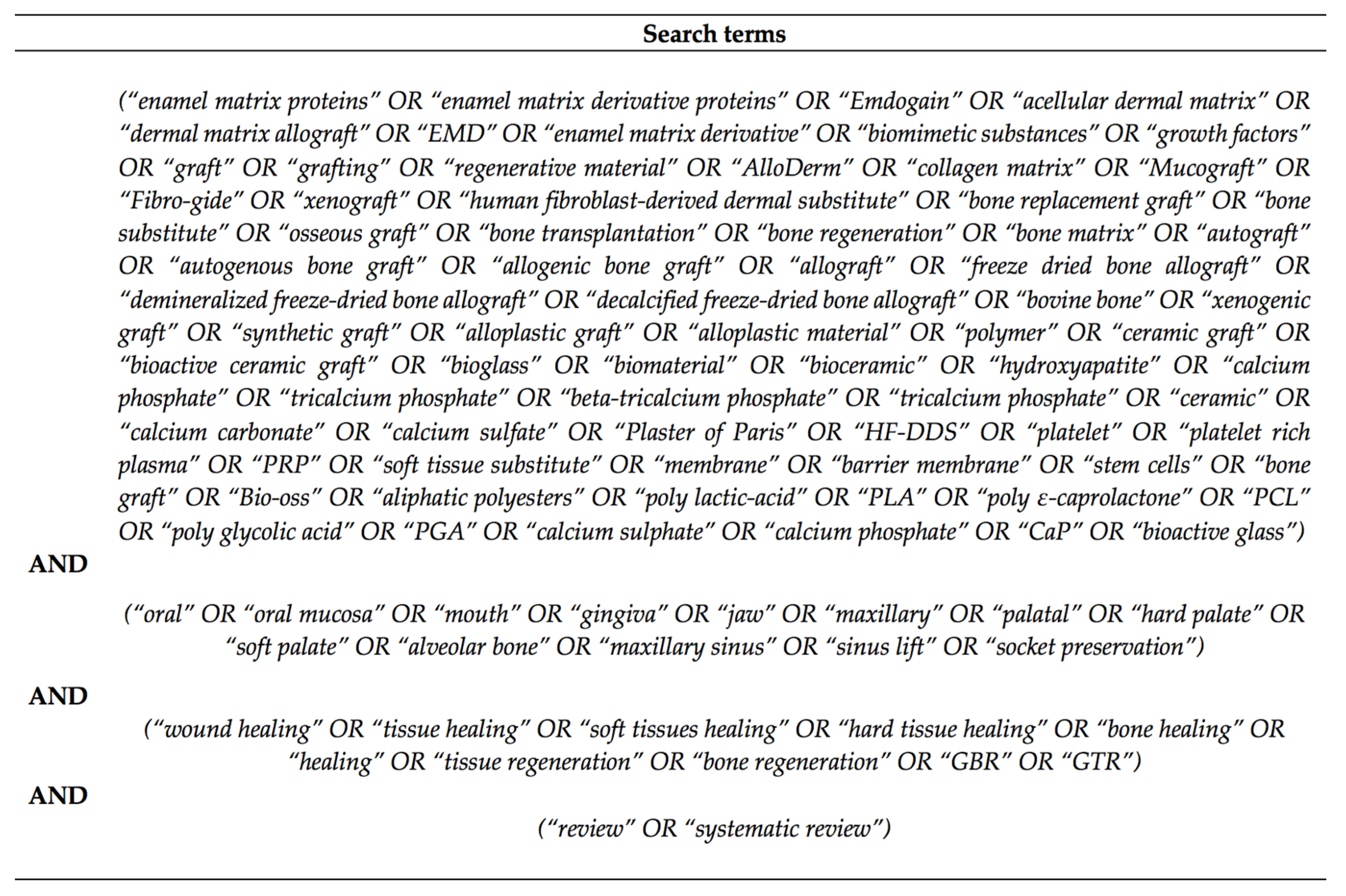
2.3. Search Strategy
2.4. Criteria for Review Selection and Inclusion
3. Results
3.1. Stem Cells
3.1.1. Background
3.1.2. Overview of Reviews
3.2. Bone Graft and Resorbable Membranes
3.2.1. Background
- -
- Autografts, obtained from the same individual that receives the graft;
- -
- Isografts, from an individual from the same species sharing the same antigenic profile (twins);
- -
- Allografts, harvested from an individual from the same species but with a different antigenic profile;
- -
- Xenografts. obtained from species other than human;
- -
- -
- Osteogenesis: the graft contains living osteoblasts that contribute to new bone formation;
- -
- Osteoinduction: the graft is able to stimulate the differentiation of osteoprogenitor cells into osteoblasts;
- -
- Osteoconduction: the graft acts as a scaffold to sustain the development of capillaries and precursor bone cells [65].
3.2.2. Bone Grafts Categories
Autografts
Allografts
Xenografts
Alloplastic Materials
3.2.3. Overview of Reviews
3.3. Growth Factors
3.3.1. Background
- -
- Bone morphogenic proteins (BMPs): cytokines able to stimulate bone cell differentiation and promote new bone formation, responsible for the osteoinductive features of bone grafts;
- -
- Fibroblast growth factor (FGF) and vascular endothelial growth factors (VEGF): mostly stimulate neoangiogenesis;
- -
- Platelet-derived growth factor (PDGF): known as one of the initiators of wound healing, with multiple functions ranging from chemotaxis and mitogenesis to promotion of angiogenesis, acts on both soft and hard tissues;
- -
- Transforming growth factor beta (TGF-β) and insulin-like growth factor (IGF): regulate collagen and fibronectin synthesis through osteoblasts or fibroblasts stimulation;
- -
- Amelogenins: extracellular matrix proteins secreted by ameloblasts that regulate hydroxyapatite crystal growth and orientation and are able to promote periodontal tissues regeneration; in the clinical practice, they are commonly found in enamel matrix derivatives (EMD) compounds, a mix of enamel matrix proteins (EMP), of which amelogenins represent circa 90% of the total protein quota [99,100];
- -
- Statins: recently discovered to possess anti-inflammatory, antimicrobial and pro-osteogenic properties.
- Pure Platelet Rich Plasma (P-PRP) or leukocyte-poor PRP that does not contain leukocytes;
- Leukocyte and PRP (L-PRP) products;
- Pure Platelet Rich Fibrin (P-PRF) or leukocyte-poor PRF;
- Leukocyte and PRF (L-PRF).
3.3.2. Overview of Reviews
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Saunders, W.B. Introduction. In Current Therapy in Oral and Maxillofacial Surgery; Bagheri, S.C., Bell, R.B., Khan, H.A., Eds.; W.B. Saunders: Saint Louis, MO, USA, 2012; p. 122. ISBN 978-1-4160-2527-6. [Google Scholar]
- AlQurashi, H.; Khurshid, Z.; Yaqin, S.A.U.; Habib, S.R.; Rokaya, D.; Zafar, M.S. Polyetherketoneketone (PEKK): An emerging biomaterial for oral implants and dental prostheses. J. Adv. Res. 2020. [Google Scholar] [CrossRef]
- Khurshid, Z.; Zafar, M.S.; Najeeb, S.; Nejatian, T.; Sefat, F. Introduction to dental biomaterials and their advances. In Advanced Dental Biomaterials; Khurshid, Z., Najeeb, S., Zafar, M.S., Sefat, F., Eds.; Woodhead Publishing: Cambridge, UK, 2019; pp. 1–5. ISBN 978-0-08-102476-8. [Google Scholar]
- Zafar, M.S.; Ullah, R.; Qamar, Z.; Fareed, M.A.; Amin, F.; Khurshid, Z.; Sefat, F. Properties of dental biomaterials. In Advanced Dental Biomaterials; Khurshid, Z., Najeeb, S., Zafar, M.S., Sefat, F., Eds.; Woodhead Publishing: Cambridge, UK, 2019; pp. 7–35. ISBN 978-0-08-102476-8. [Google Scholar]
- Tanveer, W. Biomaterials for maxillofacial prosthetic rehabilitation. In Advanced Dental Biomaterials; Khurshid, Z., Najeeb, S., Zafar, M.S., Sefat, F., Eds.; Woodhead Publishing: Cambridge, UK, 2019; pp. 615–641. ISBN 978-0-08-102476-8. [Google Scholar]
- Anil, S.; Chalisserry, E.P.; Nam, S.Y.; Venkatesan, J. Biomaterials for craniofacial tissue engineering and regenerative dentistry. In Advanced Dental Biomaterials; Khurshid, Z., Najeeb, S., Zafar, M.S., Sefat, F., Eds.; Woodhead Publishing: Cambridge, UK, 2019; pp. 643–674. ISBN 978-0-08-102476-8. [Google Scholar]
- Ferracane, J.L.; Giannobile, W.V. Novel biomaterials and technologies for the dental, oral, and craniofacial structures. J. Dent. Res. 2014, 93, 1185–1186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amghar-Maach, S.; Gay-Escoda, C.; Sánchez-Garcés, M. Ángeles Regeneration of periodontal bone defects with dental pulp stem cells grafting: Systematic Review. J. Clin. Exp. Dent. 2019, 11, e373–e381. [Google Scholar] [CrossRef] [PubMed]
- Arora, N.S.; Ramanayake, T.; Ren, Y.-F.; Romanos, G.E. Platelet-rich plasma in sinus augmentation procedures: A systematic literature review: Part II. Implant. Dent. 2010, 19, 145–157. [Google Scholar] [CrossRef]
- Barallat, L.; Ruíz-Magaz, V.; Levi, P.A.; Mareque-Bueno, S.; Galindo-Moreno, P.; Nart, J. Histomorphometric results in ridge preservation procedures comparing various graft materials in extraction sockets with Nongrafted sockets in humans: A systematic review. Implant. Dent. 2014, 23, 539–554. [Google Scholar] [CrossRef]
- Bassetti, M.A.; Bassetti, R.G.; Bosshardt, D.D. The alveolar ridge splitting/expansion technique: A systematic review. Clin. Oral Implant. Res. 2015, 27, 310–324. [Google Scholar] [CrossRef]
- Browaeys, H.; Bouvry, P.; De Bruyn, H. A literature review on biomaterials in sinus augmentation procedures. Clin. Implant. Dent. Relat. Res. 2007, 9, 166–177. [Google Scholar] [CrossRef]
- Chambrone, L.; Tatakis, D.N. Periodontal soft tissue root coverage procedures: A systematic review from the AAP regeneration workshop. J. Periodontol. 2015, 86, S8–S51. [Google Scholar] [CrossRef]
- Chan, H.-L.; Lin, G.-H.; Fu, J.-H.; Wang, H.-L. Alterations in bone quality after socket preservation with grafting materials: A systematic review. Int. J. Oral Maxillofac. Implant. 2013, 28, 710–720. [Google Scholar] [CrossRef] [Green Version]
- Corbella, S.; Taschieri, S.; Weinstein, R.L.; Del Fabbro, M. Histomorphometric outcomes after lateral sinus floor elevation procedure: A systematic review of the literature and meta-analysis. Clin. Oral Implant. Res. 2015, 27, 1106–1122. [Google Scholar] [CrossRef]
- Correia, F.; Pozza, D.H.; Gouveia, S.; Felino, A.C.; Almeida, R.F. The applications of regenerative medicine in sinus lift procedures: A systematic review. Clin. Implant. Dent. Relat. Res. 2017, 20, 229–242. [Google Scholar] [CrossRef] [PubMed]
- Danesh-Meyer, M.J.; Wikesjo, U.M.E. Gingival recession defects and guided tissue regeneration: A review. J. Periodontal Res. 2001, 36, 341–354. [Google Scholar] [CrossRef] [PubMed]
- Darby, I.B.; Morris, K.H. A systematic review of the use of growth factors in human periodontal regeneration. J. Periodontol. 2013, 84, 465–476. [Google Scholar] [CrossRef] [PubMed]
- De Risi, V.; Clementini, M.; Vittorini, G.; Mannocci, A.; De Sanctis, M. Alveolar ridge preservation techniques: A systematic review and meta-analysis of histological and histomorphometrical data. Clin. Oral Implant. Res. 2013, 26, 50–68. [Google Scholar] [CrossRef]
- Del Fabbro, M.; Bucchi, C.; Lolato, A.; Corbella, S.; Testori, T.; Taschieri, S. Healing of Postextraction sockets preserved with autologous platelet concentrates. A systematic review and meta-analysis. J. Oral Maxillofac. Surg. 2017, 75, 1601–1615. [Google Scholar] [CrossRef]
- Del Fabbro, M.; Panda, S.; Taschieri, S. Adjunctive use of plasma rich in growth factors for improving alveolar socket healing: A systematic review. J. Évid. Based Dent. Pract. 2018, 19, 166–176. [Google Scholar] [CrossRef]
- Gharpure, A.S.; Bhatavadekar, N.B. Clinical efficacy of tooth-bone graft: A systematic review and risk of bias analysis of randomized control trials and observational studies. Implant. Dent. 2018, 27, 119–134. [Google Scholar] [CrossRef]
- Giannobile, W.V.; Somerman, M.J. Growth and Amelogenin-like factors in periodontal wound healing. A systematic review. Ann. Periodontol. 2003, 8, 193–204. [Google Scholar] [CrossRef]
- Gupta, S.; Del Fabbro, M.; Chang, J. The impact of simvastatin intervention on the healing of bone, soft tissue, and TMJ cartilage in dentistry: A systematic review and meta-analysis. Int. J. Implant. Dent. 2019, 5, 17. [Google Scholar] [CrossRef]
- Horváth, A.; Mardas, N.; Mezzomo, L.A.; Needleman, I.; Donos, N. Alveolar ridge preservation. A systematic review. Clin. Oral Investig. 2012, 17, 341–363. [Google Scholar] [CrossRef]
- Ioannou, A.; Kotsakis, G.A.; Kumar, T.; Hinrichs, J.E.; Romanos, G. Evaluation of the bone regeneration potential of bioactive glass in implant site development surgeries: A systematic review of the literature. Clin. Oral Investig. 2014, 19, 181–191. [Google Scholar] [CrossRef] [PubMed]
- Ivanovic, A.; Nikou, G.; Miron, R.J.; Nikolidakis, D.; Sculean, A. Which biomaterials may promote periodontal regeneration in intrabony periodontal defects? A systematic review of preclinical studies. Quintessence Int. 2014, 45, 385–395. [Google Scholar]
- Kao, R.T.; Nares, S.; Reynolds, M.A. Periodontal regeneration—Intrabony defects: A systematic review from the AAP regeneration workshop. J. Periodontol. 2015, 86, S77–S104. [Google Scholar] [CrossRef] [PubMed]
- Macbeth, N.; Trullenque-Eriksson, A.; Donos, N.; Mardas, N. Hard and soft tissue changes following alveolar ridge preservation: A systematic review. Clin. Oral Implant. Res. 2016, 28, 982–1004. [Google Scholar] [CrossRef] [PubMed]
- Mangano, F.G.; Colombo, M.; Veronesi, G.; Caprioglio, A.; Mangano, C. Mesenchymal stem cells in maxillary sinus augmentation: A systematic review with meta-analysis. World J. Stem Cells 2015, 7, 976–991. [Google Scholar] [CrossRef] [Green Version]
- Maroulakos, M.; Kamperos, G.; Tayebi, L.; Halazonetis, D.; Ren, Y. Applications of 3D printing on craniofacial bone repair: A systematic review. J. Dent. 2019, 80, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Miron, R.J.; Sculean, A.; Cochran, D.L.; Froum, S.; Zucchelli, G.; Nemcovsky, C.; Donos, N.; Lyngstadaas, S.P.; Deschner, J.; Dard, M.; et al. Twenty years of enamel matrix derivative: The past, the present and the future. J. Clin. Periodontol. 2016, 43, 668–683. [Google Scholar] [CrossRef] [PubMed]
- Monje, A.; Pikos, M.A.; Chan, H.-L.; Suarez, F.; Gargallo-Albiol, J.; Hernández-Alfaro, F.; Galindo-Moreno, P.; Wang, H.-L. On the feasibility of utilizing allogeneic bone blocks for atrophic maxillary augmentation. BioMed Res. Int. 2014, 2014, 1–12. [Google Scholar] [CrossRef]
- Murphy, K.G.; Gunsolley, J.C. Guided tissue regeneration for the treatment of periodontal Intrabony and furcation defects. A systematic review. Ann. Periodontol. 2003, 8, 266–302. [Google Scholar] [CrossRef]
- Tavelli, L.; Ravidà, A.; Barootchi, S.; Chambrone, L.; Giannobile, W.V. Recombinant human platelet–derived growth factor: A systematic review of clinical findings in oral regenerative procedures. JDR Clin. Transl. Res. 2020. [Google Scholar] [CrossRef]
- Pranskunas, M.; Galindo-Moreno, P.; Padial-Molina, M. Extraction socket preservation using growth factors and stem cells: A systematic review. J. Oral Maxillofac. Res. 2019, 10, e7. [Google Scholar] [CrossRef] [PubMed]
- Reddy, M.S.; Aichelmann-Reidy, M.E.; Avila-Ortiz, G.; Klokkevold, P.R.; Murphy, K.G.; Rosen, P.S.; Schallhorn, R.G.; Sculean, A.; Wang, H.-L. Periodontal regeneration—Furcation defects: A consensus report from the AAP regeneration workshop. J. Periodontol. 2015, 86, S131–S133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reynolds, M.A.; Aichelmann-Reidy, M.E.; Branch-Mays, G.L.; Gunsolley, J.C. The efficacy of bone replacement grafts in the treatment of periodontal osseous defects. A systematic review. Ann. Periodontol. 2003, 8, 227–265. [Google Scholar] [CrossRef] [PubMed]
- Roca-Millan, E.; González-Navarro, B.; Izquierdo-Gómez, K.; Marí-Roig, A.; Jané-Salas, E.; López-López, J.; Velasco-Ortega, E. The application of statins in the regeneration of bone defects. Systematic review and meta-analysis. Materials 2019, 12, 2992. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rocchietta, I.; Fontana, F.; Simion, M. Clinical outcomes of vertical bone augmentation to enable dental implant placement: A systematic review. J. Clin. Periodontol. 2008, 35, 203–215. [Google Scholar] [CrossRef] [PubMed]
- Sculean, A.; Nikolidakis, D.; Schwarz, F. Regeneration of periodontal tissues: Combinations of barrier membranes and grafting materials—Biological foundation and preclinical evidence: A systematic review. J. Clin. Periodontol. 2008, 35, 106–116. [Google Scholar] [CrossRef] [PubMed]
- Sculean, A.; Nikolidakis, D.; Nikou, G.; Ivanovic, A.; Chapple, I.L.C.; Stavropoulos, A. Biomaterials for promoting periodontal regeneration in human intrabony defects: A systematic review. Periodontology 2000 2015, 68, 182–216. [Google Scholar] [CrossRef]
- Stähli, A.; Strauss, F.J.; Gruber, R. The use of platelet-rich plasma to enhance the outcomes of implant therapy: A systematic review. Clin. Oral Implant. Res. 2018, 29, 20–36. [Google Scholar] [CrossRef] [Green Version]
- Strauss, F.J.; Stähli, A.; Gruber, R. The use of platelet-rich fibrin to enhance the outcomes of implant therapy: A systematic review. Clin. Oral Implant. Res. 2018, 29, 6–19. [Google Scholar] [CrossRef]
- Varshney, S.; Dwivedi, A.; Pandey, V. Efficacy of autologous stem cells for bone regeneration during endosseous dental implants insertion—A systematic review of human studies. J. Oral Biol. Craniofacial Res. 2020, 10, 347–355. [Google Scholar] [CrossRef]
- Willenbacher, M.; Al-Nawas, B.; Berres, M.; Kämmerer, P.W.; Schiegnitz, E. The Effects of alveolar ridge preservation: A meta-analysis. Clin. Implant. Dent. Relat. Res. 2015, 18, 1248–1268. [Google Scholar] [CrossRef]
- Yen, C.-C.; Tu, Y.-K.; Chen, T.-H.; Lu, H.-K. Comparison of treatment effects of guided tissue regeneration on infrabony lesions between animal and human studies: A systematic review and meta-analysis. J. Periodontal Res. 2013, 49, 415–424. [Google Scholar] [CrossRef]
- Zhao, H.; Hu, J.; Zhao, L. Histological analysis of socket preservation using DBBM. A systematic review and meta-analysis. J. Stomatol. Oral Maxillofac. Surg. 2020. [Google Scholar] [CrossRef] [PubMed]
- Castro, A.B.; Meschi, N.; Temmerman, A.; Pinto, N.; Lambrechts, P.; Teughels, W.; Quirynen, M. Regenerative potential of leucocyte- and platelet-rich fibrin. Part A: Intra-bony defects, furcation defects and periodontal plastic surgery. A systematic review and meta-analysis. J. Clin. Periodontol. 2017, 44, 67–82. [Google Scholar] [CrossRef]
- Del Fabbro, M.; Corbella, S.; Taschieri, S.; Francetti, L.; Weinstein, R. Autologous platelet concentrate for post-extraction socket healing: A systematic review. Eur. J. Oral Implantol. 2014, 7, 333–344. [Google Scholar] [CrossRef]
- Fawzy El-Sayed, K.M.; Ahmed, G.M.; Abouauf, E.A.; Schwendicke, F. Stem/progenitor cell-mediated pulpal tissue regeneration: A systematic review and meta-analysis. Int. Endod. J. 2019, 52, 1573–1585. [Google Scholar] [CrossRef] [Green Version]
- Helgeland, E.; Shanbhag, S.; Pedersen, T.O.; Mustafa, K.; Rosén, A. Scaffold-Based Temporomandibular Joint Tissue Regeneration in Experimental Animal Models: A Systematic Review. Tissue Eng. Part B Rev. 2018, 24, 300–316. [Google Scholar] [CrossRef] [PubMed]
- Granate-Marques, A.; Polis-Yanes, C.; Seminario-Amez, M.; Jané-Salas, E.; López-López, J. Medication-related osteonecrosis of the jaw associated with implant and regenerative treatments: Systematic review. Med. Oral Patol. Oral Cir. Bucal. 2019, 24, e195–e203. [Google Scholar] [CrossRef]
- Monje, A.; Diaz, K.T.; Aranda, L.; Insua, A.; Garcia-Nogales, A.; Wang, H.L. Schneiderian Membrane Thickness and Clinical Implications for Sinus Augmentation: A Systematic Review and Meta-Regression Analyses. J. Periodontol. 2016, 87, 888–899. [Google Scholar] [CrossRef] [PubMed]
- Ragucci, G.M.; Elnayef, B.; Suárez-López Del Amo, F.; Wang, H.L.; Hernández-Alfaro, F.; Gargallo-Albiol, J. Influence of exposing dental implants into the sinus cavity on survival and complications rate: A systematic review. Int. J. Implant. Dent. 2019, 5, 6. [Google Scholar] [CrossRef] [Green Version]
- Reynolds, M.A.; Aichelmann-Reidy, M.E. Protein and peptide-based therapeutics in periodontal regeneration. J. Evid. Based Dent. Pract. 2012, 12, 118–126. [Google Scholar] [CrossRef]
- Schliephake, H.; Sicilia, A.; Nawas, B.A.; Donos, N.; Gruber, R.; Jepsen, S.; Milinkovic, I.; Mombelli, A.; Navarro, J.M.; Quirynen, M.; et al. Drugs and diseases: Summary and consensus statements of group 1. The 5th EAO Consensus Conference 2018. Clin. Oral Implants Res. 2018, 29, 93–99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Potten, C.S.; Loeffler, M. Stem cells: Attributes, cycles, spirals, pitfalls and uncertainties. Lessons for and from the crypt. Development 1990, 110, 1001–1020. [Google Scholar]
- Loeffler, M.; Roeder, I. Tissue Stem Cells: Definition, Plasticity, Heterogeneity, Self-Organization and Models—A Conceptual Approach. Cells Tissues Organs 2002, 171, 8–26. [Google Scholar] [CrossRef] [PubMed]
- Mosquera-Perez, R.; Fernández-Olavarria, A.; Diaz-Sanchez, R.-M.; Gutierrez-Perez, J.-L.; Serrera-Figallo, M.-Á.; Torres-Lagares, D. Stem cells and oral surgery: A systematic review. J. Clin. Exp. Dent. 2019, 11, e1181–e1189. [Google Scholar] [CrossRef] [PubMed]
- Miura, M.; Chen, X.-D.; Allen, M.R.; Bi, Y.; Gronthos, S.; Seo, B.-M.; Lakhani, S.; Flavell, R.A.; Feng, X.-H.; Robey, P.G.; et al. A crucial role of caspase-3 in osteogenic differentiation of bone marrow stromal stem cells. J. Clin. Investig. 2004, 114, 1704–1713. [Google Scholar] [CrossRef] [Green Version]
- Titsinides, S.; Agrogiannis, G.; Karatzas, T. Bone grafting materials in dentoalveolar reconstruction: A comprehensive review. Jpn. Dent. Sci. Rev. 2019, 55, 26–32. [Google Scholar] [CrossRef]
- Liu, X.-L.; Shi, B.; Zheng, Q.; Li, C.-H. Alveolar bone grafting and cleft lip and palate: A review. Plast. Reconstr. Surg. 2017, 140, 359e–360e. [Google Scholar] [CrossRef]
- Malinin, T.I.; Temple, H.T.; Garg, A.K. Bone allografts in dentistry: A review. Dentistry 2014, 4. [Google Scholar] [CrossRef] [Green Version]
- Bauer, T.W.; Muschler, G.F. Bone graft materials: An overview of the basic science. Clin. Orthop. Relat. Res. 2000, 371, 10–27. [Google Scholar] [CrossRef]
- Janicki, P.; Schmidmaier, G. What should be the characteristics of the ideal bone graft substitute? Combining scaffolds with growth factors and/or stem cells. Injury 2011, 42, S77–S81. [Google Scholar] [CrossRef] [PubMed]
- Hing, K.A.; Best, S.M.; Tanner, K.E.; Bonfield, W.; Revell, P.A.; Tanner, K.E. Mediation of bone ingrowth in porous hydroxyapatite bone graft substitutes. J. Biomed. Mater. Res. 2003, 68, 187–200. [Google Scholar] [CrossRef]
- Bobbert, F.S.L.; Zadpoor, A.A. Effects of bone substitute architecture and surface properties on cell response, angiogenesis, and structure of new bone. J. Mater. Chem. B 2017, 5, 6175–6192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murphy, C.M.; Haugh, M.G.; O’Brien, F.J. The effect of mean pore size on cell attachment, proliferation and migration in collagen–glycosaminoglycan scaffolds for bone tissue engineering. Biomaterials 2010, 31, 461–466. [Google Scholar] [CrossRef]
- Almazrooa, S.A.; Noonan, V.; Woo, S.-B. Resorbable collagen membranes: Histopathologic features. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2014, 118, 236–240. [Google Scholar] [CrossRef] [Green Version]
- McAllister, B.S.; Margolin, M.D.; Cogan, A.G.; Buck, D.; Hollinger, J.; Lynch, S. Eighteen-month radiographic and histologic evaluation of sinus grafting with anorganic bovine bone in the chimpanzee. Int. J. Oral Maxillofac. Implant. 1999, 14, 361–368. [Google Scholar]
- Wang, H.-L.; Tsao, Y.-P. Mineralized bone allograft-plug socket augmentation: Rationale and technique. Implant. Dent. 2007, 16, 33–41. [Google Scholar] [CrossRef]
- Pikos, M.A. Maxillary sinus membrane repair: Report of a technique for large perforations. Implant. Dent. 1999, 8, 29–35. [Google Scholar] [CrossRef]
- Taschieri, S.; Corbella, S.; Tsesis, I.; Bortolin, M.; Del Fabbro, M. Effect of guided tissue regeneration on the outcome of surgical endodontic treatment of through-and-through lesions: A retrospective study at 4-year follow-up. Oral Maxillofac. Surg. 2011, 15, 153–159. [Google Scholar] [CrossRef]
- Luitaud, C.; Laflamme, C.; Semlali, A.; Saidi, S.; Grenier, G.; Zakrzewski, A.; Rouabhia, M. Development of an engineering autologous palatal mucosa-like tissue for potential clinical applications. J. Biomed. Mater. Res. Part B Appl. Biomater. 2007, 83, 554–561. [Google Scholar] [CrossRef]
- Yamada, M.; Kubo, K.; Ueno, T.; Iwasa, F.; Att, W.; Hori, N.; Ogawa, T. Alleviation of commercial collagen sponge- and membrane-induced apoptosis and dysfunction in cultured osteoblasts by an amino acid derivative. Int. J. Oral Maxillofac. Implant. 2010, 25, 939–946. [Google Scholar]
- Bunyaratavej, P.; Wang, H.-L. Collagen membranes: A review. J. Periodontol. 2001, 72, 215–229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiapasco, M.; Casentini, P.; Zaniboni, M. Bone augmentation procedures in implant dentistry. Int. J. Oral Maxillofac. Implant. 2009, 24, 237–259. [Google Scholar]
- Araújo, M.G.; Da Silva, J.C.C.; De Mendonça, A.F.; Lindhe, J. Ridge alterations following grafting of fresh extraction sockets in man. A randomized clinical trial. Clin. Oral Implant. Res. 2014, 26, 407–412. [Google Scholar] [CrossRef] [PubMed]
- Iizuka, T.; Smolka, W.; Hallermann, W.; Mericske-Stern, R. Extensive augmentation of the alveolar ridge using autogenous calvarial split bone grafts for dental rehabilitation. Clin. Oral Implant. Res. 2004, 15, 607–615. [Google Scholar] [CrossRef]
- Kökat, A.M.; Erçöçen, A.R.; Karayazgan-Saraçoğlu, B. Simultaneous implant placement in a mandibular defect reconstructed with a free fibula graft and fabrication of a fixed metal porcelain prosthesis. J. Craniofacial Surg. 2018, 29, 1307–1311. [Google Scholar] [CrossRef]
- Osborn, T.M.; Helal, D.; Mehra, P. Iliac crest bone grafting for mandibular reconstruction: 10-year experience outcomes. J. Oral Biol. Craniofacial Res. 2017, 8, 25–29. [Google Scholar] [CrossRef] [Green Version]
- Jeong, E.C.; Yoon, S.; Jung, Y.H. Radial forearm Osteocutaneous free flap for reconstruction of hard palate with alveolar defect. J. Craniofacial Surg. 2017, 28, e438–e440. [Google Scholar] [CrossRef]
- Lee, Y.H.; Choi, J.H.; Hwang, K.; Choi, J.H. Rib bone graft adjusted to fit the facial asymmetry: A frame structure graft. J. Craniofacial Surg. 2015, 26, 2160–2162. [Google Scholar] [CrossRef]
- Atil, F.; Kocyigit, I.D.; Suer, B.T.; Alp, Y.E.; Yazan, M.; Tekin, U.; Tuz, H.H. Clinical evaluation of the use of Tibial bone grafting in Dentoalveolar reconstructive surgery. Med. Princ. Pract. 2015, 25, 72–78. [Google Scholar] [CrossRef]
- Bande, C.R.; Daware, S.; Lambade, P.; Patle, B. Reconstruction of orbital floor fractures with Autogenous bone graft application from anterior wall of maxillary sinus: A retrospective study. J. Maxillofac. Oral Surg. 2014, 14, 605–610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cho, Y.-S.; Hwang, K.-G.; Park, C. Postoperative effects of anterior nasal spine bone harvesting on overall nasal shape. Clin. Oral Implant. Res. 2012, 24, 618–622. [Google Scholar] [CrossRef] [PubMed]
- Güngörmüş, M.; Yavuz, M.S. The ascending ramus of the mandible as a donor site in maxillofacial bone grafting. J. Oral Maxillofac. Surg. 2002, 60, 1316–1318. [Google Scholar] [CrossRef] [PubMed]
- Sabhlok, S.; Waknis, P.; Gadre, K.S. Applications of coronoid process as a bone graft in maxillofacial surgery. J. Craniofacial Surg. 2014, 25, 577–580. [Google Scholar] [CrossRef]
- Peñarrocha-Oltra, D.; García-Mira, B.; Martinez, O. Localized vertical maxillary ridge preservation using bone cores and a rotated palatal flap. Int. J. Oral Maxillofac. Implant. 2005, 20, 131–134. [Google Scholar]
- Velásquez, H.; Olate, S.; Diaz, C.; Navarro, P.; Borie, E.; De Moraes, M. Quantitation of mandibular symphysis bone as source of bone grafting: Description in class I and class III skeletal conditions. J. Oral Implant. 2017, 43, 211–217. [Google Scholar] [CrossRef]
- Tolstunov, L. Maxillary tuberosity block bone graft: Innovative technique and case report. J. Oral Maxillofac. Surg. 2009, 67, 1723–1729. [Google Scholar] [CrossRef]
- Hernández-Alfaro, F.; Pages, C.M.; García, E.; Corchero, G.; Arranz, C. Palatal core graft for alveolar reconstruction: A new donor site. Int. J. Oral Maxillofac. Implant. 2005, 20, 777–783. [Google Scholar]
- Ganz, S.D. Mandibular tori as a source for onlay bone graft augmentation: A surgical procedure. Pract. Periodontics Aesthetic Dent. PPAD 1998, 9, 973–982. [Google Scholar]
- Kainulainen, V.T.; Sándor, G.K.; Clokie, C.; Keller, A.; Oikarinen, K. The zygomatic bone as a potential donor site for alveolar reconstruction—A quantitative anatomic cadaver study. Int. J. Oral Maxillofac. Surg. 2004, 33, 786–791. [Google Scholar] [CrossRef]
- Sheikh, Z.; Hamdan, N.; Ikeda, Y.; Grynpas, M.; Ganss, B.; Glogauer, M. Natural graft tissues and synthetic biomaterials for periodontal and alveolar bone reconstructive applications: A review. Biomater. Res. 2017, 21, 9. [Google Scholar] [CrossRef] [PubMed]
- Tovar, N.; Jimbo, R.; Gangolli, R.; Perez, L.; Manne, L.; Yoo, D.-Y.; Lorenzoni, F.; Witek, L.; Coelho, P. Evaluation of bone response to various anorganic bovine bone xenografts: An experimental calvaria defect study. Int. J. Oral Maxillofac. Surg. 2014, 43, 251–260. [Google Scholar] [CrossRef] [PubMed]
- Alghamdi, A.S.; Shibly, O.; Ciancio, S.G. Osseous grafting part II: Xenografts and alloplasts for periodontal regeneration—A literature review. J. Int. Acad. Periodontol. 2010, 12, 39–44. [Google Scholar] [PubMed]
- Bansal, A.K.; Shetty, D.C.; Bindal, R.; Pathak, A. Amelogenin: A novel protein with diverse applications in genetic and molecular profiling. J. Oral Maxillofac. Pathol. 2012, 16, 395–399. [Google Scholar] [CrossRef]
- Wyganowska-Swiatkowska, M.; Urbaniak, P.; Nohawica, M.; Kotwicka, M.; Jankun, J. Enamel matrix proteins exhibit growth factor activity: A review of evidence at the cellular and molecular levels. Exp. Ther. Med. 2015, 9, 2025–2033. [Google Scholar] [CrossRef] [Green Version]
- Mohan, S.P.; Jaishangar, N.; Devy, S.; Narayanan, A.; Cherian, D.; Madhavan, S.S. Platelet-rich plasma and platelet-rich fibrin in periodontal regeneration: A review. J. Pharm. Bioallied Sci. 2019, 11, S126–S130. [Google Scholar] [CrossRef]
- Kobayashi, E.; Flückiger, L.; Fujioka-Kobayashi, M.; Sawada, K.; Sculean, A.; Schaller, B.; Miron, R.J. Comparative release of growth factors from PRP, PRF, and advanced-PRF. Clin. Oral Investig. 2016, 20, 2353–2360. [Google Scholar] [CrossRef]
- Giannini, S.; Cielo, A.; Bonanome, L.; Rastelli, C.; Derla, C.; Corpaci, F.; Falisi, G. Comparison between PRP, PRGF and PRF: Lights and shadows in three similar but different protocols. Eur. Rev. Med. Pharmacol. Sci. 2015, 19, 927–930. [Google Scholar]
- Feigin, K.; Shope, B. Use of platelet-rich plasma and platelet-rich fibrin in dentistry and oral surgery: Introduction and review of the literature. J. Veter Dent. 2019, 36, 109–123. [Google Scholar] [CrossRef]
- Albanese, A.; Licata, M.; Polizzi, B.; Campisi, G. Platelet-rich plasma (PRP) in dental and oral surgery: From the wound healing to bone regeneration. Immun. Ageing 2013, 10, 1–23. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Authors | Reference | Year | Included Studies | Biomaterial Type | Wound Healing Type | Principal Findings |
|---|---|---|---|---|---|---|
| Amghar-Maach et al. | [8] | 2019 | 5 (animal studies) | stem cells | regeneration of periodontal bone | More bone volume/better periodontal health achieved with dental pulp stem cells (DPSC)grafted as cell sheets. Addition of hepatocyte growth factor (HGF) favors DPSC differentiation. |
| Arora et al. | [9] | 2010 | 6 (randomized clinical trials—RCT human studies) | growth factors (PRP) | sinus augmentation procedures | No statistically significant difference was observed in histological bone density and quality of the regenerated bone. |
| Barallat et al. | [10] | 2014 | 34 (human studies) | bone grafts | ridge preservation procedures | Controversial impact of grafting on preservation. Calcium sulfate, porcine xenograft, and magnesium enriched hydroxyapatite (MHA) showed a statistically significant additional benefit when compared with healing by blood clot formation. Demineralized freeze-dried bone allograft (DFDBA) seems to be more efficient than freeze-dried bone allograft (FDBA) in terms of percentage of newly formed bone. |
| Bassetti et al. | [11] | 2015 | 24 (18 human and 6 animal studies) | bone grafts | alveolar ridge splitting/expansion technique (ARST) | ARST seems to be a well-functioning one-stage alternative to prolonged two-stage horizontal grafting procedures. |
| Browaeys et al. | [12] | 2007 | 26 (animal studies) | bone grafts | sinus augmentation procedures | Autogenous bone represents the gold standard for sinus augmentation procedures and shows better performances with BBM or porous hydroxyapatite. Homogenous Demineralized Freeze-Dried Bone (DFDB) provides better results than heterogenous DFDB. |
| Chambrone and Tatakis | [13] | 2015 | 234 (not specificated) | bone grafts and EMD | periodontal regeneration | All root coverage (RC) procedures can offer significant drop in recession depth and clinical attachment level (CAL) improvement for Miller class I and II recession-type defects. subepithelial connective tissue graft-based procedures offered the best results for clinical practice because of their greater percentages of mean and complete RC, together with significant increase in keratinized tissue. |
| Chan et al. | [14] | 2013 | 8 (human clinical trials) | bone grafts | socket preservation procedures | Conflicting results were found with the use of xenografts on changes in the percentage of vital bone. Partial evidence suggested that alloplasts rise the amount of vital bone formation. Higher % of connective tissue was significantly reduced with the use of bone substitutes. Significant quantities of hydroxyapatite and xenograft particles detected in the healed sockets at an average of 5.6 months after grafting. |
| Corbella et al. | [15] | 2015 | 84 (human studies) | bone grafts | lateral sinus floor elevation procedure | Autogenous bone, bovine bone, and a mixture of tricalcium phosphate (TCP) and hydroxyapatite (HA) show predictable results. |
| Correia et al. | [16] | 2017 | 18 (11 clinical trials—CT and 7 RCT) | bone grafts and stem cells | sinus lift procedures | Only a few studies have demonstrated potential of regenerative medicine in sinus lift. After 6 months significative differences were outline in the vital bone and percentage of residual graft, while results from the connective tissue were not. Same conclusions were described with the use of periosteum-derived cells with collagen matrix |
| Danesh-Meyer | [17] | 2001 | 30 (human studies) | bone grafts and membrane | guided tissue regeneration | Barrier membranes do not show to provide adequate space to predictably support periodontal regeneration in gingival recession defects. |
| Darby and Morris | [18] | 2013 | 5 (human studies) | growth factors (PDGF-BB) | periodontal regeneration | The use of rhPDGF-BB led to greater CAL gain, augmented rate of bone growth, and greater percentage bone fill related to an osseoconductive control. |
| De Risi et al. | [19] | 2013 | 38 (human studies) | bone grafts | ridge preservation procedures | No major histomorphometrical and histological differences arose among different procedures or when compared to spontaneous healing. |
| Del Fabbro et al. | [20] | 2017 | 33 (human studies) | growth factors (APC) | socket preservation procedures | Soft tissue healing was statistically better for sockets treated with Autologous Platelet Concentrates (APC) seven days after surgical procedures. New bone was statistically greater for APC group in one study. |
| Del Fabbro et al. | [21] | 2018 | 8 (human studies) | growth factors (plasma-rich growth factors—PRGF) | alveolar socket healing | Better and faster epithelialization was observed in the sites treated with PRGF. The measurement of the thickness of the epithelial layer resulted in a thicker layer in the sockets treated with the PRGF. |
| Gharpure and Bhatavadekar | [22] | 2017 | 26 (18 animal studies and 8 human studies) | bone grafts | bone regeneration | Histological examination of the grafted sites from several studies revealed the generation of a dentin-bone complex, where tooth-bone graft was enclosed by newly forming bone. All reports failed to show complete resorption of the graft material and its substitution by newly formed bone. |
| Giannobile and Somerman | [23] | 2003 | 60 (human and animal studies) | growth factors (Enamel matrix derivative—EMD, bone morphogenetic proteins—BMP) | periodontal wound healing | EMD promotes bone regeneration and CAL gain. PDGF-BB promotes periodontal regeneration at the histologic level. |
| Gupta et al. | [24] | 2019 | 16 (10 animal studies and 6 human studies) | statins | oral wound healing | The topical application of simvastatin and chitosan gel could be used as a novel therapeutic approach o improve healing and reduced pain in the palatal donor site following the free gingival grafts (FGG) procedure. |
| Horváth et al. | [25] | 2012 | 14 (human studies) | bone grafts | ridge preservation procedures | Conflicting evidence exists on the benefit of alveolar ridge preservation (ARP) at the histological level. ARP does not appear to stimulate de novo hard tissue formation routinely. In addition, some graft materials may interfere with healing. |
| Ioannou et al. | [26] | 2014 | 5 (human studies) | bone graft (bioactive glass) | bone regeneration | The combination of bone graft with autogenous bone chips in a 1:1 ratio is a successful treatment modality for the direct sinus augmentation, with histological results comparable to 100% autogenous bone. |
| Ivanovic et al. | [27] | 2014 | 45 (animal studies) | bone grafts | periodontal regeneration | Among the used biomaterials, autografts, in combination with flap surgery, shown the most favorable outcomes, whereas the use of most biologic factors revealed inferior results compared to flap surgery |
| Kao et al. | [28] | 2015 | 124 (human studies) | growth factors (EMD, NBM, PRP, NHA) | periodontal regeneration | Histologic evidence of periodontal regeneration has been demonstrated when EMD is used in conjunction with nanocrystalline hydroxyapatite (NHA), autogenous bone, a bovine-derived natural bone mineral (NBM), bioactive glass, NBM + PRP,) or biphasic calcium phosphate. The most part of the studies indicate no added benefits in either radiographic or clinical gains when EMD is used with the addition of graft materials. |
| MacBeth et al. | [29] | 2016 | 9 (human studies) for q1 and 37 (human studies) for q2 | bone grafts | ridge preservation procedures | Debated data are available on alterations of width of the keratinised tissue following GBR. |
| Mangano et al. | [30] | 2015 | 39 (21 human and 18 animal studies) | stem cells | sinus augmentation procedures | BMSCs + PRP compose could give better outcomes in bone volume gain and osteogenesis comparable to that achieved by particulate cancellous bone in MSA. |
| Maroulakos et al. | [31] | 2018 | 43 (6 human and 37 animal studies) | scaffold materials and grafts | bone regeneration | The immediate and long-term bone repair was considered successful for the time of observation by biochemical, histological, micro-computed tomographic or histomorphometric findings |
| Miron et al. | [32] | 2016 | 19 (human and animal studies) | growth factors EMD) | periodontal regeneration | The use of EMD for the management of gingival recessions utilized alone is capable of improving regeneration and enhance soft tissue height/thickness. Application of EMD during conjunction with Coronally Advanced Flap (CAF) resulted in increased formation of alveolar bone, root cementum and periodontal ligament |
| Monje et al. | [33] | 2014 | 15 (human studies) | bone grafts | maxillary augmentation | Histologic analysis revealed that allogeneic block grafts perform differently in the early stages of healing when compared to autogenous block grafts |
| Murphy and Gunsolley | [34] | 2003 | 89 (human studies) | bone grafts | periodontal regeneration | Augmentation materials procedures, in addition to the physical barrier, enhance the regenerative outcome in the treatment of furcation defects treated with GTR. On the other hand, in the treatment of intrabony defects, there is no advantage to the use of augmentation materials in addition to the use of the physical barrier |
| Tavelli et al. | [35] | 2020 | 63 (human studies) | growth factors (PRGF) | periodontal regeneration | There is strong evidence that recombinant human platelet- derived growth factor (rhPDGF) is efficient in the regeneration of intrabony defects when applicated in combination with a bone matrix. In particular, rhPDGF benefits from the delivery with an osteoconductive scaffold matrix. Clinical and histological results confirmed that rhPDGF in combination with a scaffold was also efficient in the treatment of furcation defects. |
| Pranskunas et al. | [36] | 2019 | 11 (9 human and 2 animal studies) | stem cells | socket preservation procedures | The use of bioactive osteogenic molecules or mesenchymal stem cells supports bone regeneration after tooth extraction. Histologically, no particular differences are revealed between test and control groups. |
| Reddy et al. | [37] | 2015 | N.S. | bone grafts | periodontal regeneration | Histologic proof of periodontal regeneration after the application of a regenerative treatment for the management of maxillary distal, mesial, facial and mandibular lingual or facial Class II furcation defects has been demonstrated in several studies. Evidence of histologic periodontal regeneration in mandibular Class III defects is limited to one case report. Favorable results after a regenerative therapy for maxillary Class III furcation defects are limited to few clinical case reports. In Class I furcation defects, regenerative therapy could be useful in some clinical scenarios, although generally Class I furcation defects may be treated with non-regenerative therapies. |
| Reynolds et al. | [38] | 2003 | 49 (human studies) | bone grafts | regeneration of periodontal bone defects | Demineralized freeze-dried bone allograft (DFDBA) boosts the production of a new attachment apparatus in intrabony defects, while open flap debridement (OFD) results in periodontal repair characterized principally by the formation of a long junctional epithelial attachment. Several observational studies provide a large numbers of histological evidences that autogenous and demineralized allogeneic bone grafts increase the formation of new attachment. Few data also suggest that xenogenic bone grafts can sustenance the formation of a new attachment apparatus |
| Roca-Millan et al. | [39] | 2019 | 15 (animal studies) | statins | Regeneration of Periodontal bone defects | Bovine bone, autogenous bone and a mixture of tricalcium phosphate (TCP) and hydroxyapatite (HA) show predictable results. |
| Rocchietta et al. | [40] | 2008 | 18 (animal and human studies) | bone grafts | bone regeneration | Only a few studies have established the potential role of regenerative medicine in sinus lift. Statistical significance differences were outlined after 6 months in the vital bone and percentage of residual graft, while outcomes from the connective tissue were not. Same conclusions were described with the use of periosteum-derived cells with collagen matrix. |
| Sculean et al. | [41] | 2008 | 10 (Animal Studies) | Bone Grafts | Periodontal regeneration | Barrier membranes do not provide adequate space to predictably support periodontal regeneration in gingival recession defects. |
| Sculean et al. | [42] | 2015 | 58 (Human Studies) | Bone Grafts | Periodontal regeneration | The use of rhPDGF-BB led to greater percentage bone fill, greater CAL gain and increased rate of bone growth compared to an osseoconductive control. |
| Stähli et al. | [43] | 2018 | 22 (15 RCT and 7 CCT) | Growth Factors (PRP) | Bone Regeneration | No major histomorphometrical and histological differences occurred among different techniques or when compared to spontaneous healing. |
| Strauss et al. | [44] | 2018 | 12 (RCT) | Growth Factors (PRP) | Bone Regeneration | Faster and better epithelialization was appreciated in the sites treated with PRGF. The measurement of the thickness of the epithelial layer resulted in a thicker layer in the sockets treated with the PRGF. |
| Varshney et al. | [45] | 2020 | 10 (Human Studies) | Stem Cells | Bone Regeneration | Soft tissue healing was statistically better for sockets treated with Autologous Platelet Concentrates (APCs) seven days after surgery procedures. New bone was statistically greater for APC group in one study. |
| Willenbacher et al. | [46] | 2015 | 18 (Human Studies) | Bone Grafts | Ridge Preservation Procedures | Histological examination of the grafted sites from a large number of papers showed the formation of a dentin-bone complex, where tooth-bone graft was enclosed by newly forming bone. All papers failed to demonstrate a complete resorption of the graft material and its substitution by newly formed bone. |
| Yen et al. | [47] | 2013 | 22 (Human and Animal Studies) | Bone Grafts | Guided Tissue Regeneration (GTR) | Despite the quality assessments is different between human and animal studies, some papers suggested that animal models and human results displayed comparable bone-filling ratios in infrabony defects treated with GTR only or with GTR + bone grafting. |
| Zhao H. and Zhao L. | [48] | 2020 | 5 (Human Studies) | Bone Grafts | Socket preservation procedures | Socket Preservation adopting deproteinized bovine bone mineral (DBBM) did not provide extra benefit regard to post-extraction new bone generation compared to natural healing. |
| Authors | Reference | Year | Reason for Exclusion |
|---|---|---|---|
| Castro et al. | [49] | 2017 | no histological results |
| Del Fabbro et al. | [50] | 2014 | full text not found |
| Fawzy El-Sayed et al. | [51] | 2019 | different topic |
| Helgeland et al. | [52] | 2018 | different topic |
| Granate-Marques et al. | [53] | 2019 | different topic and comorbidity |
| Monje et al. | [54] | 2016 | different topic |
| Ragucci et al. | [55] | 2019 | different topic |
| Reynolds and Aichelmann-Reidy | [56] | 2012 | no systematic review |
| Schliephake et al. | [57] | 2018 | no histologic results |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Picciolo, G.; Peditto, M.; Irrera, N.; Pallio, G.; Altavilla, D.; Vaccaro, M.; Picciolo, G.; Scarfone, A.; Squadrito, F.; Oteri, G. Preclinical and Clinical Applications of Biomaterials in the Enhancement of Wound Healing in Oral Surgery: An Overview of the Available Reviews. Pharmaceutics 2020, 12, 1018. https://doi.org/10.3390/pharmaceutics12111018
Picciolo G, Peditto M, Irrera N, Pallio G, Altavilla D, Vaccaro M, Picciolo G, Scarfone A, Squadrito F, Oteri G. Preclinical and Clinical Applications of Biomaterials in the Enhancement of Wound Healing in Oral Surgery: An Overview of the Available Reviews. Pharmaceutics. 2020; 12(11):1018. https://doi.org/10.3390/pharmaceutics12111018
Chicago/Turabian StylePicciolo, Giacomo, Matteo Peditto, Natasha Irrera, Giovanni Pallio, Domenica Altavilla, Mario Vaccaro, Giuseppe Picciolo, Alessandro Scarfone, Francesco Squadrito, and Giacomo Oteri. 2020. "Preclinical and Clinical Applications of Biomaterials in the Enhancement of Wound Healing in Oral Surgery: An Overview of the Available Reviews" Pharmaceutics 12, no. 11: 1018. https://doi.org/10.3390/pharmaceutics12111018