The Social Support Networks Scale (SSNS) for Family Caregivers of Children with Cancer: A Psychometric Evaluation

 , and
, and
Abstract
:1. Introduction
1.1. Pediatric Cancer as a Health Problem
1.2. The Family Caregiver of a Child with Cancer
1.3. Effect of Social Support on Family Caregivers of Children with Cancer
1.4. Instruments for Measuring Social Support
1.5. Instruments for Measuring Social Support in Mexico
1.6. Problem Statement
2. Materials and Methods
2.1. Participants
2.2. Measuring Instruments
2.3. Procedure
2.4. Ethical Considerations
2.5. Statistical Analysis
3. Results
3.1. Sociodemographic Characteristics of Family Caregivers of Children with Cancer
3.2. Determining the Factorial Structure
Testing the Hypothetical Five-Factor Model
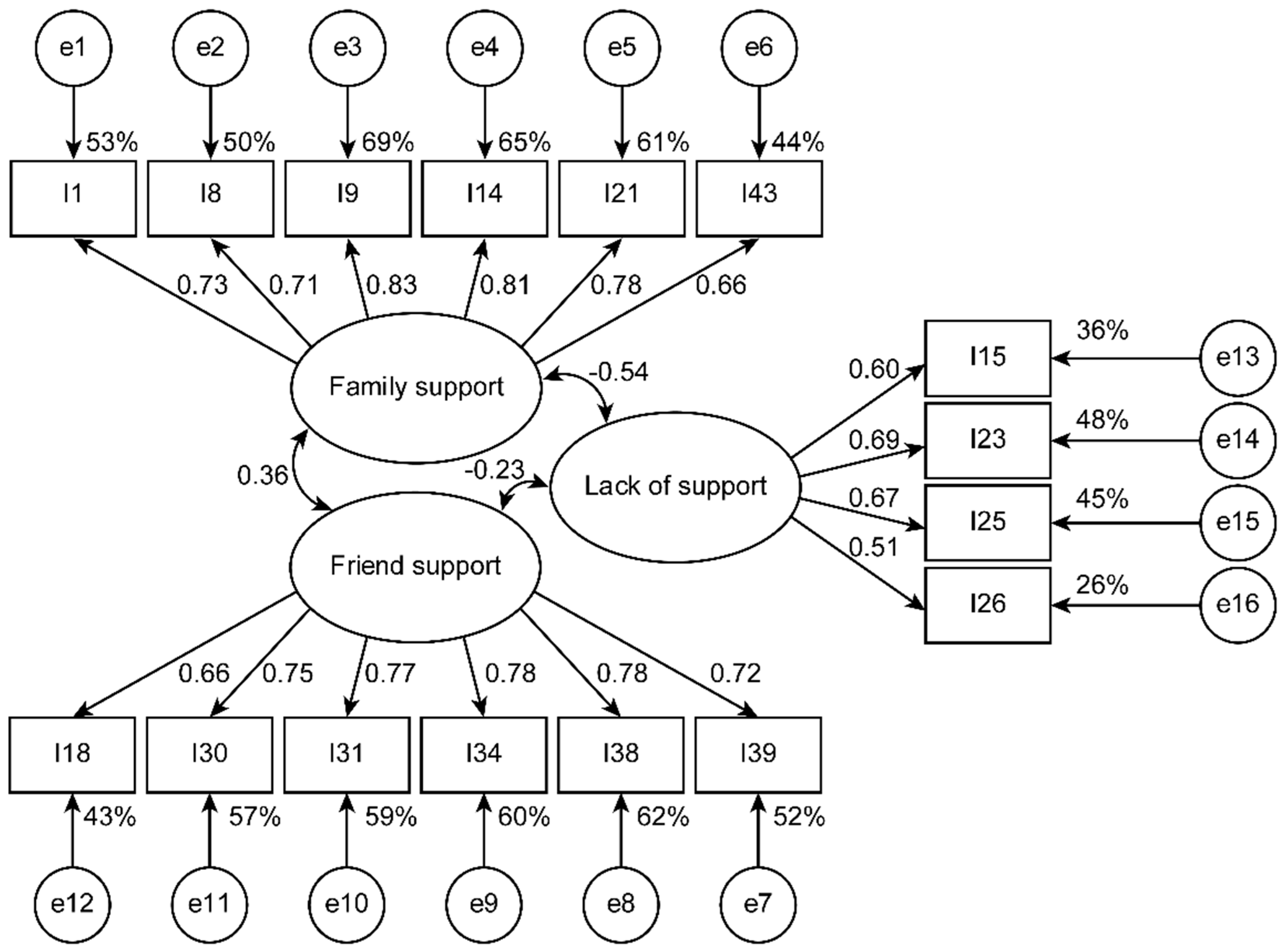
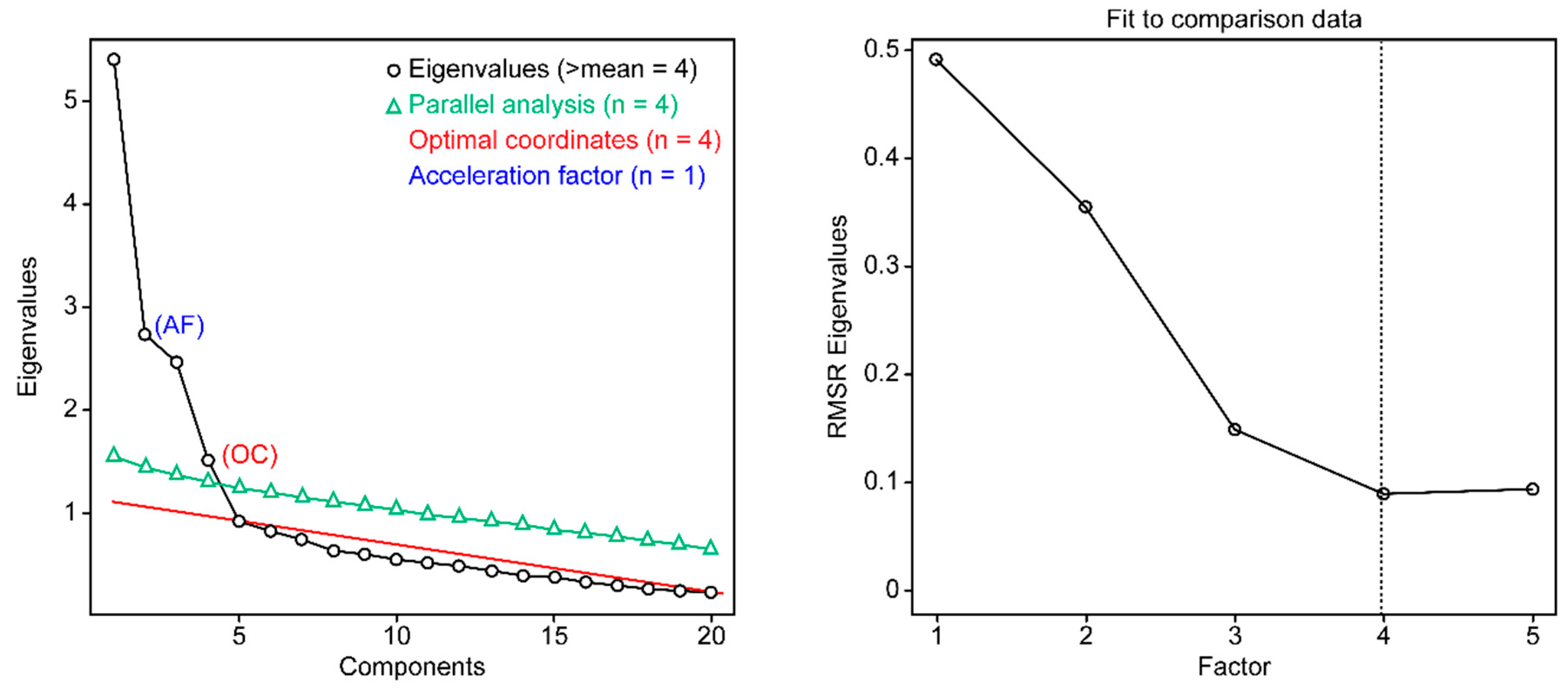
3.3. Exploration of the Factorial Structure
3.4. Reliability of the SSRS in Its Final Version (SFS-16 and RSS-4)
3.5. Description of the Distributions
3.6. Concurrent Validity
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Cáncer: Datos y Cifras [Cancer: Facts and Figures]; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Centro Nacional para la Salud de la Infancia y Adolescencia. Cáncer Infantil en México [Childhood Cancer in Mexico]; National Center for the Health of Children and Adolescents: Mexico City, Mexico, 2020. [Google Scholar]
- Toledano-Toledano, F.; Moral de la Rubia, J.; McCubbin, L.D.; Cauley, B.; Luna, D. Brief version of the coping health inventory for parents (CHIP) among family caregivers of children with chronic diseases. Health Qual. Life Outcomes 2020, 18, 104. [Google Scholar] [CrossRef] [Green Version]
- Toledano-Toledano, F.; Domínguez-Guedea, M.T. Psychosocial factors related with caregiver burden among families of children with chronic conditions. Biopsychosoc. Med. 2019, 13, 6. [Google Scholar] [CrossRef] [PubMed]
- Toledano-Toledano, F.; Luna, D. The psychosocial profile of family caregivers of children with chronic diseases: A cross-sectional study. Biopsychosoc. Med. 2020, 14, 29. [Google Scholar] [CrossRef]
- Marques, G. A família da criança com câncer: Necessidades sócio-econômicas [The family of the child with cancer: Socioeconomic needs]. Rev. Gaucha Enferm. 2017, 38, e2016–e2078. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, B.S.; Miaskowski, C.; Given, B.; Schumacher, K. The cancer family caregiving experience: An updated and expanded conceptual model. Eur. J. Oncol. Nurs. 2012, 16, 387–398. [Google Scholar] [CrossRef] [Green Version]
- Toledano-Toledano, F.; Contreras-Valdez, J.A. Validity and reliability of the Beck Depression Inventory II (BDI-II) in family caregivers of children with chronic diseases. PLoS ONE 2018, 13, e0206917. [Google Scholar] [CrossRef]
- Toledano-Toledano, F.; Moral de la Rubia, J. Factors associated with anxiety in family caregivers of children with chronic diseases. Biopsychosoc. Med. 2018, 12, 20. [Google Scholar] [CrossRef] [Green Version]
- Kasuya, R.T.; Polgar-Bailey, P.; Takeuchi, R. Caregiver burden and burnout. A guide for primary care physicians. Postgrad. Med. 2000, 108, 119–123. [Google Scholar] [CrossRef]
- Toledano-Toledano, F.; Moral de la Rubia, J.; Broche-Pérez, Y.; Domínguez-Guedea, M.T.; Granados-García, V. The measurement scale of resilience among family caregivers of children with cancer: A psychometric evaluation. BMC Public Health 2019, 19, 1164. [Google Scholar] [CrossRef] [Green Version]
- Toledano-Toledano, F.; Moral de la Rubia, J.; McCubbin, L.D.; Liebenberg, L.; Vera Jiménez, J.A.; Rivera-Rivera, L.; Hart, A.; Barajas Nava, L.A.; Salazar García, M.; Martínez Valverde, S.; et al. Validity and reliability of the Mexican resilience measurement scale in families of children with chronic conditions. Health Qual. Life Outcomes 2017, 15, 242. [Google Scholar] [CrossRef] [Green Version]
- Silva-Santos, W.; Silva-Santos, J.; Marques-Hilario, J.; Cardoso-Maia, M.; Andrade, R.D.; Halboth, N. Social support perceived by family and caregivers of children with cancer. Int. J. Pediatr. Child Health 2019, 7, 28–35. [Google Scholar] [CrossRef]
- Cohen, S. Social relationships and health. Am. Psychol. 2004, 59, 676–684. [Google Scholar] [CrossRef] [PubMed]
- Cobb, S. Presidential address-1976. Social support as a moderator of life stress. Psychosom. Med. 1976, 38, 300–314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarason, I.; Levine, H.; Basham, R.; Sarason, B. Assessing social support: The social support questionnaire. J. Personal. Soc. Psychol. 1983, 44, 127–139. [Google Scholar] [CrossRef]
- Choi, E.K.; Yoon, S.J.; Kim, J.H.; Park, H.J.; Kim, J.Y.; Yu, E.S. Depression and distress in caregivers of children with brain tumors undergoing treatment: Psychosocial factors as moderators. Psychooncology 2016, 25, 544–550. [Google Scholar] [CrossRef]
- García-Torres, M.; García-Méndez, M.; Rivera-Aragón, S. Apoyo social en adultos mexicanos: Validación de una escala [Social support in Mexican adults: Validation of a scale]. Acta Investig. Psicol. 2017, 7, 2561–2567. [Google Scholar] [CrossRef]
- Akbari, M.; Alavi, M.; Irajpour, A.; Maghsoudi, J.; Lopez, V.; Cleary, M. Support needs for family caregivers of clients with mental illness in Iran: A qualitative study. Issues Ment. Health Nurs. 2018, 39, 896–903. [Google Scholar] [CrossRef]
- Toledano-Toledano, F.; Moral de la Rubia, J.; Domínguez-Guedea, M.T.; Nabors, L.A.; Barcelata-Eguiarte, B.E.; Rocha-Pérez, E.; Luna, D.; Leyva-López, A.; Rivera-Rivera, L. Validity and Reliability of the Beck Anxiety Inventory (BAI) for Family Caregivers of Children with Cancer. Int. J. Environ. Res. Public Health 2020, 17, 7765. [Google Scholar] [CrossRef]
- Marques, G.; Araujo, B. OC11-Social support and intervention focus to minimize the effects of oncological disease in healthy siblings. Nurs. Child. Young People 2016, 28, 64. [Google Scholar] [CrossRef]
- Kuo, C.; Fitzgerald, J.; Operario, D.; Casale, M. Social support disparities for caregivers of AIDS-Orphaned children in South Africa. J. Community Psychol. 2012, 40, 631–644. [Google Scholar] [CrossRef] [Green Version]
- Littlewood, K.; Swanke, J.R.; Strozier, A.; Kondrat, D. Measuring social support among kinship caregivers: Validity and reliability of the family support scale. Child Welfare 2012, 91, 59–78. [Google Scholar] [PubMed]
- Pfeifer, L.I.; Silva, D.B.; Lopes, P.B.; Matsukura, T.S.; Santos, J.L.; Pinto, M.P. Social support provided to caregivers of children with cerebral palsy. Child Care Health Dev. 2014, 40, 363–369. [Google Scholar] [CrossRef] [PubMed]
- Bellón Saameño, J.A.; Delgado Sánchez, A.; Luna del Castillo, J.D.; Lardelli Claret, P. Validez y fiabilidad del cuestionario de apoyo social funcional Duke-UNC-11 [Validity and reliability of the Duke-UNC-11 questionnaire of functional social support]. Aten. Primaria 1996, 18, 153–156, 158–163. [Google Scholar] [PubMed]
- Costa Requena, G.; Salamero, M.; Gil, F. Validación del cuestionario MOS-SSS de apoyo social en pacientes con cáncer [Validity of the questionnaire MOS-SSS of social support in neoplastic patients]. Med. Clin. 2007, 128, 687–691. [Google Scholar] [CrossRef] [PubMed]
- Dambi, J.M.; Tapera, L.; Chiwaridzo, M.; Tadyanemhandu, C.; Nhunzvi, C. Psychometric evaluation of the Shona version of the Multidimensional Scale of Perceived Social Support Scale (MSPSS-Shona) in adult informal caregivers of patients with cancer in Harare, Zimbabwe. Malawi Med. J. 2017, 29, 89–96. [Google Scholar] [CrossRef] [Green Version]
- Martínez, B.; Sánchez, R.; Aguilar, V.; Rodríguez, P.; Riveros, R. Adaptación y validación del cuestionario MOS de apoyo social en pacientes mexicanos con VIH+ [Adaptation and validation of the MOS social support questionnaire in Mexican patients with HIV+]. Rev. Latinoam. Med. Conduct. 2014, 11, 71–85. [Google Scholar]
- Sherbourne, C.D.; Stewart, A.L. The MOS social support survey. Soc. Sci. Med. 1991, 32, 705–714. [Google Scholar] [CrossRef]
- De la Revilla, A.; Luna-del Castillo, J.; Bailón, M.; Medina, M. Validación del cuestionario MOSS de apoyo social en atención primaria [Validation of the MOSS questionnaire on social support in primary care]. Med. Fam. 2005, 6, 10–18. [Google Scholar]
- Nava-Quiroz, C. Redes de Interacción Social en la Familia Mexicana: La Búsqueda de un Modelo [Social Interaction Networks in the Mexican Family: The Search for a Model]. Ph.D. Thesis, Universidad Nacional Autónoma de México, México City, Mexico, 2002. [Google Scholar]
- López-Peñaloza, J. Resiliencia Familiar ante el Duelo [Family Resilience to Bereavement]. Ph.D. Thesis, Universidad Nacional Autónoma de México, México City, Mexico, 2008. [Google Scholar]
- Fontes, M.; Heredia, M.; Peñaloza, J.; Cedeño, M.; Rodríguez-Orozco, A. Funcionamiento familiar y su relación con las redes de apoyo social en una muestra de Morelia, México [Family functioning and their relationship with social support networks in a sample of families in the city of Morelia, Mexico]. Salud Mental 2012, 35, 147–154. [Google Scholar]
- Yu, H.; Li, L.; Liu, C.; Huang, W.; Zhou, J.; Fu, W.; Ma, Y.; Li, S.; Chang, Y.; Liu, G.; et al. Factors associated with the quality of life of family caregivers for leukemia patients in China. Health Qual. Life Outcomes 2017, 15, 55–66. [Google Scholar] [CrossRef] [Green Version]
- Baran, G.; Arda Sürücü, H.; Hülya Üzel, V. Resilience, life satisfaction, care burden and social support of mothers with a child with acute lymphoblastic leukaemia: A comparative study. Scand. J. Caring Sci. 2019, 34, 340–347. [Google Scholar] [CrossRef] [PubMed]
- Burnette, D.; Duci, V.; Dhembo, E. Psychological distress, social support, and quality of life among cancer caregivers in Albania. Psychooncology 2017, 26, 779–786. [Google Scholar] [CrossRef] [PubMed]
- Ferrando, P.; Anguiano-Carrasco, C. El análisis factorial como técnica de investigación en psicología [Factor analysis as a research technique in psychology]. Pap. Psicól. 2010, 31, 18–33. [Google Scholar]
- Kline, R. Principles and Practice of Structural Equation Modeling; Guilford Press: New York, NY, USA, 2016. [Google Scholar]
- Toledano-Toledano, F.; Rodríguez-Rey, R.; Moral de la Rubia, J.; Luna, D. A sociodemographic variables questionnaire (Q-SV) for research on family caregivers of children with chronic disease. BMC Psychol. 2019, 7, 85. [Google Scholar] [CrossRef]
- Palomar, J.; Gómez, N. Desarrollo de una escala de medición de la resiliencia con mexicanos (RESI-M) [Construction of a measurement scale of resilience in Mexicans (RESI-M)]. Interdisciplinaria 2010, 27, 7–22. [Google Scholar]
- García-Méndez, M.; Rivera-Aragón, S.; Reyes-Lagunes, I.; Díaz-Loving, R. Construcción de una escala de funcionamiento familiar [Construction of a family functioning scale]. Rev. Iberoam. Diagn. Eval. Psicol. 2006, 2, 91–110. [Google Scholar]
- WHOQOL Group. WHOQOL-BREF. Introduction, Administration, Scoring and Generic Version of the Assessment; WHO: Geneva, Switzerland, 1996. [Google Scholar]
- González-Celis, R.; Sánchez-Sosa, J. Efectos de un programa cognitivo-conductual para mejorar la calidad de vida en adultos mayores [Effects of a cognitive-behavioral program to improve the quality of life in older adults]. Rev. Mex. Psicol. 2003, 20, 43–58. [Google Scholar]
- Sociedad Mexicana de Psicología. Código Ético del Psicólogo [Ethical Code of the Psychologist], 5th ed.; Trillas: Ciudad de México, Mexico, 2010. [Google Scholar]
- American Psychological Association. Ethical Principles of Psychologists and Code of Conduct. With the 2016 Amendment to Standard 3.04; American Psychological Association Press: Washington, DC, USA, 2017. [Google Scholar]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [Green Version]
- Brown, T. Confirmatory Factor Analysis for Applied Research; Guilford Press: New York, NY, USA, 2006. [Google Scholar]
- Braeken, J.; Van Assen, M. An empirical Kaiser criterion. Psychol. Methods 2017, 22, 450–466. [Google Scholar] [CrossRef] [Green Version]
- Horn, J.L. A rationale and test for the number of factors in factor analysis. Psychometrika 1965, 30, 179–185. [Google Scholar] [CrossRef]
- Byrne, B. Structural Equation Modeling with AMOS: Basic Concepts, Applications, and Programming, 3rd ed.; Routledge: New York, NY, USA, 2016. [Google Scholar]
- Jöreskog, K.; Olsson, U.; Wallentin, F. Multivariate Analysis with LISREL; Springer International Publishing: New York, NY, USA, 2016. [Google Scholar]
- Moral de la Rubia, J. Revisión de los criterios para validez convergente estimada a través de la varianza media extraída [Review of the criteria for estimated convergent validity through the extracted mean variance]. Psychologia 2019, 13, 25–41. [Google Scholar] [CrossRef]
- Fornell, C.; Larcker, D. Evaluating structural equation models with unobservable variables and measurement error. J. Mark. Res. 1981, 18, 39–50. [Google Scholar] [CrossRef]
- Oosterwijk, P.; Van der Ark, L.; Sijtsma, K. Numerical differences between Guttmann’s reliability coefficients and the GLB. In Quantitative Psychology Research. Springer Proceedings in Mathematics and Statistics; Van der Ark, L., Bolt, D., Wang, W., Douglas, J., Wiberg, M., Eds.; Springer: Cham, Switzerland, 2016; Volume 167, pp. 155–172. [Google Scholar]
- Badii, M.; Guillen, A.; Serrato, O.; Aguilar, J. Correlación no-paramétrica y su aplicación en la investigaciones científica [Non-parametric correlation and its application in scientific research]. Int. J. Good Consci. 2014, 9, 31–40. [Google Scholar]
- Prestby, T.; App, J.; Kang, Y.; Gao, S. Understanding neighborhood isolation through spatial interaction network analysis using location big data. Environ. Plan. A Econ. Space 2020, 52, 1027–1031. [Google Scholar] [CrossRef]
- Golman, R.; Loewenstein, G.; Moene, K.O.; Zarri, L. The preference for belief consonance. J. Econ. Perspect. 2016, 30, 165–188. [Google Scholar] [CrossRef] [Green Version]
- Bahns, A.J.; Lee, J.; Crandall, C.S. Culture and mobility determine the importance of similarity in friendship. J. Cross Cult. Psychol. 2019, 50, 731–750. [Google Scholar] [CrossRef]
- Lopez, A.C. A Catholicism I know. In Y tú ¿qué Hora Traes? Unpacking the Privileges of Dominant Groups in Mexico; Lopez, A.C., Ed.; Brill Sense: Boston, MA, USA, 2019; pp. 19–41. [Google Scholar] [CrossRef]
- Wolffe, J. Towards the post-secular city? London since the 1960s. J. Relig. Hist. 2017, 41, 532–549. [Google Scholar] [CrossRef] [Green Version]
- Becci, I.; Burchardt, M.; Giorda, M. Religious super-diversity and spatial strategies in two European cities. Curr. Sociol. 2017, 65, 73–91. [Google Scholar] [CrossRef]
- Velicer, W. Determining the number of components from the matrix of partial correlations. Psychometrika 1976, 41, 321–327. [Google Scholar] [CrossRef]
- Ruscio, J.; Roche, B. Determining the number of factors to retain in an exploratory factor analysis using comparison data of known factorial structure. Psychol. Assess. 2012, 24, 282–292. [Google Scholar] [CrossRef] [Green Version]
- Raîche, G.; Walls, T.A.; Magis, D.; Riopel, M.; Blais, J.G. Non-Graphical solutions for Cattell’s scree test. Methodology 2013, 9, 23–29. [Google Scholar] [CrossRef] [Green Version]
- Fei, D. The repeatability in psychology: A topic model approach. Wirel. Pers. Commun. 2018, 103, 983–989. [Google Scholar] [CrossRef]
- Theofanidis, D.; Fountouki, A. Limitations and delimitations in the research process. Perioper. Nurs. 2019, 7, 155–162. [Google Scholar] [CrossRef]
- Fuller-Iglesias, H.R.; Antonucci, T.C. Familism, social network characteristics, and well-being among older adults in Mexico. J. Cross Cult. Gerontol. 2016, 31, 1–17. [Google Scholar] [CrossRef]
- Bustamante, A.V.; Vilar-Compte, M.; Ochoa Lagunas, A. Social support and chronic disease management among older adults of Mexican heritage: A U.S.-Mexico perspective. Soc. Sci. Med. 2018, 216, 107–113. [Google Scholar] [CrossRef]
- Taheri-Kharameh, Z.; Zamanian, H.; Montazeri, A.; Asgarian, A.; Esbiri, R. Negative religious coping, positive religious coping, and quality of life among hemodialysis patients. Nephrourol. Mon. 2016, 8, e38009. [Google Scholar] [CrossRef] [Green Version]
- Mehri Nejad, S.A.; Ramezan-Saatchi, L.; Paydar, S. Death anxiety and its relationship with social support and adherence to religion in the elderly. Salmand Iran. J. Ageing 2017, 11, 494–503. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Sociodemographic and Clinical Variables | Value Labels | Caregiver | Child | ||||||
|---|---|---|---|---|---|---|---|---|---|
| n | % | M | SD | n | % | M | SD | ||
| Sex | Woman | 515 | 81 | 302 | 48 | ||||
| Man | 118 | 19 | 331 | 52 | |||||
| Age (years) | 1–2 | 31.70 | 7.58 | 226 | 35.7 | 5.75 | 4.92 | ||
| 3–10 | 279 | 44.1 | |||||||
| 11–17 | 128 | 20.2 | |||||||
| 18–29 | 266 | 42 | |||||||
| 30–39 | 260 | 41.1 | |||||||
| 40–52 | 107 | 16.9 | |||||||
| Civil status | Married | 257 | 40.6 | ||||||
| Cohabitant | 244 | 38.5 | |||||||
| Divorced/separated | 71 | 11.2 | |||||||
| Single | 55 | 8.7 | |||||||
| Widowed | 6 | 1 | |||||||
| Number of children | 1 | 172 | 27.2 | 2.32 | 1.17 | ||||
| 2 | 202 | 31.9 | |||||||
| 3 | 183 | 28.9 | |||||||
| 4–10 | 76 | 12 | |||||||
| Scholarship | Unschooled | 18 | 2.8 | ||||||
| Primary | 124 | 19.6 | |||||||
| Lower secondary | 282 | 44.5 | |||||||
| Upper secondary | 163 | 25.8 | |||||||
| Higher education | 46 | 7.3 | |||||||
| Occupation | Housewife | 413 | 65.2 | ||||||
| Office employee | 87 | 13.7 | |||||||
| Merchant | 58 | 9.2 | |||||||
| Unemployed | 44 | 7 | |||||||
| Manual worker | 26 | 4.1 | |||||||
| Student | 5 | 0.8 | |||||||
| Income | From 0–1 | 390 | 61.6 | ||||||
| (minimum wages) * | From 1–2 | 140 | 22.1 | ||||||
| From 2–3 | 85 | 13.4 | |||||||
| From 3–4 | 9 | 1.4 | |||||||
| From 4–6 | 6 | 0.9 | |||||||
| From 6–8 | 2 | 0.3 | |||||||
| Hospitalization time | ≤1 week | 392 | 61.9 | ||||||
| ≤1 month | 148 | 23.4 | |||||||
| <6 months | 50 | 7.9 | |||||||
| <2 years | 20 | 3.2 | |||||||
| ≥2 years | 23 | 3.6 | |||||||
| Diagnosis | Leukemia | 280 | 44.2 | ||||||
| Lymphoma | 157 | 24.8 | |||||||
| CNS tumors | 83 | 13.1 | |||||||
| Rhabdomyosarcoma | 44 | 6.9 | |||||||
| Neuroblastoma | 33 | 5.2 | |||||||
| Wilms’ tumor | 20 | 3.2 | |||||||
| Retinoblastoma | 13 | 2.1 | |||||||
| Bone tumors | 3 | 0.5 | |||||||
| χ2 | χ2 | df | p | χ2/df | RMSEA (90% CI) | TLI | CFI | GFI | AGFI | SRMR |
|---|---|---|---|---|---|---|---|---|---|---|
| 1. Five factors [32]. Subsample A (n = 316) | ||||||||||
| 2537.851 | 935 | <0.001 | 2.714 | 0.074 (0.070, 0.077) | 0.742 | 0.756 | 0.693 | 0.652 | 0.073 | |
| 2. Four factors with 33 items (EFA). Subsample A (n = 316) | ||||||||||
| 1441.219 | 489 | <0.001 | 2.947 | 0.079 (0.074, 0.083) | 0.806 | 0.820 | 0.773 | 0.739 | 0.063 | |
| 3a. Three factors for socio-family support with 16 items (CFA). Subsample A (n = 316) | ||||||||||
| 213.231 | 101 | <0.001 | 2.111 | 0.059 (0.048, 0.071) | 0.931 | 0.942 | 0.926 | 0.901 | 0.055 | |
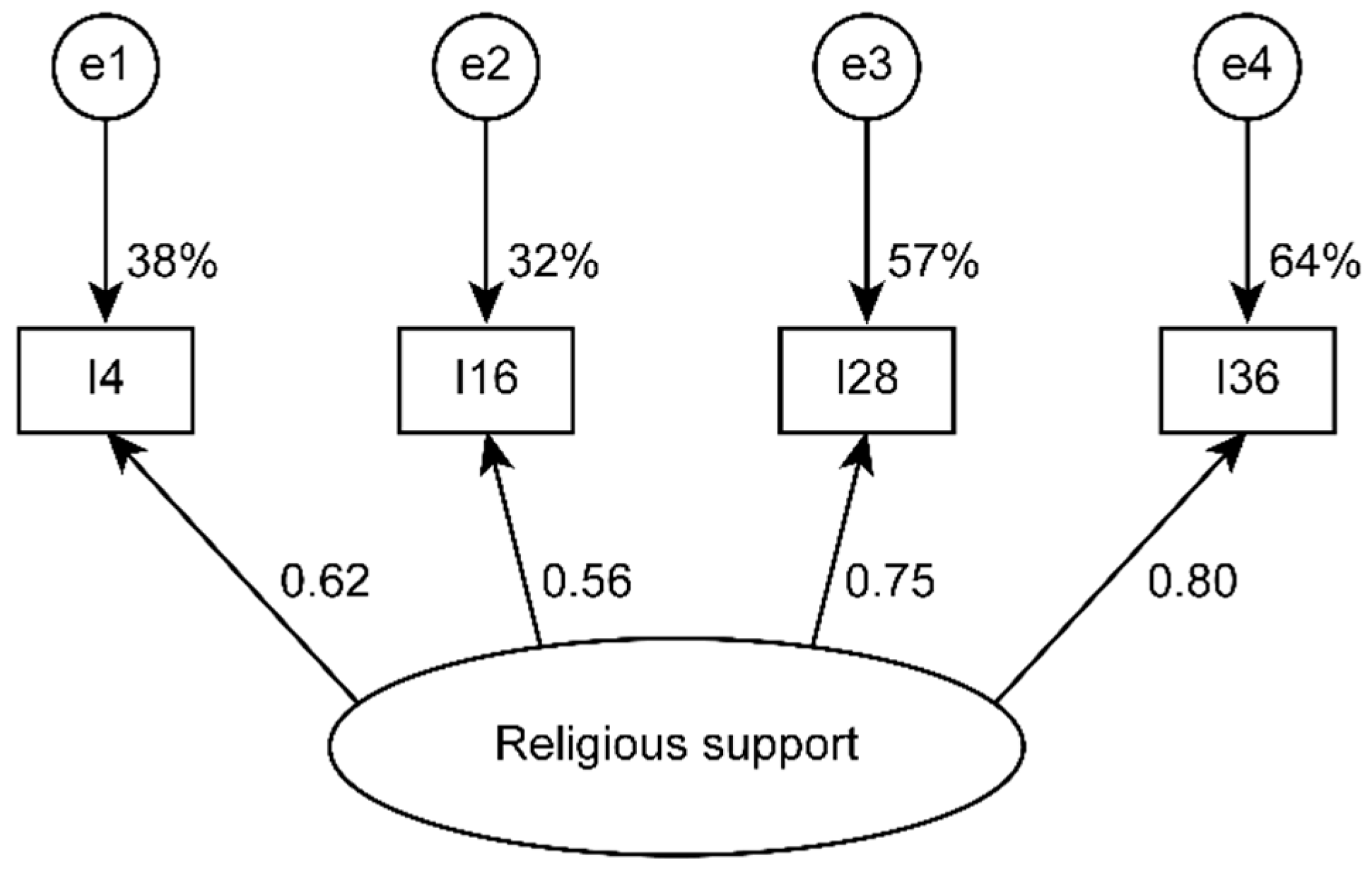
| 3b. Single-factor model with 4 indicators for religious support. Subsample A (n = 316) | ||||||||||
| 4.792 | 2 | 0.091 | 2.396 | 0.067 (0, 0.146) | 0.975 | 0.992 | 0.993 | 0.964 | 0.022 | |
| 4a. Three factors for socio-family support with 16 items. Subsample B (n = 317) | ||||||||||
| 275.856 | 101 | <0.001 | 2.731 | 0.074 (0.064, 0.085) | 0.909 | 0.923 | 0.903 | 0.870 | 0.056 | |
| 4b. Single-factor model with 4 indicators for religious support. Subsample B (n = 317) | ||||||||||
| 0.378 | 2 | 0.828 | 0.189 | 0 (0, 0.066) | 1 | 1 | 0.999 | 0.997 | 0.006 |
| Models | NI | Sample | ||||||
|---|---|---|---|---|---|---|---|---|
| Total (n = 633) | B (n = 317) | |||||||
| λ2 | ω | AVE | r2Fi,F2 | r2Fi,F3 | r2Fi,F4 | r2Fi,F5 | ||
| López-Peñaloza [32] | 45 | 0.926 | ||||||
| F1: Friend support | 15 | 0.913 | 0.912 | 0.414 | 0.236 | 0.099 | 0.017 | 0.908 |
| F2: Family support | 15 | 0.921 | 0.924 | 0.456 | 0.346 | 0.008 | 0.238 | |
| F3: Lack of support | 7 | 0.703 | 0.698 | 0.272 | <0.001 | 0.079 | ||
| F4: Religious support | 4 | 0.775 | 0.779 | 0.474 | 0.027 | |||
| F5: Neighbor support | 4 | 0.606 | 0.576 | 0.269 | ||||
| EFA—4 factors | 33 | 0.908 | ||||||
| Adjusted model: 4 factors | 20 | 0.846 | ||||||
| SFS-16: 3 factors | 16 | 0.875 | ||||||
| F1: Family support | 6 | 0.881 | 0.888 | 0.571 | 0.130 | 0.293 | ||
| F2: Friend support | 6 | 0.865 | 0.881 | 0.554 | 0.053 | |||
| F3: Lack of support | 4 | 0.717 | 0.714 | 0.387 | ||||
| Single-factor model for religious support | 4 | 0.775 | 0.781 | 0.476 | ||||
| Items | Statistics | Structure Loadings | ||||
|---|---|---|---|---|---|---|
| M | SD | FAS | FRS | RS | LS | |
| 1. My family cares for me as I care for them. | 4.263 | 0.975 | 0.712 | |||
| 3. In my family, we are all equally important. | 4.525 | 0.806 | 0.695 | |||
| 4. My faith in God helps me overcome any difficulty. | 4.351 | 0.855 | 0.630 | |||
| 7. My family trusts me, and I trust them. | 4.411 | 0.802 | 0.671 | |||
| 8. I feel supported by my parents. | 4.218 | 1.095 | 0.668 | |||
| 9. Our family is very close. | 4.174 | 1.020 | 0.788 | |||
| 12. I have my partner’s support. | 4.095 | 1.261 | 0.470 | |||
| 14. We talk about problems in our family. | 4.196 | 0.985 | 0.727 | |||
| 15. When a problem comes up in my family, we solve it violently. | 1.595 | 0.926 | 0.466 | |||
| 16. When I have problems, I go to church. | 3.266 | 1.112 | 0.510 | |||
| 18. My friends and I get together to talk, go to parties, go to the movies, etc. | 2.987 | 1.171 | 0.629 | |||
| 21. In my family, we encourage each other to improve ourselves. | 4.222 | 0.916 | 0.752 | |||
| 22. My friends and I know very little about each other. | 2.722 | 1.095 | 0.523 | |||
| 23. My family and I cannot spend much time together because we fight. | 2.101 | 1.161 | 0.632 | |||
| 24. My friends support me when I need them. | 3.592 | 1.036 | 0.555 | |||
| 25. There is not enough trust in my family. | 2.196 | 1.232 | 0.455 | |||
| 26. It is difficult to work with friends because we end up fighting. | 2.203 | 1.091 | 0.596 | |||
| 27. At work, most of my colleagues and I form a team to stay ahead. | 3.623 | 1.005 | 0.500 | |||
| 28. Prayer groups help me overcome things. | 3.649 | 1.177 | 0.715 | |||
| 30. My friends and I know each other very well. | 3.294 | 0.972 | 0.680 | |||
| 31. Outside of work, my colleagues and I get together to go out. | 3.098 | 1.051 | 0.683 | |||
| 33. When someone gets sick in my family, everyone worries. | 4.373 | 0.963 | 0.708 | |||
| 34. My friends and I visit each other’s houses. | 3.307 | 1.091 | 0.694 | |||
| 35. At work, we hide information that is useful for everyone. | 2.373 | 1.017 | 0.457 | |||
| 36. My religious beliefs help me overcome any problem. | 3.899 | 1.079 | 0.850 | |||
| 37. Living within my family is excellent. | 3.949 | 0.914 | 0.742 | |||
| 38. My friends seek each other to discuss our problems. | 3.446 | 1.011 | 0.740 | |||
| 39. At work, we lend each other books, articles, etc. | 3.089 | 1.041 | 0.651 | |||
| 41. In my family, we are very communicative with each other. | 3.953 | 1.027 | 0.727 | |||
| 42. My friends and I think friendship comes first. | 3.589 | 0.944 | 0.689 | |||
| 43. It is normal to speak openly in our family. | 4.028 | 0.934 | 0.756 | |||
| 44. Despite our activities, we make time to spend as a family. | 4.142 | 0.927 | 0.740 | |||
| 45. My friends and I think that our friendship is valuable. | 3.788 | 0.954 | 0.813 | |||
| Number of items | 13 | 10 | 4 | 6 | ||
| Guttman’s λ2 | 0.924 | 0.887 | 0.774 | 0.721 | ||
| Statistics | SFS-16 | FAS-6 | FRS-6 | LS-4 | RSS-4 |
|---|---|---|---|---|---|
| [1, 1.8) | 0.5% | 3% | 6.6% | 47.4% | 2.7% |
| [1.8, 2.6) | 4% | 1.4% | 14.8% | 31.3% | 6.3% |
| [2.6, 3.4) | 21.8% | 7% | 38.4% | 14.7% | 19.1% |
| [3.4, 4.2) | 51% | 34.4% | 32.4% | 5.7% | 36.3% |
| [4.2, 5] | 22.7% | 54.2% | 7.7% | 0.9 | 35.6% |
| M | 3.756 | 4.176 | 3.166 | 1.989 | 3.773 |
| SD | 0.615 | 0.790 | 0.844 | 0.810 | 0.822 |
| Mdn | 3.813 | 4.333 | 3.167 | 2 | 4 |
| SIQR | 0.406 | 0.500 | 0.500 | 0.625 | 0.500 |
| ZSk | −6.938 | −17.711 | −3.557 | 7.361 | −7.907 |
| ZK3 | 4.376 | 19.644 | 0.546 | 1.165 | 2.582 |
| K2 | 67.290 *** | 699.591 *** | 12.949 *** | 55.539 *** | 69.193 *** |
| Max(│D│) | 0.060 *** | 0.148 *** | 0.098 *** | 0.123 *** | 0.132 *** |
| P10 | 3.000 | 3.333 | 2 | 1 | 2.750 |
| P20 | 3.250 | 3.667 | 2.5 | 1 | 3 |
| P25 | 3.375 | 3.833 | 2.667 | 1.250 | 3.250 |
| P30 | 3.500 | 4 | 2.833 | 1.500 | 3.500 |
| P40 | 3.625 | 4.167 | 3 | 1.750 | 3.750 |
| P50 | 3.813 | 4.333 | 3.167 | 2 | 4 |
| P60 | 4.000 | 4.500 | 3.500 | 2 | 4 |
| P70 | 4.125 | 4.667 | 3.667 | 2.250 | 4.250 |
| P75 | 4.188 | 4.833 | 3.667 | 2.500 | 4.250 |
| P80 | 4.250 | 4.833 | 3.833 | 2.750 | 4.500 |
| P90 | 4.438 | 5 | 4.167 | 3 | 4.750 |
| Scale | Factor | λ2 | SFS-16 | FAS-6 | FRS-6 | LS-4 | RSS-4 |
|---|---|---|---|---|---|---|---|
| Family functioning scale | 0.888 | 0.642 ** | 0.616 ** | 0.309 ** | −0.600 ** | 0.020 ns | |
| Positive family environment | 0.789 | 0.584 ** | 0.579 ** | 0.304 ** | −0.467 ** | 0.037 ns | |
| Cohesion | 0.804 | 0.536 ** | 0.597 ** | 0.251 ** | −0.439 ** | 0.073 ns | |
| Hostility | 0.679 | −0.394 ** | −0.422 ** | −0.156 ** | 0.409 ** | −0.037 ns | |
| Troubles with rules/feelings | 0.695 | −0.481 ** | −0.368 ** | −0.243 ** | 0.533 ** | 0.043 ns | |
| Quality of life scale | Quality of life scale | 0.866 | 0.411 ** | 0.385 ** | 0.233 ** | −0.316 ** | −0.078 ns |
| Physical health | 0.529 | 0.182 ** | 0.159 ** | 0.102 * | −0.123 ** | −0.086 * | |
| Psychological health | 0.568 | 0.330 ** | 0.341 ** | 0.174 ** | −0.263 ** | 0.020 ns | |
| Social relationships | 0.680 | 0.418 ** | 0.357 ** | 0.258 ** | −0.344 ** | −0.039 ns | |
| Environment | 0.763 | 0.397 ** | 0.354 ** | 0.245 ** | −0.310 ** | −0.102 ** | |
| General quality of life | - | 0.385 ** | 0.407 ** | 0.174 ** | −0.267 ** | −0.006 ns | |
| Health condition | - | 0.346 ** | 0.330 ** | 0.182 ** | −0.271 ** | −0.014 ns | |
| Resilience scale | 0.952 | 0.438 ** | 0.493 ** | 0.234 ** | −0.329 ** | 0.070 ns | |
| Strength and confidence | 0.938 | 0.263 ** | 0.329 ** | 0.100 * | −0.231 ** | −0.024 ns | |
| Social competence | 0.863 | 0.343 ** | 0.288 ** | 0.291 ** | −0.226 ** | 0.103 ** | |
| Family support | 0.893 | 0.493 ** | 0.590 ** | 0.181 ** | −0.391 ** | 0.061 ns | |
| Social support | 0.917 | 0.526 ** | 0.546 ** | 0.297 ** | −0.377 ** | 0.125 ** | |
| Structure | 0.760 | 0.172 ** | 0.216 ** | 0.152 ** | −0.033ns | 0.070 ns |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Toledano-Toledano, F.; Moral de la Rubia, J.; Reyes Frometa, R.; González Betanzos, F.; Villavicencio Guzmán, L.; Salazar García, M. The Social Support Networks Scale (SSNS) for Family Caregivers of Children with Cancer: A Psychometric Evaluation. Int. J. Environ. Res. Public Health 2020, 17, 7820. https://doi.org/10.3390/ijerph17217820
Toledano-Toledano F, Moral de la Rubia J, Reyes Frometa R, González Betanzos F, Villavicencio Guzmán L, Salazar García M. The Social Support Networks Scale (SSNS) for Family Caregivers of Children with Cancer: A Psychometric Evaluation. International Journal of Environmental Research and Public Health. 2020; 17(21):7820. https://doi.org/10.3390/ijerph17217820
Chicago/Turabian StyleToledano-Toledano, Filiberto, José Moral de la Rubia, René Reyes Frometa, Fabiola González Betanzos, Laura Villavicencio Guzmán, and Marcela Salazar García. 2020. "The Social Support Networks Scale (SSNS) for Family Caregivers of Children with Cancer: A Psychometric Evaluation" International Journal of Environmental Research and Public Health 17, no. 21: 7820. https://doi.org/10.3390/ijerph17217820