Application of Epidemiological Geographic Information System: An Open-Source Spatial Analysis Tool Based on the OMOP Common Data Model



Abstract
:1. Introduction
2. Materials and Methods
2.1. AEGIS
2.2. Standardized Databases: OMOP-CDM and GADM
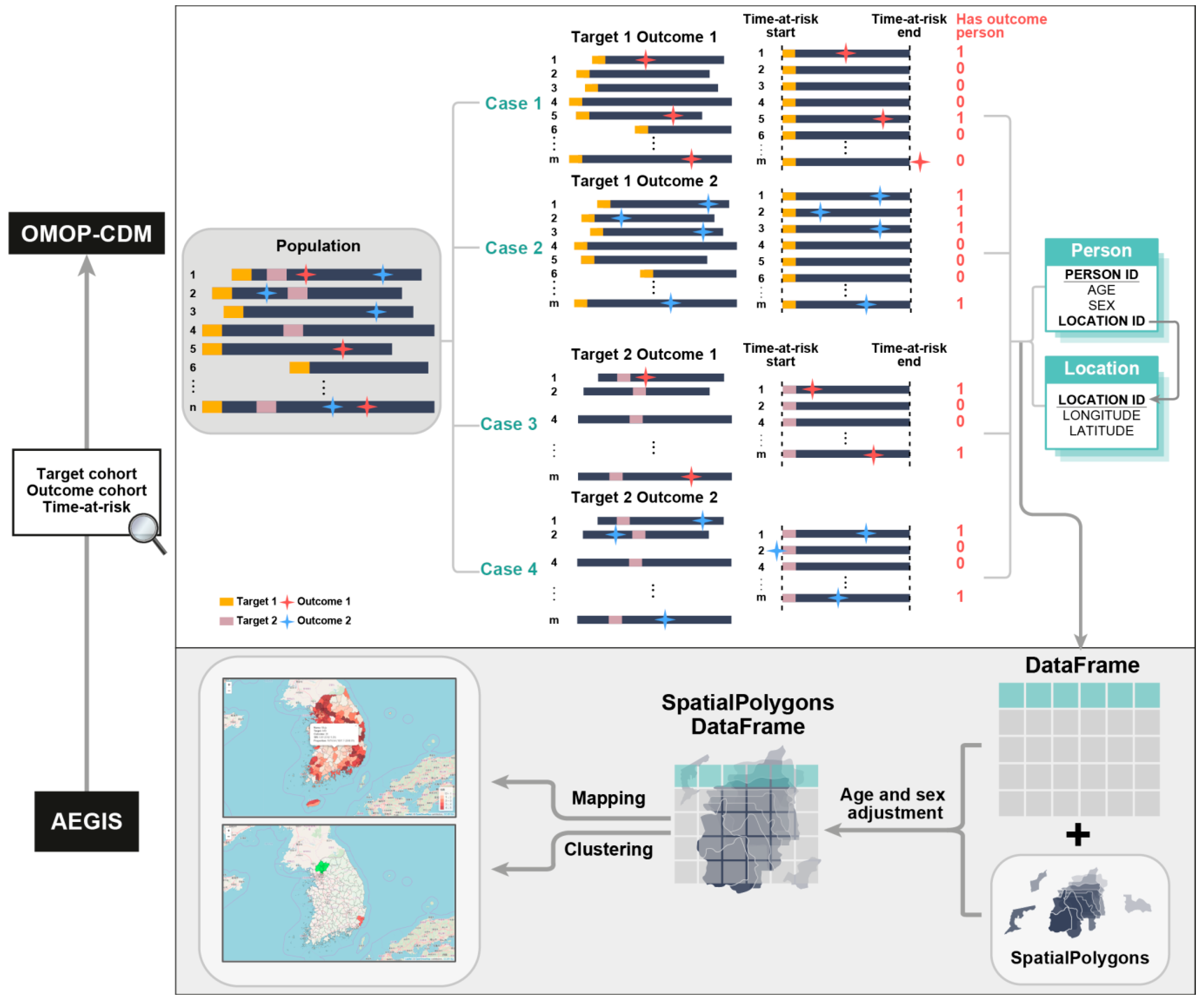
2.3. Overview of the Process Model in AEGIS
2.4. Spatial Statistics
2.5. Data Sources
2.6. Code Availability
2.7. Data Availability
2.8. Applicability of AEGIS
2.9. Verification of Methodological Quality of AEGIS
3. Results
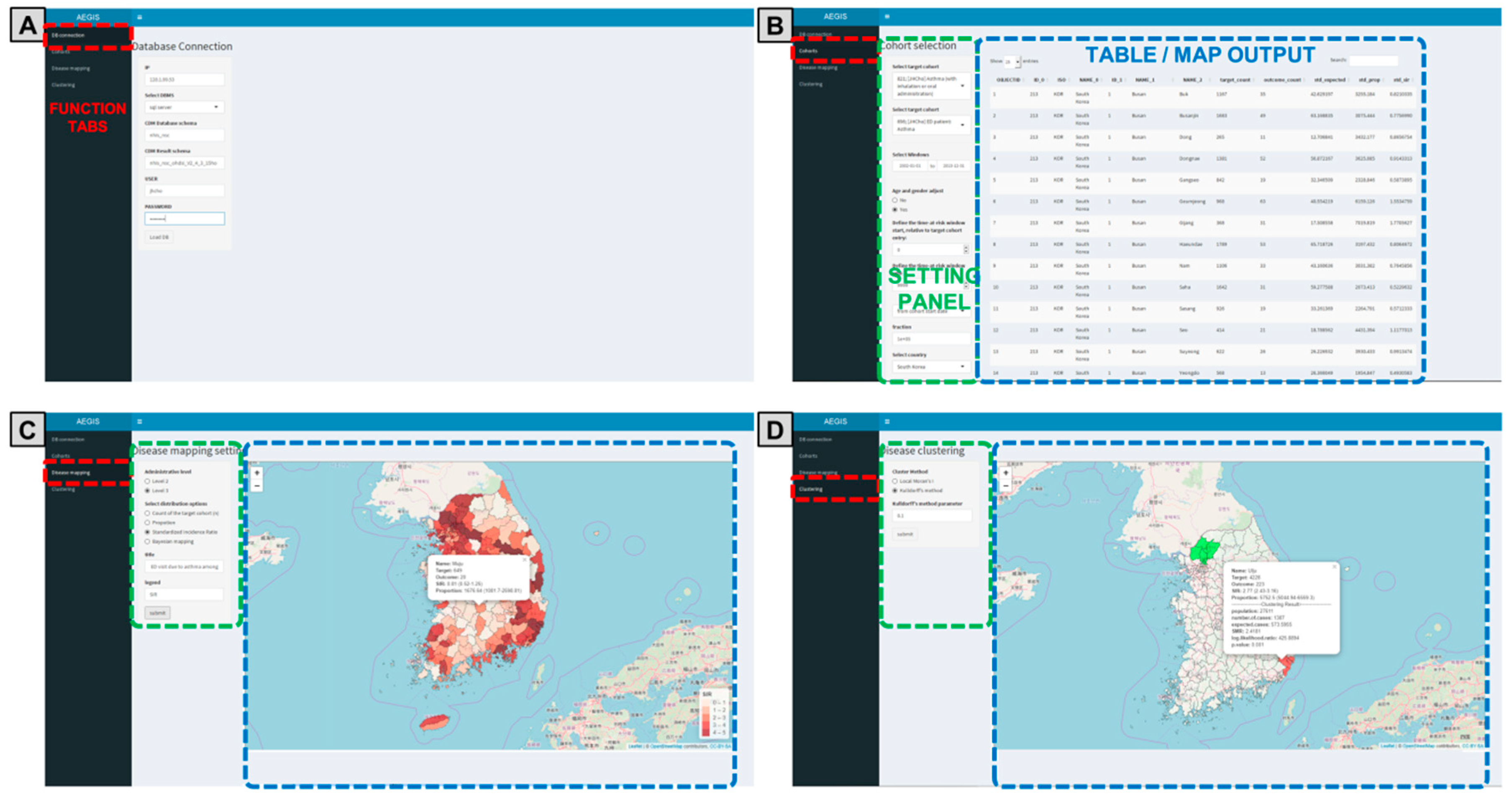
3.1. Graphical User Interface of AEGIS
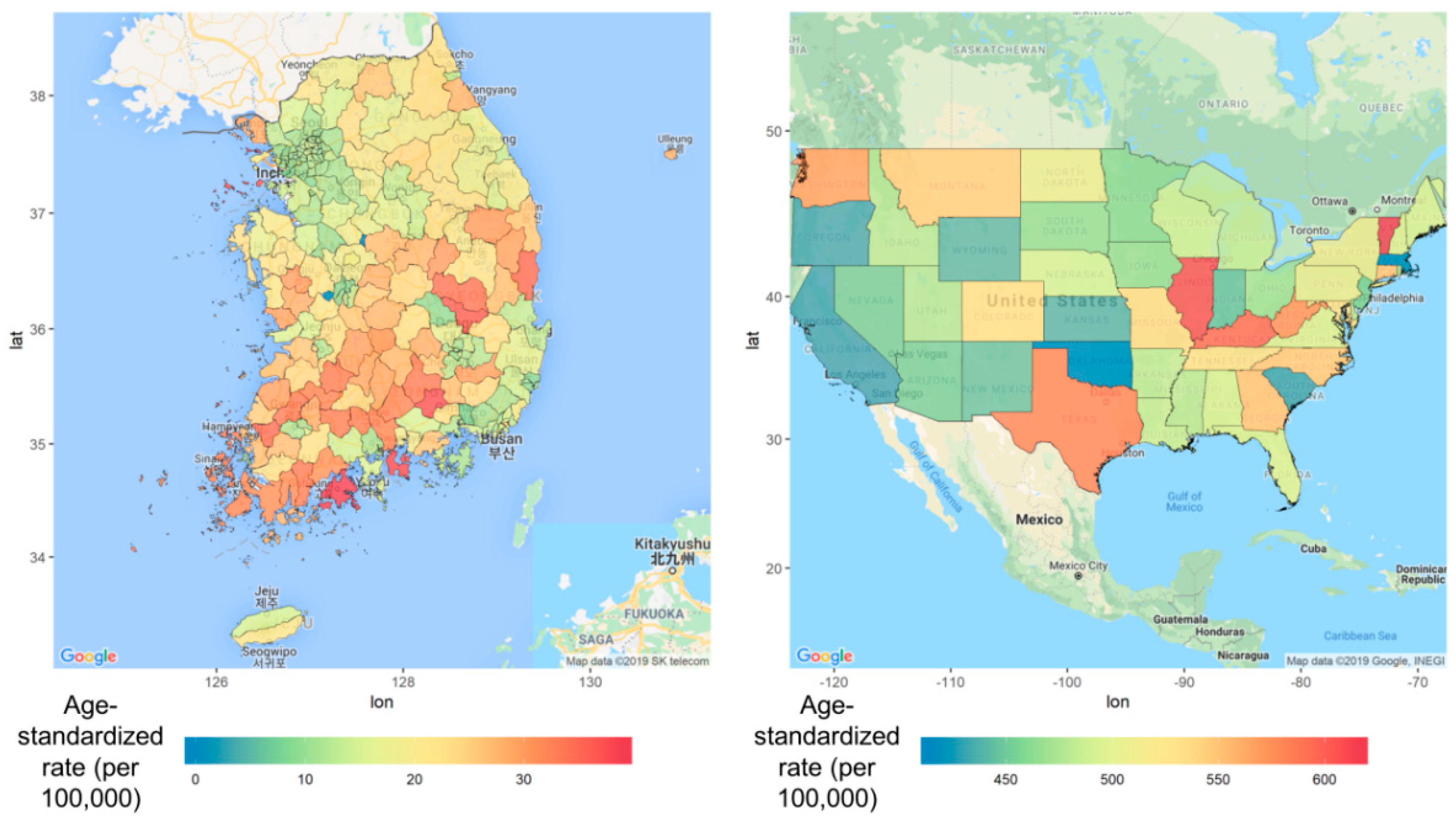
3.2. Geographical Distribution of Major Cancers
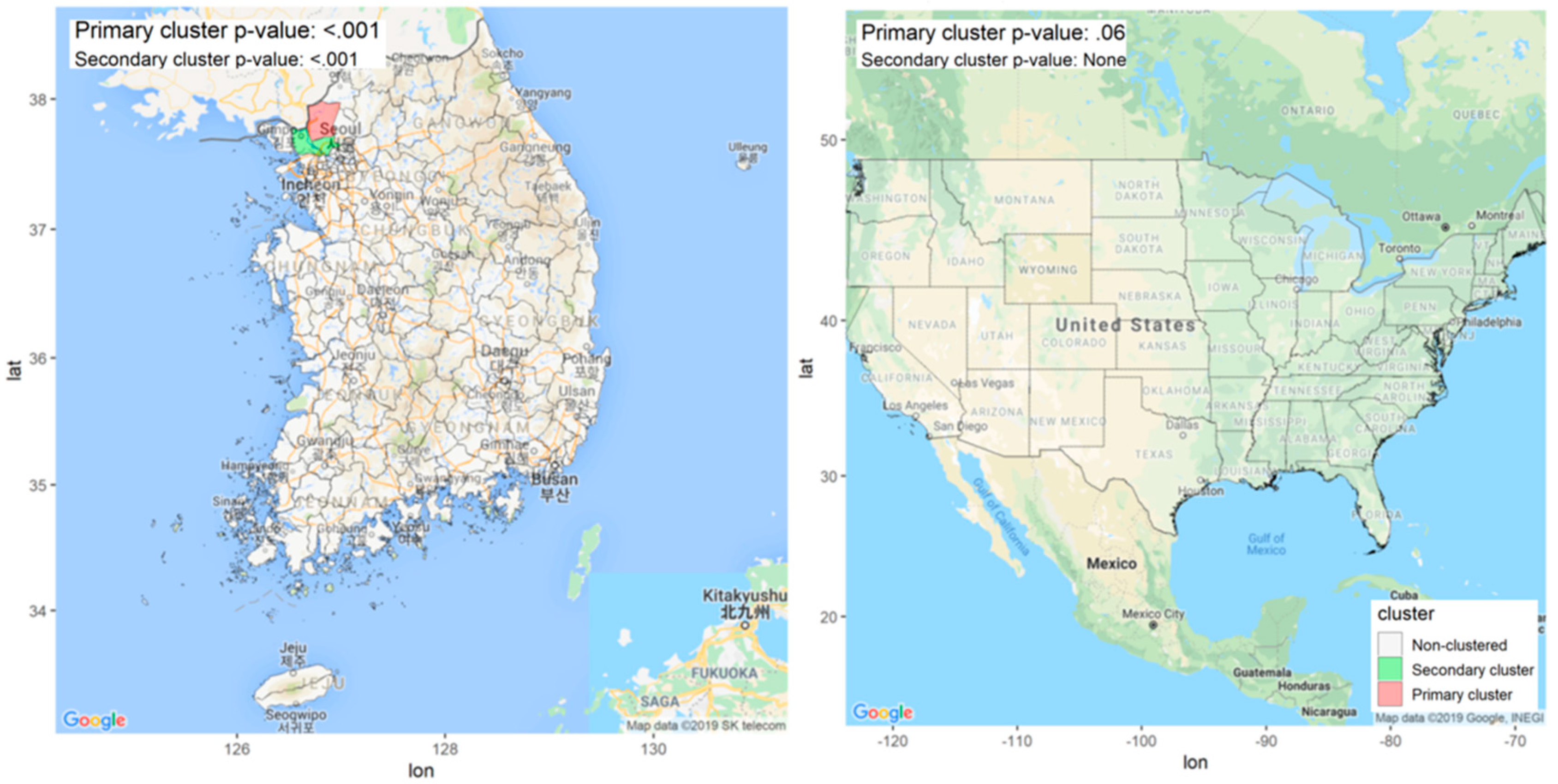
3.3. Identification of Endemic Areas of Malaria
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lansdorp-Vogelaar, I.; Goede, S.L.; Ma, J.; Xiau-Cheng, W.; Pawlish, K.; Van Ballegooijen, M.; Jemal, A. State disparities in colorectal cancer rates: Contributions of risk factors, screening, and survival differences. Cancer 2015, 121, 3676–3683. [Google Scholar] [CrossRef] [Green Version]
- Dwyer-Lindgren, L.; Bertozzi-Villa, A.; Stubbs, R.W.; Morozoff, C.; Kutz, M.J.; Huynh, C.; Barber, R.M.; Shackelford, K.A.; Mackenbach, J.P.; Van Lenthe, F.J.; et al. US county-level trends in mortality rates for major causes of death, 1980–2014. JAMA J. Am. Med. Assoc. 2016, 316, 2385–2401. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cliff, A.D.; Ord, J.K. Spatial Autocorrelation; Pion: London, UK, 1973; Available online: https://journals.sagepub.com/doi/abs/10.1177/030913259501900205?journalCode=phgb (accessed on 20 September 2020).
- Besag, J. Rejoinder. Ann. Inst. Stat. Math. 1991, 43, 45–59. [Google Scholar] [CrossRef]
- Anselin, L. Local Indicators of Spatial Association—LISA. Geogr. Anal. 1995, 27, 93–115. [Google Scholar] [CrossRef]
- Kulldorff, M. A spatial scan statistic. Commun. Stat. Methods 1997, 26, 1481–1496. [Google Scholar] [CrossRef]
- Elliott, P.; Wartenberg, D. Spatial epidemiology: Current approaches and future challenges. Environ. Health Perspect. 2004, 112, 998–1006. [Google Scholar] [CrossRef]
- Kihal, W.; Padilla, C.; Deguen, S. The need for, and value of, a spatial scan statistical tool for tackling social health inequalities. Glob. Health Promot. 2017, 24, 99–102. [Google Scholar] [CrossRef]
- Hripcsak, G.; Duke, J.D.; Shah, N.H.; Reich, C.G.; Huser, V.; Schuemie, M.J.; Suchard, M.A.; Park, R.W.; Wong, I.C.K.; Rijnbeek, P.R.; et al. Observational Health Data Sciences and Informatics (OHDSI): Opportunities for Observational Researchers. Stud. Health Technol. Inform. 2015, 216, 574–578. [Google Scholar] [CrossRef]
- Hripcsak, G.; Ryan, P.B.; Duke, J.D.; Shah, N.H.; Park, R.W.; Huser, V.; Suchard, M.A.; Schuemie, M.J.; DeFalco, F.J.; Perotte, A.; et al. Characterizing treatment pathways at scale using the OHDSI network. Proc. Natl. Acad. Sci. USA 2016, 113, 7329–7336. [Google Scholar] [CrossRef] [Green Version]
- Home OHDSI/CommonDataModel Wiki. Available online: https://github.com/ohdsi/commondatamodel/wiki (accessed on 27 May 2020).
- You, S.C.; Lee, S.; Cho, S.Y.; Park, H.; Jung, S.; Cho, J.; Yoon, D.; Park, R.W. Conversion of National Health Insurance Service-National Sample Cohort (NHIS-NSC) Database into Observational Medical Outcomes Partnership-Common Data Model (OMOP-CDM). Stud. Health Technol. Inform. 2017, 245, 467–470. [Google Scholar] [CrossRef]
- Resources:2019_data_network [Observational Health Data Sciences and Informatics]. Available online: https://www.ohdsi.org/web/wiki/doku.php?id=resources:2019_data_network (accessed on 13 October 2019).
- GADM. GADM Database of Global Administrative Areas-Version 2.8. 2018. Available online: http://www.gadm.org (accessed on 20 September 2020).
- Team, R.C. R: A Language and Environment for Statistical Computing. 2013. Available online: https://cran.r-project.org/ (accessed on 25 October 2020).
- Chang, W.; Cheng, J.; Allaire, J.; Xie, Y.; McPherson, J. Shiny: Web application framework for R. R Package Version 2017. Available online: https://cran.r-project.org/web/packages/shiny/index.html (accessed on 25 October 2020).
- Hernán, M.A.; Robins, J.M. Using Big Data to Emulate a Target Trial When a Randomized Trial Is Not Available. Am. J. Epidemiol. 2016, 183, 758–764. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Documentation: Software: Atlas [Observational Health Data Sciences and Informatics]. Available online: http://www.ohdsi.org/web/wiki/doku.php?id=documentation:software:atlas (accessed on 30 November 2018).
- Hripcsak, G.; Shang, N.; Peissig, P.L.; Rasmussen, L.V.; Liu, C.; Benoit, B.; Carroll, R.J.; Carrell, D.S.; Denny, J.C.; Dikilitas, O.; et al. Facilitating phenotype transfer using a common data model. J. Biomed. Inform. 2019, 96, 103253. [Google Scholar] [CrossRef] [PubMed]
- Lindgren, F.; Rue, H. Bayesian Spatial Modelling with R-INLA. J. Stat. Softw. 2015, 63. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.; Lee, J.S.; Park, S.H.; Shin, S.A.; Kim, K.W. Cohort Profile: The National Health Insurance Service-National Sample Cohort (NHIS-NSC), South Korea. Int. J. Epidemiol. 2017, 46, e15. [Google Scholar] [CrossRef]
- ETL-NHIS_NSC. Available online: https://github.com/OHDSI/ETL---Korean-NSC (accessed on 7 May 2019).
- OHDSI/ETL-CMS: Workproducts to ETL CMS Datasets into OMOP Common Data Model. Available online: https://github.com/OHDSI/ETL-CMS (accessed on 5 July 2019).
- Jaehyeong, C. Application for Epidemiological Geographic Information System (AEGIS): An Open Source Spatial Analysis Tool Based on CDM. Available online: https://github.com/ohdsi/aegis (accessed on 20 September 2020).
- National Health Insurance Data Sharing Service. Available online: https://nhiss.nhis.or.kr/bd/ab/bdaba000eng.do;jsessionid=FO28A6WJMpDaJqefHZmShBa1a4Eywx8xeH0RGFasM8AFME8j4nIHEWsgW3KwgfG1.primrose22_servlet_engine1 (accessed on 28 May 2020).
- CMS 2008-2010 Data Entrepreneurs’ Synthetic Public Use File (DE-SynPUF) | CMS. Available online: https://www.cms.gov/Research-Statistics-Data-and-Systems/Downloadable-Public-Use-Files/SynPUFs/DE_Syn_PUF (accessed on 28 May 2020).
- Roth, G.A.; Abate, D.; Abate, K.H.; Abay, S.M.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdela, J.; Abdelalim, A.; et al. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1736–1788. [Google Scholar] [CrossRef] [Green Version]
- Yabroff, K.R.; Lund, J.; Kepka, D.; Mariotto, A. Economic Burden of Cancer in the US. Cancer Epidemiol. Biomark. Prev. 2011, 20, 2006–2014. [Google Scholar] [CrossRef] [Green Version]
- Lee, K.S.; Chang, H.S.; Lee, S.M.; Park, E.C. Economic burden of cancer in Korea during 2000–2010. Cancer Res. Treat. 2015, 47, 387–398. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. World Malaria Report 2015; World Health Organization: Geneva, Switzerland, 2016; ISBN 9241565152. [Google Scholar]
- Autino, B.; Noris, A.; Russo, R.; Castelli, F. Epidemiology of malaria in endemic areas. Mediterr. J. Hematol. Infect. Dis. 2012, 4. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Interactive Atlas of Heart Disease and Stroke; CDC: Atlanta, GA, USA, 2014.
- KOSIS KOrean Statistical Information Service. Available online: http://kosis.kr/eng/ (accessed on 7 May 2019).
- Jung, K.W.; Won, Y.J.; Kong, H.J.; Lee, E.S.; Kim, C.H.; Yoo, C.I.; Kim, Y.D.; Nam, H.S.; Huh, J.S.; Youm, J.H.; et al. Cancer statistics in Korea: Incidence, mortality, survival, and prevalence in 2016. Cancer Res. Treat. 2019, 51, 417–430. [Google Scholar] [CrossRef] [Green Version]
- Moon, J.J.; Cho, S.Y. Incidence patterns of vivax malaria in civilians residing in a high-risk county of Kyonggi-do (province), Korea. Korean J. Parasitol. 2001, 39, 293–299. [Google Scholar] [CrossRef] [Green Version]
- Hwang, S.M.; Yoon, S.J.; Jung, Y.M.; Kwon, G.Y.; Jo, S.N.; Jang, E.J.; Kwon, M.O. Assessing the impact of meteorological factors on malaria patients in demilitarized zones in Republic of Korea. Infect. Dis. Poverty 2016, 5, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Battle, K.E.; Lucas, T.C.D.; Nguyen, M.; Howes, R.E.; Nandi, A.K.; Twohig, K.A.; Pfeffer, D.A.; Cameron, E.; Rao, P.C.; Casey, D.; et al. Mapping the global endemicity and clinical burden of Plasmodium vivax, 2000–2017: A spatial and temporal modelling study. Lancet 2019, 394, 332–343. [Google Scholar] [CrossRef] [Green Version]
- Won, Y.; Jung, K.; Oh, C.; Kong, H.; Lee, D.H.; Lee, K.H. Geographical Variations and Trends in Major Cancer Incidences throughout Korea during 1999–2013. Cancer Res. Treat. Off. J. Korean Cancer Assoc. 2018, 50, 1281–1293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chai, J.Y. Re-emerging Plasmodium vivax malaria in the Republic of Korea. Korean J. Parasitol. 1999, 37, 129–143. [Google Scholar] [CrossRef] [Green Version]
- Han, E.T.; Lee, D.H.; Park, K.D.; Seok, W.S.; Kim, Y.S.; Tsuboi, T.; Shin, E.H.; Chai, J.Y. Reemerging vivax malaria: Changing patterns of annual incidence and control programs in the Republic of Korea. Korean J. Parasitol. 2006, 44, 285–294. [Google Scholar] [CrossRef] [Green Version]
- Mace, K.E.; Arguin, P.M.; Lucchi, N.W.; Tan, K.R. Malaria Surveillance—United States, 2016. MMWR. Surveill. Summ. 2019, 68, 1–35. [Google Scholar] [CrossRef] [Green Version]
- Lanska, D.J.; Kryscio, R. Geographic distribution of hospitalization rates, case fatality, and mortality from stroke in the United States. Neurology 1994, 44, 1541. [Google Scholar] [CrossRef]
- El-Saed, A.; Kuller, L.H.; Newman, A.B.; Lopez, O.; Costantino, J.; McTigue, K.; Cushman, M.; Kronmal, R. Geographic variations in stroke incidence and mortality among older populations in four US communities. Stroke 2006, 37, 1975–1979. [Google Scholar] [CrossRef] [Green Version]
- Reis, B.Y.; Kirby, C.; Hadden, L.E.; Olson, K.; McMurry, A.J.; Daniel, J.B.; Mandl, K.D. AEGIS: A robust and scalable real-time public health surveillance system. J. Am. Med. Inform. Assoc. 2007, 14, 581–588. [Google Scholar] [CrossRef] [Green Version]
- Moraga, P. SpatialEpiApp: A Shiny web application for the analysis of spatial and spatio-temporal disease data. Spat. Spatiotemporal. Epidemiol. 2017, 23, 47–57. [Google Scholar] [CrossRef] [Green Version]
- Song, C.; Shi, X.; Bo, Y.; Wang, J.; Wang, Y.; Huang, D. Exploring spatiotemporal nonstationary effects of climate factors on hand, foot, and mouth disease using Bayesian Spatiotemporally Varying Coefficients (STVC) model in Sichuan, China. Sci. Total Environ. 2019, 648, 550–560. [Google Scholar] [CrossRef] [PubMed]
- Song, C.; Shi, X.; Wang, J. Spatiotemporally Varying Coefficients (STVC) model: A Bayesian local regression to detect spatial and temporal nonstationarity in variables relationships. Ann. GIS 2020, 26, 277–291. [Google Scholar] [CrossRef]
- STVCapp. Available online: https://chaosong.shinyapps.io/stvcapp/ (accessed on 18 October 2020).
- Kim, D.Y.; Kim, I.H.; Jeong, S.H.; Cho, Y.K.; Lee, J.H.; Jin, Y.J.; Lee, D.; Suh, D.J.; Han, K.H.; Park, N.H.; et al. A nationwide seroepidemiology of hepatitis C virus infection in South Korea. Liver Int. 2013, 33, 586–594. [Google Scholar] [CrossRef]
- Moon, S.; Han, J.H.; Bae, G.R.; Cho, E.; Kim, B. Hepatitis A in Korea from 2011 to 2013: Current epidemiologic status and regional distribution. J. Korean Med. Sci. 2016, 31, 67–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woon Kwak, C.; Han, K.T.; Mo Nam, C.; Tae Moon, K.; Yoon, H.S.; Park, E.C. Income disparity and mortality among patients with alcohol use disorder in South Korea. Psychiatry Res. 2017, 258, 358–364. [Google Scholar] [CrossRef] [PubMed]
- Barber, R.M.; Fullman, N.; Sorensen, R.J.D.; Bollyky, T.; McKee, M.; Nolte, E.; Abajobir, A.A.; Abate, K.H.; Abbafati, C.; Abbas, K.M.; et al. Healthcare Access and Quality Index based on mortality from causes amenable to personal health care in 195 countries and territories, 1990–2015: A novel analysis from the Global Burden of Disease Study 2015. Lancet 2017, 390, 231–266. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| South Korea | United States | Netherlands | |
|---|---|---|---|
| Level 1: nation | South Korea | United States | Netherlands |
| Level 2: states | Seoul | Illinois | South Holland |
| Level 3: county | Gangnam-gu | Springfield | Rotterdam |
| Cancer Site | Incidence | Mortality | |||||
|---|---|---|---|---|---|---|---|
| 2004–2008 | 2009–2013 | 2004–2008 | |||||
| Moran’s I | p-Value | Moran’s I | p-Value | Moran’s I | p-Value | ||
| Colorectal | Men | 0.08 | 0.17 | 0.05 | 0.23 | −0.06 | 0.23 |
| Women | −0.01 | 0.95 | 0.03 | 0.56 | −0.06 | 0.56 | |
| Liver | Men | 0.37 | <0.001 | 0.39 | <0.001 | −0.05 | 0.05 |
| Women | 0.42 | <0.001 | 0.44 | <0.001 | −0.18 | <0.001 | |
| Lung | Men | 0.34 | <0.001 | 0.34 | <0.001 | −0.05 | <0.001 |
| Women | 0.38 | <0.001 | 0.40 | <0.001 | −0.08 | 0.58 | |
| Stomach | Men | 0.33 | <0.001 | 0.32 | <0.001 | −0.05 | 0.57 |
| Women | 0.40 | <0.001 | 0.39 | <0.001 | −0.05 | 0.45 | |
| Thyroid | Men | 0.40 | <0.001 | 0.40 | <0.001 | - | - |
| Women | 0.29 | <0.001 | 0.30 | <0.001 | - | - | |
| Breast | Men | - | - | - | - | - | - |
| Women | 0.36 | <0.001 | 0.36 | 0.08 | −0.09 | 0.05 | |
| Prostate | Men | 0.36 | <0.001 | 0.39 | <0.001 | −0.08 | 0.05 |
| Women | - | - | - | - | - | - | |
| Cancer Site | National Incidences (Cases Per 100,000 Persons) | ||||
|---|---|---|---|---|---|
| 2004–2008 | 2009–2013 | ||||
| AEGIS | Statistics Korea 1 | AEGIS | Statistics Korea 2 | ||
| Colorectal | Men | 47.2 (31.8–66.6) | 47.6 | 61.8 (41.7–86.9) | 69.5 |
| Women | 33.3 (22.2–47.2) | 33.7 | 44.5 (29.1–64.4) | 44.5 | |
| Liver | Men | 48.9 (31.3–72.3) | 45.9 | 46.4 (32.6–63.8) | 49.3 |
| Women | 17.4 (10.3–26.9) | 15.4 | 18.5 (12.2–26.2) | 17.4 | |
| Lung | Men | 59.6 (42–81.8) | 51.7 | 62.9 (47.5–80.6) | 61.5 |
| Women | 20.5 (13.5–28.9) | 20.7 | 25.1 (13.6–41.4) | 26.9 | |
| Stomach | Men | 67.4 (47.8–91.8) | 72.4 | 73.4 (52.5–99.2) | 85.8 |
| Women | 33.6 (23.9–45.4) | 35.7 | 34.1 (26.9–42) | 41.6 | |
| Thyroid | Men | 8.6 (3.1–18.5) | 9.5 | 24.8 (12.2–43.9) | 28.3 |
| Women | 52.1 (29.6–83.8) | 56.6 | 104.9 (65.8–156.9) | 136.4 | |
| Breast | Men | - | - | - | - |
| Women | 33.2 (23.3–45.0) | 44.6 | 44.9 (26.1–70.9) | 64.3 | |
| Prostate | Men | 20.7 (11–34.6) | 18.4 | 28.0 (15.3–45.9) | 36.2 |
| Women | - | - | - | - | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cho, J.; You, S.C.; Lee, S.; Park, D.; Park, B.; Hripcsak, G.; Park, R.W. Application of Epidemiological Geographic Information System: An Open-Source Spatial Analysis Tool Based on the OMOP Common Data Model. Int. J. Environ. Res. Public Health 2020, 17, 7824. https://doi.org/10.3390/ijerph17217824
Cho J, You SC, Lee S, Park D, Park B, Hripcsak G, Park RW. Application of Epidemiological Geographic Information System: An Open-Source Spatial Analysis Tool Based on the OMOP Common Data Model. International Journal of Environmental Research and Public Health. 2020; 17(21):7824. https://doi.org/10.3390/ijerph17217824
Chicago/Turabian StyleCho, Jaehyeong, Seng Chan You, Seongwon Lee, DongSu Park, Bumhee Park, George Hripcsak, and Rae Woong Park. 2020. "Application of Epidemiological Geographic Information System: An Open-Source Spatial Analysis Tool Based on the OMOP Common Data Model" International Journal of Environmental Research and Public Health 17, no. 21: 7824. https://doi.org/10.3390/ijerph17217824