Association between Psychological Factors and Evacuation Status and the Incidence of Cardiovascular Diseases after the Great East Japan Earthquake: A Prospective Study of the Fukushima Health Management Survey

 ,
,  , , , , , , , ,
, , , , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
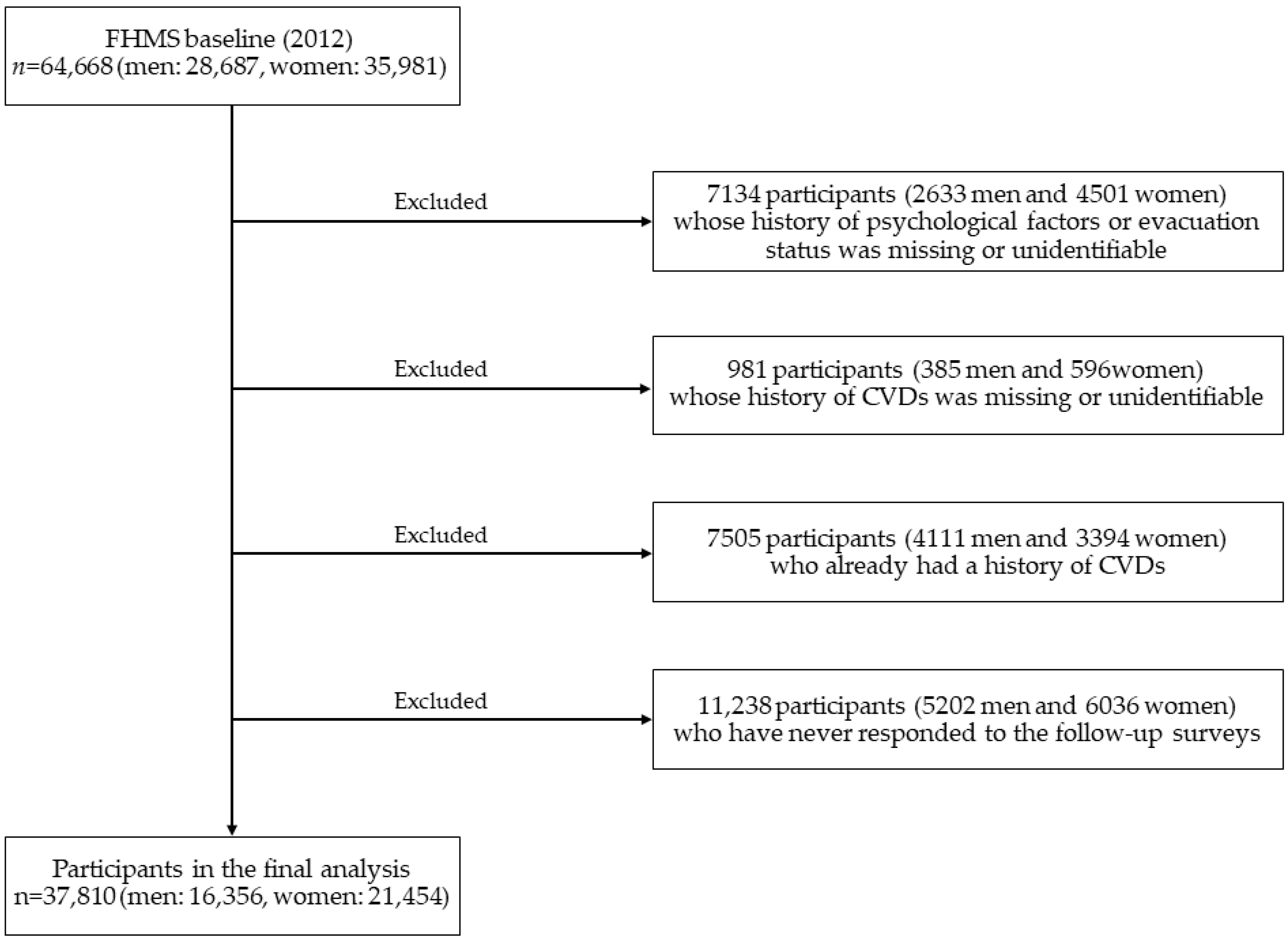
2.1. Participants
2.2. Measurements
2.2.1. Onset and Mortality of Cardiovascular Diseases
2.2.2. Psychological Factors and Evacuation Status
2.2.3. Lifestyle Behaviors, Social Factors, and Other Risk Factors for Cardiovascular Diseases
2.3. Statistical Analysis
3. Results
3.1. Cardiovascular Risk Factors of Participants at Baseline
3.2. Psychological Factors or Evacuation Status on Cardiovascular Diseases
3.3. Combination of Psychological Factors and Evacuation Status on Cardiovascular Diseases
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Yasumura, S.; Hosoya, M.; Yamashita, S.; Kamiya, K.; Abe, M.; Akashi, M.; Kodima, K.; Ozasa, K. Study protocol for the Fukushima Health Management Survey. J. Epidemiol. 2012, 22, 375–383. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trevisan, M.; Celentano, E.; Meucci, C.; Farinaro, E.; Jossa, F.; Krogh, V.; Giumetti, D.; Panico, S.; Scottoni, A.; Mancini, M. Short-term effect of natural disasters on coronary heart disease risk factors. Arterioscler. Thromb. Vasc. Biol. 1986, 6, 491–494. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kario, K.; Matsuo, T.; Kayaba, K.; Soukejima, S.; Kagamimori, S.; Shimada, K. Earthquake-induced cardiovascular disease and related risk factors in focusing on the Great Hanshin-Awaji Earthquake. J. Epidemiol. 1998, 8, 131–139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sumner, D. Health effects resulting from the Chernobyl accident. Med. Confl. Surviv. 2007, 23, 31–45. [Google Scholar] [CrossRef]
- Swerdel, J.N.; Janevic, T.M.; Cosgrove, N.M.; Kostis, J.B. Myocardial Infarction Data Acquisition System (MIDAS 24) Study Group. The effect of Hurricane Sandy on cardiovascular events in New Jersey. J. Am. Heart Assoc. 2014, 3, e001354. [Google Scholar] [CrossRef] [Green Version]
- Jordan, H.T.; Miller-Archie, S.A.; Cone, J.E.; Morabia, A.; Stellman, S.D. Heart disease among adults exposed to the September 11, 2001 World Trade Center disaster: Results from the World Trade Center Health Registry. Prev. Med. 2011, 53, 370–376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kitamura, T.; Kiyohara, K.; Iwami, T. The Great East Japan Earthquake and out-of-hospital cardiac arrest. N. Engl. J. Med. 2013, 369, 2165–2166. [Google Scholar] [CrossRef] [Green Version]
- Aoki, T.; Fukumoto, Y.; Yasuda, S.; Sakata, Y.; Ito, K.; Takahashi, J.; Miyata, S.; Tsuji, I.; Shimokawa, H. The Great East Japan Earthquake Disaster and cardiovascular diseases. Eur. Heart J. 2012, 33, 2796–2803. [Google Scholar] [CrossRef] [Green Version]
- Nakano, M.; Kondo, M.; Wakayama, Y.; Kawana, A.; Hasebe, Y.; Shafee, M.A.; Fukuda, K.; Shimokawa, H. Increased incidence of tachyarrhythmias and heart failure hospitalization in patients with implanted cardiac devices after the Great East Japan Earthquake Disaster. Circ. J. 2012, 76, 1283–1285. [Google Scholar] [CrossRef] [Green Version]
- Ho, J.E.; Paultre, F.; Mosca, L. Lifestyle changes in New Yorkers after September 11, 2001 (data from the Post-Disaster Heart Attack Prevention Program). Am. J. Cardiol. 2002, 90, 680–682. [Google Scholar] [CrossRef]
- Kario, K.; McEwen, B.S.; Pickering, T.G. Disasters and the heart: A review of the effects of earthquake-induced stress on cardiovascular disease. Hypertens. Res. 2003, 26, 355–367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vieweg, W.V.R.; Hasnain, M.; Mezuk, B.; Levy, J.R.; Lesnefsky, E.J.; Pandurangi, A.K. Depression.; stress.; and heart disease in earthquakes and Takotsubo cardiomyopathy. Am. J. Med. 2011, 124, 900–907. [Google Scholar] [CrossRef]
- Remch, M.; Laskaris, Z.; Flory, J.; Mora-McLaughlin, C.; Morabia, A. Post-traumatic stress disorder and cardiovascular diseases: A cohort study of men and women involved in cleaning the debris of the World Trade Center Complex. Circ. Cardiovasc. Qual. Outcomes 2018, 11, e004572. [Google Scholar] [CrossRef]
- Edmondson, D.; Gamboa, C.; Cohen, A.; Anderson, A.H.; Kutner, N.; Kronish, I.; Mills, M.S.; Muntner, P. Association of posttraumatic stress disorder and depression with all-cause and cardiovascular disease mortality and hospitalization among Hurricane Katrina survivors with end-stage renal disease. Am. J. Public Health 2013, 103, e130–e137. [Google Scholar] [CrossRef]
- Zhang, W.; Ohira, T.; Yasumura, S.; Maeda, M.; Otsura, A.; Harigane, M.; Horikoshi, N.; Suzuki, Y.; Yabe, H.; Nagai, M.; et al. Effects of socioeconomic factors on cardiovascular-related symptoms among residents in Fukushima after the Great East Japan Earthquake: A cross-sectional study using data from the Fukushima Health Management Survey. BMJ Open 2017, 7, e014077. [Google Scholar] [CrossRef]
- Santavirta, T. Unaccompanied evacuation and adult mortality: Evaluating the Finnish policy of evacuating children to foster care during World War II. Am. J. Public Health 2014, 104, 1759–1765. [Google Scholar] [CrossRef] [PubMed]
- Cwikel, J.; Abdelgani, A.; Goldsmith, J.R.; Quastel, M.; Yevelson, I.I. Two-year follow-up study of stress-related disorders among immigrants to Israel from the Chernobyl area. Environ. Health Perspect. 1997, 105, 1545–1550. [Google Scholar] [PubMed]
- Moriyama, N.; Iwasa, H.; Tsubokura, M.; Kuroda, Y.; Yasumura, S. Living in the Restoration Public Housing after the Great East Japan Earthquake Correlates with Lower Subjective Well-Being of Older Adults. Int. J. Environ. Res. Public Health 2019, 16, 2696. [Google Scholar] [CrossRef] [Green Version]
- Suzuki, Y.; Yabe, H.; Yasumura, S.; Ohira, T.; Niwa, S.-I.; Ohtsuru, A.; Mashiko, H.; Maeda, M.; Abe, M. Psychological distress and the perception of radiation risks: The Fukushima health management survey. Bull. World Health Organ. 2015, 93, 598–605. [Google Scholar] [CrossRef]
- Ohira, T.; Hosoya, M.; Yasumura, S.; Satoh, H.; Suzuki, H.; Sakai, A.; Ohtsuru, A.; Kawasaki, Y.; Takahashi, A.; Ozasa, K.; et al. Evacuation and risk of hypertension after the Great East Japan Earthquake: The Fukushima Health Management Survey. Hypertension 2016, 68, 558–564. [Google Scholar] [CrossRef] [PubMed]
- Ohira, T.; Hosoya, M.; Yasumura, S.; Satoh, H.; Suzuki, H.; Sakai, A.; Ohtsuru, A.; Kawasaki, Y.; Takahashi, A.; Ozasa, K.; et al. Effect of evacuation on body weight after the Great East Japan Earthquake. Am. J. Prev. Med. 2016, 50, 553–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hashimoto, S.; Nagai, M.; Fukuma, S.; Ohira, T.; Hosoya, M.; Yasumura, S.; Satoh, H.; Suzuki, H.; Sakai, A.; Ohtsuru, A.; et al. Influence of post-disaster evacuation on incidence of metabolic syndrome. J. Atheroscler. Thromb. 2017, 24, 327–337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Satoh, H.; Ohira, T.; Hosoya, M.; Sakai, A.; Watanabe, T.; Ohtsuru, A.; Kawasaki, Y.; Suzuki, H.; Takahashi, A.; Kobashi, G.; et al. Evacuation after the Fukushima Daiichi Nuclear Power Plant accident is a cause of diabetes: Results from the Fukushima Health Management Survey. J. Diabet. Res. 2015, 2015, 627390. [Google Scholar] [CrossRef] [PubMed]
- Kawasaki, Y.; Nakano, I.; Hosoya, M.; Yasumura, S.; Ohira, T.; Satoh, H.; Suzuki, H.; Sakai, A.; Ohtsuru, A.; Takahashi, A.; et al. Influence of post-disaster evacuation on childhood obesity and hyperlipidemia. Pediatr. Int. 2020, 62, 669–676. [Google Scholar] [CrossRef]
- Takahashi, A.; Ohira, T.; Hosoya, M.; Yasunura, S.; Nagai, M.; Ohira, H.; Hashimoto, S.; Satoh, H.; Sakai, A.; Ohtsuru, A.; et al. Effect of evacuation on liver function after the Fukushima Daiichi nuclear power plant accident: The Fukushima Health Management Survey. J. Epidemiol. 2017, 27, 180–185. [Google Scholar] [CrossRef]
- Hayashi, Y.; Nagai, M.; Ohira, T.; Satoh, H.; Sakai, A.; Ohtsura, A.; Hosoya, M.; Kawasaki, Y.; Suzuki, H.; Takahashi, A.; et al. The impact of evacuation on the incidence of chronic kidney disease after the Great East Japan Earthquake: The Fukushima Health Management Survey. Clin. Exp. Nephrol. 2017, 21, 995–1002. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakai, A.; Ohira, T.; Hosoya, M.; Ohtsuru, A.; Satoh, H.; Kawasaki, Y.; Suzuki, H.; Takahashi, A.; Kobashi, G.; Ozasa, K.; et al. Life as an evacuee after the Fukushima Daiichi nuclear power plant accident is a cause of polycythemia: The Fukushima Health Management Survey. BMC Public Health 2014, 14, 1318. [Google Scholar] [CrossRef] [Green Version]
- Yabe, H.; Suzuki, Y.; Mashiko, H.; Nakayama, Y.; Hisata, M.; Niwa, S.-I.; Yasumura, S.; Yamashita, S.; Kamiya, K.; Abe, M.; et al. Psychological distress after the Great East Japan Earthquake and Fukushima Daiichi Nuclear power plant accident: Results of a mental health and lifestyle survey through the Fukushima Health Management Survey in FY2011 and FY2012. Fukushima J. Med. Sci. 2014, 60, 57–67. [Google Scholar] [CrossRef] [Green Version]
- Suzuki, Y.; Yabe, H.; Horikoshi, N.; Yasumura, S.; Kawakami, N.; Ohtsura, A.; Moshiko, H.; Maeda, M. Diagnostic accuracy of Japanese posttraumatic stress measures after a complex disaster: The Fukushima Health Management Survey. Asia Pac. Psychiatry 2017, 9, e12248. [Google Scholar] [CrossRef] [Green Version]
- Iwasa, H.; Suzuki, Y.; Shiga, T.; Maeda, M.; Yabe, H.; Yasumura, S.; Mental Health Group of the Fukushima Health Management Survey. Psychometric evaluation of the Japanese version of the posttraumatic stress disorder checklist in community dwellers following the Fukushima Daiichi Nuclear Power Plant Incident: The Fukushima Health Management Survey. SAGE Open 2016, 6, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Kessler, R.C.; Adler, L.; Barkley, R.; Biederman, J.; Conners, K.; Demler, O.; Farone, S.V.; Greenhill, L.L.; Howes, M.J.; Secnik, K.; et al. The prevalence and correlates of adult ADHD in the United States: Results from the National Comorbidity Survey Replication. Am. J. Psychiatry 2006, 163, 716–723. [Google Scholar] [CrossRef]
- Furukawa, T.A.; Kessler, R.C.; Slade, T.; Andrews, G. The performance of the K6 and K10 screening scales for psychological distress in the Australian National Survey of Mental Health and Well-Being. Psychol. Med. 2003, 33, 357–362. [Google Scholar] [CrossRef] [PubMed]
- Sakurai, K.; Nishi, A.; Kondo, K.; Yanagida, K.; Kawakami, N. Screening performance of K6/K10 and other screening instruments for mood and anxiety disorders in Japan. Psychiatry Clin. Neurosci. 2011, 65, 434–441. [Google Scholar] [CrossRef] [PubMed]
- Blanchard, E.B.; Jones-Alexander, J.; Buckley, T.C.; Forneris, C.A. Psychometric properties of the PTSD Checklist (PCL). Behav. Res. Ther. 1996, 34, 669–673. [Google Scholar] [CrossRef]
- Wilcosky, T.C.; Chambless, L.E. A comparison of direct adjustment and regression adjustment of epidemiologic measures. J. Chronic. Dis. 1985, 38, 849–856. [Google Scholar] [CrossRef]
- Jordan, H.T.; Stellman, S.D.; Morabia, A.; Miller-Archie, S.A.; Alper, H.; Laskaris, Z.; Brakenbill, R.M.; Cone, J.E. Cardiovascular disease hospitalizations in relation to exposure to the September 11, 2001 World Trade Center disaster and posttraumatic stress disorder. J. Am. Heart Assoc. 2013, 2, e000431. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, K.; Deng, X.; He, D.; Huang, D.; Wu, Q.; Wen, S.; Zhou, F.; Kang, Y.; Chen, M. Prognostic implication of earthquake-related loss and depressive symptoms in patients with heart failure following the 2008 Earthquake in Sichuan. Clin. Cardiol. 2011, 34, 755–760. [Google Scholar] [CrossRef]
- Orth-Gomér, K.; Rosengren, A.; Wilhelmsen, L. Lack of social support and incidence of coronary heart disease in middle-aged Swedish men. Psychosom. Med. 1993, 55, 37–43. [Google Scholar] [CrossRef] [Green Version]
- Valtorta, N.K.; Kanaan, M.; Gilbody, S.; Ronzi, S.; Hanratty, B. Loneliness and social isolation as risk factors for coronary heart disease and stroke: Systematic review and meta-analysis of longitudinal observational studies. Heart 2016, 102, 1009–1016. [Google Scholar] [CrossRef] [Green Version]
- Eng, P.M.; Rimm, E.B.; Fitzmaurice, G.; Kawachi, I. Social ties and change in social ties in relation to subsequent total and cause-specific mortality and coronary heart disease incidence in men. Am. J. Epidemiol. 2002, 155, 700–709. [Google Scholar] [CrossRef]


{kind=link}
| Cardiovascular Risk Factors | Evacuee | Non-Evacuee | p for Difference |
|---|---|---|---|
| Men | |||
| Number at risk | 5990 | 10,336 | |
| Age (years) | 57.6 | 58.4 | <0.001 |
| Psychological distress (%) | 13.6 | 9.2 | <0.001 |
| Trauma reaction (%) | 21.1 | 14.4 | <0.001 |
| Current smoker (%) | 35.6 | 33.2 | 0.03 |
| Alcohol consumption ≥ once/month (%) | 68.6 | 71.5 | <0.001 |
| Physical activity ≥ once/month (%) | 47.8 | 47.5 | 0.38 |
| Unsatisfied with sleep (%) | 64.9 | 56.5 | <0.001 |
| Job loss (%) | 28.0 | 13.9 | <0.001 |
| Loss of family members (%) | 23.6 | 16.9 | <0.001 |
| High perception of radiation risks (%) | 61.4 | 56.4 | <0.001 |
| History of hypertension (%) | 46.4 | 44.2 | <0.001 |
| History of hyperlipidemia (%) | 39.7 | 37.0 | <0.001 |
| History of diabetes (%) | 22.6 | 21.1 | <0.001 |
| Family history of CVD | 35.2 | 35.8 | 0.47 |
| Women | |||
| Number at risk | 8172 | 13,282 | |
| Age (years) | 55.7 | 56.5 | <0.001 |
| Psychological distress (%) | 18.5 | 13.9 | <0.001 |
| Trauma reaction (%) | 27.1 | 20.5 | <0.001 |
| Current smoker (%) | 10.7 | 9.3 | 0.02 |
| Alcohol consumption ≥ once/month (%) | 30.6 | 30.6 | 0.38 |
| Physical activity ≥ once/month (%) | 52.3 | 53.3 | 0.002 |
| Unsatisfied with sleep (%) | 75.7 | 67.1 | <0.001 |
| Job loss (%) | 33.9 | 18.8 | <0.001 |
| Loss of family members (%) | 24.8 | 18.2 | <0.001 |
| High perception of radiation risks (%) | 67.5 | 62.5 | <0.001 |
| History of hypertension (%) | 37.6 | 36.9 | <0.001 |
| History of hyperlipidemia (%) | 35.7 | 34.7 | 0.002 |
| History of diabetes (%) | 14.7 | 15.1 | 0.67 |
| Family history of CVD | 37.2 | 38.2 | 0.14 |
| Men | Women | p for Interaction a | |
|---|---|---|---|
| Person-years | 59,087 | 79,350 | |
| Psychological distress | |||
| Total CVD (n) | 301 | 449 | |
| Incidence rate/1000 person-years | 5.09 | 5.66 | |
| Model 1 b | 1.48 (1.31–1.67) | 1.48 (1.33–1.64) | 0.93 |
| Model 2 c | 1.34 (1.18–1.52) | 1.39 (1.25–1.55) | 0.90 |
| Model 3 d | 1.30 (1.15–1.48) | 1.36 (1.22–1.51) | 0.94 |
| Stroke (n) | 92 | 111 | |
| Incidence rate/1000 person-years | 1.56 | 1.40 | |
| Model 1 | 1.66 (1.33–2.07) | 1.48 (1.20–1.83) | 0.45 |
| Model 2 | 1.53 (1.22–1.92) | 1.39 (1.12–1.73) | 0.49 |
| Model 3 | 1.47 (1.17–1.85) | 1.34 (1.08–1.67) | 0.45 |
| Heart disease (n) | 262 | 381 | |
| Incidence rate/1000 person-years | 4.43 | 4.80 | |
| Model 1 | 1.56 (1.37–1.77) | 1.49 (1.33–1.67) | 0.59 |
| Model 2 | 1.40 (1.22–1.60) | 1.40 (1.24–1.57) | 0.73 |
| Model 3 | 1.36 (1.19–1.56) | 1.36 (1.21–1.53) | 0.70 |
| Trauma reaction | |||
| Total CVD (n) | 523 | 662 | |
| Incidence rate/1000 person-years | 8.85 | 8.34 | |
| Model 1 | 1.54 (1.40–1.70) | 1.43 (1.30–1.57) | 0.37 |
| Model 2 | 1.42 (1.29–1.52) | 1.35 (1.23–1.49) | 0.41 |
| Model 3 | 1.37 (1.23–1.51) | 1.31 (1.19–1.44) | 0.37 |
| Stroke (n) | 174 | 170 | |
| Incidence rate/1000 person-years | 2.94 | 2.14 | |
| Model 1 | 1.86 (1.56–2.22) | 1.49 (1.24–1.79) | 0.09 |
| Model 2 | 1.78 (1.49–2.14) | 1.41 (1.17–1.70) | 0.08 |
| Model 3 | 1.68 (1.40–2.02) | 1.35 (1.12–1.64) | 0.07 |
| Heart disease (n) | 437 | 559 | |
| Incidence rate/1000 person-years | 7.40 | 7.04 | |
| Model 1 | 1.56 (1.40–1.73) | 1.44 (1.30–1.59) | 0.39 |
| Model 2 | 1.43 (1.28–1.59) | 1.35 (1.22–1.50) | 0.45 |
| Model 3 | 1.37 (1.23–1.53) | 1.31 (1.18–1.46) | 0.41 |
| Evacuation status | |||
| Total CVD (n) | 871 | 819 | |
| Incidence rate/1000 person-years | 14.74 | 10.32 | |
| Model 1 | 1.18 (1.09–1.29) | 1.07 (0.98–1.17) | 0.10 |
| Model 2 | 1.13 (1.02–1.24) | 1.03 (0.94–1.14) | 0.13 |
| Model 3 | 1.11 (1.01–1.22) | 1.03 (0.94–1.14) | 0.19 |
| Stroke (n) | 247 | 182 | |
| Incidence rate/1000 person-years | 4.18 | 2.29 | |
| Model 1 | 1.21 (1.03–1.42) | 0.93 (0.77–1.11) | 0.03 |
| Model 2 | 1.17 (0.98–1.40) | 0.90 (0.74–1.10) | 0.04 |
| Model 3 | 1.15 (0.97–1.38) | 0.90 (0.74–1.10) | 0.06 |
| Heart disease (n) | 719 | 698 | |
| Incidence rate/1000 person-years | 12.17 | 8.80 | |
| Model 1 | 1.17 (1.06–1.28) | 1.10 (1.00–1.21) | 0.29 |
| Model 2 | 1.11 (1.00–1.23) | 1.04 (0.93–1.16) | 0.35 |
| Model 3 | 1.09 (0.98–1.21) | 1.04 (0.93–1.16) | 0.43 |
| Neither | Only Psychological | Only Evacuation | Both | |
|---|---|---|---|---|
| Men | ||||
| Person-years | 31,101 | 6218 | 16,702 | 5067 |
| Psychological distress | ||||
| Total CVD (n) | 1162 | 156 | 726 | 145 |
| Model 1 a | 1.00 | 1.50 (1.27–1.77) | 1.17 (1.07–1.29) | 1.65 (1.39–1.96) |
| Model 2 b | 1.00 | 1.37 (1.15–1.62) | 1.13 (1.02–1.25) | 1.46 (1.22–1.76) |
| Model 3 c | 1.00 | 1.34 (1.13–1.59) | 1.12 (1.01–1.24) | 1.39 (1.16–1.67) |
| Stroke (n) | 328 | 47 | 202 | 45 |
| Model 1 | 1.00 | 1.65 (1.22–2.25) | 1.18 (0.99–1.41) | 1.89 (1.38–2.58) |
| Model 2 | 1.00 | 1.54 (1.13–2.10) | 1.17 (0.96–1.41) | 1.75 (1.26–2.44) |
| Model 3 | 1.00 | 1.50 (1.10–2.04) | 1.15 (0.95–1.39) | 1.64 (1.18–2.29) |
| Heart disease (n) | 960 | 138 | 595 | 124 |
| Model 1 | 1.00 | 1.60 (1.34–1.91) | 1.16 (1.05–1.28) | 1.70 (1.41–2.05) |
| Model 2 | 1.00 | 1.44 (1.21–1.73) | 1.11 (0.99–1.24) | 1.49 (1.22–1.82) |
| Model 3 | 1.00 | 1.42 (1.19–1.70) | 1.10 (0.98–1.23) | 1.42 (1.17–1.74) |
| Trauma reaction | ||||
| Total CVD (n) | 1057 | 261 | 609 | 262 |
| Model 1 | 1.00 | 1.48 (1.30–1.71) | 1.13 (1.02–1.25) | 1.75 (1.53–2.00) |
| Model 2 | 1.00 | 1.38 (1.21–1.59) | 1.09 (0.98–1.22) | 1.58 (1.37–1.84) |
| Model 3 | 1.00 | 1.34 (1.16–1.53) | 1.08 (0.97–1.21) | 1.50 (1.29–1.74) |
| Stroke (n) | 287 | 88 | 161 | 86 |
| Model 1 | 1.00 | 1.83 (1.44–2.32) | 1.14 (0.94–1.38) | 2.08 (1.64–2.65) |
| Model 2 | 1.00 | 1.76 (1.38–2.24) | 1.13 (0.92–1.39) | 2.01 (1.54–2.61) |
| Model 3 | 1.00 | 1.69 (1.32–2.15) | 1.12 (0.91–1.38) | 1.85 (1.42–2.40) |
| Heart disease (n) | 880 | 218 | 500 | 219 |
| Model 1 | 1.00 | 1.49 (1.28–1.73) | 1.11 (0.99–1.24) | 1.76 (1.52–2.04) |
| Model 2 | 1.00 | 1.38 (1.19–1.60) | 1.07 (0.95–1.20) | 1.57 (1.34–1.84) |
| Model 3 | 1.00 | 1.33 (1.14–1.55) | 1.06 (0.94–1.19) | 1.49 (1.27–1.75) |
| Women | ||||
| Person-years | 37,141 | 11,498 | 21,371 | 9339 |
| Psychological distress | ||||
| Total CVD (n) | 1002 | 257 | 627 | 192 |
| Model 1 | 1.00 | 1.53 (1.34–1.76) | 1.08 (0.98–1.19) | 1.50 (1.29–1.75) |
| Model 2 | 1.00 | 1.45 (1.26–1.66) | 1.05 (0.94–1.17) | 1.38 (1.18–1.63) |
| Model 3 | 1.00 | 1.41 (1.22–1.62) | 1.04 (0.94–1.16) | 1.35 (1.15–1.59) |
| Stroke (n) | 265 | 64 | 135 | 47 |
| Model 1 | 1.00 | 1.44 (1.09–1.89) | 0.89 (0.73–1.10) | 1.41 (1.03–1.92) |
| Model 2 | 1.00 | 1.34 (1.01–1.77) | 0.87 (0.70–1.09) | 1.29 (0.93–1.79) |
| Model 3 | 1.00 | 1.28 (0.97–1.69) | 0.87 (0.69–1.08) | 1.26 (0.91–1.75) |
| Heart disease (n) | 832 | 218 | 522 | 163 |
| Model 1 | 1.00 | 1.56 (1.35–1.82) | 1.11 (0.99–1.23) | 1.53 (1.29–1.81) |
| Model 2 | 1.00 | 1.47 (1.26–1.71) | 1.06 (0.94–1.19) | 1.38 (1.15–1.65) |
| Model 3 | 1.00 | 1.43 (1.22–1.66) | 1.06 (0.94–1.19) | 1.35 (1.13–1.61) |
| Trauma reaction | ||||
| Total CVD (n) | 880 | 379 | 536 | 283 |
| Model 1 | 1.00 | 1.55 (1.37–1.75) | 1.11 (1.00–1.24) | 1.41 (1.23–1.61) |
| Model 2 | 1.00 | 1.47 (1.30–1.66) | 1.08 (0.97–1.22) | 1.30 (1.13–1.50) |
| Model 3 | 1.00 | 1.42 (1.26–1.61) | 1.08 (0.97–1.22) | 1.27 (1.10–1.46) |
| Stroke (n) | 225 | 104 | 116 | 283 |
| Model 1 | 1.00 | 1.63 (1.30–2.06) | 0.97 (0.77–1.21) | 1.27 (0.97–1.67) |
| Model 2 | 1.00 | 1.55 (1.22–1.96) | 0.95 (0.75–1.20) | 1.17 (0.88–1.57) |
| Model 3 | 1.00 | 1.48 (1.16–1.87) | 0.95 (0.75–1.20) | 1.14 (0.85–1.52) |
| Heart disease (n) | 735 | 315 | 454 | 244 |
| Model 1 | 1.00 | 1.54 (1.35–1.76) | 1.13 (1.00–1.27) | 1.46 (1.26–1.69) |
| Model 2 | 1.00 | 1.45 (1.27–1.66) | 1.08 (0.95–1.23) | 1.32 (1.13–1.54) |
| Model 3 | 1.00 | 1.41 (1.23–1.61) | 1.08 (0.95–1.22) | 1.28 (1.09–1.50) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sanoh, T.; Eguchi, E.; Ohira, T.; Hayashi, F.; Maeda, M.; Yasumura, S.; Suzuki, Y.; Yabe, H.; Takahashi, A.; Takase, K.; et al. Association between Psychological Factors and Evacuation Status and the Incidence of Cardiovascular Diseases after the Great East Japan Earthquake: A Prospective Study of the Fukushima Health Management Survey. Int. J. Environ. Res. Public Health 2020, 17, 7832. https://doi.org/10.3390/ijerph17217832
Sanoh T, Eguchi E, Ohira T, Hayashi F, Maeda M, Yasumura S, Suzuki Y, Yabe H, Takahashi A, Takase K, et al. Association between Psychological Factors and Evacuation Status and the Incidence of Cardiovascular Diseases after the Great East Japan Earthquake: A Prospective Study of the Fukushima Health Management Survey. International Journal of Environmental Research and Public Health. 2020; 17(21):7832. https://doi.org/10.3390/ijerph17217832
Chicago/Turabian StyleSanoh, Toshiki, Eri Eguchi, Tetsuya Ohira, Fumikazu Hayashi, Masaharu Maeda, Seiji Yasumura, Yuriko Suzuki, Hirooki Yabe, Atsushi Takahashi, Kanae Takase, and et al. 2020. "Association between Psychological Factors and Evacuation Status and the Incidence of Cardiovascular Diseases after the Great East Japan Earthquake: A Prospective Study of the Fukushima Health Management Survey" International Journal of Environmental Research and Public Health 17, no. 21: 7832. https://doi.org/10.3390/ijerph17217832