Development and Psychometric Testing of the Self-Care in COVID-19 (SCOVID) Scale, an Instrument for Measuring Self-Care in the COVID-19 Pandemic

 , and
, and
Abstract
:1. Introduction
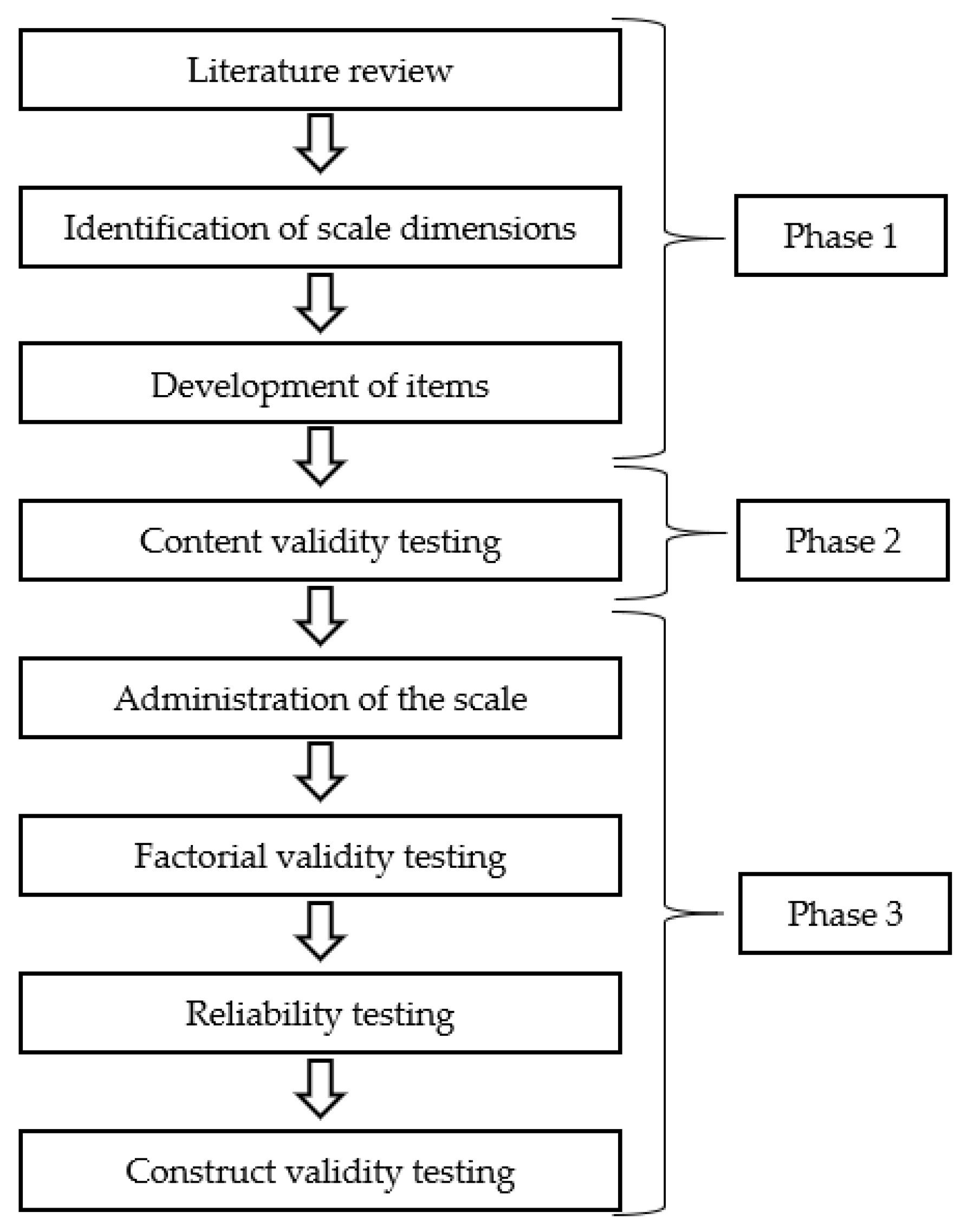
2. Materials and Methods
- (a)
- First Phase: Development of the SCOVID Scale Items:
- (b)
- Second Phase: Content Validity of the SCOVID Scale Items:
- (c)
- Third Phase: Testing of the SCOVID Scale:
2.1. Ethical Considerations
2.2. Data Analysis
3. Results
3.1. SCOVID Scale Content Validity
3.2. Sociodemographic Characteristics of Participants Who Completed the SCOVID Scale
3.3. Descriptive Analysis of the SCOVID Scale Items
3.4. Factorial Validity of the SCOVID Scale
3.5. Construct Validity of the SCOVID Scale
3.6. Reliability of the SCOVID Scale
3.7. Measurement Errors of the SCOVID Scale
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- WHO. COVID-19 Weekly Epidemiological Update 10. Available online: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20201020-weekly-epi-update-10.pdf (accessed on 22 October 2020).
- Zhai, P.; Ding, Y.; Wu, X.; Long, J.; Zhong, Y.; Li, Y. The Epidemiology, Diagnosis and Treatment of COVID-19. Int. J. Antimicrob. Agents 2020, 55, 105955. [Google Scholar] [CrossRef] [PubMed]
- Bai, Y.; Yao, L.; Wei, T.; Tian, F.; Jin, D.-Y.; Chen, L.; Wang, M. Presumed Asymptomatic Carrier Transmission of COVID-19. JAMA 2020, 323, 1406–1407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, X.; Yang, R. COVID-19 Transmission through Asymptomatic Carriers Is a Challenge to Containment. Influ. Other Respir. Viruses 2020, 14, 474–475. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Coronavirus Disease (COVID-19) Advice for the Public. Available online: https://www.who.int/emergencies/diseases/novel-Coronavirus-2019/Advice-for-Public (accessed on 10 July 2020).
- CDC. Coronavirus Disease 2019–How to Protect Yourself & Others. Available online: https://www.cdc.gov/coronavirus/2019-ncov/prevent-Getting-sick/prevention.Html (accessed on 10 July 2020).
- ECDC. Infographic: COVID-19. Available online: https://www.ecdc.europa.eu/en/publications-data/Infographic-Covid-19 (accessed on 10 July 2020).
- Riegel, B.; Jaarsma, T.; Strömberg, A. A Middle-Range Theory of Self-Care of Chronic Illness. Adv. Nurs. Sci. 2012, 35, 194–204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chu, D.K.; Akl, E.A.; Duda, S.; Solo, K.; Yaacoub, S.; Schünemann, H.J.; El-Harakeh, A.; Bognanni, A.; Lotfi, T.; Loeb, M.; et al. Physical Distancing, Face Masks, and Eye Protection to Prevent Person-to-Person Transmission of SARS-CoV-2 and COVID-19: A Systematic Review and Meta-Analysis. Lancet 2020, 395, 1973–1987. [Google Scholar] [CrossRef]
- Ruppar, T.M.; Cooper, P.S.; Mehr, D.R.; Delgado, J.M.; Dunbar-Jacob, J.M. Medication Adherence Interventions Improve Heart Failure Mortality and Readmission Rates: Systematic Review and Meta-Analysis of Controlled Trials. J. Am. Heart Assoc. 2016, 5, e002606. [Google Scholar] [CrossRef] [PubMed]
- Lenferink, A.; Brusse-Keizer, M.; Van Der Valk, P.D.; Frith, P.A.; Zwerink, M.; Monninkhof, E.M.; Van Der Palen, J.; Effing, T.W. Self-Management Interventions Including Action Plans for Exacerbations Versus Usual Care in Patients with Chronic Obstructive Pulmonary Disease. Cochrane Database Syst. Rev. 2017, 8, CD011682. [Google Scholar] [CrossRef]
- Ahmed, Z.; Ahmed, O.; Aibao, Z.; Hanbin, S.; Siyu, L.; Ahmad, A. Epidemic of COVID-19 in China and Associated Psychological Problems. Asian J. Psychiatry 2020, 51, 102092. [Google Scholar] [CrossRef]
- Esposito, S.; Principi, N.; Leung, C.C.; Migliori, G.B. Universal Use of Face Masks for Success against COVID-19: Evidence and Implications for Prevention Policies. Eur. Respir. J. 2020, 55, 2001260. [Google Scholar] [CrossRef]
- Terwee, C.B.; Prinsen, C.; Chiarotto, A.; De Vet, H.; Bouter, L.M.; Alonso, J.; Westerman, M.J.; Patrick, D.L.; Mokkink, L.B. COSMIN Methodology for Assessing the Content Validity of PROMs–user Manual. Available online: https://www.cosmin.nl/wp-content/uploads/COSMIN-methodology-for-content-validity-user-manual-v1.pdf (accessed on 15 July 2020).
- De Vet, H.C.W.; Terwee, C.B.; Mokkink, L.B.; Knol, D.L. Measurement in Medicine; Cambridge University Press (CUP): Cambridge, UK, 2011. [Google Scholar]
- Ramezani, T.; Sharifirad, G.; Rajati, F.; Rajati, M.; Mohebi, S. Effect of Educational Intervention on Promoting Self-Care in Hemodialysis Patients: Applying the Self-Efficacy Theory. J. Educ. Heal. Promot. 2019, 8, 65. [Google Scholar] [CrossRef]
- Kurtz, M.E.; Kurtz, J.C.; Given, C.W.; Given, B.A. Patient Optimism and Mastery—Do They Play a Role in Cancer Patients’ Management of Pain and Fatigue? J. Pain Symptom Manag. 2008, 36, 1–10. [Google Scholar] [CrossRef]
- Crowley, T.; Van Der Merwe, A.; Kidd, M.; Skinner, D. Adolescent Human Immunodeficiency Virus Self-Management: Associations with Treatment Adherence, Viral Suppression, Sexual Risk Behaviours and Health-Related Quality of Life. South. Afr. J. HIV Med. 2020, 21, 11. [Google Scholar] [CrossRef]
- Müller-Tasch, T.; Löwe, B.; Lossnitzer, N.; Frankenstein, L.; Täger, T.; Haass, M.; Katus, H.; Schultz, J.H.; Herzog, W. Anxiety and Self-Care Behaviour in Patients With Chronic Systolic Heart Failure: A Multivariate Model. Eur. J. Cardiovasc. Nurs. 2017, 17, 170–177. [Google Scholar] [CrossRef] [PubMed]
- Iovino, P.; De Maria, M.; Matarese, M.; Vellone, E.; Ausili, D.; Riegel, B. Depression and self-care in Older Adults with Multiple Chronic Conditions: A Multivariate Analysis. J. Adv. Nurs. 2020, 76, 1668–1678. [Google Scholar] [CrossRef]
- Chen, G.; Gully, S.M.; Eden, D. Validation of a New General Self-Efficacy Scale. Organ. Res. Methods 2001, 4, 62–83. [Google Scholar] [CrossRef] [Green Version]
- Caprara, G.V.; Alessandri, G.; Eisenberg, N.; Kupfer, A.; Steca, P.; Caprara, M.G.; Yamaguchi, S.; Fukuzawa, A.; Abela, J. The Positivity Scale. Psychol. Assess. 2012, 24, 701–712. [Google Scholar] [CrossRef] [PubMed]
- Jenkinson, C.; Coulter, A.; Wright, L. Short Form 36 (SF36) Health Survey Questionnaire: Normative Data for Adults of Working Age. BMJ 1993, 306, 1437–1440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.W.; Löwe, B. A Brief Measure for Assessing Generalized Anxiety Disorder. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [Green Version]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W. The PHQ-9. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Polit, D.F.; Beck, C.T.; Owen, S.V. Is the CVI an Acceptable Indicator of Content Validity? Appraisal and Recommendations. Res. Nurs. Heal. 2007, 30, 459–467. [Google Scholar] [CrossRef]
- Hu, L.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. A Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates, Inc.: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Muthén, L.K.; Muthen, B.O. Mplus User’s Guide: Statistical Analysis with Latent Variables, User’s Guide; Muthén & Muthén: Losa Angeles, CA, USA, 2017. [Google Scholar]
- Fornell, C.; Larcker, D.F. Evaluating structural equation models with unobservable variables and measurement error. J. Mark. Res. 1981, 18, 39–50. [Google Scholar] [CrossRef]
- Raykov, T. Scale Construction and Development Using Structural Equation Modeling. In Handbook of Structural Equation Modeling; Hoyle, R.H., Ed.; The Guilford Press: New York, NY, USA, 2012. [Google Scholar]
- Brown, J.D. Standard Error Vs. Standard Error of Measurement. Available online: http://hosted.jalt.org/test/PDF/Brown4.pdf (accessed on 15 July 2020).
- Beckerman, H.; Roebroeck, M.; Lankhorst, G.; Becher, J.; Bezemer, P.; Verbeek, A. Smallest Real Difference, a Link Between Reproducibility and Responsiveness. Qual. Life Res. 2001, 10, 571–578. [Google Scholar] [CrossRef]
- Fornell, C. Issues in the application of covariance structure analysis: A comment. J. Consum. Res. 1983, 9, 443–448. [Google Scholar] [CrossRef]
- Bagozzi, R.P. Issues in the Application of Covariance Structure Analysis: A Further Comment. J. Consum. Res. 1983, 9, 449–450. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | M (SD) |
|---|---|
| Age | 48.79 (15.81) |
| N (%) | |
| Gender | |
| Male | 220 (47.7) |
| emale | 241 (52.3) |
| Marital status | |
| Single | 115 (24.9) |
| Married/Partnered | 291 (63.1) |
| Divorced | 33 (7.2) |
| Widowed | 22 (4.8) |
| Level of education | |
| No title | 2 (0.4) |
| Elementary school | 24 (5.2) |
| Middle school | 63 (13.7) |
| High school | 222 (48.2) |
| University degree | 150 (31.5) |
| Region of residence | |
| Northern Italy | 45 (9.8) |
| Central Italy | 200 (43.4) |
| Southern Italy | 216 (46.9) |
| Nationality | |
| Italian | 456 (98.9) |
| Other | 5 (1.1) |
| Occupation | |
| Employee | 156 (33.8) |
| Freelance | 69 (15.0) |
| Worker | 27 (5.9) |
| Student | 31 (6.7) |
| Other | 76 (16.5) |
| Unemployed | 14 (3.0) |
| Retired | 88 (19.1) |
| Perceived income adequacy | |
| Less than needed | 15 (3.3) |
| Enough for living | 307 (66.6) |
| More than needed | 139 (30.2) |
| Item | M | SD | Skewness | Kurtosis |
|---|---|---|---|---|
| 1. Wash your hands with water and soap or disinfectant solution after carrying out activities at risk of contagion (e.g., using public transport, grocery shopping in supermarkets) | 4.74 | 0.59 | −2.95 | 10.95 |
| 2. Ensure home hygiene using chlorine- or alcohol-based products | 4.06 | 1.07 | −1.10 | 0.48 |
| 3. Avoid handshakes and/or hugs with people other than members of your household | 4.69 | 0.71 | −2.93 | 9.86 |
| 4. Do something to relieve stress (e.g., take medication, do yoga, listen to music) | 3.52 | 1.25 | −0.43 | −0.79 |
| 5. Don’t touch (your own) eyes, nose, or mouth with your hands when outside home, even when wearing gloves | 4.28 | 0.98 | −1.49 | 1.86 |
| 6. Avoid places where a distance of at least one meter between people is not respected | 4.43 | 0.82 | −1.57 | 2.65 |
| 7. Disinfect surfaces and objects shared with other people (e.g., handles, switches, desks, keyboards, remote controls, telephones) | 3.82 | 1.24 | −0.80 | −0.39 |
| 8. Maintain regular physical activity (e.g., walking, running, exercise bike, online guided exercises) | 3.42 | 1.30 | −0.35 | −0.95 |
| 9. Try to maintain your usual hobbies or cultivate new ones (e.g., reading, painting, gardening, cooking) | 3.78 | 1.09 | −0.72 | 0.00 |
| 10. Maintain a healthy and balanced diet appropriate to activities during the day | 3.78 | 1.03 | −0.71 | 0.18 |
| 11. Try to maintain a well-groomed appearance despite not being able to go to the hairdresser or beautician | 4.01 | 0.97 | −0.90 | 0.45 |
| 12. Maintain a distance of at least one meter from other people outside the home | 4.64 | 0.65 | −2.21 | 6.23 |
| 13. Wear disposable gloves in public places when there is a risk of contagion (e.g., on public transport, in the supermarket) | 4.35 | 1.10 | −1.79 | 2.34 |
| 14. Maintain a healthy lifestyle (e.g., avoiding or limiting smoking, not abusing alcohol or other drugs) | 4.26 | 1.05 | −1.47 | 1.42 |
| 15. Try to keep in touch with other people, other than members of your own household (e.g., friends, relatives, colleagues) by means of phone calls, video calls, e-mails, etc. | 4.38 | 0.80 | −1.36 | 2.07 |
| 16. Cover your nose and mouth (e.g., by using a face mask) when there is a risk of contagion | 4.77 | 0.61 | −3.33 | 12.93 |
| 17. Limit to leave home | 4.23 | 0.95 | −1.19 | 0.85 |
| 18. Maintain a regular sleep-wake rhythm (e.g., going to bed at the same time and waking up at the same time every day) | 3.61 | 1.20 | −0.51 | −0.68 |
| 19. Try to maintain a daily routine | 4.01 | 0.89 | −0.68 | 0.12 |
| 20. Ensure air changes in rooms shared with other people (e.g., workplace, home) | 4.57 | 0.66 | −1.40 | 1.24 |
| Total SCOVID scale score | 79.19 | 13.40 | −1.02 | 2.45 |
| Individual protective measures score | 87.21 | 13.73 | −2.09 | 6.82 |
| Environmental disinfection score | 78.74 | 21.05 | −1.01 | 0.31 |
| Social distancing score | 87.43 | 14.64 | −1.73 | 4.04 |
| Preventing COVID-19 score | 85.03 | 13.16 | −1.44 | 3.39 |
| Maintaining wellbeing score | 70.01 | 18.19 | −0.48 | 0.29 |
| SCOVID/Other Scales | General Self-Efficacy Scale | Positivity Scale | GAD-7 Scale | PHQ-9 Scale | SF-36 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| PF | PHL | EHL | E/F | EW | SF | P | GH | |||||
| Individual protective measures | 0.42 b | 0.39 b | −0.16 b | −0.28 b | 0.13 b | 0.23 b | 0.19 b | 0.20 b | 0.25 b | 0.24 b | 0.12 b | 0.20 b |
| Environmental disinfection | 0.32 b | 0.26 b | −0.03 | −0.14 b | 0.03 | 0.09 | 0.14 b | 0.12 b | 0.04 | 0.05 | −0.12 b | 0.12 a |
| Social distancing | 0.3 b | 0.26 b | −0.19 b | −0.23 b | −0.01 | 0.15 b | 0.16 b | 0.17 b | 0.14 b | 0.15 b | −0.02 | 0.06 |
| Preventing COVID-19 | 0.43 b | 0.38 b | −0.15 b | −0.26 b | 0.07 | 0.20 b | 0.20 b | 0.19 b | 0.18 b | 0.19 b | 0.00 | 0.16 b |
| Maintaining wellbeing | 0.48 b | 0.41 b | −0.26 b | −0.35 b | 0.16 b | 0.21 b | 0.22 b | 0.36 b | 0.25 b | 0.26 b | 0.04 | 0.24 b |
| SCOVID Total | 0.50 b | 0.44 b | −0.22 b | −0.33 b | 0.13 b | 0.22 b | 0.23 b | 0.30 b | 0.23 b | 0.24 b | 0.02 | 0.22 b |
| SCOVID Factors and Scale | Factor Score Determinacy | Composite Reliability | Global Reliability Index | Cronbach’s Alpha | ICC (95% CI) |
|---|---|---|---|---|---|
| Individual protective measures | 0.89 | 0.76 | |||
| Environmental disinfection | 0.89 | 0.71 | |||
| Social distancing | 0.89 | 0.73 | |||
| Preventing COVID-19 | 0.88 | ||||
| Maintaining wellbeing | 0.91 | 0.80 | |||
| SCOVID Total | 0.82 | 0.91 | 0.88 | 0.91 (0.88–0.93) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Maria, M.; Ferro, F.; Ausili, D.; Alvaro, R.; De Marinis, M.G.; Di Mauro, S.; Matarese, M.; Vellone, E. Development and Psychometric Testing of the Self-Care in COVID-19 (SCOVID) Scale, an Instrument for Measuring Self-Care in the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 7834. https://doi.org/10.3390/ijerph17217834
De Maria M, Ferro F, Ausili D, Alvaro R, De Marinis MG, Di Mauro S, Matarese M, Vellone E. Development and Psychometric Testing of the Self-Care in COVID-19 (SCOVID) Scale, an Instrument for Measuring Self-Care in the COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2020; 17(21):7834. https://doi.org/10.3390/ijerph17217834
Chicago/Turabian StyleDe Maria, Maddalena, Federico Ferro, Davide Ausili, Rosaria Alvaro, Maria Grazia De Marinis, Stefania Di Mauro, Maria Matarese, and Ercole Vellone. 2020. "Development and Psychometric Testing of the Self-Care in COVID-19 (SCOVID) Scale, an Instrument for Measuring Self-Care in the COVID-19 Pandemic" International Journal of Environmental Research and Public Health 17, no. 21: 7834. https://doi.org/10.3390/ijerph17217834