Targeting EphA2 in Bladder Cancer Using a Novel Antibody-Directed Nanotherapeutic

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Histology and EphA2 Immunohistochemistry
2.2. Nanotherapeutic (EphA2-ILs-DTXp) Generation
2.3. PDX Models BL-0382, BL-0293, and BL-0440
2.4. PDX Model BL417362
2.5. In Vivo Activity
2.6. Statistical Analysis
3. Results
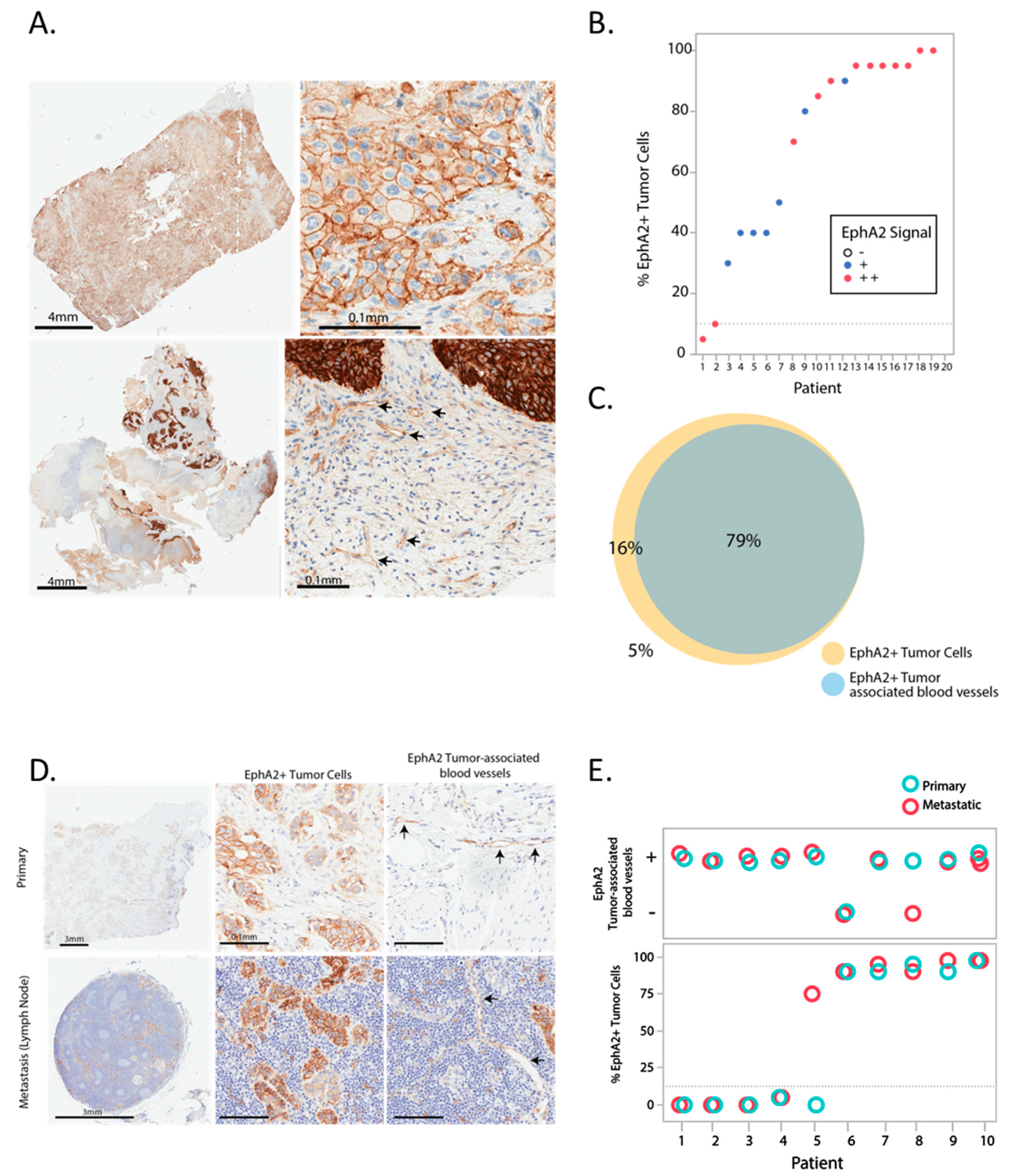
3.1. Expression Pattern of EphA2 in Bladder Cancer
3.2. Correlation of EphA2 Expression with Overall Survival in Bladder Cancer
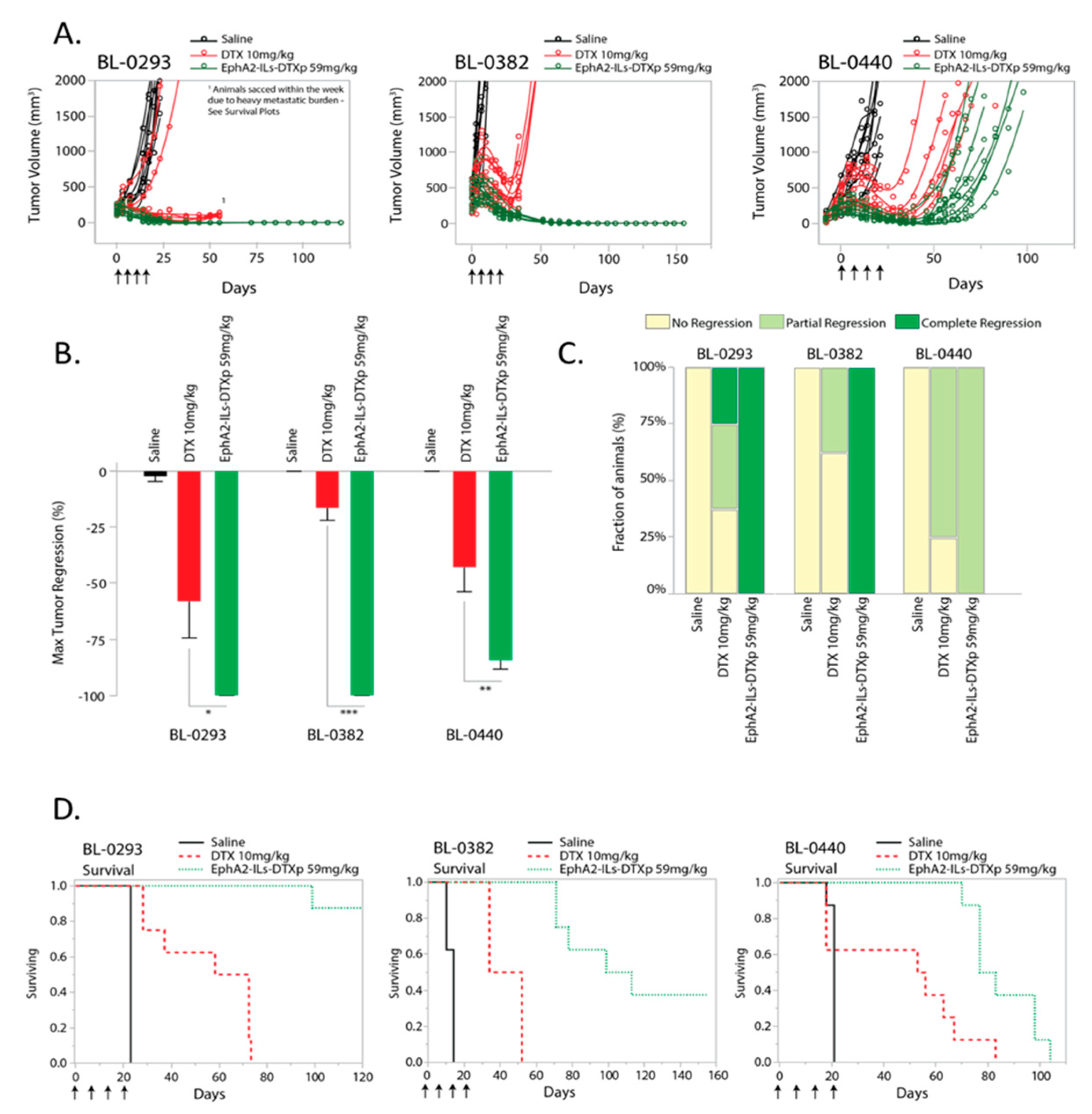
3.3. Efficacy of EphA2-Targeted Antibody-Directed Nanotherapeutic in Patient-Derived Models of Bladder Cancer
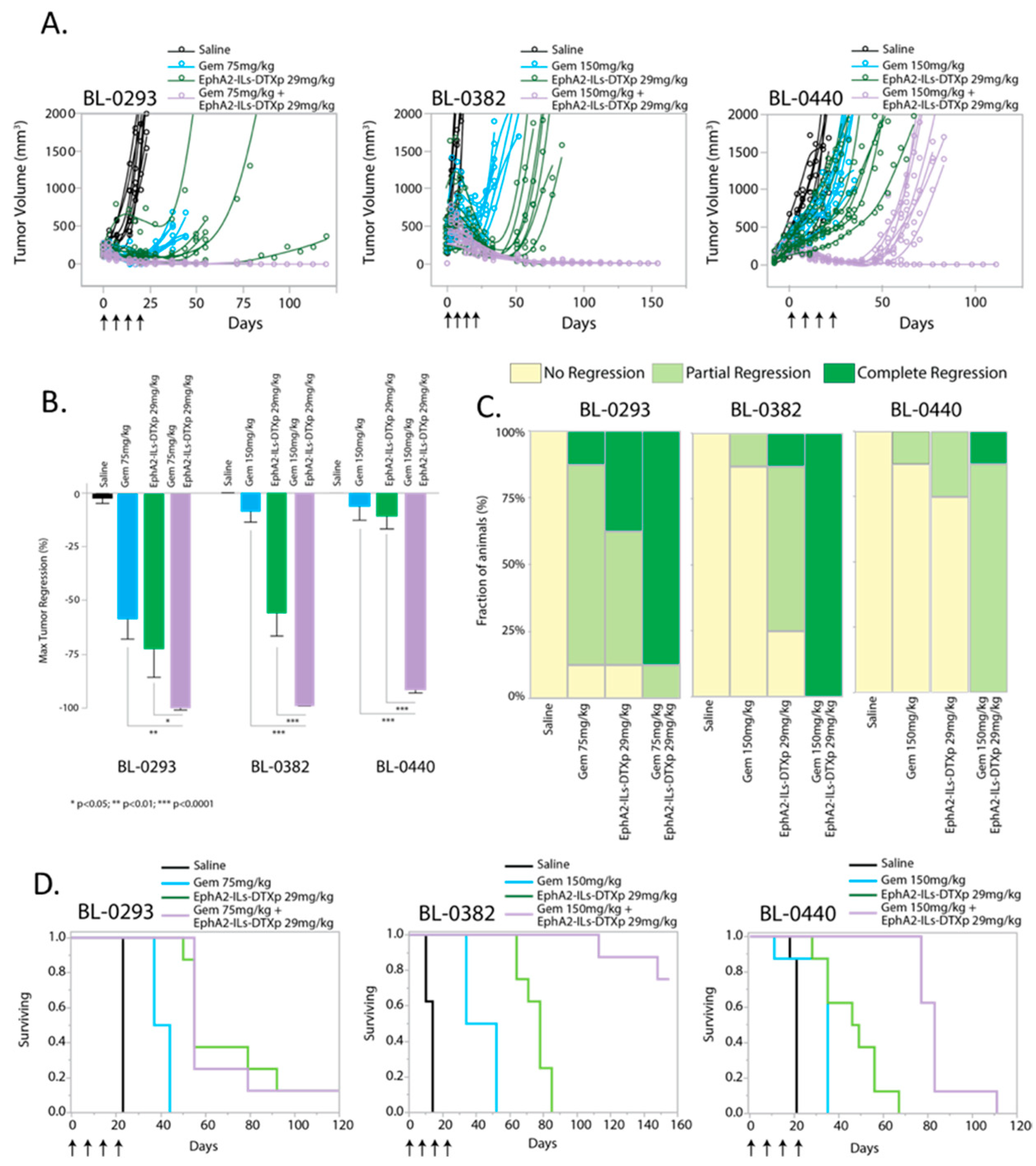
3.4. EphA2-ILs-DTXp Synergizes with Gemcitabine in PDX Models of Bladder Cancer
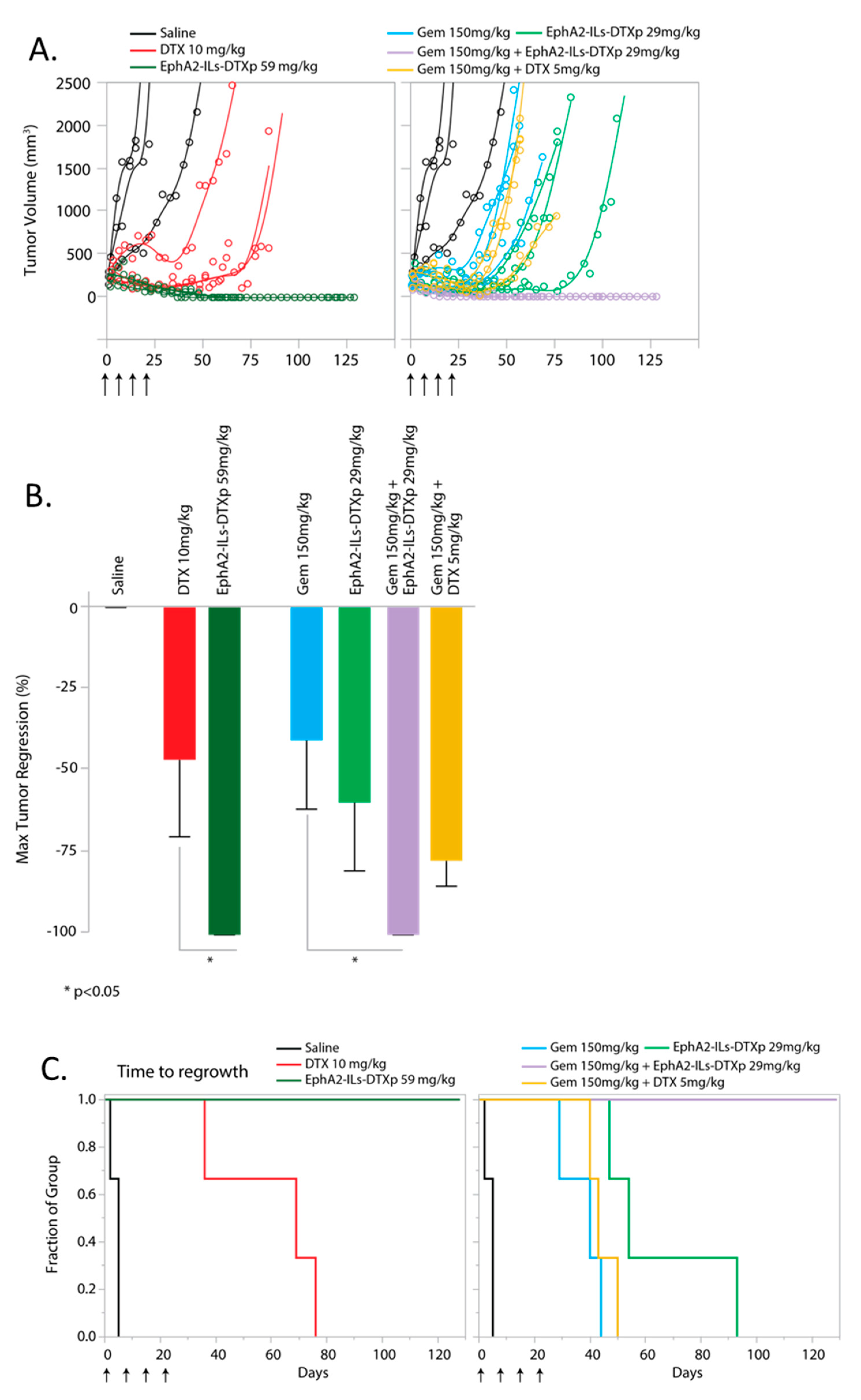
3.5. EphA2-ILs-DTXp in Combination with Gemcitabine is Superior to Free Docetaxel in Combination with Gemcitabine
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2018. CA Cancer J. Clin. 2018, 68, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Lei, A.Q.; Cheng, L.; Pan, C.X. Current treatment of metastatic bladder cancer and future directions. Expert Rev. Anticancer Ther. 2011, 11, 1851–1862. [Google Scholar] [CrossRef] [PubMed]
- Bellmunt, J.; Fougeray, R.; Rosenberg, J.E.; von der Maase, H.; Schutz, F.A.; Salhi, Y.; Culine, S.; Choueiri, T.K. Long-term survival results of a randomized phase III trial of vinflunine plus best supportive care versus best supportive care alone in advanced urothelial carcinoma patients after failure of platinum-based chemotherapy. Ann. Oncol. 2013, 24, 1466–1472. [Google Scholar] [CrossRef] [PubMed]
- Naiki, T.; Kawai, N.; Hashimoto, Y.; Okamura, T.; Ando, R.; Yasui, T.; Okada, A.; Etani, T.; Tozawa, K.; Kohri, K. Gemcitabine and docetaxel, an effective second-line chemotherapy for lung metastasis of urothelial carcinoma. Int. J. Clin. Oncol. 2014, 19, 516–522. [Google Scholar] [CrossRef] [PubMed]
- Yafi, F.A.; North, S.; Kassouf, W. First- and second-line therapy for metastatic urothelial carcinoma of the bladder. Curr. Oncol. 2011, 18, e25–e34. [Google Scholar] [CrossRef] [Green Version]
- Inoue, T.; Obara, T.; Saito, M.; Kumazawa, T.; Narita, S.; Horikawa, Y.; Yuasa, T.; Tsuchiya, N.; Satoh, S.; Habuchi, T. Combination therapy consisting of gemcitabine, docetaxel and carboplatin as a second-line chemotherapy for patients with MVAC-treated metastatic urothelial carcinoma. Hinyokika Kiyo. 2008, 54, 581–585. [Google Scholar]
- Bellmunt, J.; de Wit, R.; Vaughn, D.J.; Fradet, Y.; Lee, J.L.; Fong, L.; Vogelzang, N.J.; Climent, M.A.; Petrylak, D.P.; Choueiri, T.K.; et al. Pembrolizumab as Second-Line Therapy for Advanced Urothelial Carcinoma. N. Engl. J. Med. 2017, 376, 1015–1026. [Google Scholar] [CrossRef] [Green Version]
- Vlachostergios, P.J.; Jakubowski, C.D.; Niaz, M.J.; Lee, A.; Thomas, C.; Hackett, A.L.; Patel, P.; Rashid, N.; Tagawa, S.T. Antibody-Drug Conjugates in Bladder Cancer. Bladder Cancer 2018, 4, 247–259. [Google Scholar] [CrossRef] [Green Version]
- Balar, A.V.; Castellano, D.; O’Donnell, P.H.; Grivas, P.; Vuky, J.; Powles, T.; Plimack, E.R.; Hahn, N.M.; de Wit, R.; Pang, L.; et al. First-line pembrolizumab in cisplatin-ineligible patients with locally advanced and unresectable or metastatic urothelial cancer (KEYNOTE-052): A multicentre, single-arm, phase 2 study. Lancet Oncol. 2017, 18, 1483–1492. [Google Scholar] [CrossRef]
- Balar, A.V.; Galsky, M.D.; Rosenberg, J.E.; Powles, T.; Petrylak, D.P.; Bellmunt, J.; Loriot, Y.; Necchi, A.; Hoffman-Censits, J.; Perez-Gracia, J.L.; et al. Atezolizumab as first-line treatment in cisplatin-ineligible patients with locally advanced and metastatic urothelial carcinoma: A single-arm, multicentre, phase 2 trial. Lancet 2017, 389, 67–76. [Google Scholar] [CrossRef] [Green Version]
- Powles, T.; Durán, I.; van der Heijden, M.S.; Loriot, Y.; Vogelzang, N.J.; De Giorgi, U.; Oudard, S.; Retz, M.M.; Castellano, D.; Bamias, A.; et al. Atezolizumab versus chemotherapy in patients with platinum-treated locally advanced or metastatic urothelial carcinoma (IMvigor211): A multicentre, open-label, phase 3 randomised controlled trial. Lancet 2018, 391, 748–757. [Google Scholar] [CrossRef]
- Dietrich, B.; Srinivas, S. Urothelial carcinoma: The evolving landscape of immunotherapy for patients with advanced disease. Res. Rep. Urol. 2018, 10, 7–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pasquale, E.B. Eph receptors and ephrins in cancer: Bidirectional signalling and beyond. Nat. Rev. Cancer 2010, 10, 165–180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abraham, S.; Knapp, D.W.; Cheng, L.; Snyder, P.W.; Mittal, S.K.; Bangari, D.S.; Kinch, M.; Wu, L.; Dhariwal, J.; Mohammed, S.I. Expression of EphA2 and Ephrin A-1 in carcinoma of the urinary bladder. Clin. Cancer Res. 2006, 12, 353–360. [Google Scholar] [CrossRef] [Green Version]
- Brannan, J.M.; Dong, W.; Prudkin, L.; Behrens, C.; Lotan, R.; Bekele, B.N.; Wistuba, I.; Johnson, F.M. Expression of the receptor tyrosine kinase EphA2 is increased in smokers and predicts poor survival in non-small cell lung cancer. Clin. Cancer Res. 2009, 15, 4423–4430. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brantley-Sieders, D.M.; Zhuang, G.; Hicks, D.; Fang, W.B.; Hwang, Y.; Cates, J.M.; Coffman, K.; Jackson, D.; Bruckheimer, E.; Muraoka-Cook, R.S.; et al. The receptor tyrosine kinase EphA2 promotes mammary adenocarcinoma tumorigenesis and metastatic progression in mice by amplifying ErbB2 signaling. J. Clin. Investig. 2008, 118, 64–78. [Google Scholar] [CrossRef]
- Gokmen-Polar, Y.; Toroni, R.A.; Hocevar, B.A.; Badve, S.; Zhao, Q.; Shen, C.; Bruckheimer, E.; Kinch, M.S.; Miller, K.D. Dual targeting of EphA2 and ER restores tamoxifen sensitivity in ER/EphA2-positive breast cancer. Breast Cancer Res. Treat. 2011, 127, 375–384. [Google Scholar] [CrossRef]
- Yuan, W.J.; Ge, J.; Chen, Z.K.; Wu, S.B.; Shen, H.; Yang, P.; Hu, B.; Zhang, G.W.; Chen, Z.H. Over-expression of EphA2 and EphrinA-1 in human gastric adenocarcinoma and its prognostic value for postoperative patients. Dig. Dis. Sci. 2009, 54, 2410–2417. [Google Scholar] [CrossRef]
- Miyazaki, T.; Kato, H.; Fukuchi, M.; Nakajima, M.; Kuwano, H. EphA2 overexpression correlates with poor prognosis in esophageal squamous cell carcinoma. Int. J. Cancer 2003, 103, 657–663. [Google Scholar] [CrossRef]
- Mudali, S.V.; Fu, B.; Lakkur, S.S.; Luo, M.; Embuscado, E.E.; Iacobuzio-Donahue, C.A. Patterns of EphA2 protein expression in primary and metastatic pancreatic carcinoma and correlation with genetic status. Clin. Exp. Metastasis 2006, 23, 357–365. [Google Scholar] [CrossRef] [Green Version]
- Dunne, P.D.; Dasgupta, S.; Blayney, J.K.; McArt, D.G.; Redmond, K.L.; Weir, J.A.; Bradley, C.A.; Sasazuki, T.; Shirasawa, S.; Wang, T.; et al. EphA2 expression is a key driver of migration and invasion and a poor prognostic marker in colorectal cancer. Clin. Cancer Res. 2016, 22, 230–242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zeng, G.; Hu, Z.; Kinch, M.S.; Pan, C.X.; Flockhart, D.A.; Kao, C.; Gardner, T.A.; Zhang, S.; Li, L.; Baldridge, L.A.; et al. High-level expression of EphA2 receptor tyrosine kinase in prostatic intraepithelial neoplasia. Am. J. Pathol. 2003, 163, 2271–2276. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.; Zhang, X.; Qiu, Y.; Huang, D.; Zhang, S.; Xie, L.; Qi, L.; Yu, C.; Zhou, X.; Hu, G.; et al. Clinical significance of EphA2 expression in squamous-cell carcinoma of the head and neck. J. Cancer Res. Clin. Oncol. 2011, 137, 761–769. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.F.; Fokas, E.; Bieker, M.; Rose, F.; Rexin, P.; Zhu, Y.; Pagenstecher, A.; Engenhart-Cabillic, R.; An, H.X. Increased expression of EphA2 correlates with adverse outcome in primary and recurrent glioblastoma multiforme patients. Oncol. Rep. 2008, 19, 151–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thaker, P.H.; Deavers, M.; Celestino, J.; Thornton, A.; Fletcher, M.S.; Landen, C.N.; Kinch, M.S.; Kiener, P.A.; Sood, A.K. EphA2 expression is associated with aggressive features in ovarian carcinoma. Clin. Cancer Res. 2004, 10, 5145–5150. [Google Scholar] [CrossRef] [Green Version]
- Yang, N.Y.; Fernandez, C.; Richter, M.; Xiao, Z.; Valencia, F.; Tice, D.A.; Pasquale, E.B. Crosstalk of the EphA2 receptor with a serine/threonine phosphatase suppresses the Akt-mTORC1 pathway in cancer cells. Cell. Signal. 2011, 23, 201–212. [Google Scholar] [CrossRef] [Green Version]
- Annunziata, C.M.; Kohn, E.C.; LoRusso, P.; Houston, N.D.; Coleman, R.L.; Buzoianu, M.; Robbie, G.; Lechleider, R. Phase 1, open-label study of MEDI-547 in patients with relapsed or refractory solid tumors. Invest. New Drugs 2013, 31, 77–84. [Google Scholar] [CrossRef] [Green Version]
- Wu, B.; Wang, S.; De, S.K.; Barile, E.; Quinn, B.A.; Zharkikh, I.; Purves, A.; Stebbins, J.L.; Oshima, R.G.; Fisher, P.B.; et al. Design and characterization of novel EphA2 agonists for targeted delivery of chemotherapy to cancer cells. Chem. Biol. 2015, 22, 876–887. [Google Scholar] [CrossRef] [Green Version]
- Wykosky, J.; Gibo, D.M.; Debinski, W. A novel, potent, and specific ephrinA1-based cytotoxin against EphA2 receptor expressing tumor cells. Mol. Cancer Ther. 2007, 6, 3208–3218. [Google Scholar] [CrossRef] [Green Version]
- Kamoun, W.S.; Kirpotin, D.B.; Huang, Z.R.; Tipparaju, S.K.; Noble, C.O.; Hayes, M.E.; Luus, L.; Koshkaryev, A.; Kim, J.; Olivier, K.; et al. Antitumour activity and tolerability of an EphA2-targeted nanotherapeutic in multiple mouse models. Nat. Biomed. Eng. 2019, 3, 264–280. [Google Scholar] [CrossRef]
- Uruga, H.; Bozkurtlar, E.; Huynh, T.G.; Muzikansky, A.; Goto, Y.; Gomez-Caraballo, M.; Hata, A.N.; Gainor, J.F.; Mark, E.J.; Engelman, J.A.; et al. Programmed cell death ligand (PD-L1) expression in stage II and III lung adenocarcinomas and nodal metastases. J. Thorac. Oncol. 2017, 12, 458–466. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geddie, M.L.; Kohli, N.; Kirpotin, D.B.; Razlog, M.; Jiao, Y.; Kornaga, T.; Rennard, R.; Xu, L.; Schoerberl, B.; Marks, J.D.; et al. Improving the developability of an anti-EphA2 single-chain variable fragment for nanoparticle targeting. MAbs 2017, 9, 58–67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flaig, T.W.; Spiess, P.E.; Agarwal, N.; Bangs, R.; Boorjian, S.A.; Buyyounouski, M.K.; Chang, S.; Downs, T.M.; Efstathiou, J.A.; Friedlander, T.; et al. Bladder cancer, version 3.2020, NCCN clinical practice guidelines in oncology. J. Natl. Compr. Canc. Netw. 2020, 18, 329–354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Witjes, J.A.; Bruins, H.M.; Cathomas, R.; Compérat, E.M.; Cowan, N.C.; Gakis, G.; Hernández, V.; Linares Espinós, E.; Lorch, A.; Neuzillet, Y.; et al. European association of urology guidelines on muscle-invasive and metastatic bladder cancer: Summary of the 2020 guidelines. Eur. Urol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Pan, C.X.; Zhang, H.; Tepper, C.G.; Lin, T.Y.; Davis, R.R.; Keck, J.; Ghosh, P.M.; Gill, P.; Airhart, S.; Bult, C.; et al. Development and characterization of bladder cancer patient-derived xenografts for molecularly guided targeted therapy. PLoS ONE 2015, 10, e0134346. [Google Scholar] [CrossRef]
- Sanofi-Aventis. TAXOTERE (docetaxel) Injection Concentrate, Intravenous Infusion (IV), Package Insert; Sanofi-Aventis: Bridgewater, NJ, USA, 2010. [Google Scholar]
- Dumont, N.; Merrigan, S.; Turpin, J.; Lavoie, C.; Papavasiliou, V.; Geretti, E.; Espelin, C.W.; Luus, L.; Kamoun, W.S.; Ghasemi, O.; et al. Nanoliposome targeting in breast cancer is influenced by the tumor microenvironment. Nanomedicine 2019, 17, 71–81. [Google Scholar] [CrossRef]
- Cui, X.D.; Lee, M.J.; Yu, G.R.; Kim, I.H.; Yu, H.C.; Song, E.Y.; Kim, D.G. EFNA1 ligand and its receptor EphA2: Potential biomarkers for hepatocellular carcinoma. Int. J. Cancer 2010, 126, 940–949. [Google Scholar] [CrossRef]
- Ishikawa, M.; Miyahara, R.; Sonobe, M.; Horiuchi, M.; Mennju, T.; Nakayama, E.; Kobayashi, M.; Kikuchi, R.; Kitamura, J.; Imamura, N.; et al. Higher expression of EphA2 and ephrin-A1 is related to favorable clinicopathological features in pathological stage I non-small cell lung carcinoma. Lung Cancer 2012, 76, 431–438. [Google Scholar] [CrossRef] [Green Version]
- De Santis, M.; Bellmunt, J.; Mead, G.; Kerst, J.M.; Leahy, M.; Maroto, P.; Gil, T.; Marreaud, S.; Daugaard, G.; Skoneczna, I.; et al. Randomized phase II/III trial assessing gemcitabine/carboplatin and methotrexate/carboplatin/vinblastine in patients with advanced urothelial cancer who are unfit for cisplatin-based chemotherapy: EORTC study 30986. J. Clin. Oncol. 2012, 30, 191–199. [Google Scholar] [CrossRef]
- von der Maase, H.; Sengelov, L.; Roberts, J.T.; Ricci, S.; Dogliotti, L.; Oliver, T.; Moore, M.J.; Zimmermann, A.; Arning, M. Long-term survival results of a randomized trial comparing gemcitabine plus cisplatin, with methotrexate, vinblastine, doxorubicin, plus cisplatin in patients with bladder cancer. J. Clin. Oncol. 2005, 23, 4602–4608. [Google Scholar] [CrossRef]
- Research, C.G.A. Comprehensive molecular characterization of urothelial bladder carcinoma. Nature 2014, 507, 315–322. [Google Scholar] [CrossRef] [Green Version]
- Rizvi, N.A.; Hellmann, M.D.; Snyder, A.; Kvistborg, P.; Makarov, V.; Havel, J.J.; Lee, W.; Yuan, J.; Wong, P.; Ho, T.S.; et al. Cancer immunology. Mutational landscape determines sensitivity to PD-1 blockade in non-small cell lung cancer. Science 2015, 348, 124–128. [Google Scholar] [CrossRef] [Green Version]
- Yarchoan, M.; Hopkins, A.; Jaffee, E.M. Tumor mutational burden and response rate to PD-1 inhibition. N. Engl. J. Med. 2017, 377, 2500–2501. [Google Scholar] [CrossRef] [PubMed]
- Kamoun, W.S.; Dugast, A.S.; Suchy, J.J.; Grabow, S.; Fulton, R.B.; Sampson, J.F.; Luus, L.; Santiago, M.; Koshkaryev, A.; Sun, G.; et al. Synergy between EphA2-ILs-DTXp, a novel EphA2-Targeted nanoliposomal taxane, and PD-1 inhibitors in preclinical tumor models. Mol. Cancer Ther. 2020, 19, 270–281. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient ID | Resection Site | % EphA2+ Tumor Cells | EphA2 TAV |
|---|---|---|---|
| 110056928 | Bladder | 0 | + |
| Lymph Node | 0 | + | |
| 110060015 | Bladder | 90 | + |
| Cervix | 97.5 1 | + | |
| 110066840 | Bladder | 90 | + |
| Lymph Node | 95 | + | |
| 110067477 | Bladder | 0 | + |
| Lymph Node | 75 | + | |
| 110068115 | Bone | 75 | + |
| 110068802 | Bladder | 0 | + |
| Soft Tissue | 0 | + | |
| 110069061 | Bladder | 5 | + |
| Lymph Node | 5 | + | |
| 110071199 | Bladder | 0 | + |
| Lymph Node | 0 | + | |
| 110071455 | Bladder | 97.5 1 | + |
| Lymph Node | 97.5 1 | + | |
| Uterus | 97.5 1 | + | |
| 110076214 | Bladder | 95 | + |
| Seminal Vesicle | 90 | - |
| Monotherapy | |||||||
| PDX Model | Treatment Group- | n | Max Regression | Survival | |||
| mean | std | p | median | p | |||
| BL-0293 | DTX 10 mg/kg | 8 | −58 | 46 | p < 0.05 | 65 | p < 0.0001 |
| EPhA2-ILs-DTXp 59 mg/kg | 8 | −100 | 0 | Not reached | |||
| BL-0382 | DTX 10 mg/kg | 8 | −16 | 16 | p < 0.001 | 43 | p < 0.0001 |
| EPhA2-ILs-DTXp 59 mg/kg | 8 | −100 | 0 | 106 | |||
| BL-0440 | DTX 10 mg/kg | 8 | −43 | 31 | p < 0.01 | 54.5 | p < 0.01 |
| EPhA2-ILs-DTXp 59 mg/kg | 8 | −84 | 12 | 80 | |||
| BL417362 | DTX 10 mg/kg | 3 | −47 | 41 | p < 0.05 | 83 | p < 0.05 |
| EPhA2-ILs-DTXp 59 mg/kg | 3 | −100 | 0 | Not reached | |||
| Gemcitabine Combination | |||||||
| PDX Model | Treatment Group | n | Max Regression | Survival | |||
| mean | std | p1 | median | p1 | |||
| BL-0293 | Gem 75 mg/kg | 8 | −58 | 26 | p < 0.01 | 41 | n.s. |
| EPhA2-ILs-DTXp 29 mg/kg | 8 | −72 | 37 | p < 0.05 | 55 | n.s. | |
| EPhA2-ILs-DTXp + Gem | 8 | −99 | 2 | 55 | |||
| BL-0382 | Gem 150 mg/kg | 8 | −9 | 14 | p < 0.0001 | 43 | p < 0.0001 |
| EPhA2-ILs-DTXp 29 mg/kg | 8 | −57 | 30 | p < 0.0001 | 78 | p < 0.0001 | |
| EPhA2-ILs-DTXp + Gem | 8 | −100 | 0 | Not reached | |||
| BL-0440 | Gem 150 mg/kg | 8 | −6 | 18 | p < 0.0001 | 35 | p < 0.0001 |
| EPhA2-ILs-DTXp 29 mg/kg | 8 | −11 | 16 | p < 0.0001 | 48 | p < 0.0001 | |
| EPhA2-ILs-DTXp + Gem | 8 | −93 | 4 | 83 | |||
| BL417362 | Gem 150 mg/kg | 3 | −41 | 36 | p < 0.05 | 59 | p < 0.05 |
| EPhA2-ILs-DTXp 29 mg/kg | 3 | −60 | 36 | n.s. | 83 | p < 0.05 | |
| DTX + Gem | 3 | −77 | 13 | n.s. | 59 | p < 0.05 | |
| EPhA2-ILs-DTXp + Gem | 3 | −100 | 0 | Not reached | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kamoun, W.; Swindell, E.; Pien, C.; Luus, L.; Cain, J.; Pham, M.; Kandela, I.; Huang, Z.R.; Tipparaju, S.K.; Koshkaryev, A.; et al. Targeting EphA2 in Bladder Cancer Using a Novel Antibody-Directed Nanotherapeutic. Pharmaceutics 2020, 12, 996. https://doi.org/10.3390/pharmaceutics12100996
Kamoun W, Swindell E, Pien C, Luus L, Cain J, Pham M, Kandela I, Huang ZR, Tipparaju SK, Koshkaryev A, et al. Targeting EphA2 in Bladder Cancer Using a Novel Antibody-Directed Nanotherapeutic. Pharmaceutics. 2020; 12(10):996. https://doi.org/10.3390/pharmaceutics12100996
Chicago/Turabian StyleKamoun, Walid, Elden Swindell, Christine Pien, Lia Luus, Jason Cain, Minh Pham, Irawati Kandela, Zhaohua Richard Huang, Suresh K. Tipparaju, Alexander Koshkaryev, and et al. 2020. "Targeting EphA2 in Bladder Cancer Using a Novel Antibody-Directed Nanotherapeutic" Pharmaceutics 12, no. 10: 996. https://doi.org/10.3390/pharmaceutics12100996