Altered Gut Microbiome and Environmental Factors Associated with Development of Eczema in Hong Kong Infants: A 4-Month Pilot Study

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
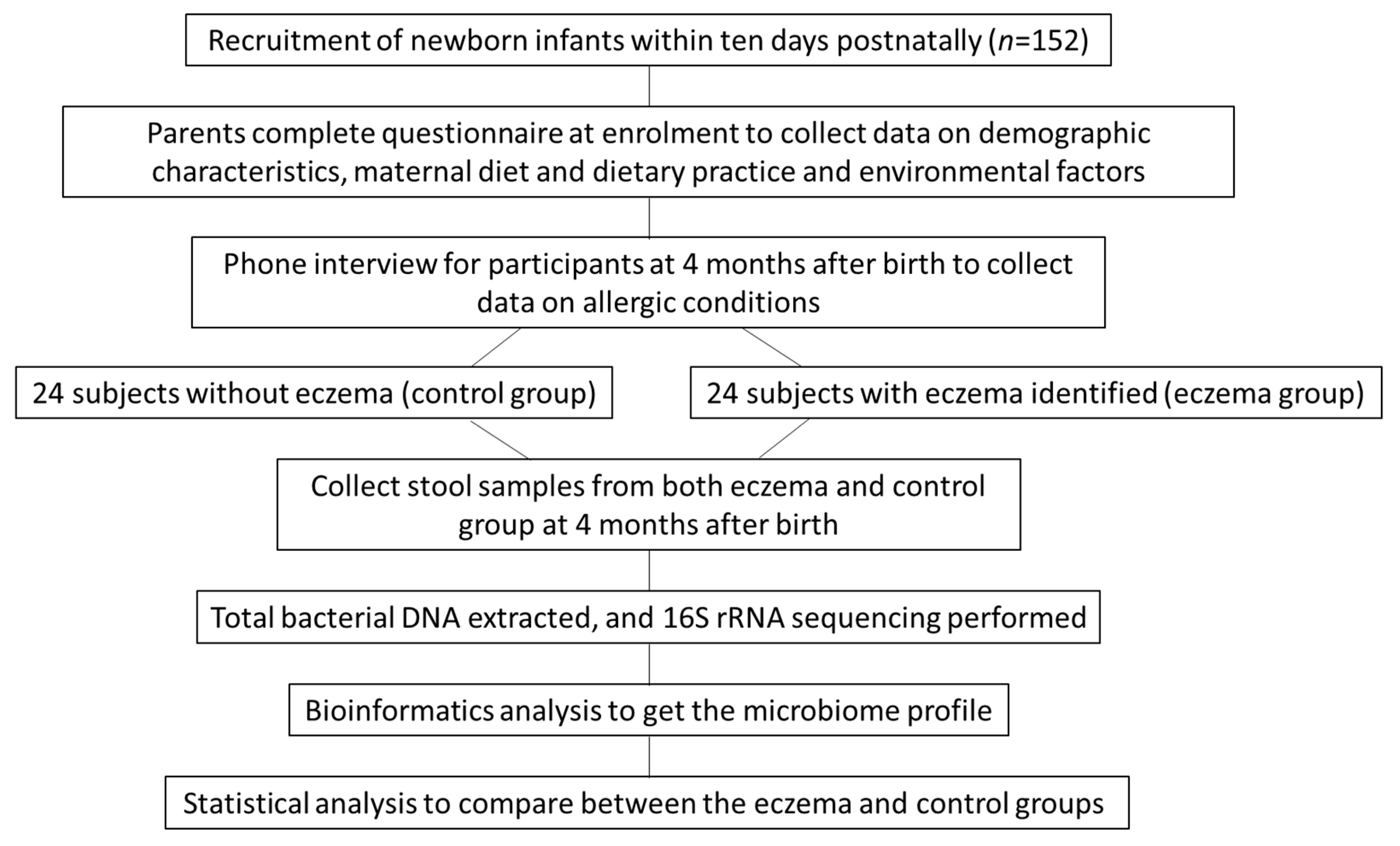
2.1. Subjects
2.2. Study Design
2.3. Questionnaire Data
2.3.1. Demographic Data
2.3.2. Maternal Diet
2.3.3. Environmental Factors and Allergy Data
2.3.4. Gut Microbiome Analysis
2.4. Statistical Analysis
3. Results
3.1. General Characteristics and Occurrence of Eczema
3.2. Association of Gut Microbiome and Eczema
3.3. Association of Maternal Diets, Use of Supplements, Environmental Factors and Eczema
3.4. Association of Environmental Factors and Eczema
3.5. Multivariate Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Thomsen, S.F. Atopic dermatitis: Natural history, diagnosis, and treatment. ISRN Allergy 2014, 2014, 354250. [Google Scholar] [CrossRef] [Green Version]
- Plötz, S.G.; Wiesender, M.; Todorova, A.; Ring, J. What is new in atopic dermatitis/eczema? Expert Opin. Emerg. Drugs 2014, 19, 441–458. [Google Scholar] [CrossRef] [PubMed]
- Williams, H.C. Clinical practice. Atopic dermatitis. N. Engl. J. Med. 2005, 352, 2314–2324. [Google Scholar] [CrossRef] [PubMed]
- Chan, Y.T.; Ho, H.K.; Lai, C.K.; Lau, C.S.; Lau, Y.L.; Lee, T.H.; Leung, T.F.; Wong, G.W.; Wu, Y.Y. Hong Kong Allergy Alliance. Allergy in Hong Kong: An unmet need in service provision and training. Hong Kong Med. J. 2015, 21, 52–60. [Google Scholar]
- Hooper, L.V.; Littman, D.R.; Macpherson, A.J. Interactions between the microbiota and the immune system. Science 2012, 336, 1268–1273. [Google Scholar] [CrossRef] [Green Version]
- Marlow, G.; Han, D.Y.; Wickens, K.; Stanley, T.; Crane, J.; Mitchell, E.A.; Dekker, J.; Barthow, C.; Fitzharris, P.; Ferguson, L.R.; et al. Differential effects of two probiotics on the risks of eczema and atopy associated with single nucleotide polymorphisms to Toll-like receptors. Pediatric Allergy Immunol. 2015, 26, 262–271. [Google Scholar] [CrossRef]
- Chan, C.W.; Wong, R.S.; Law, P.T.; Wong, C.L.; Tsui, S.K.; Tang, W.P.; Sit, J.W. Environmental factors associated with altered gut microbiota in children with eczema: A systematic review. Int. J. Mol. Sci. 2016, 17, 1147. [Google Scholar] [CrossRef] [Green Version]
- Shi, B.; Bangayan, N.J.; Curd, E.; Taylor, P.A.; Gallo, R.L.; Leung, D.Y.M.; Li, H. The skin microbiome is different in pediatric versus adult atopic dermatitis. J. Allergy Clin. Immunol. 2016, 138, 1233–1236. [Google Scholar] [CrossRef] [Green Version]
- Flohr, C.; Mann, J. New insights into the epidemiology of childhood atopic dermatitis. Allergy 2014, 69, 3–16. [Google Scholar] [CrossRef]
- Storrø, O.; Øien, T.; Langsrud, Ø.; Rudi, K.; Dotterud, C.; Johnsen, R. Temporal variations in early gut microbial colonization are associated with allergen-specific immunoglobulin E but not atopic eczema at 2 years of age. Clin. Exp. Allergy 2011, 41, 1545–1554. [Google Scholar] [CrossRef]
- Chan, C.W.; Law, B.M.; Liu, Y.H.; Ambrocio, A.R.; Au, N.; Jiang, M.; Chow, K.M. The association between maternal stress and childhood eczema: A systematic review. Int. J. Environ. Res. Public Health 2018, 15, 395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taylor-Robinson, D.C.; Williams, H.; Pearce, A.; Law, C.; Hope, S. Do early-life exposures explain why more advantaged children get eczema? Findings from the U.K. Millennium Cohort Study. Br. J. Dermatol. 2016, 174, 569–578. [Google Scholar] [CrossRef] [PubMed]
- Minasyan, A.; Babajanyan, A.; Campbell, D.E.; Nanan, R. Validation of a Comprehensive Early Childhood Allergy Questionnaire. Pediatric Allergy Immunol. 2015, 26, 522–529. [Google Scholar] [CrossRef]
- Hanifin, J.M.; Rajka, G. Diagnostic features of atopic dermatitis. Acta Derm. Venereol. Suppl. 1980, 92, 44–47. [Google Scholar]
- Stalder, J.F.; Atherton, D.J.; Bieber, T. Consensus Report of the European Task Force on Atopic Dermatitis Severity scoring of atopic dermatitis: The SCORAD index. Consensus Report of the European Task Force on Atopic Dermatitis. Dermatology 1993, 186, 23–31. [Google Scholar]
- Dharmage, S.C.; Lowe, A.J.; Matheson, M.C.; Burgess, J.A.; Allen, K.J. Atopic dermatitis and the atopic march revisited. Allergy 2014, 69, 17–27. [Google Scholar] [CrossRef] [PubMed]
- Carroll, C.L.; Balkrishnan, R.; Feldman, S.R.; Fleischer, A.B.; Manuel, J.C. The burden of atopic dermatitis: Impact on the patient, family, and society. Pediatric Dermatol. 2005, 22, 192–199. [Google Scholar] [CrossRef]
- Deckers, I.A.; McLean, S.; Linssen, S.; Mommers, M.; Van Schayck, C.P.; Sheikh, A. Investigating international time trends in the incidence and prevalence of atopic eczema 1990–2010: A systematic review of epidemiological studies. PLoS ONE 2012, 7, e39803. [Google Scholar] [CrossRef] [Green Version]
- Asher, M.I.; Montefort, S.; Björkstén, B.; Lai, C.K.; Strachan, D.P.; Weiland, S.K.; Williams, H.; ISAAC Phase Three Study Group. Worldwide time trends in the prevalence of symptoms of asthma, allergic rhinoconjunctivitis, and eczema in childhood: ISAAC Phases One and Three repeat multicountry cross-sectional surveys. Lancet 2006, 368, 733–743. [Google Scholar] [CrossRef]
- Bieber, T. Atopic dermatitis. N. Engl. J. Med. 2008, 358, 1483–1494. [Google Scholar] [CrossRef]
- Forno, E.; Onderdonk, A.B.; McCracken, J.; Litonjua, A.A.; Laskey, D.; Delaney, M.L.; DuBois, A.M.; Gold, D.R.; Ryan, L.M.; Weiss, S.T.; et al. Diversity of the gut microbiota and eczema in early life. Clin. Mol. Allergy 2008, 22, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abrahamsson, T.R.; Jakobsson, H.E.; Andersson, A.F. Low diversity of the gut microbiota in infants with atopic eczema. J. Allery Clin. Immunol. 2012, 129, 434–440. [Google Scholar] [CrossRef] [Green Version]
- Tang, M.F.; Sy, H.Y.; Kwok, J.S.; Tam, W.H.; Hon, K.L.; Tung, C.K.; Wong, G.W.; Tsui, S.K.; Leung, T.F. Eczema susceptibility and composition of faecal microbiota at 4 weeks of age: A pilot study in Chinese infants. Br. J. Dermatol. 2016, 174, 898–900. [Google Scholar] [CrossRef] [PubMed]
- Ahmadizar, F.; Vijverberg, S.J.; Arets, H.G.; de Boer, A.; Turner, S.; Devereux, G.; Arabkhazaeli, A.; Soares, P.; Mukhopadhyay, S.; Garssen, J.; et al. Early life antibiotic use and the risk of asthma and asthma exacerbations in children. Pediatric Allergy Immunol. 2017, 28, 430–437. [Google Scholar] [CrossRef]
- Strachan, D.P. Hay fever, hygiene and household size. Br. Med J. 1989, 299, 1259–1260. [Google Scholar] [CrossRef] [Green Version]
- Verhasselt, V.; Milcent, V.; Cazareth, J.; Kanda, A.; Fleury, S. Breast milk-mediated transfer of an antigen induces tolerance and protection from allergic asthma. Nat. Med. 2008, 14, 170–175. [Google Scholar] [CrossRef] [PubMed]
- Sjogren, Y.M.; Jenmalm, M.C.; Böttcher, M.F.; Björkstén, B.; Sverremark-Ekström, E. Altered early infant gut microbiota in children developing allergy up to 5 years of age. Clin. Exp. Allergy 2009, 39, 518–526. [Google Scholar] [CrossRef] [Green Version]
- Bisgaard, H.; Li, N.; Bonnelykke, K.; Chawes, B.L.; Skov, T. Reduced diversity of the intestinal microbiota during infancy is associated with increased risk of allergic disease at school age. J. Allergy Clin. Immunol. 2011, 128, 646–652. [Google Scholar] [CrossRef]
- Ismail, I.H.; Oppedisano, F.; Joseph, S.J.; Boyle, R.J.; Licciardi, P.V. Reduced gut microbial diversity in early life is associated with later development of eczema but not atopy in high-risk infants. Pediatric Allergy Immunol. 2012, 23, 674–681. [Google Scholar] [CrossRef]
- Jenmalm, M.C. Childhood immune maturation and allergy development: Regulation by maternal immunity and microbial exposure. Am. J. Reprod. Immunol. 2011, 66 (Suppl. S1), 75–80. [Google Scholar] [CrossRef] [Green Version]
- Gollwitzer, E.S.; Marsland, B.J. Impact of early-life exposures on immune maturation and susceptibility to disease. Trends Immunol. 2015, 36, 684–696. [Google Scholar] [CrossRef]
- West, C.E.; Jenmalm, M.C.; Prescott, S.L. The gut microbiota and its role in the development of allergic disease: A wider perspective. Clin. Exp. Allergy 2015, 45, 43–53. [Google Scholar] [CrossRef] [Green Version]
- Jenmalm, M.C. The mother-offspring dyad: Microbial transmission, immuneinteractions and allergy development. J. Intern. Med. 2017, 282, 484–495. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Eczema | ||||
|---|---|---|---|---|
| Demographic Characteristics | All (n = 48) | No (n = 24) | Yes (n = 24) | p-Value |
| Mother’s age (years) † | 31.9 (3.9) | 31.5 (4.5) | 32.4 (3.5) | 0.394 # |
| Sex of the infant | ||||
| Female | 25 (52.1%) | 15 (62.5%) | 10 (41.7%) | 0.149 # |
| Male | 23 (47.9%) | 9 (37.5%) | 14 (58.3%) | |
| Low birth weight (<2.5 kg) | ||||
| No | 46 (95.8%) | 24 (100.0%) | 22 (91.7%) | 0.489 ψ |
| Yes | 2 (4.2%) | 0 (0.0%) | 2 (8.3%) | |
| Gestational age (weeks) | ||||
| 37–38 | 13 (27.1%) | 8 (33.3%) | 5 (20.8%) | 0.494 ψ |
| 39–40 | 29 (60.4%) | 14 (58.3%) | 15 (62.5%) | |
| >40 | 6 (12.5%) | 2 (8.3%) | 4 (16.7%) | |
| Mode of delivery | ||||
| Vaginal | 38 (79.2%) | 19 (79.2%) | 19 (79.2%) | 0.999 # |
| Cesarian section | 10 (20.8%) | 5 (20.8%) | 5 (20.8%) | |
| The infant is the first child | ||||
| No | 25 (52.1%) | 14 (58.3%) | 11 (45.8%) | 0.386 # |
| Yes | 23 (47.9%) | 10 (41.7%) | 13 (54.2%) | |
| Number of siblings of the infant | ||||
| 0 | 24 (50.0%) | 11 (45.8%) | 13 (54.2%) | 0.882 ψ |
| 1 | 22 (45.8%) | 12 (50.0%) | 10 (41.7%) | |
| 2 | 2 (4.2%) | 1 (4.2%) | 1 (4.2%) | |
| Mother’s education | ||||
| Secondary | 25 (52.1%) | 15 (62.5%) | 10 (41.7%) | 0.149 # |
| Tertiary | 23 (47.9%) | 9 (37.5%) | 14 (58.3%) | |
| Father’s education | ||||
| Secondary | 21 (43.8%) | 15 (62.5%) | 6 (25.0%) | 0.009 # |
| Tertiary | 27 (56.3%) | 9 (37.5%) | 18 (75.0%) | |
| Monthly household income (HK$) | ||||
| 10,000–19,999 | 7 (14.6%) | 4 (16.7%) | 3 (12.5%) | 0.233 ψ |
| 20,000–29,999 | 11 (22.9%) | 7 (29.2%) | 4 (16.7%) | |
| 30,000–59,999 | 23 (47.9%) | 12 (50.0%) | 11 (45.8%) | |
| ≥60,000 | 7 (14.6%) | 1 (4.2%) | 6 (25.0%) | |
| Control | Eczema | ||||
|---|---|---|---|---|---|
| Genus | Mean ± S.D. | Median (IQR) | Mean ± S.D. | Median (IQR) | p-Value # |
| Klebsiella | 3.33 ± 4.63 | 1.62 (0.65–3.59) | 6.69 ± 13.47 | 2.90 (1.21–5.76) | 0.219 |
| Escherichia | 27.12 ± 15.66 | 25.26 (13.85–39.77) | 13.97 ± 17.30 | 17.36 (12.53–31.45) | 0.418 |
| Lactobacillus | 3.45 ± 11.10 | 0.47 (0.08–1.25) | 1.70 ± 2.34 | 0.62 (0.16–2.06) | 0.503 |
| Bifidobacterium | 12.49 ± 12.24 | 6.41 (4.61–14.58) | 18.98 ± 15.03 | 13.21 (7.90–23.07) | 0.040 * |
| Bacteroides | 15.10 ± 8.83 | 14.62 (9.22–19.15) | 13.00 ± 11.43 | 9.97 (7.72–13.88) | 0.097 |
| Clostridium | 6.66 ± 9.75 | 3.16 (0.99–8.33) | 3.42 ± 6.42 | 1.26 (0.38–3.38) | 0.112 |
| Parabacteroides | 5.73 ± 8.92 | 2.62 (1.61–5.91) | 5.17 ± 6.57 | 3.32 (1.19–7.05) | 0.772 |
| Collinsella | 2.06 ± 5.37 | 0.36 (0.17–1.07) | 2.04 ± 3.90 | 0.61 (0.25–1.99) | 0.144 |
| Ruminococcaceae | 0.38 ± 0.57 | 0.19 (0.02–0.56) | 1.18 ± 4.81 | 0.09 (0.03–0.40) | 0.465 |
| Streptococcus | 3.17 ± 4.76 | 1.85 (0.91–3.03) | 2.78 ± 3.34 | 2.02 (0.92–3.77) | 0.928 |
| Ruminococcus | 0.66 ± 0.70 | 0.40 (0.23–0.88) | 1.71 ± 4.00 | 0.55 (0.21–1.14) | 0.575 |
| Veillonella | 2.64 ± 3.25 | 1.11 (0.58–4.05) | 3.42 ± 4.31 | 1.42 (0.72–6.32) | 0.430 |
| Megamonas | 0.78 ± 3.27 | 0.02 (0.00–0.20) | 0.09 ± 0.16 | 0.02 (0.01–0.12) | 0.728 |
| Akkermansia | 1.78 ± 4.14 | 0.09 (0.01–0.63) | 0.08 ± 0.10 | 0.03 (0.01–0.16) | 0.089 |
| Hungatella | 1.30 ± 2.69 | 0.27 (0.12–1.15) | 0.73 ± 1.07 | 0.18 (0.05–1.23) | 0.358 |
| Lachnoclostridium | 1.03 ± 1.87 | 0.38 (0.11–0.94) | 0.95 ± 1.87 | 0.35 (0.09–0.92) | 0.646 |
| Megasphaera | 0.40 ± 1.53 | 0.04 (0.02–0.14) | 0.45 ± 1.21 | 0.07 (0.03–0.13) | 0.258 |
| Enterococcus | 1.17 ± 1.49 | 0.68 (0.31–1.37) | 1.05 ± 1.05 | 0.75 (0.52–1.14) | 0.674 |
| Prevotella | 0.28 ± 0.54 | 0.00 (0.00–0.43) | 0.32 ± 1.27 | 0.01 (0.00–0.01) | 0.795 |
| Atopobium | 0.03 ± 0.06 | 0.01 (0.00–0.02) | 0.30 ± 1.14 | 0.02 (0.00–0.13) | 0.091 |
| Item | Eczema | |||
|---|---|---|---|---|
| All (n = 48) | No (n = 24) | Yes (n = 24) | p-Value | |
| How many servings of fruit did you have every day on average during pregnancy (including all kinds of fresh, frozen, canned or dried fruits but excluding fruit juice and fruit desserts like mango pancake, apple pie, etc.)? | ||||
| None, or less than 1 serving per day | 7 (14.6%) | 4 (16.7%) | 3 (12.5%) | 0.385 ψ |
| 1 serving per day | 16 (33.3%) | 10 (41.7%) | 6 (25.0%) | |
| 1 serving per day | 25 (52.1%) | 10 (41.7%) | 15 (62.5%) | |
| How many glasses of fruit juice did you drink every day on average during pregnancy (excluding sugar-added fruit juice)? | ||||
| None, or less than 1 glass per day | 47 (97.9%) | 24 (100.0%) | 23 (95.8%) | 0.999 ψ |
| 1 glass per day | 0 (.0%) | 0 (0.0%) | 0 (0.0%) | |
| 2 glasses (or more) per day | 1 (2.1%) | 0 (0.0%) | 1 (4.2%) | |
| How many servings of vegetables did you have every day on average during pregnancy (including fresh, frozen or canned vegetables but excluding vegetable juice)? | ||||
| None, or less than 1 serving per day | 3 (6.3%) | 1 (4.2%) | 2 (8.3%) | 0.365 ψ |
| 1 serving per day | 18 (37.5%) | 12 (50.0%) | 6 (25.0%) | |
| 2 servings per day | 18 (37.5%) | 8 (33.3%) | 10 (41.7%) | |
| 3 servings (or more) per day | 9 (18.8%) | 3 (12.5%) | 6 (25.0%) | |
| How many tael(s) * of meat, fish and eggs did you eat every day during pregnancy? | ||||
| None, or less than 1 tael | 1 (2.1%) | 0 (.0%) | 1 (4.2%) | 0.999 ψ |
| 1 to 2 taels per day | 6 (12.5%) | 3 (12.5%) | 3 (12.5%) | |
| 3 to 4 taels per day | 24 (50.0%) | 12 (50.0%) | 12 (50.0%) | |
| 5 taels (or more) per day | 17 (35.4%) | 9 (37.5%) | 8 (33.3%) | |
| How many servings of bean products did you have every day on average during pregnancy? | ||||
| None, or less than half serving per day | 28 (58.3%) | 14 (58.3%) | 14 (58.3%) | 0.999 ψ |
| Half a serving per day | 5 (10.4%) | 3 (12.5%) | 2 (8.3%) | |
| 1 serving per day | 11 (22.9%) | 5 (20.8%) | 6 (25.0%) | |
| 2 servings (or more) per day | 4 (8.3%) | 2 (8.3%) | 2 (8.3%) | |
| How many dairy products did you have every day during pregnancy? | ||||
| None, or less than 1 glass per day | 17 (35.4%) | 13 (54.2%) | 4 (16.7%) | 0.007 ψ |
| 1 glass per day | 26 (54.2%) | 8 (33.3%) | 18 (75.0%) | |
| 2 glasses (or more) per day | 5 (10.4%) | 3 (12.5%) | 2 (8.3%) | |
| How often did you eat stir-/deep-fried food or food with a large amount of oil during pregnancy (e.g., French fries, fried rice/noodles, sweet and sour pork, tempura, etc.)? | ||||
| None, or less than once a day | 41 (85.4%) | 21 (87.5%) | 20 (83.3%) | 0.999 ψ |
| Once a day | 7 (14.6%) | 3 (12.5%) | 4 (16.7%) | |
| How often did you have desserts or sugary foods and drinks during pregnancy (e.g., soft drinks, ice cream, chocolate, sweets, cake, pineapple buns, sugar-added coffee or tea, etc.)? | ||||
| None, or less than once a day | 29 (60.4%) | 14 (58.3%) | 15 (62.5%) | 0.901 ψ |
| Once a day | 14 (29.2%) | 8 (33.3%) | 6 (25.0%) | |
| Twice a day | 4 (8.3%) | 2 (8.3%) | 2 (8.3%) | |
| 3 times (or more) a day | 1 (2.1%) | 0 (0.0%) | 1 (4.2%) | |
| How many serving(s) of grains did you eat every day on average during pregnancy (including pasta; noodles; oatmeal; rice; bread; biscuits or starchy vegetables such as potatoes, taro, etc.)? | ||||
| None, or less than 1 serving per day | 1 (2.1%) | 0 (0.0%) | 1 (4.2%) | 0.057 ψ |
| 1 serving per day | 9 (18.8%) | 2 (8.3%) | 7 (29.2%) | |
| 2 servings per day | 22 (45.8%) | 15 (62.5%) | 7 (29.2%) | |
| 3 servings (or more) per day | 16 (33.3%) | 7 (29.2%) | 9 (37.5%) | |
| How many serving(s) of whole grains did you eat every day on average during pregnancy (including oatmeal, rice (red or brown), whole meal bread, high-fiber biscuits, etc.)? | ||||
| None, or less than 1 serving per day | 38 (79.2%) | 20 (83.3%) | 18 (75.0%) | 0.477 # |
| 1 serving per day | 10 (20.8%) | 4 (16.7%) | 6 (25.0%) | |
| Item | Eczema | |||
|---|---|---|---|---|
| All (n = 48) | No (n = 24) | Yes (n = 24) | p-Value | |
| Which of the following describe most accurately your daily dietary practices during pregnancy (excluding snacks at tea time or at night)? | ||||
| 3 regular meals daily | 31 (64.6%) | 15 (62.5%) | 16 (66.7%) | 0.999 ψ |
| 3 meals daily but taken irregularly | 13 (27.1%) | 6 (25.0%) | 7 (29.2%) | |
| 1 to 2 meals daily at regular hours | 1 (2.1%) | 1 (4.2%) | 0 (.0%) | |
| Irregular meals | 3 (6.3%) | 2 (8.3%) | 1 (4.2%) | |
| How often did you have snacks apart from regular meals during pregnancy (including at tea time and at night)? | ||||
| None, or less than once a day | 22 (45.8%) | 11 (45.8%) | 11 (45.8%) | 0.752 ψ |
| Once a day | 22 (45.8%) | 10 (41.7%) | 12 (50.0%) | |
| Twice (or more) a day | 4 (8.3%) | 3 (12.5%) | 1 (4.2%) | |
| Which of the following describes most accurately your breakfast habits during pregnancy? | ||||
| No breakfast at all | 1 (2.1%) | 0 (.0%) | 1 (4.2%) | 0.999 ψ |
| No breakfast most of the time | 2 (4.2%) | 1(4.2%) | 1 (4.2%) | |
| Breakfast most of the time | 45 (93.8%) | 23 (95.8%) | 22 (91.7%) | |
| How many meals (including breakfast, lunch, dinner and tea time and night snacks) did you or your family members make every day on average during your pregnancy? | ||||
| Less than 1 meal per day | 4 (8.3%) | 3 (12.5%) | 1 (4.2%) | 0.752 ψ |
| 1 meal per day | 17 (35.4%) | 9 (37.5%) | 8 (33.3%) | |
| 2 meals per day | 17 (35.4%) | 8 (33.3%) | 9 (37.5%) | |
| 3 meals (or more) per day | 10 (20.8%) | 4 (16.7%) | 6 (25.0%) | |
| Did you take any supplements during pregnancy? | ||||
| No | 5 (10.4%) | 3 (12.5%) | 2 (8.3%) | 0.037 ψ |
| Yes, <3 months | 4 (8.3%) | 4 (16.7%) | 0 (.0%) | |
| Yes, 3–6 months | 4 (8.3%) | 1 (4.2%) | 3 (12.5%) | |
| Yes, 6–9 months | 22 (45.8%) | 13 (54.2%) | 9 (37.5%) | |
| Yes, 9–12 months | 13 (27.1%) | 3 (12.5%) | 10 (41.7%) | |
| Item | Eczema | |||
|---|---|---|---|---|
| All (n = 48) | No (n = 24) | Yes (n = 24) | p-Value | |
| Family history of eczema | ||||
| No | 33 (68.8%) | 18 (75.0%) | 15 (62.5%) | 0.350 # |
| Yes | 15 (31.3%) | 6 (25.0%) | 9 (37.5%) | |
| Family history of asthma | ||||
| No | 43 (89.6%) | 21 (87.5%) | 22 (91.7%) | 0.999 ψ |
| Yes | 5 (10.4%) | 3 (12.5%) | 2 (8.3%) | |
| Family history of pollen allergy | ||||
| No | 46 (95.8%) | 23 (95.8%) | 23 (95.8%) | 0.999 ψ |
| Yes | 2 (4.2%) | 1 (4.2%) | 1 (4.2%) | |
| Family history of food allergy | ||||
| No | 40 (83.3%) | 21 (87.5%) | 19 (79.2%) | 0.701 ψ |
| Yes | 8 (16.7%) | 3 (12.5%) | 5 (20.8%) | |
| Have you breastfed (for any length of time), or are you breastfeeding your child now? | ||||
| No | 7 (14.6%) | 5 (20.8%) | 2 (8.3%) | 0.416 ψ |
| Yes | 41 (85.4%) | 19 (79.2%) | 22 (91.7%) | |
| Was your child taking formula, as either the main or complementary food (for any time)? | ||||
| No | 40 (83.3%) | 19 (79.2%) | 21 (87.5%) | 0.701 ψ |
| Yes | 8 (16.7%) | 5 (20.8%) | 3 (12.5%) | |
| Were you smoking during pregnancy? | ||||
| No | 46 (95.8%) | 22 (91.7%) | 24 (100.0%) | 0.489 ψ |
| Yes | 2 (4.2%) | 2 (8.3%) | 0 (0.0%) | |
| Does anybody currently smoke inside your child’s home? | ||||
| No | 35 (72.9%) | 19 (79.2%) | 16 (66.7%) | 0.330 # |
| Yes | 13 (27.1%) | 5 (20.8%) | 8 (33.3%) | |
| Did you receive any antibiotic treatment during pregnancy? | ||||
| No | 37 (77.1%) | 17 (70.8%) | 20 (83.3%) | 0.494 ψ |
| Yes | 10 (20.8%) | 6 (25.0%) | 4 (16.7%) | |
| Do not know | 1 (2.1%) | 1 (4.2%) | 0 (.0%) | |
| Did you have any pet at home during pregnancy? | ||||
| No | 33 (68.8%) | 20 (83.3%) | 13 (54.2%) | 0.029 # |
| Yes | 15 (31.3%) | 4 (16.7%) | 11 (45.8%) | |
| Did you have any furry pet at home during pregnancy? | ||||
| No | 35 (72.9%) | 20 (83.3%) | 15 (62.5%) | 0.104 # |
| Yes | 13 (27.1%) | 4 (16.7%) | 9 (37.5%) | |
| Do you have any pet at home now? | ||||
| No | 38 (79.2%) | 21 (87.5%) | 17 (70.8%) | 0.155 # |
| Yes | 10 (20.8%) | 3 (12.5%) | 7 (29.2%) | |
| Do you have any furry pet at home now? | ||||
| No | 39 (81.3%) | 21 (87.5%) | 18 (75.0%) | 0.461 ψ |
| Yes | 9 (18.8%) | 3 (12.5%) | 6 (25.0%) | |
| Did a doctor ever say you had an infection during pregnancy? | ||||
| No | 29 (60.4%) | 14 (58.3%) | 15 (62.5%) | 0.768 # |
| Yes | 19 (39.6%) | 10 (41.7%) | 9 (37.5%) | |
| What is your rating of the air quality in the area where you live? | ||||
| Good | 26 (54.2%) | 13 (54.2%) | 13 (54.2%) | 0.999 ψ |
| Moderate | 20 (41.7%) | 10 (41.7%) | 10 (41.7%) | |
| Bad | 2 (4.2%) | 1 (4.2%) | 1 (4.2%) | |
| Item | Eczema | |||||
|---|---|---|---|---|---|---|
| No (n = 24) | Yes (n = 24) | ORU | p | ORA (95% CI) | p | |
| Father’s education | ||||||
| Secondary | 15 (71.4%) | 6 (28.6%) | 1 | 1 | ||
| Tertiary | 9 (33.3%) | 18 (66.7%) | 5.00 | 0.011 | 9.93 (1.83–53.71) | 0.008 |
| Dairy products consumed daily during pregnancy | ||||||
| <1 glass | 13 (76.5%) | 4 (23.5%) | 1 | NS | ||
| ≥1 glass | 11 (35.5%) | 20 (64.5%) | 5.91 | 0.009 | ||
| Cereal food consumed daily during pregnancy | ||||||
| ≤1 proportion | 2 (20.0%) | 8 (80.0%) | 1 | 1 | ||
| ≥2 proportions | 22 (57.9%) | 16 (42.1%) | 0.18 | 0.046 | 0.10 (0.01–0.82) | 0.032 |
| Having taken nutritional supplements for more than 9 months during pregnancy | ||||||
| No | 21 (60.0%) | 14 (40.0%) | 1 | 1 | ||
| Yes | 3 (23.1%) | 10 (76.9%) | 4.99 | 0.030 | 10.75 (1.57–73.46) | 0.015 |
| Having pets at home during pregnancy | ||||||
| No | 20 (60.6%) | 13 (39.4%) | 1 | NS | ||
| Yes | 4 (26.7%) | 11 (73.3%) | 4.23 | 0.035 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chan, C.W.H.; Yuet Wa Chan, J.; Leung, T.F.; Choi, K.C.; Tsui, S.K.W.; Wong, C.L.; Chow, K.M. Altered Gut Microbiome and Environmental Factors Associated with Development of Eczema in Hong Kong Infants: A 4-Month Pilot Study. Int. J. Environ. Res. Public Health 2020, 17, 7634. https://doi.org/10.3390/ijerph17207634
Chan CWH, Yuet Wa Chan J, Leung TF, Choi KC, Tsui SKW, Wong CL, Chow KM. Altered Gut Microbiome and Environmental Factors Associated with Development of Eczema in Hong Kong Infants: A 4-Month Pilot Study. International Journal of Environmental Research and Public Health. 2020; 17(20):7634. https://doi.org/10.3390/ijerph17207634
Chicago/Turabian StyleChan, Carmen Wing Han, Judy Yuet Wa Chan, Ting Fan Leung, Kai Chow Choi, Stephen Kwok Wing Tsui, Cho Lee Wong, and Ka Ming Chow. 2020. "Altered Gut Microbiome and Environmental Factors Associated with Development of Eczema in Hong Kong Infants: A 4-Month Pilot Study" International Journal of Environmental Research and Public Health 17, no. 20: 7634. https://doi.org/10.3390/ijerph17207634