The Design, Content and Delivery of Relationship and Sexuality Education Programmes for People with Intellectual Disabilities: A Systematic Review of the International Evidence


Abstract
:1. Introduction
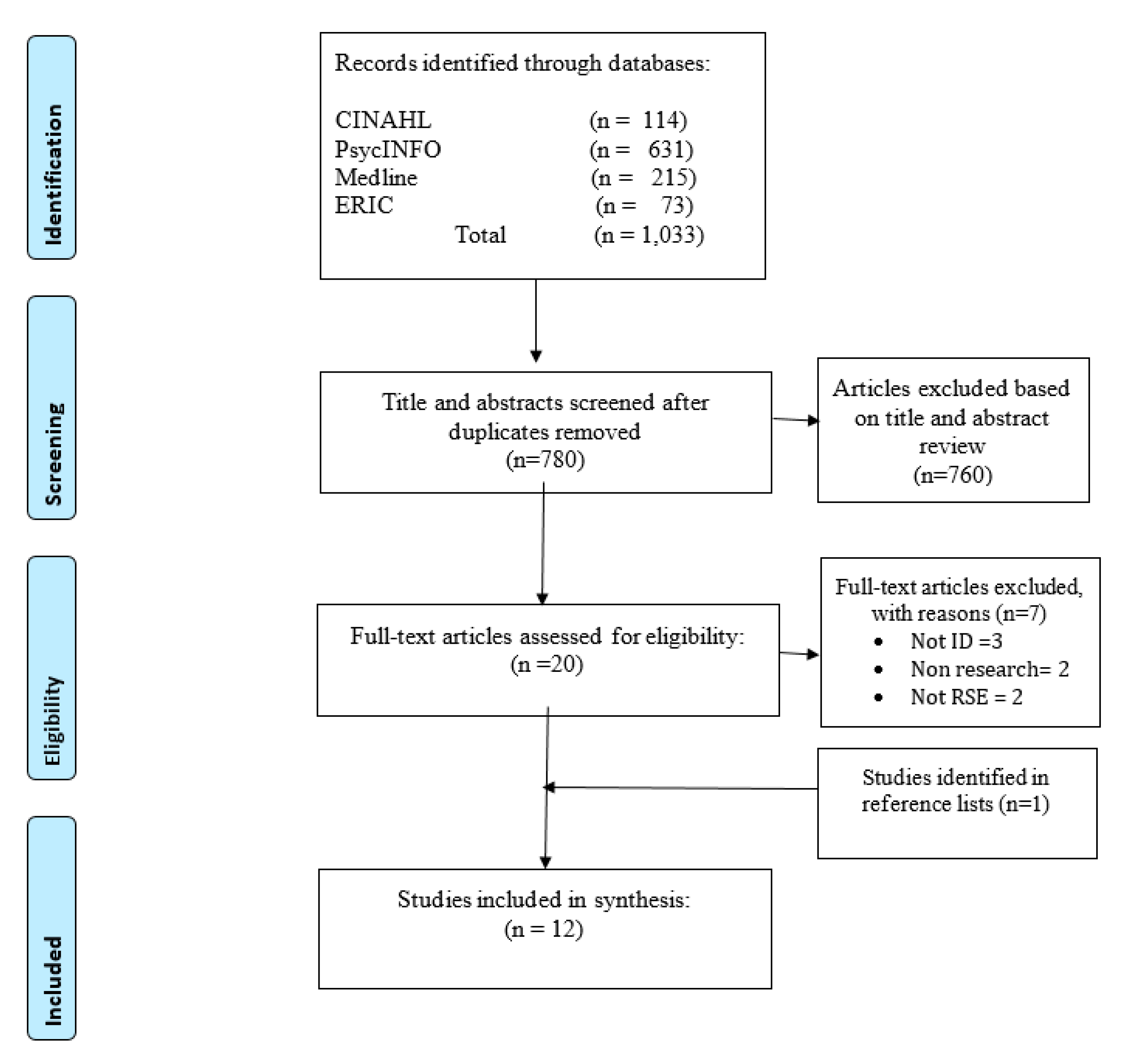
2. Methods
- to identify who is involved in the design and development of RSE programmes for people with intellectual disabilities,
- to establish the content of the RSE programmes,
- to identify who delivers the RSE programmes and
- to identify if evaluations have been undertaken of the RSE programmes.
2.1. Search Strategy
Ethics Statement
2.2. Inclusion and Exclusion Criteria
- focused on the design, content, delivery or evaluation of RSE programmes specific to people with ID,
- utilized an empirical research design,
- were published in the English language.
- were published from inception to August 2020.
- did not focus exclusively on RSE programmes for people with ID,
- did not address the design, content, delivery or evaluation of RSE programmes specific to people with ID,
- were not empirical research,
- were not published in English and
- were grey literature and theses.
2.3. Data Extraction and Synthesis
2.4. Quality Assessment
3. Results
3.1. Study Characteristics
3.2. Data Analysis and Synthesis
3.2.1. Principles Informing RSE Programme Development
3.2.2. Design and Content of RSE Programmes
3.2.3. Delivery of RSE Programmes
3.2.4. Evaluation of RSE Programmes
4. Discussion
4.1. Policy
4.2. Practice
4.3. Education
5. Strengths and Limitations
6. Future Research
7. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization. Sexual Health, Human Rights and the Law; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Diderichsen, F.; Hallqvist, J.; Whitehead, M. Differential vulnerability and susceptibility: How to make use of recent development in our understanding of mediation and interaction to tackle health inequalities. Int. J. Epidemiol. 2019, 48, 268–274. [Google Scholar] [CrossRef] [PubMed]
- Richardson, E.; Fenton, L.; Parkinson, J.; Pulford, A.; Taulbut, M.; McCartney, G.; Robinson, M. The Impact of Income-Based Policies on Population Health and Health Inequalities in Scotland: A Modelling Study. Lancet Pub. Health 2020, 5, E150–E156. [Google Scholar] [CrossRef] [Green Version]
- Nutbeam, D. Health education and health promotion revisited. Health Ed. J. 2019, 78, 705–709. [Google Scholar] [CrossRef] [Green Version]
- Battel-Kirk, B.; Barry, M. Evaluating progress in the uptake and impact of Health Promotion competencies in Europe. Health Promot. Int. 2020, 35, 779–789. [Google Scholar] [CrossRef] [PubMed]
- Kwasnicka, D.; Dombrowski, S.; White, M.; Sniehotta, F. Theoretical explanations for maintenance of behaviour change: A systematic review of behaviour theories. Health Psychol. Rev. 2016, 10, 277–296. [Google Scholar] [CrossRef] [PubMed]
- Gabarron, E.; Wynn, R. Use of social media for sexual health promotion: A scoping review. Glob. Health Action. 2016, 9, 32193. [Google Scholar] [CrossRef]
- Martin, P.; Cousin, L.; Gottot, S.; Bourmaud, A.; de La Rochebrochard, E.; Alberti, C. Participatory Interventions for Sexual Health Promotion for Adolescents and Young Adults on the Internet: Systematic Review. J. Med. Internet Res. 2020, 22, e15378. [Google Scholar] [CrossRef] [PubMed]
- Toskin, I.; Blondeel, K. Advancing STI Prevention Through Sexual Health Promotion: Brief Sexuality-Related Communication and Sexual Health Indicators. J. Sex Med. 2017, 14, e230. [Google Scholar] [CrossRef]
- Marrazzo, J.; Dombrowski, J.; Mayer, K. Sexually transmitted infections in the era of antiretroviral-based HIV prevention: Priorities for discovery research, implementation science, and community involvement. PLoS Med. 2018, 15, e1002485. [Google Scholar] [CrossRef] [Green Version]
- Widman, L.; Nesi, J.; Kamke, K.; Choukas-Bradley, S.; Stewart, J. Technology-based interventions to reduce sexually transmitted infections and unintended pregnancy among youth. J. Adolesc. Health. 2018, 62, 651–660. [Google Scholar] [CrossRef]
- Lunde, B.; Perry, R.; Sridhar, A.; Chen, K. An evaluation of contraception education and health promotion applications for patients. Women’s Health Issues 2017, 27, 29–35. [Google Scholar] [CrossRef]
- Reid, N.; Kron, A.; Rajakulendran, T.; Kahan, D.; Noble, A.; Stergiopoulos, V. Promoting Wellness and Recovery of Young Women Experiencing Gender-Based Violence and Homelessness: The Role of Trauma-Informed Health Promotion Interventions. Violence Against Women 2020, 23, 1077801220923748. [Google Scholar] [CrossRef]
- Burns, S.; Hendriks, J.; Mayberry, L.; Duncan, S.; Lobo, R.; Pelliccione, L. Evaluation of the implementation of a relationship and sexuality education project in Western Australian schools: Protocol of a multiple, embedded case study. BMJ Open 2019, 9, e026657. [Google Scholar] [CrossRef] [PubMed]
- Aventin, Á.; Gough, A.; McShane, T.; Gillespie, K.; O’Hare, L.; Young, H.; Lewis, R.; Warren, E.; Buckley, K.; Lohan, M. Engaging parents in digital sexual and reproductive health education: Evidence from the JACK trial. Reproductive Health 2020, 17, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Janssens, A.; Blake, S.; Allwood, M.; Ewing, J.; Barlow, A. Exploring the content and delivery of relationship skills education programmes for adolescents: A systematic review. Sex Educ. 2020, 20, 494–516. [Google Scholar] [CrossRef]
- Department of Education. Relationships Education, Relationships and Sex Education (RSE) and Health Education: Guidance for Governing Bodies, Proprietors, Head Teachers, Principals, Senior Leadership Teams, Teachers; HMSO: London, UK, 2018. [Google Scholar]
- Ezer, P.; Kerr, L.; Fisher, C.; Heywood, W.; Lucke, J. Australian students’ experiences of sexuality education at school. Sex Education. 2019, 19, 597–613. [Google Scholar] [CrossRef]
- Lohan, M.; Aventin, Á.; Clarke, M.; Curran, R.; Maguire, L.; Hunter, R.; McDowell, C.; McDaid, L.; Young, H.; White, J.; et al. JACK trial protocol: A phase III multicentre cluster randomised controlled trial of a school-based relationship and sexuality education intervention focusing on young male perspectives. BMJ Open 2018, 8, e022128. [Google Scholar] [CrossRef] [Green Version]
- McCann, E.; Marsh, L.; Brown, M. People with intellectual disabilities, relationship and sex education programmes: A systematic review. Health Educ. J. 2019, 78, 885–900. [Google Scholar] [CrossRef]
- Scottish Government. The Keys to Life: Improving Quality of Life for People with Learning Disabilities; The Sationery Office: Edinburgh, Scotland, 2013. [Google Scholar]
- Louw, J.; Kirkpatrick, B.; Leader, G. Enhancing social inclusion of young adults with intellectual disabilities: A systematic review of original empirical studies. J. Appl. Res. Intellect Disabil. 2020, 33, 793–807. [Google Scholar] [CrossRef]
- Alonso-Sardón, M.; Iglesias-de-Sena, H.; Fernández-Martín, L.; Mirón-Canelo, J. Do health and social support and personal autonomy have an influence on the health-related quality of life of individuals with intellectual disability? BMC Health Serv. Res. 2019, 19, 63. [Google Scholar] [CrossRef]
- Fulford, C.; Cobigo, V. Friendships and intimate relationships among people with intellectual disabilities: A thematic synthesis. J. Appl. Res. Intellect Disabil. 2018, 31, e18–e35. [Google Scholar] [CrossRef] [PubMed]
- Cook, A. Employing a social justice framework to promote postsecondary transition for students with intellectual disability. Int. J. Educ. Vocat Guid. 2017, 17, 311–328. [Google Scholar] [CrossRef]
- English, B.; Tickle, A. Views and experiences of people with intellectual disabilities regarding intimate relationships: A qualitative metasynthesis. Sex Disabil. 2018, 36, 149–173. [Google Scholar] [CrossRef]
- Darragh, J.; Reynolds, L.; Ellison, C.; Bellon, M. Let’s talk about sex: How people with intellectual disability in Australia engage with online social media and intimate relationships. Cyberpsychology. 2017, 11. [Google Scholar] [CrossRef] [Green Version]
- Bates, C.; Terry, L.; Popple, K. Supporting people with learning disabilities to make and maintain intimate relationships. Tizard Learn. Disabil. Rev. 2017, 22, 16. [Google Scholar] [CrossRef]
- Brown, M.; McCann, E. The views and experiences of families and direct care support workers regarding the expression of sexuality by adults with intellectual disabilities: A narrative review of the international research evidence. Res. Dev. Disabil. 2019, 90, 80–91. [Google Scholar] [CrossRef]
- Rushbrooke, E.; Murray, C.; Townsend, S. The experiences of intimate relationships by people with intellectual disabilities: A qualitative study. J. Appl. Res. Intellect. Disabil. 2014, 27, 531–541. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, M.; Forrester-Jones, R.; Bates, C.; Skillman, K.; Elson, N. Love and loving relationships: What they mean for people with learning disabilities. J. Intellect Disabil. Res. 2020, 63, 863. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 1. [Google Scholar] [CrossRef] [Green Version]
- Noyes, J.; Booth, A.; Moore, G.; Flemming, K.; Tunçalp, Ö.; Shakibazadeh, E. Synthesising quantitative and qualitative evidence to inform guidelines on complex interventions: Clarifying the purposes, designs and outlining some methods. BMJ Glob. Health 2019, 4, e000893. [Google Scholar] [CrossRef]
- Veritas Health Innovation. Covidence systematic review software. Melbourne, Australia. Available online: www.covidence.org. (accessed on 13 October 2020).
- Terry, G.; Hayfield, N.; Clarke, V.; Braun, V. Thematic analysis. In The Sage Handbook of Qualitative Research in Psychology; Sage Publishing: Thousand Oaks, CA, USA, 2017. [Google Scholar]
- Hong, Q.; Fàbregues, S.; Bartlett, G.; Boardman, F.; Cargo, M.; Dagenais, P.; Gagnon, M.; Griffiths, F.; Nicolau, B.; O’Cathain, A.; et al. The Mixed Methods Appraisal Tool (MMAT) version 2018 for information professionals and researchers. Educ. Informat. 2018, 34, 285–291. [Google Scholar] [CrossRef] [Green Version]
- Frawley, P.; Bigby, C. “I’m in their shoes”: Experiences of peer educators in sexuality and relationship education. J. Intellect Dev. Disabil. 2014, 39, 67–76. [Google Scholar] [CrossRef]
- Lafferty, A.; McConkey, R.; Simpson, A. Reducing the barriers to relationships and sexuality education for persons with intellectual disabilities. J. Intellect Disabil. 2012, 16, 29–43. [Google Scholar] [CrossRef]
- Löfgren-Mårtenson, L. “I want to do it right!” A pilot study of Swedish sex education and young people with intellectual disabilities. Sex Disabil. 2012, 30, 209–225. [Google Scholar] [CrossRef] [Green Version]
- Louw, J. A qualitative exploration of teacher and school staff experiences when teaching sexuality education programmes at special needs schools in South Africa. Sex Res. Soc. Policy 2017, 14, 425–433. [Google Scholar] [CrossRef]
- Nelson, B.; Odberg Pettersson, K.; Emmelin, M. Experiences of teaching sexual and reproductive health to students with intellectual disabilities. Sex Educ. 2020, 20, 398–412. [Google Scholar] [CrossRef] [Green Version]
- Phasha, T.; Runo, M. Sexuality Education in Schools for Learners with Intellectual Disabilities in Kenya: Empowerment or disempowerment? Sex Disabil. 2017, 35, 353–370. [Google Scholar] [CrossRef]
- Schaafsma, D.; Stoffelen, J.; Kok, G.; Curfs, L. Exploring the development of existing sex education programmes for people with intellectual disabilities: An intervention mapping approach. J. Appl. Res. Intellect Disabil. 2013, 26, 157–166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilson, N.; Frawley, P. Transition staff discuss sex education and support for young men and women with intellectual and developmental disability. J. Intellect. Dev. Disabil. 2016, 41, 209–221. [Google Scholar] [CrossRef]
- Swango-Wilson, A. Perception of sex education for individuals with developmental and cognitive disability: A four cohort study. Sex Disabil. 2009, 27, 223. [Google Scholar] [CrossRef]
- Katoda, H.; Gunilla, W.; Mannerfeldt, R. School nurses and health education for pupils with and without intellectual handicaps: A study conducted in Japan and Sweden. Nurse Educ. Today. 1990, 10, 437–447. [Google Scholar] [CrossRef]
- Louw, J.; Kosciulek, J.; Chen, R. Investigating educators’ views of sexuality, HIV and AIDS education in working with students with disabilities in South African schools. J. Appl. Rehabil. Couns. 2014, 45, 9–17. [Google Scholar] [CrossRef]
- Murray, B. Sexual health education for adolescents with developmental disabilities. Health Educ. J. 2019, 78, 1000–1011. [Google Scholar] [CrossRef]
- World Health Organization. Standards for Sexuality Education in Europe: A framework for Policy Makers, Educational and Health Authorities and Specialists; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Reynolds, K. Relationships and sexuality education for children with special educational needs and disabilities. J. Health Visit. 2019, 7, 78–84. [Google Scholar] [CrossRef]
- Al Hazmi, A.; Ahmad, A. Universal Design for Learning to Support Access to the General Education Curriculum for Students with Intellectual Disabilities. World J. Educ. 2018, 8, 66–72. [Google Scholar] [CrossRef] [Green Version]
- Pound, P.; Denford, S.; Shucksmith, J.; Tanton, C.; Johnson, A.; Owen, J.; Hutten, R.; Mohan, L.; Bonell, C.; Abraham, C.; et al. What is best practice in sex and relationship education? A synthesis of evidence, including stakeholders’ views. BMJ Open 2017, 7, 5. [Google Scholar] [CrossRef]
- Baines, S.; Emerson, E.; Robertson, J.; Hatton, C. Sexual activity and sexual health among young adults with and without mild/moderate intellectual disability. BMC Public Health 2018, 18, 667. [Google Scholar] [CrossRef]
- Robinson, K.; Smith, E.; Davies, C. Responsibilities, tensions and ways forward: Parents’ perspectives on children’s sexuality education. Sex Educ. 2017, 17, 333–347. [Google Scholar] [CrossRef]
- McDaniels, B.; Fleming, A. Sexuality education and intellectual disability: Time to address the challenge. Sex Disabil. 2016, 34, 215–225. [Google Scholar] [CrossRef]
- Whittle, C.; Butler, C. Sexuality in the lives of people with intellectual disabilities: A meta-ethnographic synthesis of qualitative studies. Res. Dev. Disabil. 2018, 75, 68–81. [Google Scholar] [CrossRef]
- Medina-Rico, M.; López-Ramos, H.; Quiñonez, A. Sexuality in people with intellectual disability: Review of literature. Sex Disabil. 2018, 36, 231–248. [Google Scholar] [CrossRef]
- Björnsdóttir, K.; Stefánsdóttir, Á.; Stefánsdóttir, G. People with intellectual disabilities negotiate autonomy, gender and sexuality. Sex Disabil. 2017, 35, 295–311. [Google Scholar] [CrossRef]
- Ditchman, N.; Easton, A.; Batchos, E.; Rafajko, S.; Shah, N. The impact of culture on attitudes toward the sexuality of people with intellectual disabilities. Sex Disabil. 2017, 35, 245–260. [Google Scholar] [CrossRef]
- Tamas, D.; Jovanovic, N.; Rajic, M.; Ignjatovic, V.; Prkosovacki, B. Professionals, parents and the general public: Attitudes towards the sexuality of persons with intellectual disability. Sex Disabil. 2019, 37, 245–258. [Google Scholar] [CrossRef]
- Olsen, A.; Carter, C. Responding to the needs of people with learning disabilities who have been raped: Co-production in action. Tizard Learn Disabil. Rev. 2016, 21, 30. [Google Scholar] [CrossRef] [Green Version]
- Curran, T.; Jones, M.; Ferguson, S.; Reed, M.; Lawrence, A.; Cull, N.; Stabb, M. Disabled young people’s hopes and dreams in a rapidly changing society: A co-production peer research study. Disabil Soc. 2020, 22, 1–8. [Google Scholar] [CrossRef]
- Hanass-Hancock, J.; Nene, S.; Johns, R.; Chappell, P. The impact of contextual factors on comprehensive sexuality education for learners with intellectual disabilities in South Africa. Sex Disabil. 2018, 36, 123–140. [Google Scholar] [CrossRef]


{kind=link}
| Studies | Q1 | Q2 | Q3 | Q4 | Q5 | Quality Score |
|---|---|---|---|---|---|---|
| Frawley & Bigby (2014) | Y | Y | Y | Y | Y | H |
| Lafferty et al. (2012) | Y | Y | Y | Y | Y | H |
| Löfgren-Mårtenson (2012) | Y | Y | Y | Y | Y | H |
| Louw (2017) | Y | Y | Y | Y | Y | H |
| Nelson et al. (2020) | Y | Y | Y | Y | Y | H |
| Phasha & Runo (2017) | Y | Y | Y | Y | Y | H |
| Schaafsma et al. (2013) | Y | Y | Y | Y | Y | H |
| Swango-Wilson (2009) | Y | CT | CT | N | N | L |
| Wilson & Frawley (2016) | Y | Y | Y | Y | Y | H |
| Studies | Q1 | Q2 | Q3 | Q4 | Q5 | Quality Score |
|---|---|---|---|---|---|---|
| Katoda et al. (1990) | Y | CT | Y | N | CT | M |
| Louw (2014) | Y | N | CT | CT | Y | M |
| Murray (2019) | Y | CT | Y | CT | Y | M |
| Citation and Country | Aim | Design, Content and Delivery | Sample | Methods | Key Findings | Recommendations |
|---|---|---|---|---|---|---|
| Frawley & Bigby (2014) Australia | Identify the experiences of people with intellectual disability (ID) as peer educators in sexuality and relationship education. | Co-produced with people with ID Peer educators | Peer educators (n = 16) | Qualitative: interviews using thematic analysis | People with ID as peer educators acquire new knowledge and skills about relationships and available community resources and supports evident. Sharing their personal insights and experiences as a peer educator resulted in their greater empowerment and confidence. | Participating as a peer educator appears beneficial to individuals. Future work needs to focus on identifying the effectiveness of peer education and the outcomes for programme participants. |
| Katoda et al. (1990) Sweden | Identify the views of school nurses on health education and sexual relationships for young people with ID. | Health education and interpersonal relationships Delivered within regular curriculum | School nurses (n = 600) | Quantitative: questionnaire using descriptive statistical analysis | Swedish school nurses (47%) were more involved in delivering the programme compared to 1% of Japanese nurses. Nurses identified by parents as most appropriate to deliver sex education followed by teachers. Only 2% of nurse participants thought that nurses should have a lead role due to their limited knowledge of ID issues. 70% of Swedish participants thought nurses required education on ID compared to 91% of Japanese who stated they did not. Swedish nurses provided education on sex and interpersonal relationships, food and exercise and ‘our body.’ | Sex and relationship education should be fully integrated with the school curriculum and delivered collaboratively by parents, teachers and school nurses. Specific teaching materials need to be developed with guidelines for parents, teachers and school nurses regarding their use. |
| Lafferty et al. (2012) UK | Identify the barriers to the delivery of relationship and sexuality education (RSE) for people with ID. | Interactive CD-ROM Sex, sexuality and relationships | Family carers, professionals and front-line staff (n = 100) | Qualitative: interviews and focus groups using thematic analysis | Main programme content related to the protection of vulnerable young people with ID and the lack of appropriate training, poor education resources and ‘cultural prohibitions.’ The barriers need to be identified, discussed and adequately addressed to improve RSE programmes’ content and delivery. | Training and information about RSE programmes are required. Risk management procedures need to be in place. RSE programmes should be available to support the empowerment of young people with ID. |
| Lofgren-Martenson (2012) Sweden | Explore the experiences of sex education programmes in young people with ID. | RSE education framework didactic delivery in gender segregated groups Content more focused on sexual risks | Young people with ID (n = 16) | Qualitative: interviews using thematic analysis | Current programmes focus more on sexual risk opposed to sexual pleasure and intimacy. There is a need for RSE education frameworks and teaching models to assist professionals to deliver RSE education programmes relevant to the needs of young people with ID. | Future studies should include young people with ID. There needs to be collaborators in the research to address different gender perspectives and co-create sex education programmes. Future studies should focus on learning strategies to reduce sexual risk behaviours and promote affirmative attitudes towards the expression of sexuality. |
| Louw at al. (2014) South Africa | Identify the views of teachers and childcare providers regarding sexuality, HIV and AIDS education in special needs schools. | Health education HIV/AIDS and sexuality education Collaborative approach by teachers and health professionals | Special school educators (n = 78) | Quantitative: questionnaire using descriptive and inferential statistical analysis | Teachers had high level of knowledge regarding the topic area and teaching sexuality education. However, some teachers questioned if they should be responsible for delivering RSE programmes. The personal attitudes and beliefs of teachers has the potential to influence teaching practice. | Policy research required on the impact and outcomes of RSE programmes. A proactive collaborative approach is needed to support RSE programme design and delivery. Tailored RSE materials are required for people with ID. Participatory action research is needed involving all key stakeholders, including young people with ID and their parents to identify the effectiveness of programmes. |
| Louw (2017) South Africa | Identify the experiences of teachers and school staff when delivering RSE programmes in special needs schools. | Sex education manuals Visual materials re sex and relationships School staff and parental involvement | Teachers (n = 68) School staff (n = 10) | Qualitative: questionnaire using thematic analysis | Students with ID have a fundamental right to receive RSE education relevant to their needs. Appropriate RSE curriculum is required and adequate support available to enable young people with ID to meaningfully engage and participate in RSE programmes. | Need up-to-date, evidence-based RSE programmes that are developed by experts in the field. This may address the possibility of teachers imposing their own values and beliefs. Parents need to be supportive of their children’s involvement in structured RSE programmes. |
| Murray (2019) Canada | Develop, deliver and evaluate a sex education programme for young people with ID. | Community development approach Sexuality, sexual relationships and intimacy Interactive approaches to learning | Young people with mild ID (n = 93) | Quantitative: questionnaire using descriptive statistical analysis | Reinforce the need for sexual health education for young people with ID and increase opportunities to develop healthy sexual relationships and intimacy. RSE programmes need to promote positive sexual identities and decrease risk of sexual harm. | Future research could utilise focus groups to more fully understand the perceptions of young people with ID regarding the education sessions. The benefits of a peer-to-peer model of education delivery needs to be researched. |
| Nelson et al. (2020) Sweden | Explore the experiences of teaching sexual and reproductive health to students with ID. | Sexual health and reproduction education Various teachers | Teachers (n = 10) | Qualitative: interviews and phenomenological analysis | Teachers are the main source of information for students. Teachers need to adapt content to student needs. Teachers lack knowledge and confidence regarding religion and cultural aspects and lack skills in sexual health issues. | Teachers need access to specific materials and resources. Teacher training programmes must address issues related to culture and different religious ideologies. An evaluation of learning outcomes needs to be undertaken. |
| Phasha & Runo (2017) South Africa | Identify the sexuality education needs of learners with intellectual disabilities in schools in Kenya. | Erratic and ineffective sexuality education. Mainly risky behaviours School, friends and mothers | Students with mild ID (n = 56) | Qualitative: interviews and focus groups using thematic analysis | Sex education is patchy with no formalised RSE programmes, resulting in a lack in ability to make informed decision regarding sex issues. RSE programmes need to educate regarding avoiding risky or dangerous situations. Content should be well structured to empower young people with ID and include anatomy, health, personal hygiene, reproduction and expressions of love. RSE programmes should begin at an early age. | Teachers require additional training regarding sexuality issues. Future research needs to address topics such as community attitudes towards young people with ID and their sexual and human rights, the benefits of training programmes for teachers, and evaluation of programmes undertaken. |
| Schaafsma et al. (2013) Netherlands | Explore the development of sex education programmes for people with ID. | Various teaching and learning methods adopted. Knowledge, teaching skills, tailoring, empowerment and enjoying sexuality. | Programme developers (n = 11) | Qualitative: interviews using content analysis | RSE programmes currently lack theoretical models and specific outcomes, and there is a need for systematic evaluations to identify behaviour change. RSE programmes need to include young people with ID in the development. | Future sex education programmes need to be developed using systematic theories, models and evidence-based approaches and be fully evaluated to identify their impact and outcomes. |
| Swango-Wilson (2009) USA | Identify the expectations and the development of a sex education programme. | Current materials too broad and overwhelming. Relationship development and skills for responsible sexual activity. | People with ID (n = 3), parents (n = 3), professionals (n = 6) | Qualitative: interviews using thematic analysis | Regarding RSE programme content, parents expressed fear and denial regarding the expression of sexuality. Young people with ID identified relationships and knowledge. ID professionals identified safety and legal issues. Health professionals identified health issues and concerns. Across the groups, all identified the need to involve care givers to enable them to support social, situational learning opportunities. | Evidence-based programmes need to be developed involving people with ID at all stages. Professionals need to build upon their experience of working with young people with ID. Further research is required to identify whether sex education programmes decrease the risk of sexual abuse and exploitation. Rigorous RSE programme evaluations are needed to identify effectiveness and outcomes. |
| Wilson & Frawley (2016) Australia | Identify the support offered to young people with intellectual and developmental disability (IDD). | Transition to work staff (TTW) to include sexuality and relationship information in programmes. | Support staff (n = 17) | Qualitative: focus groups using thematic analysis | Some support workers felt perceived as ‘reluctant counsellors’. Participants felt poorly prepared to deliver and discuss sex education and sexuality issues and relied on their own attitudes and values to guide their practice. Possibility of ‘blurred’ lines between education and social support role. | Further research is needed regarding policy and practice development to inform RSE programme design, delivery and evaluation to identify effectiveness and outcomes. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brown, M.; McCann, E.; Truesdale, M.; Linden, M.; Marsh, L. The Design, Content and Delivery of Relationship and Sexuality Education Programmes for People with Intellectual Disabilities: A Systematic Review of the International Evidence. Int. J. Environ. Res. Public Health 2020, 17, 7568. https://doi.org/10.3390/ijerph17207568
Brown M, McCann E, Truesdale M, Linden M, Marsh L. The Design, Content and Delivery of Relationship and Sexuality Education Programmes for People with Intellectual Disabilities: A Systematic Review of the International Evidence. International Journal of Environmental Research and Public Health. 2020; 17(20):7568. https://doi.org/10.3390/ijerph17207568
Chicago/Turabian StyleBrown, Michael, Edward McCann, Maria Truesdale, Mark Linden, and Lynne Marsh. 2020. "The Design, Content and Delivery of Relationship and Sexuality Education Programmes for People with Intellectual Disabilities: A Systematic Review of the International Evidence" International Journal of Environmental Research and Public Health 17, no. 20: 7568. https://doi.org/10.3390/ijerph17207568