1. Introduction
Gestational diabetes mellitus (GDM) is characterized by hyperglycemia diagnosed for the first time during pregnancy, and it is usually detected by routine testing during pregnancy, generally between 24 and 28 weeks [
1]. GDM is one of the most common complications during pregnancy, with an estimated prevalence of 5.8–12.9% globally [
2]. In China, GDM ranks first among maternal complications, with a prevalence is 14.8–23.0%, which has increased rapidly in recent decades [
3,
4]. GDM is associated with a higher incidence of fetal and maternal morbidity. In addition to the increased incidence of perinatal conditions, such as perinatal mortality, macrosomia, and preeclampsia [
5], women with a history of GDM are at higher risks of subsequently developing type 2 diabetes mellitus (T2DM) [
2,
6]. Increasing lines of evidence suggest that nutrition therapy plays an important role in blood glucose management and preventing T2DM in women with prior GDM [
7]. In particular, consuming a diet based on low-glycemic index (GI) foods results in better glycemic control than following conventional healthy dietary recommendations [
8,
9]. A meta-analysis conducted in 2019 that included 29 studies compared different dietary strategies for glycemic control among Chinese women with GDM [
10]. Six of them compared a low-GI diet with standard dietary interventions and found that low-GI diets were associated with improved glycemic control. GI-based approaches have been proven to help improve the carbohydrate and overall diet quality, self-care practices, and metabolic outcomes among diabetes patients [
11,
12]. Thus, Chinese women with prior GDM may benefit from a diet emphasizing low-GI foods.
A few studies focused on pregnant women have identified a poor understanding of GDM [
13]. A qualitative exploratory study assessed the awareness of GDM among rural Chinese women, and the authors reported a serious lack of knowledge, low level of risk awareness, and poor self-care behavior among the study group [
14]. Few studies focused on the concept of the GI have been conducted on postpartum rural Chinese women with a history of GDM. Thus, for this population, there are no relevant documented data on awareness of the GI or on the use of a low-GI diet.
As mentioned above, dietary choice is crucial for preventing T2DM in women with prior GDM. Thus, it is important to analyze the factors related to the behavior of the target population. Health behavior theories such as the theory of planned behavior (TPB) provide a framework for understanding human behavior [
15]. According to the TPB, three constructs influence intentions (INT): attitudes toward the behavior (ATT), subjective norms regarding the behavior (SN), and perceived behavior control (PBC); these intentions then influence actions [
16]. The TPB is widely used to explain the associations between intentions to eat a between healthy diet and adherence behavior [
17,
18]. Eades and colleagues conducted a study using semi-structured interviews according to the TPB [
19]. Their finding revealed that changing the diet was the first choice related to lifestyle changes during and after pregnancy among women with GDM; this practice was most commonly motivated by instrumental attitude, such as concern for the fetus and the desire to avoid taking medication to treat GDM. In addition, women who lived outside the main towns (i.e., with less PBC) reported less motivation for maintaining healthy practices (i.e., blood testing) postnatally. In summary, the TPB is suitable for explaining health-related behaviors among women with GDM.
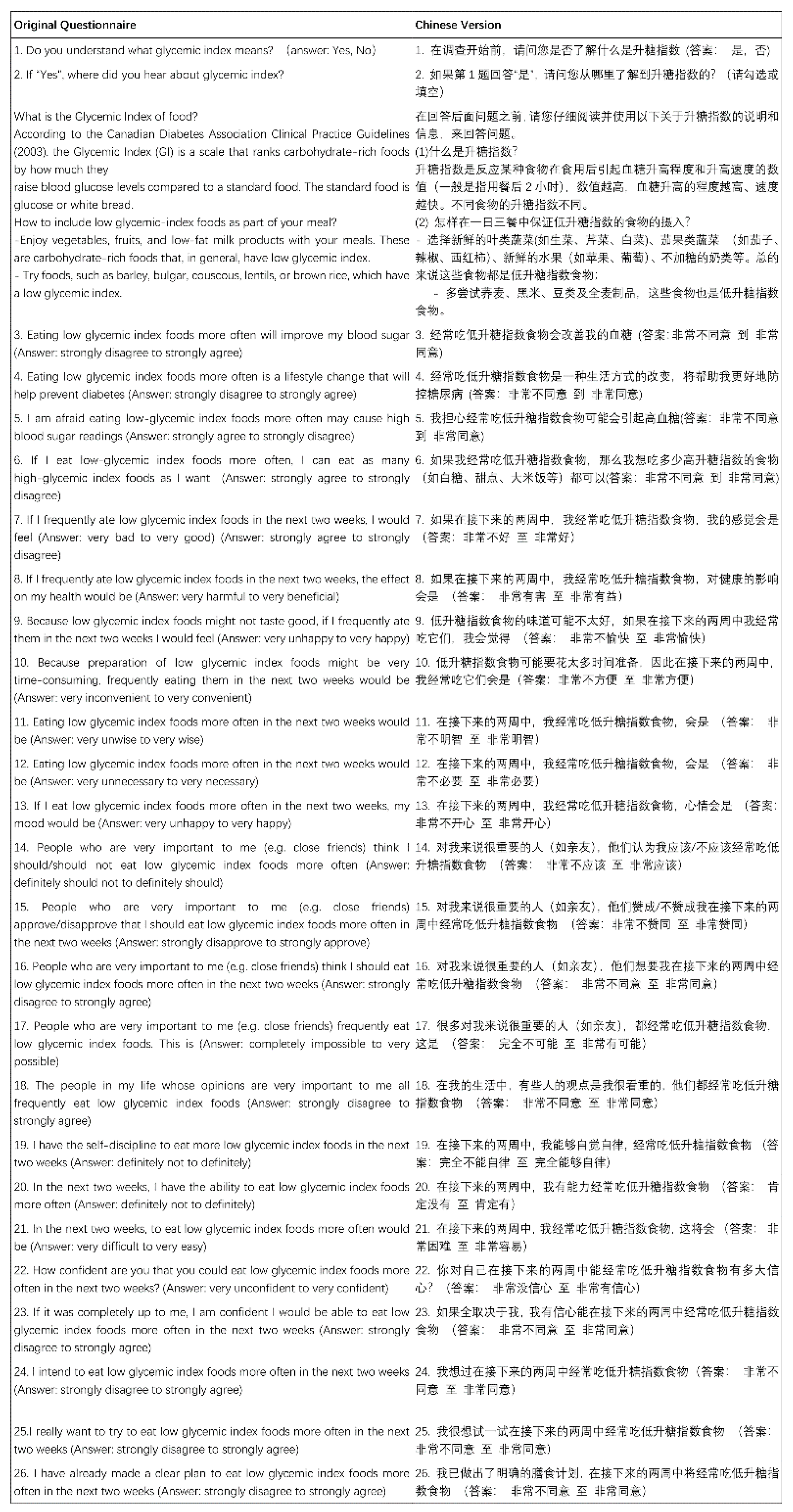
Under the framework of the TPB, Watanabe and colleagues developed a tool to assess intentions to eat low-GI foods (IELQ) in adults with diabetes in Canada [
20]. This questionnaire evaluated seven factors, including knowledge of the GI, instrumental attitude, experiential attitude, subjective norms, descriptive norms, PBC, and behavioral intention. They found that the IELQ had acceptable validity (factor loading range, 0.53–0.96) and reliability (Cronbach alpha range, 0.78–0.93), explaining 62.9% of the total variance in intentions to eat low-GI foods. These results indicate that IELQ is a valid tool for assessing TPB constructs that contribute to the intention to eat a low-GI diet in people with diabetes.
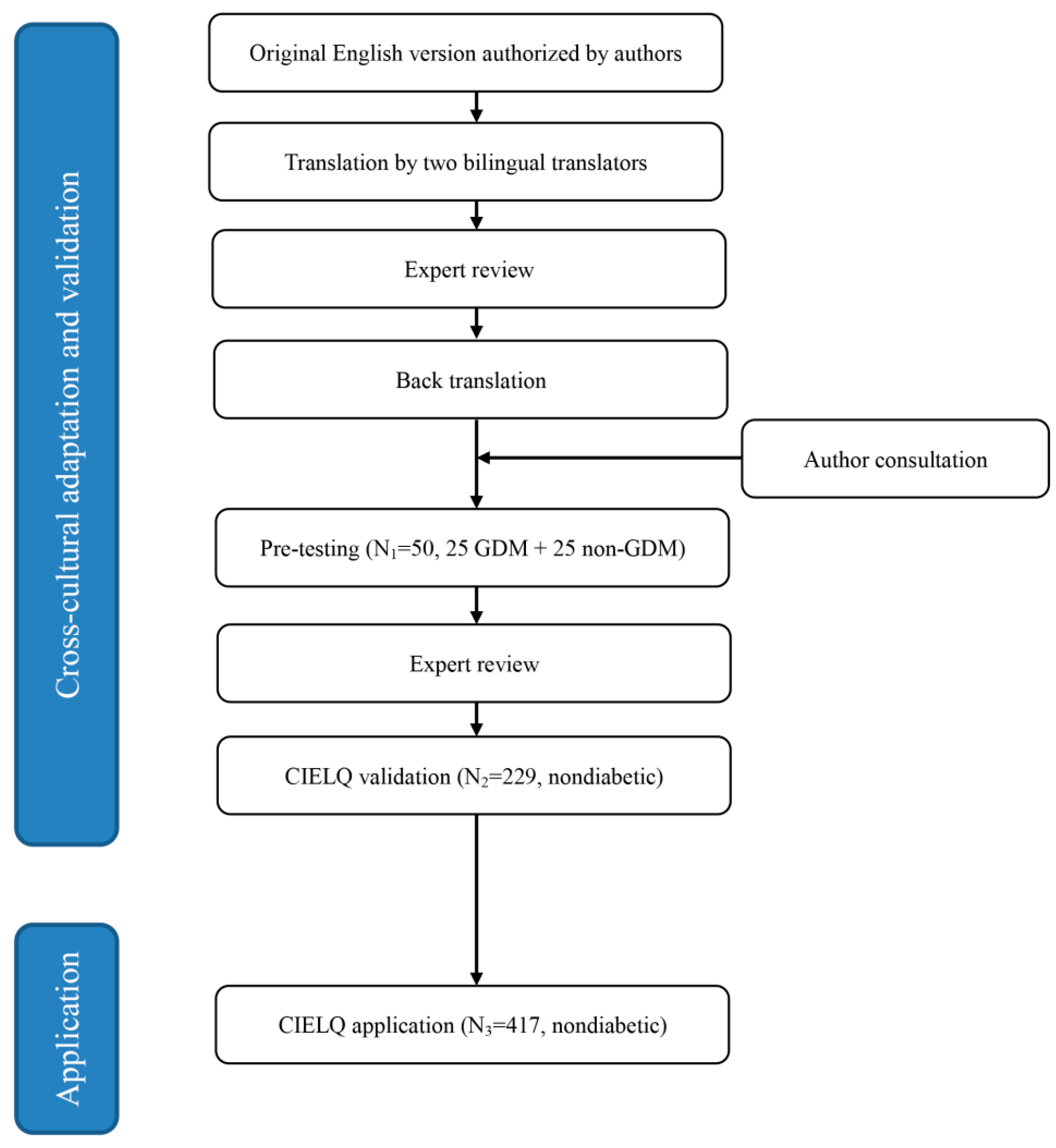
Nevertheless, this instrument was not culturally adapted for use in other countries; nor was a similar tool developed for assessing the intention to eat low-GI foods in rural Chinese women with a prior history of GDM. Because of the importance of intention in actually performing a health-related behavior according to the TPB, it is crucial to determine the intention of eating low-GI foods among a target population and explore the potential influence of this intention. Thus, we conducted this study to (1) adapt the IELQ and validate a Chinese version (CIELQ) to assess the intention to eat low-GI foods among Chinese women with GDM in rural areas and (2) explore the association between the CIELQ results and glycemic status.
4. Discussion
To the best of our knowledge, this was the first study conducted among rural Chinese women to assess their intention to eat low-GI foods. We cross-culturally adapted and validated the questionnaire developed by Watanabe and colleagues [
20], and the Chinese version was found to have a satisfactory fitness. In the primary application of the questionnaire, we found that the score for the TPB factors was associated with education level, diabetes history of family members, awareness of GI, and having had a glycemic test in the last three months. The scores for instrumental attitude and PBC were associated with the glycemic level in the 2h-OGTT.
The prevalence of GDM has increased in China in recent years. It was reported that the adjusted prevalence of gestational diabetes mellitus increased by 2.8 times from 1999 to 2008, from 2.4 to 6.8% [
30]. A meta-analysis that summarized studies conducted after 2000 reported that the total incidence of GDM in mainland China was 14.8% (95% confidence interval 12.8–16.7%) [
3]. Although the blood glucose levels of women with a history of GDM often normalize shortly after delivery, these women eventually have a substantially increased risk of developing T2DM later in life [
31,
32]. Fortunately, systematic postpartum lifestyle interventions can help to prevent the progression of GDM to T2DM [
7]. Shyam and colleagues reported that low-GI diets successfully improved glucose tolerance in women with a previous history of GDM [
8]. After a six month intervention, the women in the conventional healthy dietary recommendations group were found to have a higher blood glucose level on the 2h-OGTT, while the women in the low-GI diet group were found to have a lower blood glucose level on the 2h-OGTT (median (inter-quartile range): −0.2(2.8) vs. +0.8 (2.0) mmol/L,
p = 0.025).
Over the past decades, the TPB has gained popularity and been widely applied for interpreting health-related behaviors, such as smoking, alcohol consumption, and weight reduction [
15]. Watanabe et al. developed a questionnaire to assess intentions to eat low-GI foods (IELQ) in adults with diabetes based on the TPB and reported satisfactory fitness, validity, and reliability [
20]. However, no such tool had been developed for rural Chinese women with a history of GDM. We conducted this study to adapt and validate the IELQ and test its fitness to the TPB in our population with the aim of providing evidence for designing an intervention program for rural Chinese women to prevent the progression of GDM to diabetes.
The culturally adapted CIELQ was found to have satisfactory performance in terms of reliability and validity. The Cronbach’s alpha value for the whole questionnaire was 0.945, and it ranged from 0.724 to 0.901 among the domains, similar to the results for the original questionnaire (0.78 to 0.93) [
20]. Moreover, the ICC in the one week retest indicated good test-retest reliability. The CFA results indicated acceptable fitness of the tool; the CMIN/DF was 2.57, and the CFI was 0.91. By adding the correlation of Q7 and Q8 according to the modification index, the RMSEA value decreased from 0.083 to 0.077. This decrease in the RMSEA value might be explained by the logical correlation between Q7 and Q8. In this case, we hypothesized that people might feel good when eating low-GI foods because they realized that it was beneficial to their health.
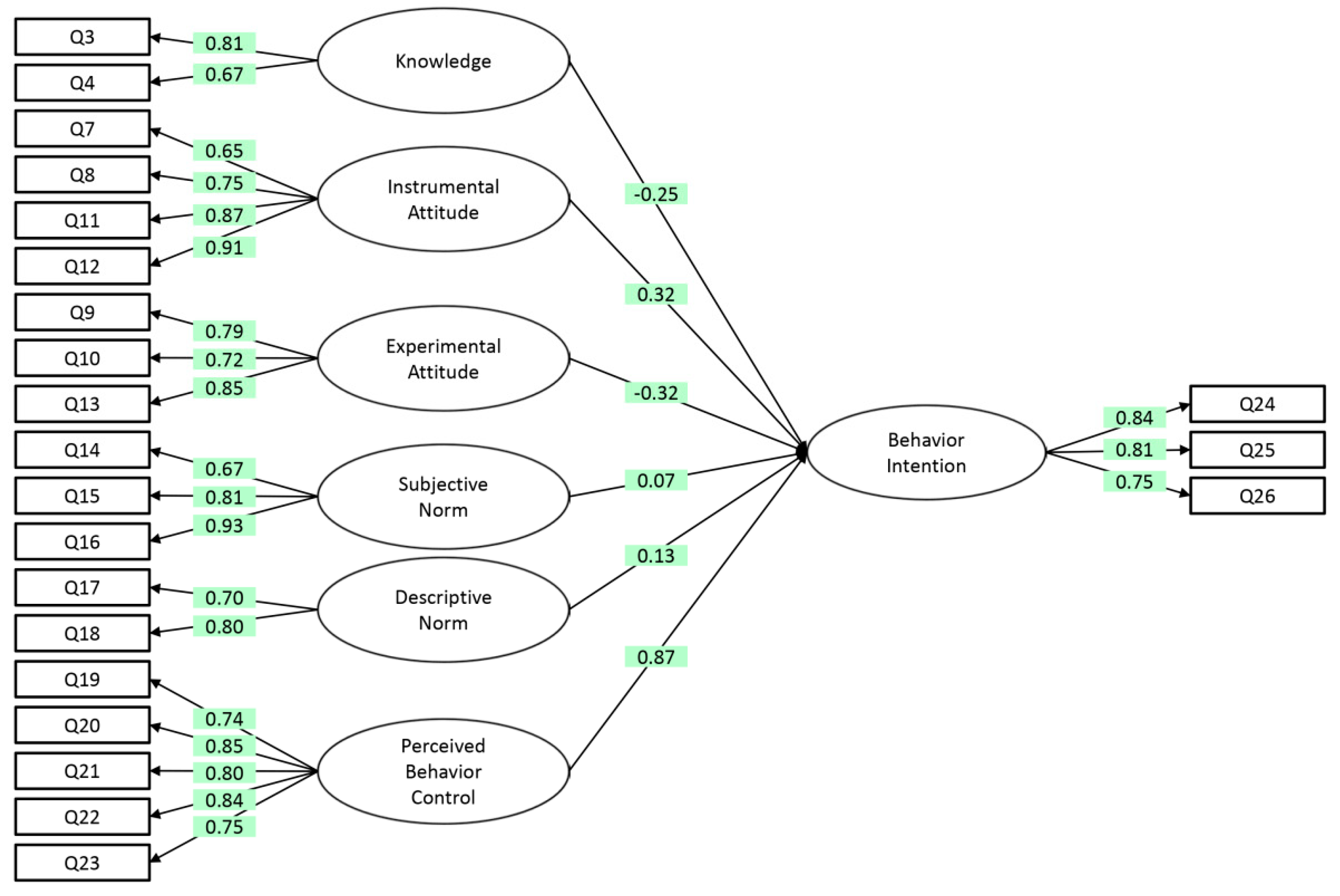
After adapting the CIELQ to the study population, the results indicated that the CIELQ was a valid TPB-based instrument for assessing the intention to eat a low-GI diet among nondiabetic, nonpregnant Chinese women with a history of GDM. As shown in
Figure 2, higher scores for knowledge, instrumental attitude, experimental attitude, subjective norms, and descriptive norms were associated with a higher score for the intention to eat low GI diets (all standardized coefficients of regression >0.6, except for knowledge [0.54]).
These findings are understandable because of the low awareness of the GI in this study population; less than one-fifth of the participants understood the meaning of the GI. Different from the study conducted by Watanabe and colleagues [
20], which included patients with diabetes, we included nondiabetic, nonpregnant women with a history GDM in this study. The awareness of the GI in this study was much lower than the awareness reported for American adults with T2DM (46.7%) and for Canadian women with T2DM (63%) [
33,
34]. In addition, women who reported having knowledge of the GI concept also reported that the most frequent source of GI information was doctors (45 cases, 56.3%). This implied that diabetes education regarding the GI is insufficient among rural Chinese women with a history of GDM. The Obstetrics and Gynecology Branch of the Chinese Medical Association has advocated patient education and the postpartum follow-up of women with GDM [
24], and further studies are needed to determine whether information on the GI should be emphasized during patient education and postpartum follow-up. In addition, education programs to develop awareness of the GI among rural women with a history of GDM are needed to increase the practice of eating a low-GI diet to prevent the potential long-term side effects of GDM.
Although a method using 24 h recalls over three consecutive days was applied to assess the dietary intake of the participants, we failed to calculate the GI for the mixed diet. Instead, we examined the correlation of the score for the Chinese Healthy Eating Index (CHEI) and that for the intention to eat low-GI foods. The CHEI is a valid tool for assessing diet quality in Chinese populations [
35,
36]. The CHEI score reflects dietary food intake by adding the scores for 17 types of food that are divided into two groups. Group one includes total grains, whole grains and mixed beans, tubers, total vegetables, dark vegetables, fruits, dairy, soybeans, fish and seafood, poultry, eggs, seeds, and nuts. Higher scores for group one indicate higher consumption levels of the foods in this group. Group two includes red meat, cooking oils, sodium, added sugars, and alcohol, which are encoded by a reverse method. We found that the CHEI score was marginally positively correlated with the score for intention in the CIELQ (Pearson correlation, r = 0.132,
p = 0.008). Obviously, a high CHEI score indicates a healthy diet; this may serve as a rough estimation of the practice of eating low-GI foods. Admittedly, additional studies are needed to directly assess the association between the intention to eat low-GI foods and actually consuming low-GI foods.
We did not detect any significant association between FPG level and the score for TPB factors in the logistic regression. The
R2 of the regression model was relatively small (0.177), indicating that many covariates that could influence FPG level were ignored, such as gene polymorphisms, diet, physical activity, dietary supplements, and sleep patterns [
37,
38,
39,
40,
41,
42].
Regarding the 2h-OGTT, women with a higher score for instrumental attitude were associated with a higher risk of impaired glucose tolerance (IGT, OR = 1.330,
p = 0.025); women with a higher score for PBC were associated with a lower risk of IGT (OR = 0.793,
p = 0.035). Again, the
R2 of the regression model was relatively small (0.291). Previous studies have shown that behavior can be predicted by intention and PBC [
15]. Moreover, instrumental attitude was positively associated with intention, and intention positively influences action [
43]. The study conducted by Rhodes and colleagues showed that instrumental attitude contributed to perceived importance and concern regarding physical activities; it was significantly different among those with different physical activity engagement levels [
44]. We initially hypothesized that the higher the scores for TPB variables were, the lower the risk of IGT. However, the association between instrumental attitude and risk of IGT in this study was counterintuitive. We suspected that this was due to bias resulting from a low awareness of the GI among the study population. Instrumental attitude refers to an individual’s evaluation of a behavior’s outcome, and is represented by adjective pairs such as valuable-worthless and harmful-beneficial [
45]. To determine whether a behavior is beneficial, knowledge of the behavior and its relevant concepts are indispensable. However, more than 80% of the participants reported that they did not understand the GI. Thus, it was not surprising to find that the association between instrumental attitude and risk of IGT deviated from the anticipated result. PBC, which is defined as an individual’s perception of the ease or difficulty of performing a particular behavior, is an independent predictor of intention [
46]. According to the TPB, intention along with PBC triggers the behavior [
16]. Our findings were consistent with this structure; we hypothesized that women with a higher score for PBC were more willing to eat low-GI foods and benefit from glycemic control and be associated with a lower risk of IGT.
The CIELQ was found to have acceptable reliability and validity among nondiabetic, nonpregnant rural Chinese women with a history of GDM and a promising adaptability for other women of gestational age. However, our study still had several limitations. The awareness of the GI was low; in addition, we failed to assess participants’ knowledge of the GI in depth. As we mentioned above, the level of understanding of the GI could affect the attitude toward eating a low-GI diet and in turn influence other components in the TPB. Nondiabetic, nonpregnant rural Chinese women with a history of GDM were chosen for this study, but further studies in different populations are required before extrapolating the conclusions of this study to other groups. Nearly half of the participants included in this study were members of a minority ethnic group (43.9%); this is vastly different from the general trend for the Chinese population. According to the 2010 population census of China, the percentage of minority females aged 19–45 was 8.3% [
47]. Further studies are needed to test the feasibility of the instrument in populations with a Han majority. Although HbA1c is a widely recognized indicator of the long-term glycemic status, we did not assess it in this study. In China, the HbA1c levels of patients are not widely used as diagnostic criteria because of the lack of standardization of HbA1c testing [
24]. In addition, the inconsistencies in the cut-offs for the HbA1c level prevent distinguishing GDM patients from non-GDM patients. We did not directly collect information on the behavior of following a low-GI diet, such as the frequency that participants ate low-GI foods. In addition, information on some covariates that influence blood glucose levels was not considered. Further studies should include this information to better control for potential bias.
Comprehension of the predictors of the dietary behavior of women with a history of GMD is first needed before developing, implementing, and evaluating an effective nutritional intervention program and policy to prevent the progression of GDM to diabetes. Cultural background and characteristics of the subgroup population affect the reliability and validity of a questionnaire; cross-cultural adaptation and validation of the original questionnaire are essential. In this study, the fitness of TPB constructs to assess the intention to eat a low-GI diet provides a basic framework for health workers focused on women’s health in China to develop an intervention program. In particular, providing education on the concept of the GI needs to be emphasized when developing an intervention program. The association between the risk of IGT and PBC score indicates the importance of targeted learning objectives and program activities to ensure that the PBC of eating a low-GI diet is improved among rural Chinese women with a history of GDM.

 ,
, 



{kind=link}
{kind=link}
{kind=link}
{kind=link}

