Recruitment and Baseline Characteristics of Participants in the “Sanadak” Trial: A Self-Help App for Syrian Refugees with Post-traumatic Stress

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
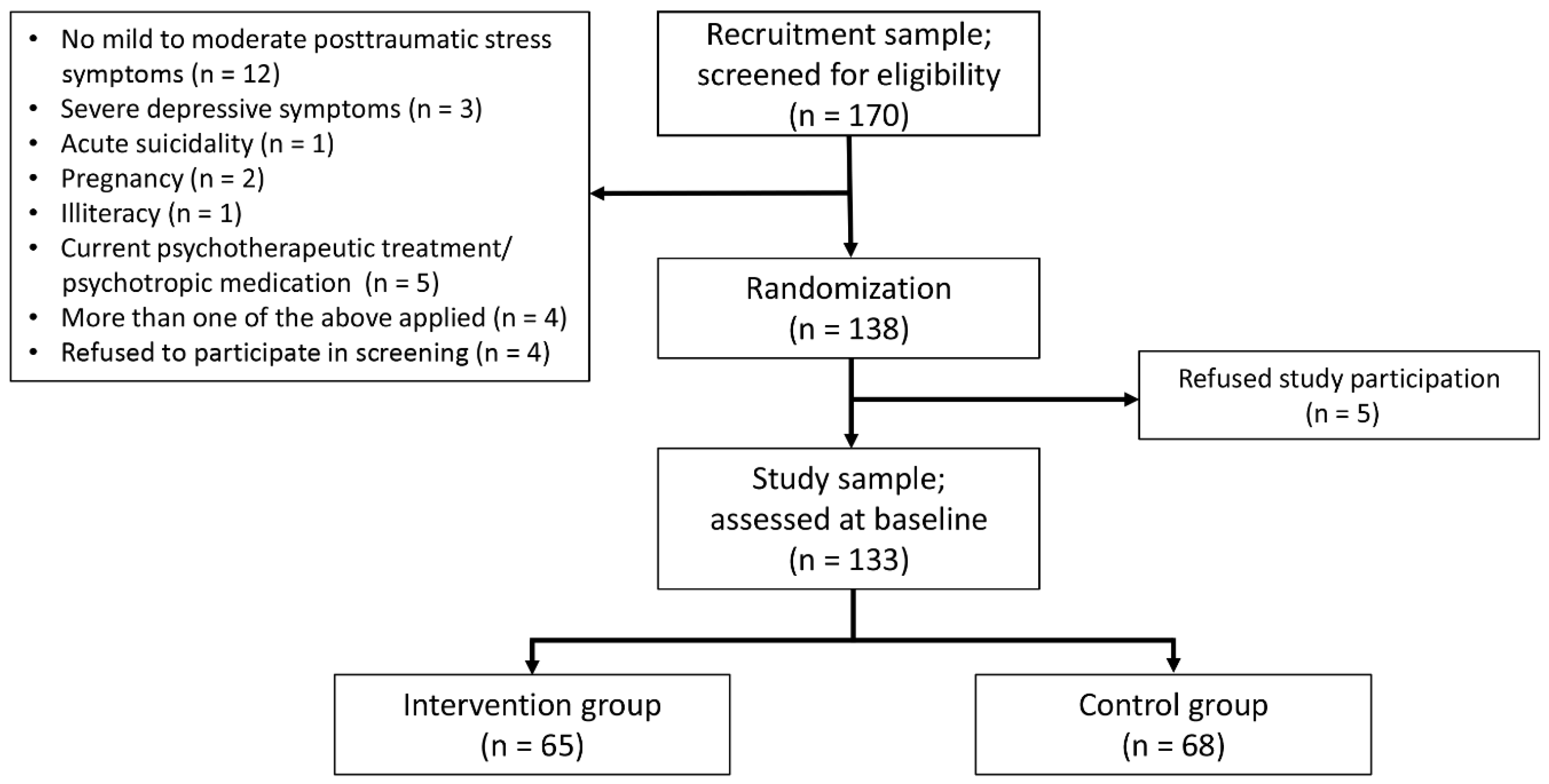
2.1. Recruitment and Recruitment Procedures
2.2. Randomization
2.3. Assessments and Instruments
2.4. Data Entry and Data Quality Control
2.5. Ethics and Registration
2.6. Statistical Analyses
3. Results
3.1. Recruitment Sample Characteristics
3.1.1. Sociodemographic Characteristics of the Recruitment Sample
3.1.2. Escape- and Trauma-Related Characteristics of the Recruitment Sample
3.1.3. Secondary Mental Health Characteristics of the Recruitment Sample
3.2. Study Sample Characteristics
3.2.1. Escape and Trauma-Related Characteristics of the “Sanadak” Study Sample
3.2.2. Secondary Mental Health Characteristics of the “Sanadak” Study Sample
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Mediendienst Integration. Zahlen Und Fakten: Syrische Flüchtlinge. Available online: https://mediendienst-integration.de/migration/flucht-asyl/syrische-fluechtlinge.html (accessed on 30 April 2020).
- Georgiadou, E.; Zbidat, A.; Schmitt, G.M.; Erim, Y. Prevalence of Mental Distress among Syrian Refugees With Residence Permission in Germany: A Registry-Based Study. Front. Psychiatry 2018, 9, 393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fazel, M.; Wheeler, J.; Danesh, J. Prevalence of serious mental disorder in 7000 refugees resettled in western countries: A systematic review. Lancet 2005, 365, 1309–1314. [Google Scholar] [CrossRef]
- PeConga, E.K.; Thøgersen, M.H. Post-traumatic stress disorder, depression, and anxiety in adult Syrian refugees: What do we know? Scand. J. Public Health 2019, 26, 140349481988213. [Google Scholar] [CrossRef] [PubMed]
- Lindert, J.; Brähler, E.; Wittig, U.; Mielck, A.; Priebe, S. Depressivität, Angst und posttraumatische Belastungsstörung bei Arbeitsmigranten, Asylbewerbern und Flüchtlingen. PPmP Psychother. Psychosom. Med. Psychol. 2008, 58, 109–122. [Google Scholar] [CrossRef]
- Li, S.S.Y.; Liddell, B.J.; Nickerson, A. The Relationship between Post-Migration Stress and Psychological Disorders in Refugees and Asylum Seekers. Curr. Psychiatry Rep. 2016, 18, 1–9. [Google Scholar] [CrossRef]
- Association, A.P. (Ed.) Diagnostic and Statistical Manual of Mental Disorders. In Criteria for Post-Traumatic Stress Disorder; American Psychiatric Association: Philadelphia, PA, USA, 2013. [Google Scholar]
- Sierau, S.; Schneider, E.; Nesterko, Y.; Von Klitzing, K.; Glaesmer, H. Psychische Belastung bei unbegleiteten jungen Geflüchteten in Jugendhilfeeinrichtungen. Psychiatr. Prax. 2018, 46, 135–140. [Google Scholar] [CrossRef]
- Winkler, J.; Brandl, E.J.; Bretz, H.J.; Heinz, A.; Schouler-Ocak, M. Psychische Symptombelastung bei Asylsuchenden in Abhängigkeit vom Aufenthaltsstatus. Psychiatr. Prax. 2018, 46, 191–199. [Google Scholar] [CrossRef] [Green Version]
- Wenk-Ansohn, M.; Heeke, C.; Böttche, M.; Stammel, N. Acute short-term multimodal treatment for newly arrived traumatized refugees: Reflections on the practical experience and evaluation. Torture J. 2018, 28, 99–117. [Google Scholar] [CrossRef]
- Nesterko, Y.; Jäckle, D.; Friedrich, M.; Holzapfel, L.; Glaesmer, H. Prevalence of post-traumatic stress disorder, depression and somatisation in recently arrived refugees in Germany: An epidemiological study. Epidemiol. Psychiatr. Sci. 2019, 29, e40. [Google Scholar] [CrossRef] [Green Version]
- Marshall, G.N.; Schell, T.L.; Elliott, M.N.; Berthold, S.M.; Chun, C.-A. Mental Health of Cambodian Refugees 2 Decades after Resettlement in the United States. JAMA 2005, 294, 571–579. [Google Scholar] [CrossRef] [Green Version]
- Golchert, J.; Röhr, S.; Berg, F.; Grochtdreis, T.; Hoffmann, R.; Jung, F.U.; Nagl, M.; Plexnies, A.; Renner, A.; König, H.-H.; et al. HELP@APP: Development and evaluation of a self-help app for traumatized Syrian refugees in Germany–a study protocol of a randomized controlled trial. BMC Psychiatry 2019, 19, 131. [Google Scholar] [CrossRef] [Green Version]
- Röhr, S.; Wittmann, F.; Jung, F.; Hoffmann, R.; Renner, A.; Dams, J.; Grochtdreis, T.; Kersting, A.; König, H.-H.; Riedel-Heller, S.G. Strategien zur Rekrutierung von Geflüchteten für Interventionsstudien: Erkenntnisse aus dem „Sanadak“-Trial. PPmP Psychother. Psychosom. Med. Psychol. 2019, 69, 484–489. [Google Scholar] [CrossRef] [PubMed]
- Foa, E.B.; McLean, C.P.; Zang, Y.; Zhong, J.; Powers, M.B.; Kauffman, B.Y.; Rauch, S.; Porter, K.; Knowles, K. Psychometric properties of the Posttraumatic Diagnostic Scale for DSM–5 (PDS–5). Psychol. Assess. 2016, 28, 1166–1171. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W. The PHQ-9. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Von Glischinski, M.; Teismann, T.; Prinz, S.; Gebauer, J.E.; Hirschfeld, G. Depressive Symptom Inventory Suicidality Subscale: Optimal Cut Points for Clinical and Non-Clinical Samples. Clin. Psychol. Psychother. 2016, 23, 543–549. [Google Scholar] [CrossRef]
- Leppert, K.; Koch, B.; Brähler, E.; Straß, B. Die Resilienzskala (RS)–Überprüfung der Langform RS-25 und einer Kurzform RS-13. Klin. Diagn. Eval. 2008, 1, 226–243. [Google Scholar]
- Huber, S.; Huber, O.W. The Centrality of Religiosity Scale (CRS). Religions 2012, 3, 710–724. [Google Scholar] [CrossRef]
- Brauns, H.; Steinmann, S. Educational Reform in France, West-Germany and the United Kingdom: Updating the CASMIN Educational Classification. Available online: https://nbn-resolving.org/urn:nbn:de:0168-ssoar-208169 (accessed on 30 April 2020).
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.W.; Löwe, B. A Brief Measure for Assessing Generalized Anxiety Disorder. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [Green Version]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W. The PHQ-15: Validity of a New Measure for Evaluating the Severity of Somatic Symptoms. Psychosom. Med. 2002, 64, 258–266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwarzer, R.; Jerusalem, M. Skalen zur Erfassung von Lehrer-und Schülermerkmalen. Dokumentation der psychometrischen Verfahren im Rahmen der Wissenschaftlichen Begleitung des Modellversuchs Selbstwirksame Schulen; Freie Universität Berlin: Berlin, Germany, 1999. [Google Scholar]
- Corrigan, P.W.; Michaels, P.J.; Vega, E.; Gause, M.; Watson, A.C.; Rüsch, N. Self-stigma of mental illness scale—Short form: Reliability and validity. Psychiatry Res. 2012, 199, 65–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lubben, J.E. Assessing social networks among elderly populations. Fam. Community Health 1988, 11, 42–52. [Google Scholar] [CrossRef]
- Kendel, F.; Spaderna, H.; Sieverding, M.; Dunkel, A.; Lehmkuhl, E.; Hetzer, R.; Regitz-Zagrosek, V. Eine deutsche Adaptation des ENRICHD Social Support Inventory (ESSI). Diagnostica 2011, 57, 99–106. [Google Scholar] [CrossRef] [Green Version]
- EuroQol Group EuroQol—A new facility for the measurement of health-related quality of life. Health Policy 1990, 16, 199–208. [CrossRef]
- Kocalevent, R.-D.; Hinz, A.; Braehler, E. Standardization of a screening instrument (PHQ-15) for somatization syndromes in the general population. BMC Psychiatry 2013, 13, 91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Federal Office for Migration and Refugees. The Stages of the German Asylum Procedure: An Overview of the Individual Procedural Steps and the Legal Basis. Available online: https://www.bamf.de/SharedDocs/Anlagen/EN/AsylFluechtlingsschutz/Asylverfahren/das-deutsche-asylverfahren.pdf?__blob=publicationFile&v=12 (accessed on 30 April 2020).
- Leiler, A.; Bjärtå, A.; Ekdahl, J.; Wasteson, E. Mental health and quality of life among asylum seekers and refugees living in refugee housing facilities in Sweden. Soc. Psychiatry Psychiatr. Epidemiol. 2018, 54, 543–551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Euteneuer, F.; Schäfer, S.J. Brief Report: Subjective Social Mobility and Depressive Symptoms in Syrian Refugees to Germany. J. Immigr. Minor. Health 2018, 20, 1533–1536. [Google Scholar] [CrossRef]
- Krysinska, K.; Lester, D. Post-Traumatic Stress Disorder and Suicide Risk: A Systematic Review. Arch. Suicide Res. 2010, 14, 1–23. [Google Scholar] [CrossRef] [PubMed]
- Amin, M.R.; Helgesson, M.; Runeson, B.; Tinghög, P.; Mehlum, L.; Qin, P.; Holmes, E.A.; Mittendorfer-Rutz, E. Suicide attempt and suicide in refugees in Sweden—A nationwide population-based cohort study. Psychol. Med. 2019, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Björkenstam, E.; Helgesson, M.; Amin, M.R.; Mittendorfer-Rutz, E. Mental disorders, suicide attempt and suicide: Differences in the association in refugees compared with Swedish-born individuals. Br. J. Psychiatry 2019, 352, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Henriksson, M.M.; Aro, H.M.; Marttunen, M.J.; E Heikkinen, M.; Isometsä, E.T.; I Kuoppasalmi, K.; Lönnqvist, J.K. Mental disorders and comorbidity in suicide. Am. J. Psychiatry 1993, 150, 935–940. [Google Scholar] [CrossRef]
- Scholz, U.; Doña, B.G.; Sud, S.; Schwarzer, R. Is General Self-Efficacy a Universal Construct? Eur. J. Psychol. Assess. 2002, 18, 242–251. [Google Scholar] [CrossRef]
- Gottvall, M.; Vaez, M.; Saboonchi, F. Social support attenuates the link between torture exposure and post-traumatic stress disorder among male and female Syrian refugees in Sweden. BMC Int. Health Hum. Rights 2019, 19, 1–11. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | Recruitment Sample | Randomized 1 | Non-Randomized 1 | p-Value |
|---|---|---|---|---|
| (n = 170) | (n = 133) | (n = 32) | ||
| Age (M, SD) | Ø 32.8 (11.2) | Ø 33.3 (11.2) | Ø 30.4 (11.8) | 0.19 |
| Gender | ||||
| Male | 104 (61.2%) | 82 (61.6%) | 19 (59.4%) | |
| Female | 66 (38.8%) | 51 (38.3%) | 13 (40.6%) | 0.812 |
| Net personal income (monthly) | ||||
| <500 € | 35 (20.6%) | 26 (19.5%) | 8 (25.0%) | |
| 500–999 € | 90 (52.9%) | 70 (52.6%) | 19 (59.4%) | |
| 1000–1499 € | 20 (11.8%) | 15 (11.3%) | 5 (15.6%) | |
| 1500–1999 € | 12 (7.1%) | 10 (7.5%) | 0 | |
| 2000–2499 € | 6 (3.5%) | 6 (4.5%) | 0 | |
| 2500–2999 € | 2 (1.2%) | 2 (1.5%) | 0 | |
| not specified | 5 (2.9%) | 4 (3.0%) | 0 | 0.392 |
| Education (school based) | ||||
| <12 years | 53 (31.2%) | 37 (27.8%) | 11 (35.5%) | |
| ≥12 years | 113 (66.5%) | 94 (70.7%) | 19 (61.3%) | |
| not specified | 4 (2.3%) | 2 (1.5%) | 2 (6.2%) | 0.54 |
| Educational level (CASMIN) | ||||
| Low | 34 (24.3%) | 25 (22.9%) | 7 (26.9%) | |
| Middle | 58 (41.4%) | 44 (40.4%) | 14 (53.8%) | |
| High | 48 (34.3%) | 40 (36.7%) | 5 (19.2%) | 0.229 |
| Work permit | ||||
| Yes | 151 (88.8%) | 117 (88.0%) | 29 (90.6%) | |
| No | 12 (7.1%) | 11 (8.3%) | 1 (3.1%) | |
| Not specified | 10 (5.9%) | 5 (3.7%) | 2 (6.2%) | 0.512 |
| Status of employment 2 | ||||
| Not employed | 117 (68.8%) | 90 (67.7%) | 24 (75.0%) | |
| Marginally employed | 24 (14.1%) | 20 (15.0%) | 4 (12.5%) | |
| Part-time employment | 15 (8.8 %) | 13 (9.8%) | 2 (6.2%) | |
| Full-time employment | 12 (7.1%) | 8 (6.0%) | 2 (6.2%) | |
| Not specified | 2 (1.2%) | 2 (1.5%) | / | 0.886 |
| Status of unemployment 2 | ||||
| Integration program | 7 (5.7%) | 6 (6.2%) | 1 (4.3%) | |
| Federal Voluntary Service | 5 (4.1%) | 4 (4.1%) | 1 (4.3%) | |
| Apprentice | 4 (3.2%) | 4 (4.1%) | / | |
| Labour market (re-)training | 1 (0.8%) | 1 (1.0%) | / | |
| Language course | 16 (13.0%) | 11 (11.3%) | 5 (21.7%) | |
| Solely housekeeping | 14 (11.4%) | 13 (13.4%) | 1 (4.3%) | |
| Student | 43 (35.0%) | 33 (34.0%) | 8 (34.8%) | |
| Registered as unemployed | 27 (22.0%) | 23 (23.7%) | 4 (17.4%) | |
| Not specified | 6 (4.9%) | 2 (2.1%) | 3 (13.0%) | 0.278 |
| Living situation | ||||
| Alone | 38 (22.3%) | 33 (24.8%) | 4 (12.5%) | |
| With family/relatives | 98 (57.6%) | 73 (54.9%) | 22 (68.7%) | |
| With other people (private home) | 31 (18.2%) | 25 (18.8%) | 5 (15.6%) | |
| Communal accommodation | 3 (1.8%) | 2 (1.5%) | 1 (3.1%) | 0.373 |
| Family status | ||||
| Single | 83 (48.8%) | 69 (51.9%) | 11 (34.4%) | |
| Married | 69 (40.6%) | 51 (38.3%) | 16 (50.0%) | |
| Divorced | 10 (5.9%) | 7 (5.3%) | 3 (9.4%) | |
| Widowed | 3 (1.8%) | 3 (2.3%) | 0 | |
| Not specified | 5 (2.9%) | 3 (2.3%) | 2 (6.2%) | 0.259 |
| Residence Status 3 | ||||
| Asylum applicant | 21 (12.3%) | 15 (11.3%) | 4 (12.5%) | |
| Residence permit: | ||||
| Refugee status | 74 (43.5%) | 63 (47.4%) | 10 (31.2%) | |
| Subsidiary protection | 14 (8.2%) | 11 (8.3%) | 3 (9.4%) | |
| Humanitarian protection | 40 (23.5%) | 27 (20.3%) | 12 (37.5%) | |
| Not specified | 21 (12.3%) | 17 (12.8%) | 3 (9.4%) | 0.408 |
| Variables | Recruitment Sample (n = 170) | Randomized 1 (n = 133) | Non-Randomized 1 (n = 32) | p-Value |
|---|---|---|---|---|
| Escape route 2 | ||||
| By airplane | 76 (44.7%) | 59 (44.4%) | 15 (46.9%) | |
| Via land | 113 (66.5%) | 86 (64.7%) | 24 (75.0%) | |
| Via sea | 99 (58.2%) | 76 (57.1%) | 20 (62.5%) | |
| Via transit country | 31 (18.2%) | 23 (17.3%) | 7 (21.9%) | 0.985 |
| Time since Syria was left (month) | Ø 49.8 (18.7) | Ø 50.4 (19.3) | Ø 47.2 (16.9) | 0.39 |
| Time spent in Germany (month) | Ø 41.0 (13.3) | Ø 41.2 (13.9) | Ø 38.9 (10.8) | 0.383 |
| Traumatic event (PDS-5) | ||||
| Serious, life-threatening illness | 7 (4.1%) | 5 (3.8%) | 2 (6.2%) | |
| Physical assault | 11 (6.5%) | 9 (6.8%) | 1 (3.1%) | |
| Sexual assault | 2 (1.2%) | 0 | 2 (6.2%) | |
| Military/combat-related | 56 (32.9%) | 47 (35.3%) | 7 (21.9%) | |
| Child abuse | 3 (1.8%) | 3 (2.3%) | 0 | |
| Accident | 4 (2.3%) | 3 (2.3%) | 1 (3.1%) | |
| Torture/Imprisonment | 14 (8.2%) | 10 (7.5%) | 4 (12.5%) | |
| Other 3 | 66 (38.8%) | 54 (40.6%) | 11 (34.4%) | |
| Not further specified | 7 (4.1%) | 2 (1.5%) | 4 (12.5%) | 0.007, V = 0.357 |
| Posttraumatic stress symptoms (PDS-5) 2 | Ø 23.6 (13.2) | Ø 24.4 (11.1) | Ø 20.3 (20.5) 1 | 0.141 |
| Intrusion | 5.5 (4.1) | 5.6 (3.8) | 4.5 (5.1) | 0.177 |
| Avoidance | 2.6 (2.2) | 2.6 (2.2) | 2.6 (2.4) | 0.883 |
| Change in Cognition & Mood | 8.5 (5.9) | 8.7 (5.4) | 7.4 (8.1) | 0.297 |
| Arousal & Hyperactivity | 7.1 (4.4) | 7.4 (3.8) | 6.0 (6.5) | 0.11 |
| Variables | Recruitment Sample | Randomized 1 (n = 133) | Non-Randomized 1 (n = 32) | p-Value |
|---|---|---|---|---|
| (n = 170) | ||||
| Depressive symptoms (PHQ-9) | Ø 9.4 (5.8) | Ø 9.4 (5.1) | Ø 9.5 (8.2) | 0.956 |
| No/low symptom severity (<10) | 91 (53.5%) | 70 (52.6%) | 19 (59.4%) | |
| Clinical significant severity(≥10) | 79 (46.5%) | 63 (47.4%) | 13 (40.6%) | 0.492 |
| Resilience (RS-13) | Ø 64.3 (12.7) | Ø 64.4 (11.4) | Ø 63.1 (17.0) | 0.615 |
| Low (13–66) | 88 (51.8%) | 70 (52.6%) | 16 (50.0%) | |
| Middle (67–72) | 32 (18.8%) | 25 (18.8%) | 6 (18.7%) | |
| High (73–91) | 50 (29.4%) | 38 (28.6%) | 10 (31.2%) | 0.952 |
| Suicidal risk (DSI-SS) | Ø 0.4 (1.3) | Ø 0.2 (1.0) | Ø 1.0 (2.1) | 0.002, |
| d = −0.623 | ||||
| No suicidal risk (<3) | 160 (94.1%) | 128 (96.2%) | 26 (81.2%) | 0.002, |
| Elevated suicidal risk (≥3) | 10 (5.9%) | 5 (3.8%) | 6 (18.7%) | V = 0.238 |
| Variables | Study Sample | Intervention Group (n = 65) | Control Group (n = 68) | p-Value |
|---|---|---|---|---|
| (n = 133) | ||||
| Age (M, SD) | Ø 33.3 (11.2) | Ø 33.0 (11.0) | Ø 33.7 (11.4) | 0.723 |
| Gender | ||||
| Male | 82 (61.6%) | 43 (66.2%) | 39 (57.4%) | |
| Female | 51 (38.3%) | 22 (33.8%) | 29 (42.6%) | 0.297 |
| Net personal income | ||||
| <500 € | 26 (19.5%) | 13 (20.0%) | 13 (19.1%) | |
| 500–999 € | 70 (52.6%) | 32 (49.2%) | 38 (55.9%) | |
| 1000–1499 € | 15 (11.3%) | 7 (10.8%) | 8 (11.8%) | |
| 1500–1999 € | 10 (7.5%) | 6 (9.2%) | 4 (5.9%) | |
| 2000–2499 € | 6 (4.5%) | 5 (7.7%) | 1 (1.5%) | |
| 2500–2999 € | 2 (1.5%) | 0 | 2 (2.9%) | |
| not specified | 4 (3.0%) | 2 (3.1%) | 2 (2.9%) | 0.472 |
| Education (school-based) | ||||
| <12 years | 37 (27.8%) | 16 (24.6%) | 21 (30.9%) | |
| ≥12 years | 94 (70.7%) | 47 (72.3%) | 47 (69.1%) | |
| No school visit | 2 (1.5%) | 2 (3.1%) | 0 | 0.271 |
| Educational level (CASMIN) | ||||
| Low | 25 (22.9%) | 12 (24.0%) | 13 (22.0%) | |
| Middle | 44 (40.4%) | 18 (36.0%) | 26 (44.1%) | |
| High | 40 (36.7%) | 20 (40.0%) | 20 (33.9%) | 0.685 |
| Work permit | ||||
| Yes | 117 (88.0%) | 57 (87.7%) | 60 (88.2%) | |
| No | 11 (8.3%) | 6 (9.2%) | 5 (7.3%) | |
| Not specified | 5 (3.7%) | 2 (3.1%) | 3 (4.4%) | 0.933 |
| Status of employment 1 | ||||
| Not employed | 90 (67.7%) | 40 (61.5%) | 50 (73.5%) | |
| Marginally employed | 20 (15.0%) | 10 (15.4%) | 10 (14.7%) | |
| Part-time employment | 13 (9.8%) | 6 (9.2%) | 7 (10.3%) | |
| Full-time employment | 8 (6.0%) | 8 (12.3%) | / | |
| Not specified | 2 (1.5%) | 1 (1.5%) | 1 (1.5%) | 0.058 |
| Status of unemployment 1 | ||||
| Integration program | 6 (6.2%) | 2 (4.8%) | 4 (7.1%) | |
| Federal Voluntary Service | 4 (4.1%) | 1 (2.4%) | 3 (5.4%) | |
| Apprentice | 4 (4.1%) | 3 (7.1%) | 1 (1.8%) | |
| Labour market (re-)training | 1 (1.0%) | / | 1 (1.8%) | |
| Language course | 11 (11.3%) | 7 (16.7%) | 4 (7.1%) | |
| Solely housekeeping | 13 (13.4%) | 6 (14.3%) | 7 (12.5%) | |
| Student | 33 (34.0%) | 12 (28.6%) | 21 (37.5%) | |
| Registered as unemployed | 23 (23.7%) | 8 (19.0%) | 15 (26.8%) | |
| Not specified | 3 (3.1%) | 3 (7.1%) | / | 0.322 |
| Living situation | ||||
| Alone | 33 (24.8%) | 18 (27.7%) | 15 (22.1%) | |
| With family/relatives | 73 (54.9%) | 35 (53.8%) | 38 (55.9%) | |
| With other people (private home) | 25 (18.8%) | 12 (18.5%) | 13 (19.1%) | |
| Communal accommodation | 2 (1.5%) | 0 | 2 (2.9%) | 0.718 |
| Family status | ||||
| Single | 69 (51.9%) | 37 (56.9%) | 32 (47.1%) | |
| Married | 51 (38.3%) | 21 (32.3%) | 30 (44.1%) | |
| Divorced | 7 (5.3%) | 4 (6.1%) | 3 (4.4%) | |
| Widowed | 3 (2.3%) | 2 (3.1%) | 1 (1.5%) | |
| Not specified | 3 (2.3%) | 1 (1.5%) | 2 (2.9%) | 0.61 |
| Residence status 2 | ||||
| Asylum applicant | 15 (11.3%) | 7 (10.8) | 8 (11.8%) | |
| Residence permit | ||||
| Refugee status | 63 (47.4%) | 31 (47.7%) | 32 (47.0%) | |
| Subsidiary protection | 11 (8.3%) | 5 (7.7%) | 6 (8.8%) | |
| Humanitarian protection | 27 (20.3%) | 12 (18.5%) | 15 (22.1%) | |
| Not specified | 17 (12.8%) | 10 (15.4%) | 7 (10.3%) | 0.945 |
| Religion and religiosity | ||||
| Religious group | ||||
| Muslim | 74 (56.9%) | 38 (56.9%) | 36 (54.5%) | |
| Sunnis | 51 (68.9%) | 26 (68.4%) | 25 (69.4%) | |
| Shiites | 2 (2.7%) | 1 (2.6%) | 1 (2.8%) | |
| Alawis | 4 (5.4%) | 3 (7.9%) | 1 (2.8%) | |
| Not further specified | 17 (23.0%) | 8 (21.1%) | 9 (25.0%) | |
| Christian | 9 (6.9%) | 6 (9.4%) | 3 (4.5%) | |
| Other | 12 (9.2%) | 6 (9.4%) | 6 (9.4%) | |
| None | 35 (26.9%) | 14 (10.8%) | 21 (16.2%) | 0.71 |
| Religiosity | Ø 18.50 (4.17) | Ø 18.51 (3.89) | Ø 18.49 (4.46) | 0.983 |
| Not religious (<10) | 0 (0%) | 0 (0%) | 0 (0%) | |
| Religious (10–19) | 68 (52.3%) | 38 (58.5%) | 30 (46.2%) | |
| Very religious (>19) | 62 (47.7%) | 27 (41.5%) | 35 (53.8%) | 0.16 |
| Variables | Study Sample | Intervention Group (n = 65) | Control Group | p-Value |
|---|---|---|---|---|
| (n = 133) | (n = 68) | |||
| Escape route 1 | ||||
| By airplane | 59 (44.4%) | 25 (38.5%) | 34 (50.0%) | |
| By land | 86 (64.7%) | 43 (66.1%) | 43 (63.2%) | |
| By sea | 76 (57.1%) | 37 (56.9%) | 39 (57.3%) | |
| Via transit country | 23 (17.3%) | 13 (20.0%) | 10 (14.7%) | 0.669 |
| Years since Syria was left (yrs) | Ø 50.4 (19.3) | Ø 3.9 (1.6) | Ø 3.7 (1.6) | 0.472 |
| Time spent in Germany (yrs) | Ø 41.2 (13.9) | Ø 3.0 (1.1) | Ø 3.0 (1.3) | 1 |
| Traumatic event (PDS-5) | ||||
| Serious, life-threatening illness | 5 (3.8%) | 4 (6.1%) | 1 (1.5%) | |
| Physical assault | 9 (6.8%) | 4 (6.1%) | 5 (7.3%) | |
| Military/combat-related | 47 (35.3%) | 21 (32.3%) | 26 (38.2%) | |
| Child abuse | 3 (2.3%) | 1 (1.5%) | 2 (2.9%) | |
| Accident | 3 (2.3%) | 2 (3.1%) | 1 (1.5%) | |
| Torture/imprisonment | 10 (7.5%) | 3 (4.6%) | 7 (10.3%) | |
| Other | 54 (40.6%) | 29 (44.6%) | 25 (36.8%) | |
| Refusal of answer | 2 (1.5%) | 1 (1.5%) | 1 (1.5%) | 0.667 |
| Post-traumatic stress symptoms (PDS-5) | Ø 23.8 (11.6) | Ø 23.2 (10.8) | Ø 24.4 (12.4) | 0.539 |
| Intrusion | 5.6 (4.1) | 5.4 (4.0) | 5.9 (4.2) | 0.483 |
| Avoidance | 2.6 (2.1) | 2.5 (1.9) | 2.7 (2.2) | 0.584 |
| Change in cognition & mood | 8.4 (5.4) | 8.0 (5.1) | 8.8 (5.8) | 0.439 |
| Arousal & hyperactivity | 7.1 (3.7) | 7.2 (3.8) | 7.0 (3.6) | 0.772 |
| Variables | Study Sample | Intervention Group (n = 65) | Control Group (n = 68) | p-Value |
|---|---|---|---|---|
| (n = 133) | ||||
| Depressive symptoms (PHQ-9) | Ø 9.2 (5.2) | Ø 9.2 (4.8) | Ø 9.3 (5.7) | 0.84 |
| No/low symptom severity (<10) | 73 (54.9%) | 37 (56.9%) | 36 (52.9%) | |
| Clinical significant severity(≥10) | 60 (45.1%) | 28 (43.1%) | 32 (47.1%) | 0.645 |
| Generalized anxiety (GAD-7) | Ø 8.5 (5.0) | Ø 8.2 (4.4) | Ø 8.8 (5.5) | 0.483 |
| No/low symptom severity (<10) | 79 (59.4%) | 40 (61.5%) | 39 (57.3%) | |
| Clinical significant severity(≥10) | 54 (40.6%) | 25 (38.5%) | 29 (42.6%) | 0.623 |
| Somatization (PHQ-15) | ||||
| Female | Ø 10.5 (5.3) | Ø 10.0 (5.2) | Ø 11.1 (5.4) | 0.441 |
| Low symptom severity (<10) | 18 (35.3%) | 12 (41.4%) | 6 (27.3%) | |
| Medium-high symptom severity (≥10) | 33 (64.7%) | 17 (58.6%) | 16 (72.7%) | 0.296 |
| Male | Ø 7.8 (5.1) | Ø 7.7 (5.0) | Ø 7.9 (5.3) | 0.853 |
| Low symptom severity (<10) | 52 (63.4%) | 22 (56.4%) | 30 (69.8%) | |
| Medium-high symptom severity (≥10) | 30 (36.6%) | 17 (43.6%) | 13 (30.2%) | 0.21 |
| Social network size (LSNS-6) | Ø 15.1 (5.3) | Ø 15.0 (5.5) | Ø 15.2 (5.2) | 0.785 |
| Social isolation (LSNS-6 < 12) | 43 (32.3 %) | 21 (32.3%) | 22 (32.4%) | 0.996 |
| Social support (ESSI) | Ø 18.0 (4.7) | Ø 18.4 (4.1) | Ø 17.7 (5.2) | 0.388 |
| Low support | 71 (53.4%) | 32 (49.2%) | 39 (57.4%) | |
| High support | 62 (46.6%) | 33 (50.8%) | 29 (42.6%) | 0.348 |
| General self-efficacy (GSE) | Ø 27.4 (4.7) | Ø 26.8 (5.2) | Ø 28.0 (4.0) | 0.151 |
| Resilience (RS-13) | Ø 64.4 (11.4) | Ø 61.6 (11.6) | Ø 67.0 (10.3) | 0.006, |
| d = 0.480 | ||||
| Low (13–66) | 70 (52.6%) | 41 (63.1%) | 29 (42.6%) | |
| Middle (67–72) | 25 (18.8%) | 11 (16.9%) | 14 (20.6%) | 0.046, |
| High (73–91) | 38 (28.6%) | 13 (20.0%) | 25 (36.8%) | V = 0.215 |
| Self-stigmatization (SSMIS-SF) | ||||
| Awareness | 28.3 (7.5) | 28.8 (8.3) | 27.8 (6.6) | 0.449 |
| Agreement | 18.8 (6.7) | 17.6 (6.5) | 20.0 (6.8) | 0.034, d = −0.372 |
| Application | 16.5 (6.6) | 15.2 (6.2) | 17.8 (6.8) | 0.021, d = −0.404 |
| Harm to Self-esteem | 18.6 (9.5) | 18.0 (9.5) | 19.2 (9.6) | 0.454 |
| Health-related quality of life & subjective health | ||||
| EQ-5D-5L | 0.82 (0.19) | 0.79 (0.23) | 0.86 (0.13) | 0.052 |
| EQ-VAS | 73.6 (18.9) | 73.0 (20.7) | 74.2 (16.9) | 0.713 |
| Suicidal risk (DSI-SS) | Ø 0.2 (1.0) | Ø 0.03 (0.2) | Ø 0.2 (1.1) | 0.168 |
| <3 (no suicidal risk) | 128 (96.2%) | 64 (98.5%) | 65 (95.6%) | |
| ≥3 (elevated suicidal risk) | 5 (3.8%) | 1 (1.5%) | 3 (4.4%) | 0.268 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Röhr, S.; Jung, F.U.; Renner, A.; Plexnies, A.; Hoffmann, R.; Dams, J.; Grochtdreis, T.; König, H.-H.; Kersting, A.; Riedel-Heller, S.G. Recruitment and Baseline Characteristics of Participants in the “Sanadak” Trial: A Self-Help App for Syrian Refugees with Post-traumatic Stress. Int. J. Environ. Res. Public Health 2020, 17, 7578. https://doi.org/10.3390/ijerph17207578
Röhr S, Jung FU, Renner A, Plexnies A, Hoffmann R, Dams J, Grochtdreis T, König H-H, Kersting A, Riedel-Heller SG. Recruitment and Baseline Characteristics of Participants in the “Sanadak” Trial: A Self-Help App for Syrian Refugees with Post-traumatic Stress. International Journal of Environmental Research and Public Health. 2020; 17(20):7578. https://doi.org/10.3390/ijerph17207578
Chicago/Turabian StyleRöhr, Susanne, Franziska U. Jung, Anna Renner, Anna Plexnies, Rahel Hoffmann, Judith Dams, Thomas Grochtdreis, Hans-Helmut König, Anette Kersting, and Steffi G. Riedel-Heller. 2020. "Recruitment and Baseline Characteristics of Participants in the “Sanadak” Trial: A Self-Help App for Syrian Refugees with Post-traumatic Stress" International Journal of Environmental Research and Public Health 17, no. 20: 7578. https://doi.org/10.3390/ijerph17207578