Effects of Combining High-Definition Transcranial Direct Current Stimulation with Short-Foot Exercise on Chronic Ankle Instability: A Pilot Randomized and Double-Blinded Study

 , and
, and
Abstract
:1. Introduction
2. Methods
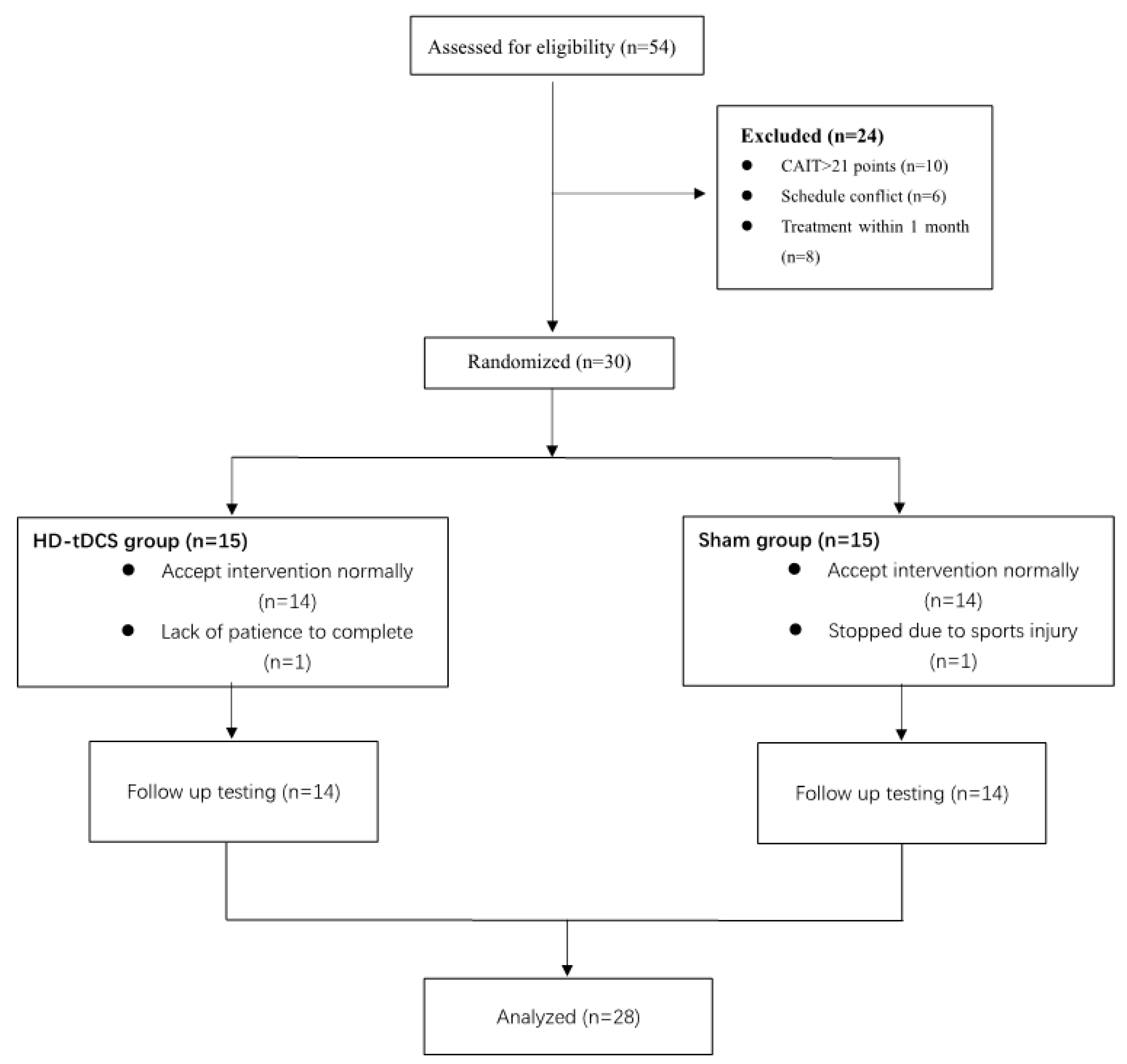
2.1. Participants
2.2. Study Design
2.3. Transcranial Direct Current Stimulation
2.4. Short-Foot Exercise
2.5. Functional Assessment
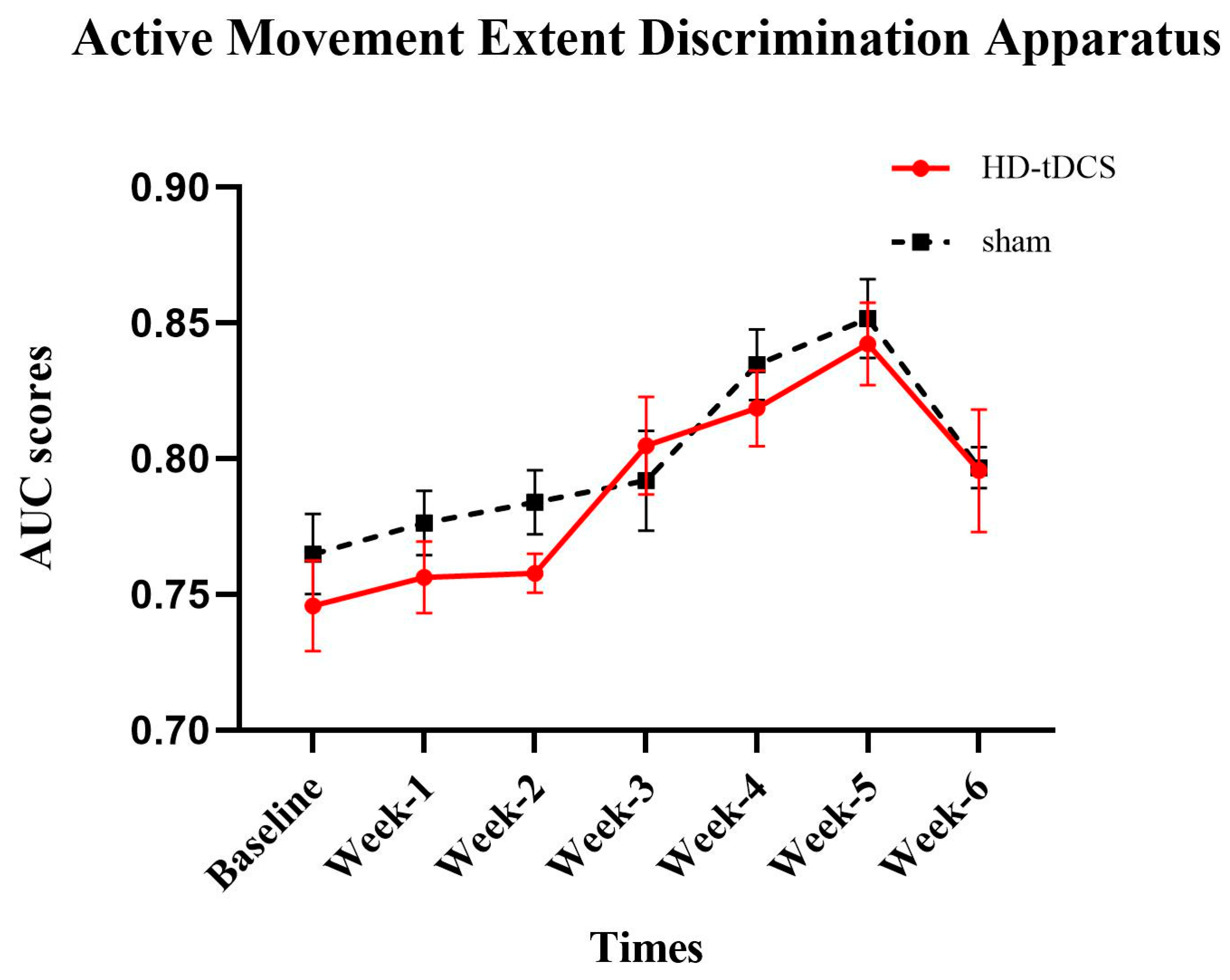
2.5.1. Active Movement Extent Discrimination Apparatus (AMEDA)
2.5.2. The Joint Position Reproduction
2.5.3. Y-Balance Test
2.5.4. Sensory Organization Test (SOT)
2.6. Statistical Analysis
3. Results
3.1. The Effects of Intervention on AMEDA
3.2. The Effects of Intervention on JPR
3.3. The Effects of Intervention on Y-Balance Test
3.4. The Effects of Intervention on SOT
4. Discussion
4.1. Proprioception
4.2. Dynamic Balance Function
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Attenborough, A.S.; Hiller, C.E.; Smith, R.M.; Stuelcken, M.; Greene, A.; Sinclair, P.J. Chronic ankle instability in sporting populations. Sports Med. 2014, 44, 1545–1556. [Google Scholar] [CrossRef] [PubMed]
- Lambers, K.; Ootes, D.; Ring, D.C. Incidence of patients with lower extremity injuries presenting to US emergency departments by anatomic region, disease category, and age. Clin. Orthop. Relat. Res. 2012, 470, 284–290. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thompson, C.; Schabrun, S.; Romero, R.; Bialocerkowski, A.; Marshall, P. Factors contributing to chronic ankle instability: A protocol for a systematic review of systematic reviews. Syst. Rev. 2016, 5, 94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hintermann, B.; Valderrabano, V.; Dereymaeker, G.; Dick, W. The HINTEGRA ankle: Rationale and short-term results of 122 consecutive ankles. Clin. Orthop. Relat. Res. 2004, 424, 57–68. [Google Scholar] [CrossRef]
- Valderrabano, V.; Hintermann, B.; Dick, W. Scandinavian total ankle replacement: A 3.7-year average followup of 65 patients. Clin. Orthop. Relat. Res. 2004, 424, 47–56. [Google Scholar] [CrossRef]
- Riemann, B.L. Is There a Link Between Chronic Ankle Instability and Postural Instability. J. Athl. Train. 2002, 37, 386–393. [Google Scholar]
- Varghese, J.P.; McIlroy, R.E.; Barnett-Cowan, M. Perturbation-evoked potentials: Significance and application in balance control research. Neurosci. Biobehav. Rev. 2017, 83, 267–280. [Google Scholar] [CrossRef]
- Kornecki, S.; Zschorlich, V. The nature of the stabilizing functions of skeletal muscles. J. Biomech. 1994, 27, 215–225. [Google Scholar] [CrossRef]
- Behm, D.G.; Anderson, K.; Curnew, R.S. Muscle Force and Activation Under Stable and Unstable Conditions. J. Strength Cond. Res. 2002, 16, 416–422. [Google Scholar] [CrossRef]
- Needle, A.R.; Baumeister, J.; Farquhar, W.B.; Greaney, J.L.; Higginson, J.S.; Kaminski, T.W.; Swanik, C.B. The relationship between the sensory responses to ankle-joint loading and corticomotor excitability. Int. J. Neurosci. 2018, 128, 435–441. [Google Scholar] [CrossRef]
- Pietrosimone, B.G.; Gribble, P.A. Chronic ankle instability and corticomotor excitability of the fibularis longus muscle. J. Athl. Train. 2012, 47, 621–626. [Google Scholar] [CrossRef] [Green Version]
- Manor, B.; Zhou, J.; Harrison, R.; Lo, O.Y.; Travison, T.G.; Hausdorff, J.M.; Pascual-Leone, A.; Lipsitz, L. Transcranial Direct Current Stimulation May Improve Cognitive-Motor Function in Functionally Limited Older Adults. Neurorehabilit. Neural Repair. 2018, 32, 788–798. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Hao, Y.; Wang, Y.; Jor’dan, A.; Pascual-Leone, A.; Zhang, J.; Fang, J.; Manor, B. Transcranial direct current stimulation reduces the cost of performing a cognitive task on gait and postural control. Eur. J. Neurosci. 2014, 39, 1343–1348. [Google Scholar] [CrossRef] [PubMed]
- Kaminski, E.; Steele, C.J.; Hoff, M.; Gundlach, C.; Rjosk, V.; Sehm, B.; Villringer, A.; Ragert, P. Transcranial direct current stimulation (tDCS) over primary motor cortex leg area promotes dynamic balance task performance. Clin. Neurophysiol. 2016, 127, 2455–2462. [Google Scholar] [CrossRef]
- Bruce, A.S.; Howard, J.S.; Van Werkhoven, H.; McBride, J.M.; Needle, A.R. The Effects of Transcranial Direct Current Stimulation on Chronic Ankle Instability. Med. Sci. Sports Exerc. 2020, 52, 335–344. [Google Scholar] [CrossRef]
- Morya, E.; Monte-Silva, K.; Bikson, M.; Esmaeilpour, Z.; Biazoli, C.E., Jr.; Fonseca, A.; Bocci, T.; Farzan, F.; Chatterjee, R.; Hausdorff, J.M.; et al. Beyond the target area: An integrative view of tDCS-induced motor cortex modulation in patients and athletes. J. Neuroeng. Rehabil. 2019, 16, 141. [Google Scholar] [CrossRef]
- Hogeveen, J.; Grafman, J.; Aboseria, M.; David, A.; Bikson, M.; Hauner, K.K. Effects of High-Definition and Conventional tDCS on Response Inhibition. Brain Stimul. 2016, 9, 720–729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hiller, C.E.; Refshauge, K.M.; Bundy, A.C.; Herbert, R.D.; Kilbreath, S.L. The Cumberland ankle instability tool: A report of validity and reliability testing. Arch. Phys. Med. Rehabil. 2006, 87, 1235–1241. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.; Cho, J.; Lee, S. Short-Foot Exercise Promotes Quantitative Somatosensory Function in Ankle Instability: A Randomized Controlled Trial. Med. Sci. Monit. 2019, 25, 618–626. [Google Scholar] [CrossRef] [PubMed]
- Datta, A.; Elwassif, M.; Battaglia, F.; Bikson, M. Transcranial current stimulation focality using disc and ring electrode configurations: FEM analysis. J. Neural Eng. 2008, 5, 163–174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nitsche, M.A.; Doemkes, S.; Karakose, T.; Antal, A.; Liebetanz, D.; Lang, N.; Tergau, F.; Paulus, W. Shaping the effects of transcranial direct current stimulation of the human motor cortex. J. Neurophysiol. 2007, 97, 3109–3117. [Google Scholar] [CrossRef] [Green Version]
- Alam, M.; Truong, D.Q.; Khadka, N.; Bikson, M. Spatial and polarity precision of concentric high-definition transcranial direct current stimulation (HD-tDCS). Phys. Med. Biol. 2016, 61, 4506–4521. [Google Scholar] [CrossRef] [PubMed]
- Xiao, S.; Wang, B.; Zhang, X.; Zhou, J.; Fu, W. Acute Effects of High-Definition Transcranial Direct Current Stimulation on Foot Muscle Strength, Passive Ankle Kinesthesia, and Static Balance: A Pilot Study. Brain Sci. 2020, 10, 246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kindred, J.H.; Kautz, S.A.; Wonsetler, E.C.; Bowden, M.G. Single Sessions of High-Definition Transcranial Direct Current Stimulation Do Not Alter Lower Extremity Biomechanical or Corticomotor Response Variables Post-stroke. Front. Neurosci. 2019, 13, 286. [Google Scholar] [CrossRef] [PubMed]
- Kikkert, S.; Mezue, M.; O’Shea, J.; Henderson Slater, D.; Johansen-Berg, H.; Tracey, I.; Makin, T.R. Neural basis of induced phantom limb pain relief. Ann. Neurol. 2019, 85, 59–73. [Google Scholar] [CrossRef] [Green Version]
- Zito, G.A.; Senti, T.; Cazzoli, D.; Muri, R.M.; Mosimann, U.P.; Nyffeler, T.; Nef, T. Cathodal HD-tDCS on the right V5 improves motion perception in humans. Front. Behav. Neurosci. 2015, 9, 257. [Google Scholar] [CrossRef] [Green Version]
- Brunoni, A.R.; Amadera, J.; Berbel, B.; Volz, M.S.; Rizzerio, B.G.; Fregni, F. A systematic review on reporting and assessment of adverse effects associated with transcranial direct current stimulation. Int. J. Neuropsychopharmacol. 2011, 14, 1133–1145. [Google Scholar] [CrossRef]
- Long, Z.; Wang, R.; Han, J.; Waddington, G.; Adams, R.; Anson, J. Optimizing ankle performance when taped: Effects of kinesiology and athletic taping on proprioception in full weight-bearing stance. J. Sci. Med. Sport 2017, 20, 236–240. [Google Scholar] [CrossRef]
- Lephart, S.M.; Pincivero, D.M.; Rozzi, S.L. Proprioception of the ankle and knee. Sports Med. 1998, 25, 149–155. [Google Scholar] [CrossRef]
- Baray, A.L.; Philippot, R.; Farizon, F.; Boyer, B.; Edouard, P.; French Association of Foot Surgery. Assessment of joint position sense deficit, muscular impairment and postural disorder following hemi-Castaing ankle ligamentoplasty. Orthop. Traumatol. Surg. Res. 2014, 100, S271–S274. [Google Scholar] [CrossRef] [Green Version]
- Johnston, W.; Dolan, K.; Reid, N.; Coughlan, G.F.; Caulfield, B. Investigating the effects of maximal anaerobic fatigue on dynamic postural control using the Y-Balance Test. J. Sci. Med. Sport 2018, 21, 103–108. [Google Scholar] [CrossRef] [Green Version]
- Shaffer, S.W.; Teyhen, D.S.; Lorenson, C.L.; Warren, R.L.; Koreerat, C.M.; Straseske, C.A.; Childs, J.D. Y-balance test: A reliability study involving multiple raters. Mil. Med. 2013, 178, 1264–1270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilson, B.R.; Robertson, K.E.; Burnham, J.M.; Yonz, M.C.; Ireland, M.L.; Noehren, B. The Relationship Between Hip Strength and the Y Balance Test. J. Sport Rehabil. 2018, 27, 445–450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pletcher, E.R.; Williams, V.J.; Abt, J.P.; Morgan, P.M.; Parr, J.J.; Wohleber, M.F.; Lovalekar, M.; Sell, T.C. Normative Data for the NeuroCom Sensory Organization Test in US Military Special Operations Forces. J. Athl. Train. 2017, 52, 129–136. [Google Scholar] [CrossRef] [Green Version]
- Harro, C.C.; Garascia, C. Reliability and Validity of Computerized Force Platform Measures of Balance Function in Healthy Older Adults. J. Geriatr. Phys. Ther. 2019, 42, E57–E66. [Google Scholar] [CrossRef]
- Unver, B.; Emin, U.E.; Eda, A. Effects of Short-Foot Exercises on Foot Posture, Pain, Disability and Plantar Pressure in Pes Planus. J. Sport Rehabil. 2019, 29, 436–440. [Google Scholar] [CrossRef] [PubMed]
- Geroin, C.; Picelli, A.; Munari, D.; Waldner, A.; Tomelleri, C.; Smania, N. Combined transcranial direct current stimulation and robot-assisted gait training in patients with chronic stroke: A preliminary comparison. Clin. Rehabil. 2011, 25, 537–548. [Google Scholar] [CrossRef] [PubMed]
- Ahn, H.; Zhong, C.; Miao, H.; Chaoul, A.; Park, L.; Yen, I.H.; Vila, M.A.; Sorkpor, S.; Abdi, S. Efficacy of combining home-based transcranial direct current stimulation with mindfulness-based meditation for pain in older adults with knee osteoarthritis: A randomized controlled pilot study. J. Clin. Neurosci. 2019, 70, 140–145. [Google Scholar] [CrossRef]
- Labbe, S.; Meftah, E.M.; Chapman, C.E. Effects of transcranial direct current stimulation of primary somatosensory cortex on vibrotactile detection and discrimination. J. Neurophysiol. 2016, 115, 1978–1987. [Google Scholar] [CrossRef] [Green Version]
- Miklovic, T.M.; Donovan, L.; Protzuk, O.A.; Kang, M.S.; Feger, M.A. Acute lateral ankle sprain to chronic ankle instability: A pathway of dysfunction. Phys. Sportsmed. 2018, 46, 116–122. [Google Scholar] [CrossRef]
- Needle, A.R.; Lepley, A.S.; Grooms, D.R. Central Nervous System Adaptation After Ligamentous Injury: A Summary of Theories, Evidence, and Clinical Interpretation. Sports Med. 2017, 47, 1271–1288. [Google Scholar] [CrossRef]
- Qi, F.; Nitsche, M.A.; Zschorlich, V.R. Modulating Observation-Execution-Related Motor Cortex Activity by Cathodal Transcranial Direct Current Stimulation. Brain Sci. 2019, 9, 121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riemann, B.L.; Myers, J.B.; Stone, D.A.; Lephart, S.M. Effect of lateral ankle ligament anesthesia on single-leg stance stability. Med. Sci. Sports Exerc. 2004, 36, 388–396. [Google Scholar] [CrossRef]
- McKeon, P.O.; Stein, A.J.; Ingersoll, C.D.; Hertel, J. Altered plantar-receptor stimulation-impairs postural control in those with chronic ankle instability. J. Sport Rehabil. 2012, 21, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Song, K.; Burcal, C.J.; Hertel, J.; Wikstrom, E.A. Increased Visual Use in Chronic Ankle Instability: A Meta-analysis. Med. Sci. Sports Exerc. 2016, 48, 2046–2056. [Google Scholar] [CrossRef]
- de Moura, M.C.D.S.; Hazime, F.A.; Marotti Aparicio, L.V.; Grecco, L.A.C.; Brunoni, A.R.; Hasue, R.H. Effects of transcranial direct current stimulation (tDCS) on balance improvement: A systematic review and meta-analysis. Somatosens. Mot. Res. 2019, 36, 122–135. [Google Scholar] [CrossRef] [PubMed]
- Kyriakareli, A.; Cousins, S.; Pettorossi, V.E.; Bronstein, A.M. Effect of transcranial direct current stimulation on vestibular-ocular and vestibulo-perceptual thresholds. Neuroreport 2013, 24, 808–812. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| HD-tDCS | Sham | p | |
|---|---|---|---|
| Gender (F/M) | 7/7 | 8/6 | |
| Age (year) | 21.14 ± 2.82 | 20.29 ± 1.49 | 0.331 |
| Height (cm) | 170.85 ± 7.35 | 170.96 ± 8.01 | 0.970 |
| Weight (kg) | 64.76 ± 13.63 | 62.45 ± 11.76 | 0.635 |
| CAIT score | 13.50 ± 4.57 | 15.79 ± 3.29 | 0.140 |
| Affected side (L/R) | 4/10 | 3/11 |
| Test | Group | Phase | Time × Group Effect | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Baseline | Week-2 | Week-3 | Week-4 | Week-5 | Week-6 | F | p | ||
| 10° inversion | HD-tDCS | 2.49 ± 1.0 | 2.66 ± 1.1 | 1.91 ± 0.9 | 2.04 ± 1.1 | 1.91 ± 0.5 | 1.88 ± 1.1 | 1.050 | 0.391 |
| sham | 2.25 ± 0.9 | 2.43 ± 0.8 | 2.29 ± 1.3 | 2.51 ± 1.1 | 2.31 ± 1.2 | 1.81 ± 0.9 | |||
| 15° inversion | HD-tDCS | 2.66 ± 1.0 | 2.55 ± 0.3 | 1.97 ± 0.3 a | 2.18 ± 0.9 | 2.11 ± 1.1 | 1.77 ± 0.8 a | 2.951 | 0.029 |
| sham | 2.09 ± 0.8 | 1.67 ± 0.5 | 1.91 ± 1.0 | 2.95 ± 1.6 | 1.95 ± 0.3 | 1.95 ± 1.3 | |||
| 15° eversion | HD-tDCS | 4.26 ± 1.1 | 3.20 ± 1.7 | 3.52 ± 1.9 | 3.19 ± 1.3 | 2.50 ± 1.3 a | 1.99 ± 0.7 a | 1.589 | 0.167 |
| sham | 4.03 ± 1.7 | 3.49 ± 1.9 | 2.62 ± 1.1 a | 3.84 ± 1.4 | 3.07 ± 1.3 a | 2.50 ± 1.0 a | |||
| Test | Group | Phase | Time × Group Effect | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | Week-1 | Week-2 | Week-3 | Week-4 | Week-5 | Week-6 | F | p | ||
| SOT1 | HD-tDCS | 94.02 ± 2.5 | 94.79 ± 1.6 | 92.91 ± 2.8 | 93.91 ± 2.7 | 93.79 ± 2.4 | 94.69 ± 2.1 | 95.39 ± 1.00 a | 1.220 | 0.299 |
| sham | 95.19 ± 2.0 | 94.64 ± 2.5 | 93.95 ± 2.0 | 94.22 ± 2.1 | 94.26 ± 2.9 | 95.05 ± 1.7 | 94.45 ± 1.9 | |||
| SOT2 | HD-tDCS | 93.12 ± 3.2 | 93.24 ± 3.0 | 92.95 ± 3.1 | 93.41 ± 2.5 | 94.37 ± 2.3 | 93.53 ± 2.9 | 94.10 ± 2.0 | 0.994 | 0.431 |
| sham | 93.81 ± 2.3 | 94.83 ± 1.4 | 94.84 ± 1.2 | 94.62 ± 1.7 | 95.11 ± 1.0 | 94.73 ± 1.5 | 94.36 ± 1.6 | |||
| SOT3 | HD-tDCS | 93.31 ± 2.6 | 94.29 ± 1.8 | 93.60 ± 3.1 | 94.26 ± 2.6 | 93.88 ± 2.2 | 93.64 ± 2.1 | 94.31 ± 1.9 | 2.081 | 0.058 |
| sham | 94.47 ± 1.2 | 93.43 ± 2.9 | 94.14 ± 2.5 | 93.83 ± 2.9 | 94.29 ± 2.1 | 94.60 ± 1.7 | 93.48 ± 2.3 | |||
| SOT4 | HD-tDCS | 85.33 ± 5.4 | 83.10 ± 6.7 | 86.14 ± 3.5 | 86.74 ± 4.0 | 88.39 ± 2.7 a | 88.14 ± 3.5 a | 88.38 ± 2.9 a | 4.761 | 0.002 |
| sham | 87.86 ± 4.0 | 86.34 ± 1.8 | 88.87 ± 1.7 | 87.26 ± 2.2 | 86.33 ± 3.8 | 86.48 ± 3.8 | 85.95 ± 4.6 | |||
| SOT5 | HD-tDCS | 77.08 ± 8.0 | 81.55 ± 5.2 a | 80.45 ± 3.4 a | 82.23 ± 2.4 a | 82.74 ± 3.8 a | 84.62 ± 4.6 a | 82.29 ± 3.8 a | 4.030 | 0.005 |
| sham | 81.46 ± 1.1 | 81.01 ± 3.9 | 83.83 ± 2.6 | 82.38 ± 4.4 | 84.67 ± 3.5 | 80.24 ± 8.7 | 83.14 ± 5.7 | |||
| SOT6 | HD-tDCS | 77.24 ± 7.4 | 78.43 ± 2.1 | 80.41 ± 3.5 | 82.12 ± 5.0 a | 84.64 ± 3.0 a | 83.87 ± 1.2 a | 85.47 ± 3.1 a | 2.586 | 0.050 |
| sham | 78.12 ± 6.0 | 81.14 ± 3.7 | 81.09 ± 3.7 | 81.61 ± 3.7 | 83.89 ± 1.8 a | 84.49 ± 1.5 a | 80.98 ± 7.4 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ma, Y.; Yin, K.; Zhuang, W.; Zhang, C.; Jiang, Y.; Huang, J.; Manor, B.; Zhou, J.; Liu, Y. Effects of Combining High-Definition Transcranial Direct Current Stimulation with Short-Foot Exercise on Chronic Ankle Instability: A Pilot Randomized and Double-Blinded Study. Brain Sci. 2020, 10, 749. https://doi.org/10.3390/brainsci10100749
Ma Y, Yin K, Zhuang W, Zhang C, Jiang Y, Huang J, Manor B, Zhou J, Liu Y. Effects of Combining High-Definition Transcranial Direct Current Stimulation with Short-Foot Exercise on Chronic Ankle Instability: A Pilot Randomized and Double-Blinded Study. Brain Sciences. 2020; 10(10):749. https://doi.org/10.3390/brainsci10100749
Chicago/Turabian StyleMa, Yuanbo, Keyi Yin, Wei Zhuang, Cui Zhang, Yong Jiang, Jin Huang, Brad Manor, Junhong Zhou, and Yu Liu. 2020. "Effects of Combining High-Definition Transcranial Direct Current Stimulation with Short-Foot Exercise on Chronic Ankle Instability: A Pilot Randomized and Double-Blinded Study" Brain Sciences 10, no. 10: 749. https://doi.org/10.3390/brainsci10100749