An Acute Application of Cerebellar Transcranial Direct Current Stimulation Does Not Improve Motor Performance in Parkinson’s Disease

 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
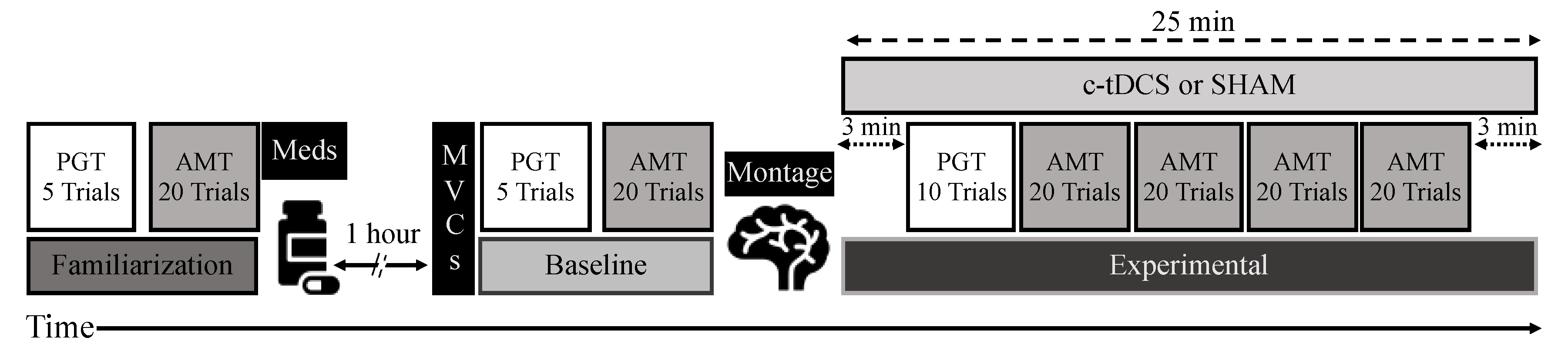
2.2. Experimental Design and Procedures
2.3. Experimental Tasks
2.3.1. MVCs
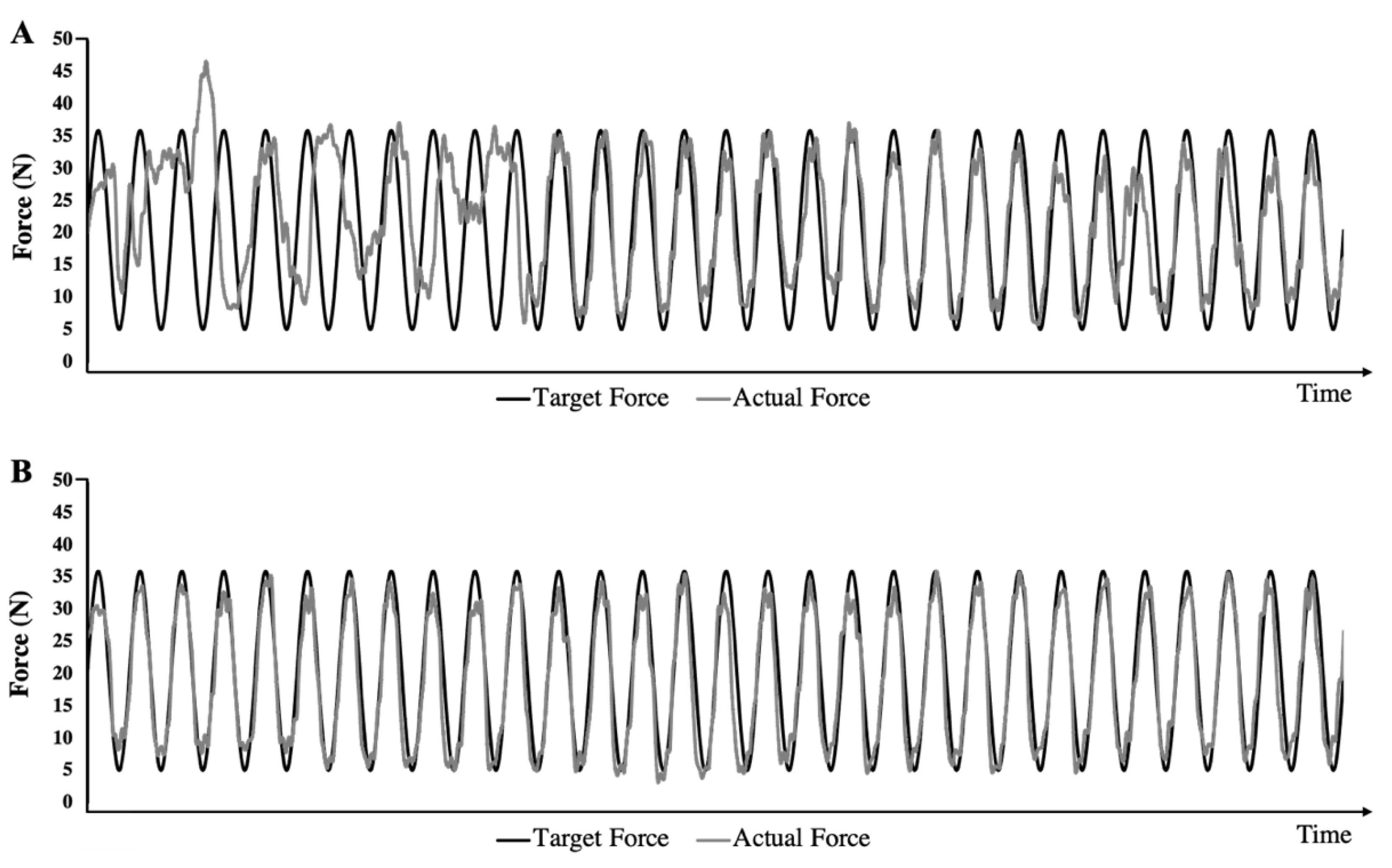
2.3.2. PGT
2.3.3. AMT
2.3.4. c-tDCS
2.4. Data Analysis
2.5. Statistical Analysis
3. Results
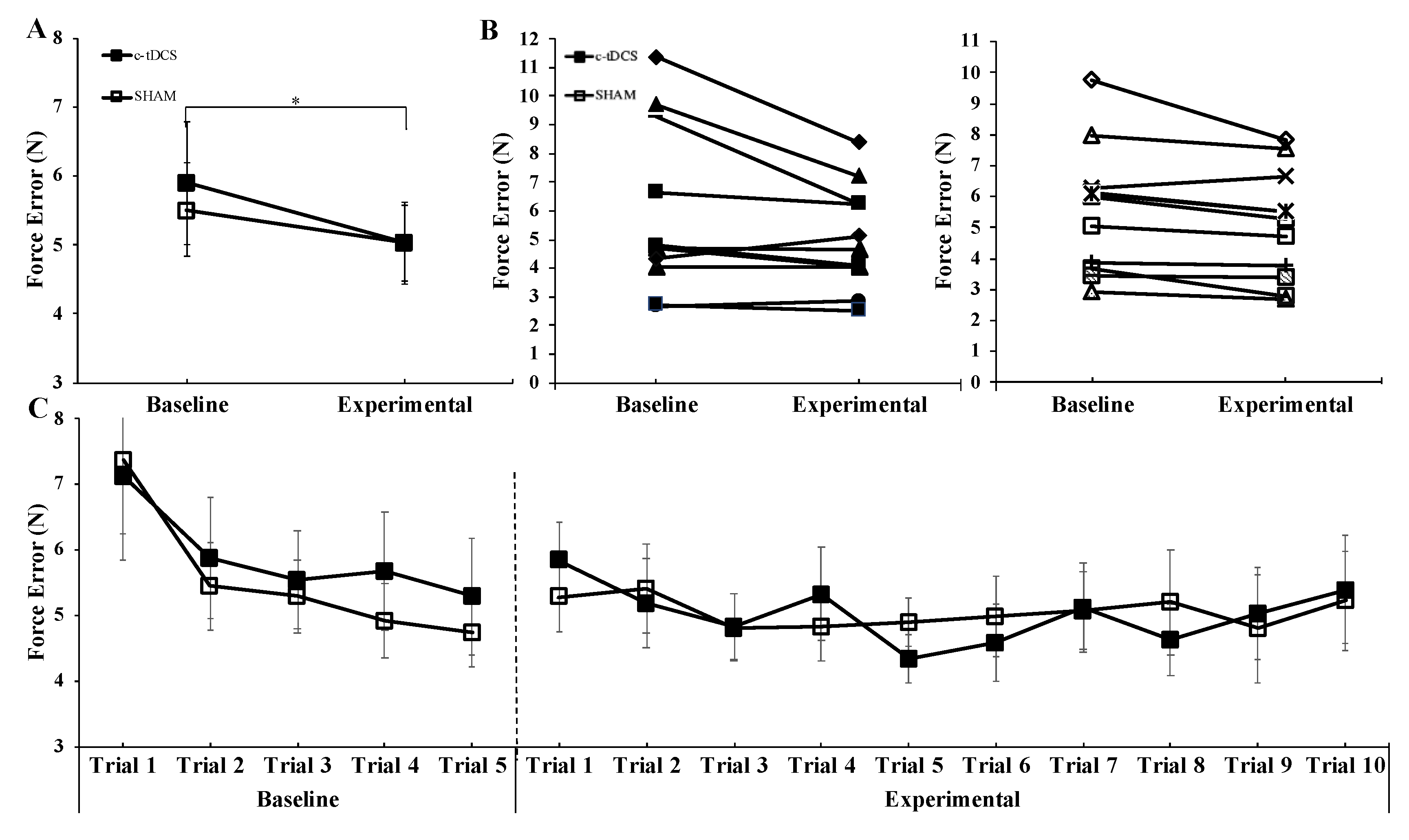
3.1. PGT
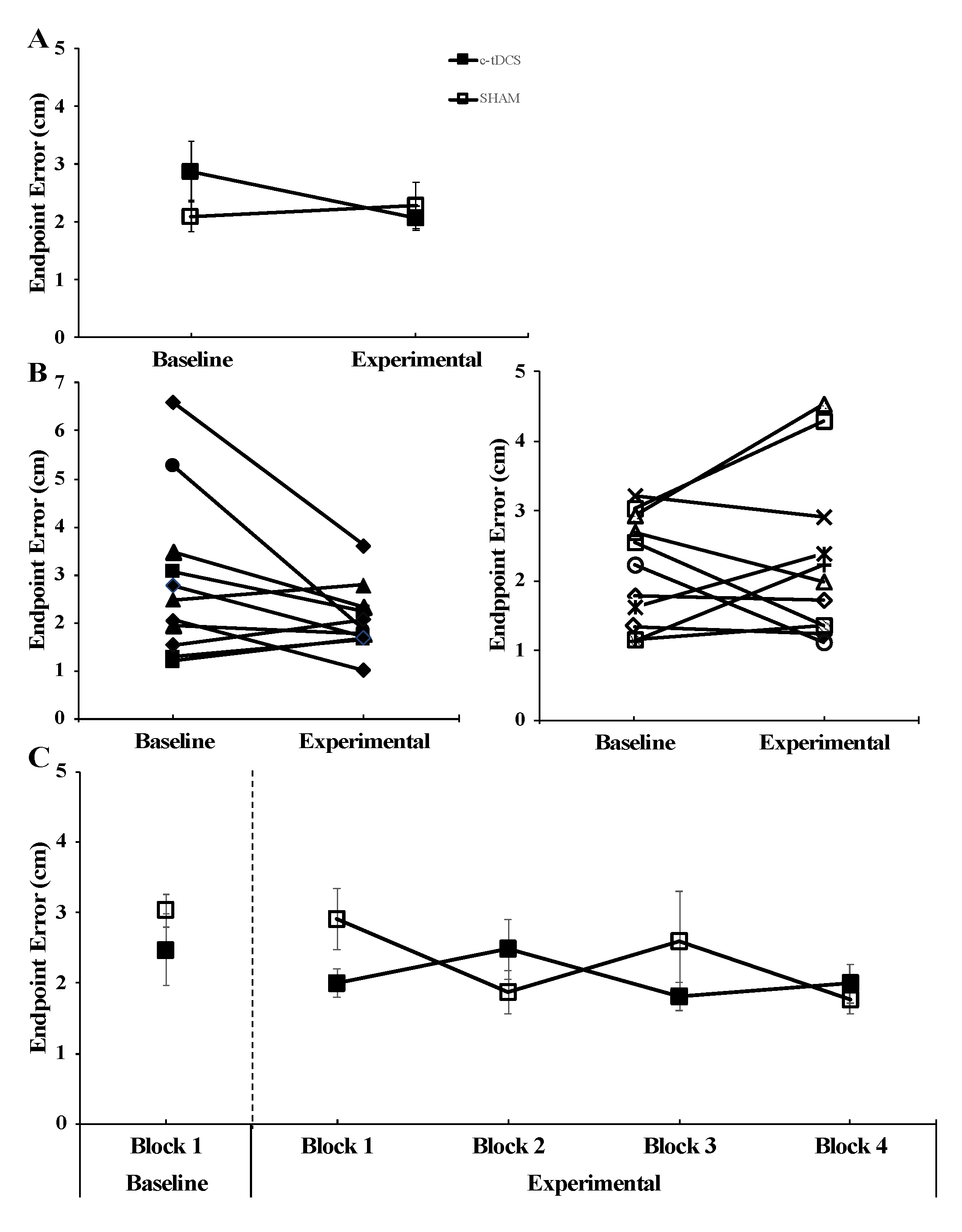
3.2. AMT
4. Discussion
4.1. Influence of Acute c-tDCS Application on Motor Performance in PD
4.2. Possible Factors Responsible for the Lack Ability of c-tDCS to Improve Motor Performance in PD
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- LeWitt, P.A.; Bharucha, A.; Chitrit, I.; Takis, C.; Patil, S.; Schork, M.A.; Pichurko, B. Perceived exertion and muscle efficiency in Parkinson’s disease: L-DOPA effects. Clin. Neuropharmacol. 1994, 17, 454–459. [Google Scholar] [CrossRef]
- Bronstein, J.M.; Tagliati, M.; Alterman, R.L.; Lozano, A.M.; Volkmann, J.; Stefani, A.; Horak, F.B.; Okun, M.S.; Foote, K.D.; Krack, P.; et al. Deep brain stimulation for Parkinson disease: An expert consensus and review of key issues. Arch. Neurol. 2011, 68, 165. [Google Scholar] [CrossRef]
- Germano, I.M.; Gracies, J.M.; Weisz, D.J.; Tse, W.; Koller, W.C.; Olanow, C.W. Unilateral stimulation of the subthalamic nucleus in Parkinson disease: A double-blind 12-month evaluation study. J. Neurosurg. 2004, 101, 36–42. [Google Scholar] [CrossRef] [Green Version]
- Cotman, C.W.; Engesser-Cesar, C. Exercise enhances and protects brain function. Exerc. Sport Sci. Rev. 2002, 30, 75–79. [Google Scholar] [CrossRef] [PubMed]
- Zigmond, M.J.; Cameron, J.L.; Hoffer, B.J.; Smeyne, R.J. Neurorestoration by physical exercise: Moving forward. Parkinsonism Relat. Disord. 2012, 18 (Suppl. S1), S147–S150. [Google Scholar] [CrossRef]
- Goodwin, V.A.; Richards, S.H.; Taylor, R.S.; Taylor, A.H.; Campbell, J.L. The effectiveness of exercise interventions for people with Parkinson’s disease: A systematic review and meta-analysis. Mov. Disord. 2008, 23, 631–640. [Google Scholar] [CrossRef] [PubMed]
- Lamotte, G.; Rafferty, M.R.; Prodoehl, J.; Kohrt, W.M.; Comella, C.L.; Simuni, T.; Corcos, D.M. Effects of Endurance Exercise Training on The Motor and Non-Motor Features of Parkinson’s Disease: A Review. J. Parkinsons Dis. 2015, 5, 621. [Google Scholar] [CrossRef] [PubMed]
- Alberts, J.L.; Linder, S.M.; Penko, A.L.; Lowe, M.J.; Phillips, M. It is not about the bike, it is about the pedaling: Forced exercise and Parkinson’s disease. Exerc. Sport Sci. Rev. 2011, 39, 177–186. [Google Scholar] [CrossRef] [PubMed]
- Corcos, D.M.; Robichaud, J.A.; David, F.J.; Leurgans, S.E.; Vaillancourt, D.E.; Poon, C.; Rafferty, M.R.; Kohrt, W.M.; Comella, C.L. A two-year randomized controlled trial of progressive resistance exercise for Parkinson’s disease. Mov. Disord. 2013, 28, 1230–1240. [Google Scholar] [CrossRef] [Green Version]
- Buch, E.R.; Santarnecchi, E.; Antal, A.; Born, J.; Celnik, P.A.; Classen, J.; Gerloff, C.; Hallett, M.; Hummel, F.C.; Nitsche, M.A.; et al. Effects of tDCS on motor learning and memory formation: A consensus and critical position paper. Clin. Neurophysiol. 2017, 128, 589–603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Broeder, S.; Nackaerts, E.; Heremans, E.; Vervoort, G.; Meesen, R.; Verheyden, G.; Nieuwboer, A. Transcranial direct current stimulation in Parkinson’s disease: Neurophysiological mechanisms and behavioral effects. Neurosci. Biobehav. Rev. 2015, 57, 105–117. [Google Scholar] [CrossRef] [PubMed]
- Stagg, C.J.; Nitsche, M.A. Physiological basis of transcranial direct current stimulation. Neuroscientist 2011, 17, 37–53. [Google Scholar] [CrossRef] [PubMed]
- Brunoni, A.R.; Nitsche, M.A.; Bolognini, N.; Bikson, M.; Wagner, T.; Merabet, L.; Edwards, D.J.; Valero-Cabre, A.; Rotenberg, A.; Pascual-Leone, A.; et al. Clinical research with transcranial direct current stimulation (tDCS): Challenges and future directions. Brain Stimul. 2012, 5, 175–195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dobbs, B.; Pawlak, N.; Biagioni, M.; Agarwal, S.; Shaw, M.; Pilloni, G.; Bikson, M.; Datta, A.; Charvet, L. Generalizing remotely supervised transcranial direct current stimulation (tDCS): Feasibility and benefit in Parkinson’s disease. J. Neuroeng. Rehabil. 2018, 15, 114. [Google Scholar] [CrossRef] [Green Version]
- Agarwal, S.; Pawlak, N.; Cucca, A.; Sharma, K.; Dobbs, B.; Shaw, M.; Charvet, L.; Biagioni, M. Remotely-supervised transcranial direct current stimulation paired with cognitive training in Parkinson’s disease: An open-label study. J. Clin. Neurosci. 2018, 57, 51–57. [Google Scholar] [CrossRef]
- Block, H.; Celnik, P. Stimulating the cerebellum affects visuomotor adaptation but not intermanual transfer of learning. Cerebellum 2013, 12, 781–793. [Google Scholar] [CrossRef]
- Hardwick, R.M.; Celnik, P.A. Cerebellar direct current stimulation enhances motor learning in older adults. Neurobiol. Aging 2014, 35, 2217–2221. [Google Scholar] [CrossRef] [Green Version]
- Jackson, A.K.; de Albuquerque, L.L.; Pantovic, M.; Fischer, K.M.; Guadagnoli, M.A.; Riley, Z.A.; Poston, B. Cerebellar Transcranial Direct Current Stimulation Enhances Motor Learning in a Complex Overhand Throwing Task. Cerebellum 2019, 18, 813–816. [Google Scholar] [CrossRef]
- Ni, Z.; Pinto, A.D.; Lang, A.E.; Chen, R. Involvement of the cerebellothalamocortical pathway in Parkinson disease. Ann. Neurol. 2010, 68, 816–824. [Google Scholar] [CrossRef]
- Wu, T.; Hallett, M. The cerebellum in Parkinson’s disease. Brain 2013, 136 Pt 3, 696–709. [Google Scholar] [CrossRef] [Green Version]
- Hummel, F.C.; Heise, K.; Celnik, P.; Floel, A.; Gerloff, C.; Cohen, L.G. Facilitating skilled right hand motor function in older subjects by anodal polarization over the left primary motor cortex. Neurobiol. Aging 2010, 31, 2160–2168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bostan, A.C.; Dum, R.P.; Strick, P.L. The basal ganglia communicate with the cerebellum. Proc. Natl. Acad. Sci. USA 2010, 107, 8452–8456. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hummel, F.C.; Voller, B.; Celnik, P.; Floel, A.; Giraux, P.; Gerloff, C.; Cohen, L.G. Effects of brain polarization on reaction times and pinch force in chronic stroke. BMC Neurosci. 2006, 7, 73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Workman, C.D.; Fietsam, A.C.; Uc, E.Y.; Rudroff, T. Cerebellar Transcranial Direct Current Stimulation in People with Parkinson’s Disease: A Pilot Study. Brain Sci. 2020, 10, 96. [Google Scholar] [CrossRef] [Green Version]
- Hore, J.; Timmann, D.; Watts, S. Disorders in timing and force of finger opening in overarm throws made by cerebellar subjects. Ann. N. Y. Acad. Sci. 2002, 978, 1–15. [Google Scholar] [CrossRef]
- Timmann, D.; Lee, P.; Watts, S.; Hore, J. Kinematics of arm joint rotations in cerebellar and unskilled subjects associated with the inability to throw fast. Cerebellum 2008, 7, 366–378. [Google Scholar] [CrossRef]
- Tseng, Y.W.; Diedrichsen, J.; Krakauer, J.W.; Shadmehr, R.; Bastian, A.J. Sensory prediction errors drive cerebellum-dependent adaptation of reaching. J. Neurophysiol. 2007, 98, 54–62. [Google Scholar] [CrossRef] [Green Version]
- Vaillancourt, D.E.; Thulborn, K.R.; Corcos, D.M. Neural basis for the processes that underlie visually guided and internally guided force control in humans. J. Neurophysiol. 2003, 90, 3330–3340. [Google Scholar] [CrossRef]
- Postuma, R.B.; Berg, D.; Stern, M.; Poewe, W.; Olanow, C.W.; Oertel, W.; Obeso, J.; Marek, K.; Litvan, I.; Lang, A.E.; et al. MDS clinical diagnostic criteria for Parkinson’s disease. Mov. Disord. 2015, 30, 1591–1601. [Google Scholar] [CrossRef]
- Poston, B.; Christou, E.A.; Enoka, J.A.; Enoka, R.M. Timing variability and not force variability predicts the endpoint accuracy of fast and slow isometric contractions. Exp. Brain Res. 2010, 202, 189–202. [Google Scholar] [CrossRef] [Green Version]
- Poston, B.; Danna-Dos Santos, A.; Jesunathadas, M.; Hamm, T.M.; Santello, M. Force-independent distribution of correlated neural inputs to hand muscles during three-digit grasping. J. Neurophysiol. 2010, 104, 1141–1154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Danna-Dos Santos, A.; Poston, B.; Jesunathadas, M.; Bobich, L.R.; Hamm, T.M.; Santello, M. Influence of fatigue on hand muscle coordination and EMG-EMG coherence during three-digit grasping. J. Neurophysiol. 2010, 104, 3576–3587. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reis, J.; Fischer, J.T.; Prichard, G.; Weiller, C.; Cohen, L.G.; Fritsch, B. Time- but Not Sleep-Dependent Consolidation of tDCS-Enhanced Visuomotor Skills. Cereb. Cortex 2013, 25, 109–117. [Google Scholar] [CrossRef]
- Reis, J.; Schambra, H.M.; Cohen, L.G.; Buch, E.R.; Fritsch, B.; Zarahn, E.; Celnik, P.A.; Krakauer, J.W. Noninvasive cortical stimulation enhances motor skill acquisition over multiple days through an effect on consolidation. Proc. Natl. Acad. Sci. USA 2009, 106, 1590–1595. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schambra, H.M.; Abe, M.; Luckenbaugh, D.A.; Reis, J.; Krakauer, J.W.; Cohen, L.G. Probing for hemispheric specialization for motor skill learning: A transcranial direct current stimulation study. J. Neurophysiol. 2011, 106, 652–661. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cantarero, G.; Spampinato, D.; Reis, J.; Ajagbe, L.; Thompson, T.; Kulkarni, K.; Celnik, P. Cerebellar direct current stimulation enhances on-line motor skill acquisition through an effect on accuracy. J. Neurosci. 2015, 35, 3285–3290. [Google Scholar] [CrossRef]
- Spraker, M.B.; Prodoehl, J.; Corcos, D.M.; Comella, C.L.; Vaillancourt, D.E. Basal ganglia hypoactivity during grip force in drug naive Parkinson’s disease. Hum. Brain Mapp. 2010, 31, 1928–1941. [Google Scholar] [CrossRef]
- Prodoehl, J.; Corcos, D.M.; Vaillancourt, D.E. Basal ganglia mechanisms underlying precision grip force control. Neurosci. Biobehav. Rev. 2009, 33, 900–908. [Google Scholar] [CrossRef] [Green Version]
- Spraker, M.B.; Corcos, D.M.; Vaillancourt, D.E. Cortical and subcortical mechanisms for precisely controlled force generation and force relaxation. Cereb. Cortex 2009, 19, 2640–2650. [Google Scholar] [CrossRef] [Green Version]
- Neely, K.A.; Planetta, P.J.; Prodoehl, J.; Corcos, D.M.; Comella, C.L.; Goetz, C.G.; Shannon, K.L.; Vaillancourt, D.E. Force control deficits in individuals with Parkinson’s disease, multiple systems atrophy, and progressive supranuclear palsy. PLoS ONE 2013, 8, e58403. [Google Scholar] [CrossRef] [Green Version]
- Poston, B.; Van Gemmert, A.W.; Sharma, S.; Chakrabarti, S.; Zavaremi, S.H.; Stelmach, G. Movement trajectory smoothness is not associated with the endpoint accuracy of rapid multi-joint arm movements in young and older adults. Acta Psychol. 2013, 143, 157–167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seidler, R.D.; Alberts, J.L.; Stelmach, G.E. Multijoint movement control in Parkinson’s disease. Exp. Brain Res. 2001, 140, 335–344. [Google Scholar] [CrossRef] [PubMed]
- van Dun, K.; Bodranghien, F.C.; Marien, P.; Manto, M.U. tDCS of the Cerebellum: Where Do We Stand in 2016? Technical Issues and Critical Review of the Literature. Front. Hum. Neurosci. 2016, 10, 199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nitsche, M.A.; Cohen, L.G.; Wassermann, E.M.; Priori, A.; Lang, N.; Antal, A.; Paulus, W.; Hummel, F.; Boggio, P.S.; Fregni, F.; et al. Transcranial direct current stimulation: State of the art 2008. Brain Stimul. 2008, 1, 206–223. [Google Scholar] [CrossRef]
- Albuquerque, L.L.; Fischer, K.M.; Pauls, A.L.; Pantovic, M.; Guadagnoli, M.A.; Riley, Z.A.; Poston, B. An acute application of transcranial random noise stimulation does not enhance motor skill acquisition or retention in a golf putting task. Hum. Mov. Sci. 2019, 66, 241–248. [Google Scholar] [CrossRef]
- Boisgontier, M.P. Motor aging results from cerebellar neuron death. Trends Neurosci. 2015, 38, 127–128. [Google Scholar] [CrossRef] [Green Version]
- Bastian, A.J.; Martin, T.A.; Keating, J.G.; Thach, W.T. Cerebellar ataxia: Abnormal control of interaction torques across multiple joints. J. Neurophysiol. 1996, 76, 492–509. [Google Scholar] [CrossRef]
- Flament, D.; Hore, J. Movement and electromyographic disorders associated with cerebellar dysmetria. J. Neurophysiol. 1986, 55, 1221–1233. [Google Scholar] [CrossRef]
- Beretta, V.S.; Conceicao, N.R.; Nobrega-Sousa, P.; Orcioli-Silva, D.; Dantas, L.; Gobbi, L.T.B.; Vitório, R. Transcranial direct current stimulation combined with physical or cognitive training in people with Parkinson’s disease: A systematic review. J. Neuroeng. Rehabil. 2020, 17, 74. [Google Scholar] [CrossRef]
- Simpson, M.W.; Mak, M. The effect of transcranial direct current stimulation on upper limb motor performance in Parkinson’s disease: A systematic review. J. Neurol. 2019, 1–10. [Google Scholar] [CrossRef]
- Steiner, K.M.; Enders, A.; Thier, W.; Batsikadze, G.; Ludolph, N.; Ilg, W.; Timmann, D. Cerebellar tDCS Does Not Improve Learning in a Complex Whole Body Dynamic Balance Task in Young Healthy Subjects. PLoS ONE 2016, 11, e0163598. [Google Scholar] [CrossRef] [Green Version]
- Sadnicka, A.; Hamada, M.; Bhatia, K.P.; Rothwell, J.C.; Edwards, M.J. Cerebellar stimulation fails to modulate motor cortex plasticity in writing dystonia. Mov. Disord. 2014, 29, 1304–1307. [Google Scholar] [CrossRef] [PubMed]
- Hamoudi, M.; Schambra, H.M.; Fritsch, B.; Schoechlin-Marx, A.; Weiller, C.; Cohen, L.G.; Reis, J. Transcranial Direct Current Stimulation Enhances Motor Skill Learning but Not Generalization in Chronic Stroke. Neurorehabil. Neural Repair. 2018, 32, 295–308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prichard, G.; Weiller, C.; Fritsch, B.; Reis, J. Effects of different electrical brain stimulation protocols on subcomponents of motor skill learning. Brain Stimul. 2014, 7, 532–540. [Google Scholar] [CrossRef] [PubMed]
- Hamada, M.; Galea, J.M.; Di Lazzaro, V.; Mazzone, P.; Ziemann, U.; Rothwell, J.C. Two distinct interneuron circuits in human motor cortex are linked to different subsets of physiological and behavioral plasticity. J. Neurosci. 2014, 34, 12837–12849. [Google Scholar] [CrossRef]
- Reis, J.; Swayne, O.B.; Vandermeeren, Y.; Camus, M.; Dimyan, M.A.; Harris-Love, M.; Perez, M.A.; Ragert, P.; Rothwell, J.C.; Cohen, L.G. Contribution of transcranial magnetic stimulation to the understanding of cortical mechanisms involved in motor control. J. Physiol. 2008, 586, 325–351. [Google Scholar] [CrossRef]
- Spampinato, D.A.; Celnik, P.A.; Rothwell, J.C. Cerebellar-Motor Cortex Connectivity: One or Two Different Networks? J. Neurosci. 2020, 40, 4230–4239. [Google Scholar] [CrossRef]
- Oldrati, V.; Schutter, D. Targeting the Human Cerebellum with Transcranial Direct Current Stimulation to Modulate Behavior: A Meta-Analysis. Cerebellum 2018, 17, 228–236. [Google Scholar] [CrossRef] [Green Version]
- Galea, J.M.; Vazquez, A.; Pasricha, N.; de Xivry, J.J.; Celnik, P. Dissociating the roles of the cerebellum and motor cortex during adaptive learning: The motor cortex retains what the cerebellum learns. Cereb. Cortex 2011, 21, 1761–1770. [Google Scholar] [CrossRef] [Green Version]
- Jayaram, G.; Tang, B.; Pallegadda, R.; Vasudevan, E.V.; Celnik, P.; Bastian, A. Modulating locomotor adaptation with cerebellar stimulation. J. Neurophysiol. 2012, 107, 2950–2957. [Google Scholar] [CrossRef] [Green Version]
- Fregni, F.; Boggio, P.S.; Santos, M.C.; Lima, M.; Vieira, A.L.; Rigonatti, S.P.; Silva, M.T.A.; Barbosa, E.R.; Nitsche, M.A.; Pascual-Leone, A. Noninvasive cortical stimulation with transcranial direct current stimulation in Parkinson’s disease. Mov. Disord. 2006, 21, 1693–1702. [Google Scholar] [CrossRef] [PubMed]
- Hummel, F.; Celnik, P.; Giraux, P.; Floel, A.; Wu, W.H.; Gerloff, C.; Cohen, L.G. Effects of non-invasive cortical stimulation on skilled motor function in chronic stroke. Brain 2005, 128 Pt 3, 490–499. [Google Scholar] [CrossRef] [Green Version]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |





© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lima de Albuquerque, L.; Pantovic, M.; Clingo, M.; Fischer, K.; Jalene, S.; Landers, M.; Mari, Z.; Poston, B. An Acute Application of Cerebellar Transcranial Direct Current Stimulation Does Not Improve Motor Performance in Parkinson’s Disease. Brain Sci. 2020, 10, 735. https://doi.org/10.3390/brainsci10100735
Lima de Albuquerque L, Pantovic M, Clingo M, Fischer K, Jalene S, Landers M, Mari Z, Poston B. An Acute Application of Cerebellar Transcranial Direct Current Stimulation Does Not Improve Motor Performance in Parkinson’s Disease. Brain Sciences. 2020; 10(10):735. https://doi.org/10.3390/brainsci10100735
Chicago/Turabian StyleLima de Albuquerque, Lidio, Milan Pantovic, Mitchel Clingo, Katherine Fischer, Sharon Jalene, Merrill Landers, Zoltan Mari, and Brach Poston. 2020. "An Acute Application of Cerebellar Transcranial Direct Current Stimulation Does Not Improve Motor Performance in Parkinson’s Disease" Brain Sciences 10, no. 10: 735. https://doi.org/10.3390/brainsci10100735