Intervention Using Body Shadow to Evoke Loading Imagery in a Patient with Complex Regional Pain Syndrome in the Foot: A Case Report


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient
2.2. Assessment of Physical Therapy before the Intervention Using Body Shadow
2.2.1. Pain Assessment
2.2.2. NLS Assessment
2.2.3. Disgust Assessment
2.2.4. Body Image Assessment
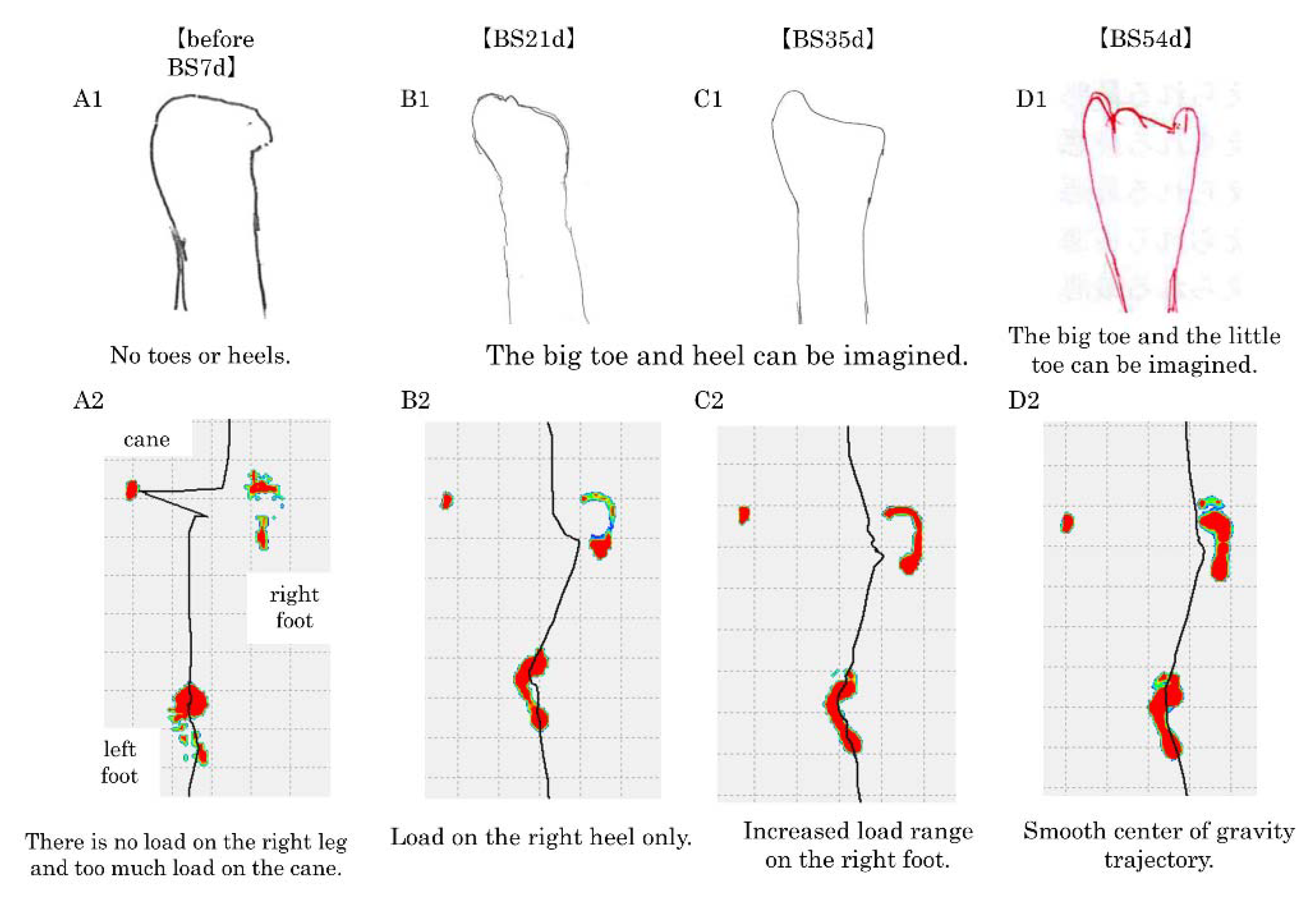
2.2.5. Gait Performance Assessment
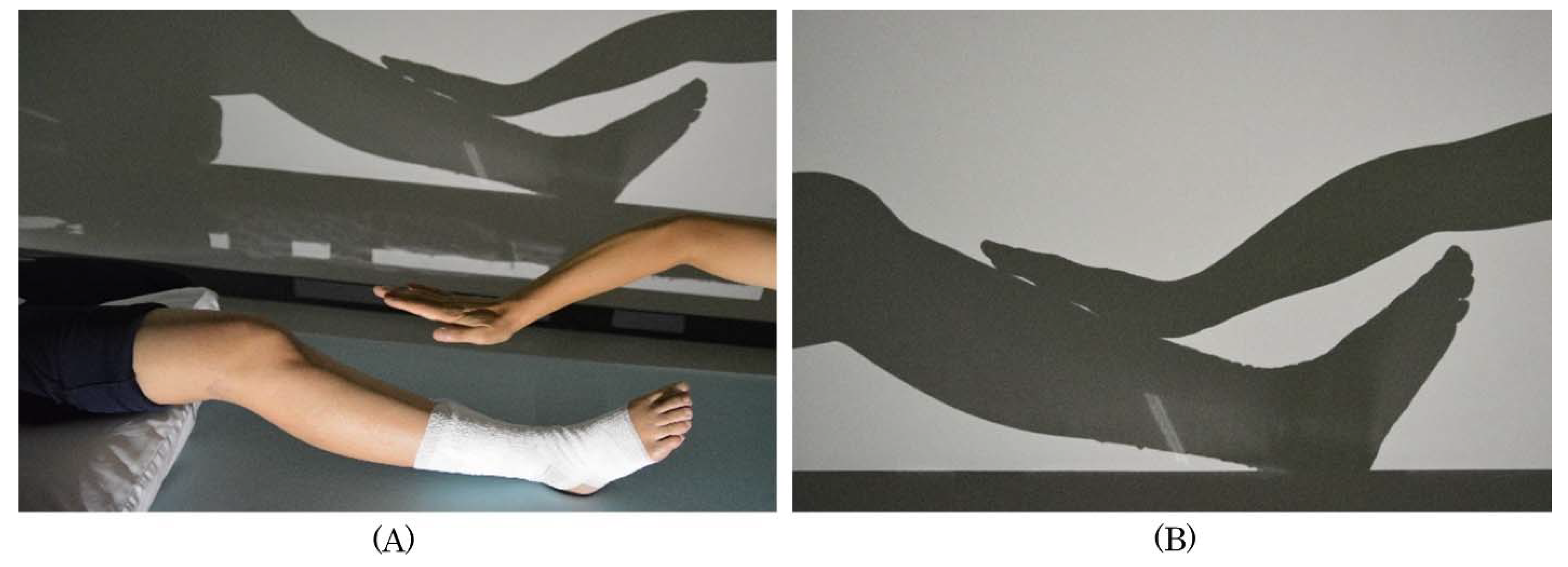
2.3. Body-Shadow Intervention and Process
2.4. Self-Exercise Instruction
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Perez, R.S.; Zollinger, P.E.; Dijkstra, P.U.; Thomassen-Hilgersom, I.L.; Zuurmond, W.W.; Rosenbrand, K.C.; Geertzen, J.H.; CRPS I task force. Evidence based guidelines for complex regional pain syndrome type 1. BMC Neurol. 2010, 10, 20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iolascon, G.; Moretti, A. Pharmacotherapeutic options for complex regional pain syndrome. Expert Opin Pharmacother. 2019, 20, 1377–1386. [Google Scholar] [CrossRef] [PubMed]
- Lewis, J.S.; Kersten, P.; McCabe, C.S.; McPherson, K.M.; Blake, D.R. Body perception disturbance: A contribution to pain in complex regional pain syndrome (CRPS). Pain 2007, 133, 111–119. [Google Scholar] [CrossRef] [PubMed]
- Reinersmann, A.; Landwehrt, J.; Krumova, E.K.; Peterburs, J.; Ocklenburg, S.; Güntürkün, O.; Maier., C. The rubber hand illusion in complex regional pain syndrome: Preserved ability to integrate a rubber hand indicates intact multisensory integration. Pain 2013, 154, 1519–1527. [Google Scholar] [CrossRef] [PubMed]
- Halicka, M.; Vittersø, A.D.; Proulx, M.J.; Bultitude, J.H. Neuropsychological changes in complex regional pain syndrome (CRPS). Behav. Neurol. 2020, 4561831. [Google Scholar] [CrossRef] [PubMed]
- Smart, K.M.; Wand, B.M.; O’Connell, N.E. Physiotherapy for pain and disability in adults with complex regional pain syndrome (CRPS) types I and II. Cochrane Database Syst. Rev. 2016, 2, CD010853. [Google Scholar] [CrossRef] [Green Version]
- Bultitude, J.H.; Rafal, R.D. Derangement of body representation in complex regional pain syndrome: Report of a case treated with mirror and prisms. Exp. Brain Res. 2010, 204, 409–418. [Google Scholar] [CrossRef] [Green Version]
- Birklein, F.; Dimova, V. Complex regional pain syndrome-up-to-date. Pain Rep. 2017, 2, e624. [Google Scholar] [CrossRef]
- Schrier, E.; Geertzen, J.H.B.; Scheper, J.; Dijkstra, P.U. Psychosocial factors associated with poor outcomes after amputation for complex regional pain syndrome type-I. PLoS ONE 2019, 14, e0213589. [Google Scholar] [CrossRef] [Green Version]
- Lohnberg, J.A.; Altmaier, E.M. A review of psychosocial factors in complex regional pain syndrome. J. Clin. Psychol. Med. Settings 2013, 20, 247–254. [Google Scholar] [CrossRef]
- Hirakawa, Y.; Fujiwara, A.; Imai, R.; Hiraga, Y.; Morioka, S. Clinical intervention using body shadows for a patient with complex regional pain syndrome who reported severe pain and self-disgust toward the affected site: A case report. J. Pain Res. 2020, 13, 971–977. [Google Scholar] [CrossRef] [PubMed]
- Osumi, M.; Okuno, H.; Nishigami, T.; Ueta, K.; Morioka, S. Tactile localization training for pain, sensory disturbance, and distorted body image: A case study of complex regional pain syndrome. Neurocase 2015, 21, 628–634. [Google Scholar] [CrossRef] [PubMed]
- Turner-Cobb, J.M.; Michalaki, M.; Osborn, M. Self-conscious emotions in patients suffering from chronic musculoskeletal pain: A brief report. Psychol. Health. 2015, 30, 495–501. [Google Scholar] [CrossRef]
- Oaten, M.J.; Stevenson, R.J.; Case, T.I. The effect of disgust on pain sensitivity. Physiol. Behav. 2015, 138, 107–112. [Google Scholar] [CrossRef] [PubMed]
- McCabe, C.S.; Haigh, R.C.; Halligan, P.W.; Blake, D.R. Simulating sensory-motor incongruence in healthy volunteers: Implications for a cortical model of pain. Rheumatology 2005, 44, 509–516. [Google Scholar] [CrossRef] [Green Version]
- Cash, T.F. Body image: Past, present, and future. Body Image 2004, 1, 1–5. [Google Scholar] [CrossRef]
- Hrabosky, J.I.; Cash, T.F.; Veale, D.; Neziroglu, F.; Soll, E.A.; Garner, D.M.; Strachan-Kinser, M.; Bakke, B.; Clauss, L.J.; Phillips, K.A. Multidimensional body image comparisons among patients with eating disorders, body dysmorphic disorder, and clinical controls: A multisite study. Body Image 2009, 6, 155–163. [Google Scholar] [CrossRef]
- Spreckelsen, P.V.; Glashouwer, K.A.; Bennik, E.C.; Wessel, I.; de Jong, P.J. Negative body image: Relationships with heightened disgust propensity, disgust sensitivity, and self-directed disgust. PLoS ONE 2018, 13, e0198532. [Google Scholar] [CrossRef]
- Wand, B.M.; Elliott, R.L.; Sawyer, A.E.; Spence, R.; Beales, D.J.; O’Sullivan, P.B.; Smith, A.J.; Gibson, W. Disrupted body-image and pregnancy-related lumbopelvic pain. A preliminary investigation. Musculoskelet. Sci. Pract. 2017, 30, 49–55. [Google Scholar] [CrossRef] [Green Version]
- Di Pietro, F.; McAuley, J.H.; Parkitny, L.; Lotze, M.; Wand, B.M.; Moseley, G.L.; Stanton, T.R. Primary somatosensory cortex function in complex regional pain syndrome: A systematic review and meta-analysis. J. Pain 2013, 14, 1001–1018. [Google Scholar] [CrossRef]
- Lewis, J.S.; Kersten, P.; McPherson, K.M.; Taylor, G.J.; Harris, N.; McCabe, C.S.; Blake, D.R. Wherever is my arm? Impaired upper limb position accuracy in complex regional pain syndrome. Pain 2010, 149, 463–469. [Google Scholar] [CrossRef] [PubMed]
- Echalier, A.; Borg, C.; Creac’h, C.; Laurent, B.; Michael, G.A. Spontaneous sensations reveal distorted body perception in complex regional pain syndrome (CRPS). Brain Cogn. 2020, 142, 105568. [Google Scholar] [CrossRef] [PubMed]
- Ramachandran, V.S.; Rogers-Ramachandran, D. Synaesthesia in phantom limbs induced with mirrors. Proc. Biol. Sci. 1996, 263, 377–386. [Google Scholar] [CrossRef] [PubMed]
- Ezendam, D.; Bongers, R.M.; Jannink, M.J. Systematic review of the effectiveness of mirror therapy in upper extremity function. Disabil. Rehabil. 2009, 31, 2135–2149. [Google Scholar] [CrossRef] [PubMed]
- Mouraux, D.; Lenoir, C.; Tuna, T.; Brassinne, E.; Sobczak, S. The long-term effect of complex regional pain syndrome type 1 on disability and quality of life after foot injury. Disabil. Rehabil. 2019, 14, 1–9. [Google Scholar] [CrossRef]
- Rommel, O.; Gehling, M.; Dertwinkel, R.; Witscher, K.; Zenz, M.; Malin, J.P.; Jänig, W. Hemisensory impairment in patients with complex regional pain syndrome. Pain 1999, 80, 95–101. [Google Scholar] [CrossRef]
- Frettlöh, J.; Hüppe, M.; Maier, C. Severity and specificity of neglect-like symptoms in patients with complex regional pain syndrome (CRPS) compared to chronic limb pain of other origins. Pain 2006, 124, 184–189. [Google Scholar] [CrossRef]
- Gustafsson, M.; Ekholm, J.; Ohman, A. From shame to respect: Musculoskeletal pain patients’ experience of a rehabilitation programme, a qualitative study. J. Rehabil. Med. 2004, 36, 97–103. [Google Scholar] [CrossRef]
- Reme, S.E. Body image concerns and distortions in people with persistent pain. Scand. J. Pain 2018, 18, 339–340. [Google Scholar] [CrossRef]
- Kodaka, K.; Kanazawa, A. Innocent body-shadow mimics physical body. Iperception 2017, 8, 2041669517706520. [Google Scholar] [CrossRef]
- Pavani, F.; Castiello, U. Binding personal and extrapersonal space through body shadows. Nat. Neurosci. 2004, 7, 14–16. [Google Scholar] [CrossRef] [PubMed]
- Kuylen, C.; Balas, B.; Thomas, L.E. My shadow, myself: Cast-body shadows are embodied. Psychon. Bull. Rev. 2014, 21, 676–681. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moseley, G.L.; Zalucki, N.; Birklein, F.; Marinus, J.; van Hilten, J.J.; Luomajoki, H. Thinking about movement hurts: The effect of motor imagery on pain and swelling in people with chronic arm pain. Arthritis Rheum. 2008, 59, 623–631. [Google Scholar] [CrossRef]
- Barke, A.; Baudewig, J.; Schmidt-Samoa, C.; Dechent, P.; Kröner-Herwig, B. Neural correlates of fear of movement in high and low fear-avoidant chronic low back pain patients: An event-related fMRI study. Pain 2012, 153, 540–552. [Google Scholar] [CrossRef] [PubMed]
- Barad, M.J.; Ueno, T.; Younger, J.; Chatterjee, N.; Mackey, S. Complex regional pain syndrome is associated with structural abnormalities in pain-related regions of the human brain. J. Pain 2014, 15, 197–203. [Google Scholar] [CrossRef] [Green Version]
- Ushida, T.; Ikemoto, T.; Taniguchi, S.; Ishida, K.; Murata, Y.; Ueda, W.; Tanaka, S.; Ushida, A.; Tani, T. Virtual pain stimulation of allodynia patients activates cortical representation of pain and emotions: A functional MRI study. Brain Topogr. 2005, 18, 27–35. [Google Scholar] [CrossRef]
- Iseki, K.; Hanakawa, T.; Shinozaki, J.; Nankaku, M.; Fukuyama, H. Neural mechanisms involved in mental imagery and observation of gait. Neuroimage 2008, 41, 1021–1031. [Google Scholar] [CrossRef] [Green Version]
- Kokkinara, E.; Kilteni, K.; Blom, K.J.; Slater, M. First person perspective of seated participants over a walking virtual body leads to illusory agency over the walking. Sci. Rep. 2016, 6, 28879. [Google Scholar] [CrossRef] [Green Version]
- Petkova, V.I.; Ehrsson, H.H. If I were you: Perceptual illusion of body swapping. PLoS ONE 2008, 3, e3832. [Google Scholar] [CrossRef] [Green Version]
- Slater, M.; Perez-Marcos, D.; Ehrsson, H.H.; Sanchez-Vives, M.V. Inducing illusory ownership of a virtual body. Front. Neurosci. 2009, 3, 214–220. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Before BS35d | Before BS7d | BS7d | BS14d | BS21d | BS35d | BS49d | BS54d | |
|---|---|---|---|---|---|---|---|---|
| SF-MPQ-2 (total) | 166 | 168 | 130 | 122 | 113 | 109 | 102 | 94 |
| SF-MPQ-2 (continuous pain) | 44 | 46 | 40 | 33 | 33 | 26 | 22 | 20 |
| SF-MPQ-2 (intermittent pain) | 42 | 41 | 26 | 23 | 22 | 22 | 22 | 20 |
| SF-MPQ-2 (neuropathic pain) | 52 | 52 | 42 | 49 | 40 | 47 | 46 | 44 |
| SF-MPQ-2 (affective descriptors) | 28 | 29 | 22 | 17 | 18 | 14 | 12 | 10 |
| NLS (total) | 480 | 475 | 390 | 285 | 270 | 210 | 155 | 145 |
| NLS-MN | 290 | 285 | 270 | 185 | 175 | 150 | 125 | 120 |
| NLS-CN | 190 | 190 | 120 | 100 | 95 | 60 | 30 | 25 |
| Disgust assessment | 9 | 10 | 7 | 5 | 4 | 3 | 2 | 4 |
| Rehabilitation program | ||||||||
| Static stretch | ||||||||
| Muscle strength training | ||||||||
| Mirror therapy | ||||||||
| Body-shadow intervention, first step | ||||||||
| Body-shadow intervention, second step | ||||||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hirakawa, Y.; Imai, R.; Shigetoh, H.; Morioka, S. Intervention Using Body Shadow to Evoke Loading Imagery in a Patient with Complex Regional Pain Syndrome in the Foot: A Case Report. Brain Sci. 2020, 10, 718. https://doi.org/10.3390/brainsci10100718
Hirakawa Y, Imai R, Shigetoh H, Morioka S. Intervention Using Body Shadow to Evoke Loading Imagery in a Patient with Complex Regional Pain Syndrome in the Foot: A Case Report. Brain Sciences. 2020; 10(10):718. https://doi.org/10.3390/brainsci10100718
Chicago/Turabian StyleHirakawa, Yoshiyuki, Ryota Imai, Hayato Shigetoh, and Shu Morioka. 2020. "Intervention Using Body Shadow to Evoke Loading Imagery in a Patient with Complex Regional Pain Syndrome in the Foot: A Case Report" Brain Sciences 10, no. 10: 718. https://doi.org/10.3390/brainsci10100718