Pulmonary Sequestration Associated with Actinomycosis: A Case Report

 ,
,
Abstract
:1. Introduction
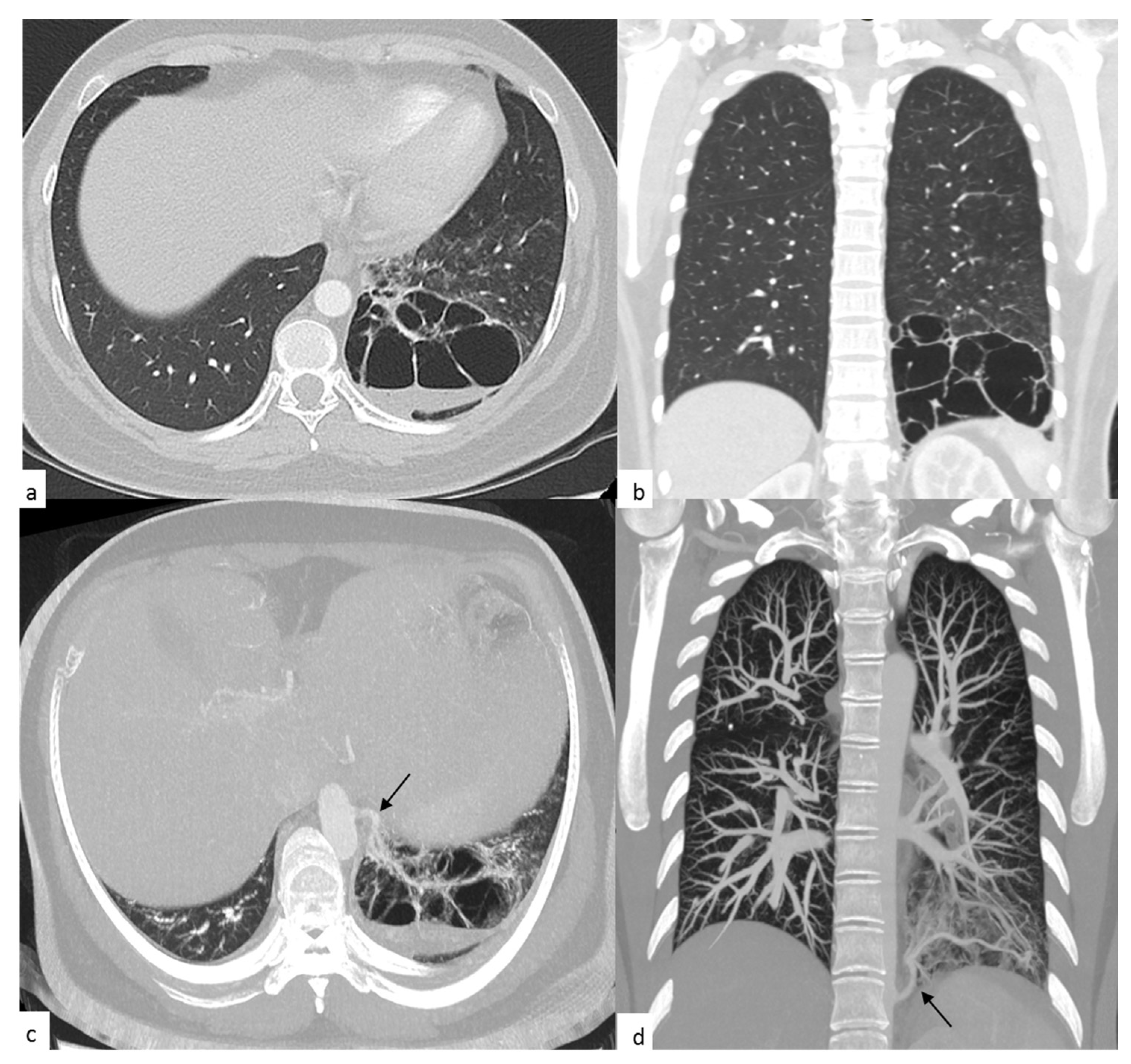
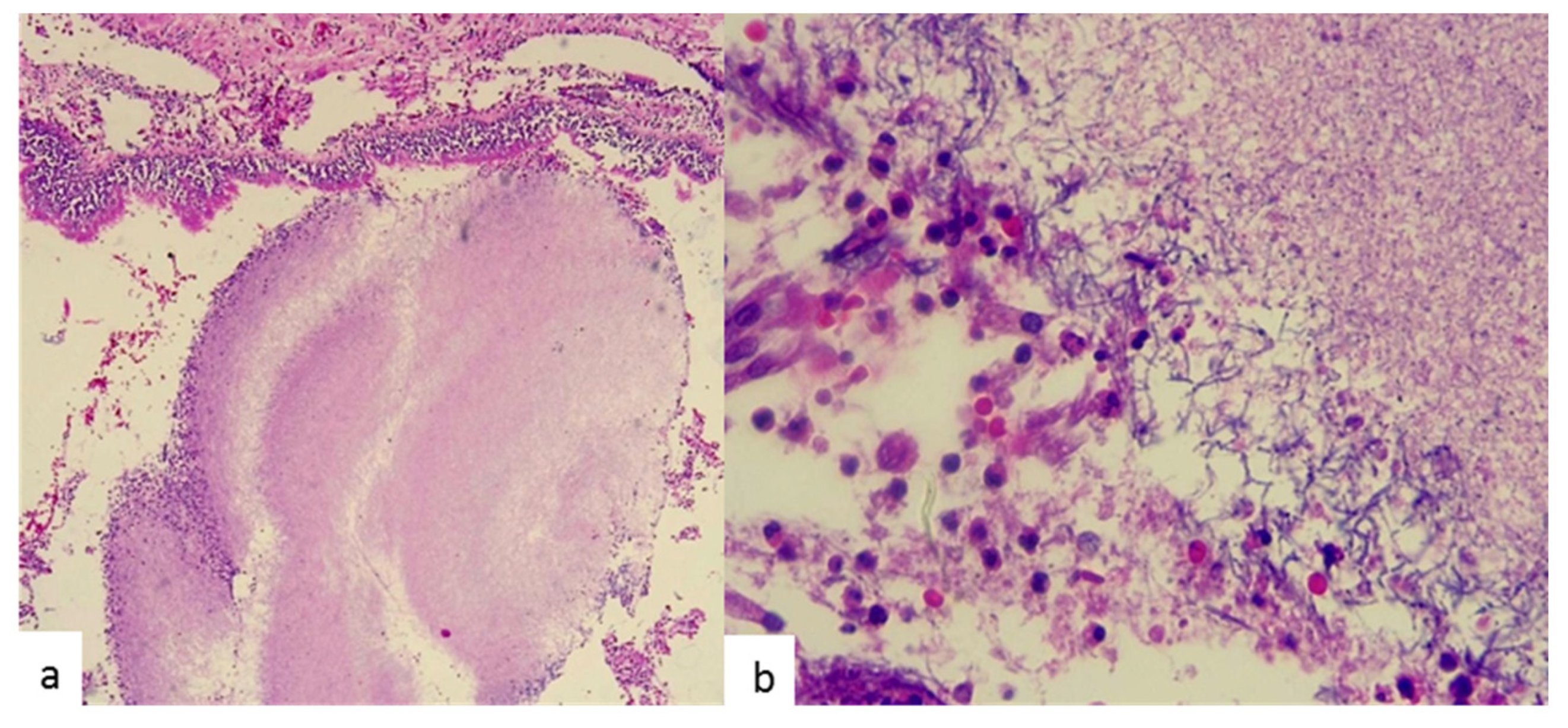
2. Case Presentation
3. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Savic, B.; Birtel, F.J.; Tholen, W.; Funke, H.D.; Knoche, R. Lung sequestration: Report of seven cases and review of 540 published cases. Thorax 1979, 34, 96–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qian, X.; Sun, Y.; Liu, D.; Wu, X.; Wang, Z.; Tang, Y. Pulmonary sequestration: A case report and literature review. Int. J. Clin. Exp. Med. 2015, 8, 21822–21825. [Google Scholar] [PubMed]
- Gezer, S.; Taştepe, İ.; Sırmalı, M.; Fındık, G.; Türüt, H.; Kaya, S.; Karaoglanoglu, N.; Cetin, G. Pulmonary sequestration: A single-institutional series composed of 27 cases. J. Thorac. Cardiovasc. Surg. 2007, 133, 955–959. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hertzenberg, C.; Daon, E.; Kramer, J. Intralobar pulmonary sequestration in adults: Three case reports. J. Thorac. Dis. 2012, 4, 516–519. [Google Scholar] [PubMed]
- Wright, C. Congenital malformations of the lung. Curr. Diagnostic Pathol. 2006, 12, 191–201. [Google Scholar] [CrossRef]
- Sun, X.; Xiao, Y. Pulmonary sequestration in adult patients: A retrospective study. Eur J. Cardio-Thoracic Surg. 2015, 48, 279–282. [Google Scholar] [CrossRef] [Green Version]
- Könönen, E.; Wade, W.G. Actinomyces and Related Organisms in Human Infections. Clin. Microbiol. Rev. 2015, 28, 419–442. [Google Scholar] [CrossRef] [Green Version]
- Kruse, W.; Flügge, K.G.F.W.; Flügge, C.; Kolle, W. Die Mikroorganismen: Mit besonderer Berücksichtigung der Ätiologie der Infektionskrankheiten; FCW Vogel: Leipzig, Germany, 1896; Volume 2. [Google Scholar]
- Li, J.; Li, Y.; Zhou, Y.; Wang, C.; Wu, B.; Wan, J. Actinomyces and Alimentary Tract Diseases: A Review of Its Biological Functions and Pathology. BioMed Res. Int. 2018, 2018, 1–8. [Google Scholar]
- Parra Medina, R.; Moreno, P.; Polo, J.F.; Bonilla, J.C. Fistula bronco-pericárdica en una mujer joven por actinomicosis pulmonar complicada. Rev. Repert. Med. Cirugía 2018, 27, 182–183. [Google Scholar] [CrossRef]
- Brown, J.R. Human actinomycosis: A study of 181 subjects. Hum. Pathol. 1973, 4, 319–330. [Google Scholar] [CrossRef]
- Wong, V.K.; Turmezei, T.D.; Weston, V.C. Actinomycosis. BMJ 2011, 343, d6099. [Google Scholar] [CrossRef]
- Valour, F.; Sénéchal, A.; Dupieux, C.; Karsenty, J.; Lustig, S.; Breton, P.; Gleizal, A.; Boussel, L.; Laurent, F.; Braun, E.; et al. Actinomycosis: Etiology, clinical features, diagnosis, treatment, and management. Infect. Drug Resist. 2014, 2014, 183–197. [Google Scholar]
- Xie, Z.; Li, S.; Zeng, Y.; Yuan, J.; Chen, G.l. Clinical analysis of pulmonary actinomycosis:report of 4 cases. New Med. 2009, 40, 644–646. [Google Scholar]
- Morikawa, H.; Tanaka, T.; Hamaji, M.; Ueno, Y. A case of aspergillosis associated with intralobar pulmonary sequestration. Asian Cardiovasc. Thorac. Ann. 2011, 19, 66–68. [Google Scholar] [CrossRef] [PubMed]
- Elia, S.; Alifano, M.; Gentile, M.; Somma, P.; D’Armiento, F.P.; Ferrante, G. Infection with Mycobacterium tuberculosis complicating a pulmonary sequestration. Ann. Thorac. Surg. 1998, 66, 566–567. [Google Scholar] [CrossRef]
- Koh, W.-J.; Hong, G.; Kim, K.; Ahn, S.; Han, J. Pulmonary sequestration infected with nontuberculous mycobacteria: A report of two cases and literature review. Asian Pac. J. Trop. Med. 2012, 5, 917–919. [Google Scholar] [CrossRef] [Green Version]
- Foucrier, A.; Woerther, P.-L.; Le Dorze, M.; Ruimy, R.; Laissy, J.-P.; Castier, Y.; Mourvillier, A. Pulmonary Sequestration Syndrome Diagnosed from a Nocardia Infection. Am. J. Respir. Crit. Care Med. 2012, 186, 288. [Google Scholar] [CrossRef]
- Pryce, D.M. Lower accessory pulmonary artery with intralobar sequestration of lung. J. Path Bact. 1946, 58, 457–467. [Google Scholar]
- Gebauer, P.W.; Mason, C.B. Intralobar Pulmonary Sequestration Associated with Anomalous Pulmonary Vessels: A Nonentity. Dis. Chest. 1959, 35, 282–288. [Google Scholar] [CrossRef]
- Wei, Y.; Li, F. Pulmonary sequestration: A retrospective analysis of 2625 cases in China. Eur J. Cardio-Thoracic Surg. 2011, 40, e39–e42. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.R.; Jung, L.Y.; Oh, I.-J.; Kim, Y.-C.; Shin, K.-C.; Lee, M.K.; Yang, S.-H.; Park, H.S.; Kim, M.-K.; Kwak, J.Y.; et al. Pulmonary actinomycosis during the first decade of 21st century: Cases of 94 patients. BMC Infect. Dis. 2013, 13, 216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bennhoff, D.F. Actinomycosis: Diagnostic and therapeutic considerations and a review of 32 cases. Laryngoscope 1984, 94, 1198–1217. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Zhang, H.; Wu, D.; Feng, M.; Yang, P.; Hu, X.; Tattevin, P.; Hong, G.; Chen, R.; Qiu, C. Pulmonary lesions associated with sputum culture-positive actinomycetes: Report of one case. Ann. Transl. Med. 2019, 7, 793. [Google Scholar] [CrossRef] [PubMed]
- Grzywa-Celińska, A.; Emeryk-Maksymiuk, J.; Szmygin-Milanowska, K.; Czekajska-Chehab, E.; Milanowski, J. Pulmonary actinomycosis—The great imitator. Ann. Agric. Environ. Med. 2018, 25, 211–212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McHugh, K.E.; Sturgis, C.D.; Procop, G.W.; Rhoads, D.D. The cytopathology of Actinomyces, Nocardia, and their mimickers. Diagn. Cytopathol. 2017, 45, 1105–1115. [Google Scholar] [CrossRef]
- Song, J.-U.; Park, H.; Jeon, K.; Um, S.-W.; Kwon, J.; Koh, W.-J. Treatment of thoracic actinomycosis: A retrospective analysis of 40 patients. Ann. Thorac. Med. 2010, 5, 80–85. [Google Scholar]
- Higashi, Y.; Nakamura, S.; Ashizawa, N.; Oshima, K.; Tanaka, A.; Miyazaki, T.; Izumikawa, K.; Yanagihara, K.; Yamamoto, Y.; Miyazak, Y.; et al. Pulmonary Actinomycosis Mimicking Pulmonary Aspergilloma and a Brief Review of the Literature. Intern. Med. 2017, 56, 449–453. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Test | Reference Ranges in Adults | On Admission | At Discharge |
|---|---|---|---|
| Leukocytes (×109/L) | 3.5–10.5 | 22.2 | 10.8 |
| Neutrophils (×109/L) | 1.40–6.50 | 20.7 | 7.6 |
| Lymphocytes (×109/L) | 1.20–3.40 | 0.4 | 1.6 |
| Monocytes (×109/L) | 0.00–1.00 | 1.1 | 1 |
| Eosinophils (×109/L) | 0.00–0.70 | 0 | 0.6 |
| Basophils (×109/L) | 0.00–0.20 | 0 | 0 |
| Hemoglobin (g/dL) | 12.00–17.00 | 12.2 | 9.6 |
| Hematocrit (%) | 36.00–54.00 | 36.6 | 28.4 |
| Mean corpuscular volume (MCV) (fL) | 80.00–100.00 | 88.5 | 88.9 |
| Mean corpuscular hemoglobin (MCH) (pg) | 27.00–33.00 | 28.7 | 30.1 |
| Mean corpuscular hemoglobin concentration (MCVC) (g/dl) | 32.00–36.00 | 32.4 | 33.9 |
| Platelet count (×109/L) | 130–450 | 315 | 256 |
| Urea nitrogen (mg/dL) | 7–18 | 11 | 8 |
| Creatinine (mg/dl) | 0.70–1.20 | 0.5 | 0.52 |
| Sodium (mmol/L) | 137–145 | 142 | 143 |
| Potassium (mmol/L) | 3.60–5.00 | 3.9 | 3.8 |
| Chloride (mmol/L) | 98–107 | 106 | 106 |
| pH | 7.35–7.45 | 7.37 | 7.48 |
| PO2 (mmHg) | 90.00–100.00 | 155 | 48 |
| PCO2 (mmHg) | 35.00–45.00 | 31 | 33 |
| HCO3 (mmol/L) | 22–28 | 31 | 33 |
| FIO2 (%) | - | 50 | 21 |
| Lactic acid (mmol/L) | 0.50–1.60 | 0.6 | 0.9 |
| Glucose, fasting (plasma) (mg/dL) | 65.00–105.00 | 103 | 85 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chaves, J.J.; Polo Nieto, F.; Gómez-Gómez, M.; Fierro Rodríguez, D.; García-Concha, D.; Parra-Medina, R. Pulmonary Sequestration Associated with Actinomycosis: A Case Report. Antibiotics 2020, 9, 687. https://doi.org/10.3390/antibiotics9100687
Chaves JJ, Polo Nieto F, Gómez-Gómez M, Fierro Rodríguez D, García-Concha D, Parra-Medina R. Pulmonary Sequestration Associated with Actinomycosis: A Case Report. Antibiotics. 2020; 9(10):687. https://doi.org/10.3390/antibiotics9100687
Chicago/Turabian StyleChaves, Juan José, Fernando Polo Nieto, María Gómez-Gómez, Diana Fierro Rodríguez, Daniel García-Concha, and Rafael Parra-Medina. 2020. "Pulmonary Sequestration Associated with Actinomycosis: A Case Report" Antibiotics 9, no. 10: 687. https://doi.org/10.3390/antibiotics9100687