COVID-19: Current Developments and Further Opportunities in Drug Delivery and Therapeutics

 ,
,
Abstract
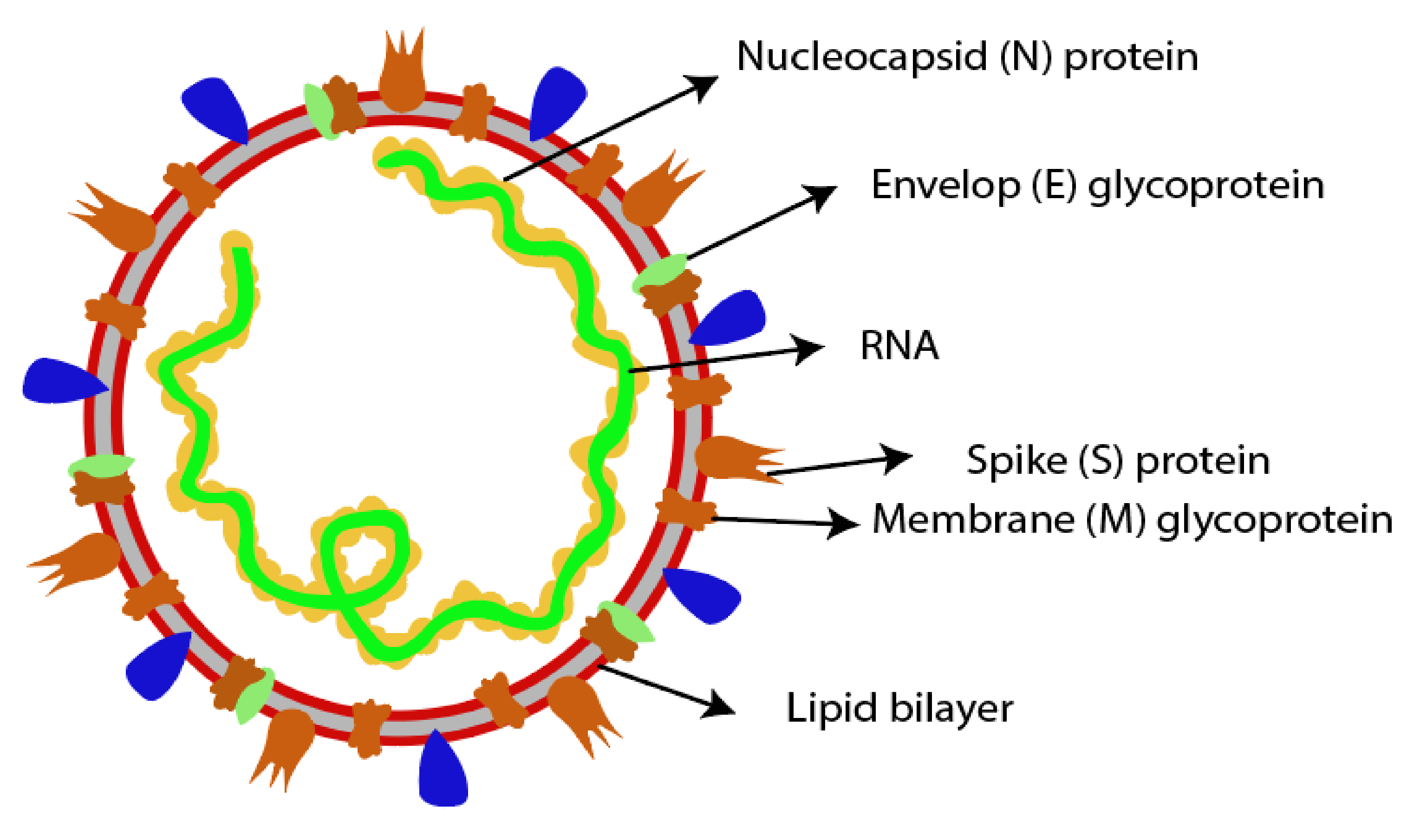
:1. Introduction to Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Infection
2. Transmission
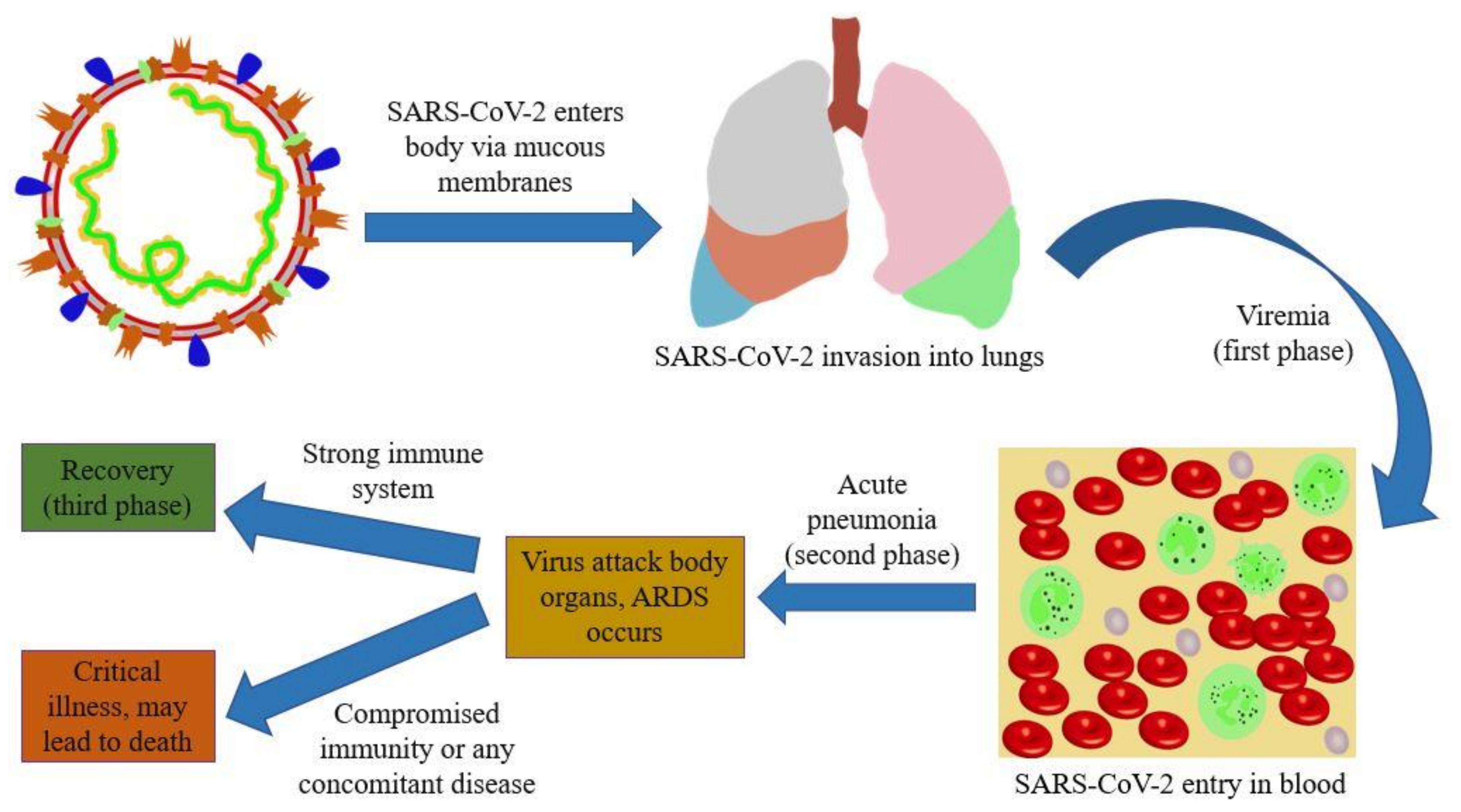
3. Pathogenesis
4. Diagnosis and Symptoms
5. Prevention
6. Pharmacologic Treatments
6.1. Antiviral Therapy

{kind=link}
{kind=link}
| Antiviral Agent | Mechanism of Action | Activity Against SARS-CoV-2 | FDA Pregnancy Category | Usage in Renal Dysfunction | Usage in Hepatic Dysfunction | References |
|---|---|---|---|---|---|---|
| Lopinavir/Ritonavir | Inhibits 3CLpro protease activity of virus | Reduced viral loads | C (lopinavir), B (ritonavir) | + | ++ | [69,70,71] |
| Remdesivir | Inhibitor of DNA/RNA polymerases, competes with ATP substrate for inclusion into nascent RNA chains resulting into delayed chain termination during viral RNA replication | Inhibited SARS-CoV-2 in-vitro, shortened the time to recovery | ** | +++ | +++ | [71] |
| Ribavirin | Interferes with DNA/RNA replication, interferes with RNA capping, inhibits natural guanosine production | Showed activity against SARS-CoV-2 in-vitro | X | ## | + | [72,73,74,75,76] |
| IFN-α | Inhibits viral synthesis, elicits natural immune responses | Used in combination with lopinavir/ritonavir and favipiravir against virus | C | + | Not recommended in patients suffering from autoimmune hepatitis, decompensated liver disease | [77,78] |
| Favipiravir | Perceived as a purine nucleotide, mistakenly, by the viral RNA polymerase | Inhibited virus in-vitro, rapid viral clearance and better treatment effects on infected individuals | ** | + | ## (in severe impairment) | [71] |
| Arbidol | Impedes virus-mediated fusion, inhibits viral invasion into the target cells, targets S-protein of SARS-CoV-2 and impedes its trimerization | Reduced mortality, its post-exposure prophylaxis served as a protective factor against COVID-19 development, showed antiviral effects against virus in combination with lopinavir/ritonavir | ** | ++ (in severe impairment) | ++ | [71] |
| Chloroquine phosphate | Inhibits viral infection by raising endosomal pH needed for cell fusion, interferes with the glycosylation of cellular receptors | Showed activity against SARS-CoV-2 in-vitro | ** | ## | ++ | [71,79] |
| Hydroxy- chloroquine | Possibly resembles chloroquine | Exhibited superior potency compared to chloroquine in-vitro, reduced the time to recovery, promoted the absorption of pneumonia | ** | ## | ++ | [71,80] |
6.2. Plasma Therapy
6.3. Anti-Inflammatory Therapy
6.4. Antimicrobial Therapy
6.5. Anticoagulant Therapy
7. Immunization
7.1. Potential Vaccine Targets
7.2. Vaccines under Development
8. Routes to Coronavirus Vaccine Delivery
8.1. Parenteral Immunization
8.2. Transcutaneous Immunization
8.3. Mucosal Immunization
9. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Cherry, J.D.; Krogstad, P. SARS: The First Pandemic of the 21st Century. Pediatr. Res. 2004, 56, 1–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barry, M.; Phan, M.V.T.; Akkielah, L.; Al-Majed, F.; Alhetheel, A.; Somily, A.M.; Alsubaie, S.S.; McNabb, S.J.; Cotten, M.; Zumla, A.; et al. Nosocomial outbreak of the Middle East Respiratory Syndrome coronavirus: A phylogenetic, epidemiological, clinical and infection control analysis. Travel Med. Infect. Dis. 2020, 395, 1063–1077. [Google Scholar] [CrossRef] [PubMed]
- Tu, Y.-F.; Chien, C.-S.; Yarmishyn, A.A.; Lin, Y.-Y.; Luo, Y.-H.; Lin, Y.-T.; Lai, W.-Y.; Yang, D.-M.; Chou, S.-J.; Yang, Y.-P.; et al. A Review of SARS-CoV-2 and the Ongoing Clinical Trials. Int. J. Mol. Sci. 2020, 21, 2657. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Law, S.; Leung, A.W.; Xu, C. Severe acute respiratory syndrome (SARS) and coronavirus disease-2019 (COVID-19): From causes to preventions in Hong Kong. Int. J. Infect. Dis. 2020, 94, 156–163. [Google Scholar] [CrossRef]
- De Felice, F.G.; Tovar-Moll, F.; Moll, J.; Munoz, D.P.; Ferreira, S.T. Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) and the Central Nervous System. Trends Neurosci. 2020, 43, 355–357. [Google Scholar] [CrossRef]
- Yuki, K.; Fujiogi, M.; Koutsogiannaki, S. COVID-19 pathophysiology: A review. Clin. Immunol. 2020, 215, 108427. [Google Scholar] [CrossRef]
- Gengler, I.; Wang, J.C.; Speth, M.M.; Sedaghat, A.R.; Sedaghat, A.R. Sinonasal pathophysiology of SARS-CoV -2 and COVID -19: A systematic review of the current evidence. Laryngoscope 2020, 5, 354–359. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 28 September 2020).
- Petersen, E.; Koopmans, M.; Go, U.; Hamer, D.H.; Petrosillo, N.; Castelli, F.; Storgaard, M.; Al Khalili, S.; Simonsen, L. Comparing SARS-CoV-2 with SARS-CoV and influenza pandemics. Lancet Infect. Dis. 2020, 20, E238–E244. [Google Scholar] [CrossRef]
- Andersen, K.G.; Rambaut, A.; Lipkin, W.I.; Holmes, E.C.; Garry, R.F. The proximal origin of SARS-CoV-2. Nat. Med. 2020, 26, 450–452. [Google Scholar] [CrossRef] [Green Version]
- Wu, D.; Wu, T.-T.; Liu, Q.; Yang, Z. The SARS-CoV-2 outbreak: What we know. Int. J. Infect. Dis. 2020, 94, 44–48. [Google Scholar] [CrossRef]
- Rothan, H.A.; Byrareddy, S.N. The epidemiology and pathogenesis of coronavirus disease (COVID-19) outbreak. J. Autoimmun. 2020, 109, 102433. [Google Scholar] [CrossRef]
- Meselson, M. Droplets and Aerosols in the Transmission of SARS-CoV-2. N. Engl. J. Med. 2020, 382, 2063. [Google Scholar] [CrossRef]
- World Health Organization. Available online: https://www.who.int/news-room/commentaries/detail/modes-of-transmission-of-virus-causing-covid-19-implications-for-ipc-precaution-recommendations (accessed on 5 September 2020).
- World Health Organization. Available online: https://www.who.int/news-room/commentaries/detail/transmission-of-sars-cov-2-implications-for-infection-prevention-precautions (accessed on 5 September 2020).
- Khan, S.; Liu, J.; Xue, M. Transmission of SARS-CoV-2, Required Developments in Research and Associated Public Health Concerns. Front. Med. 2020, 7, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Vivanti, A.J.; Vauloup-Fellous, C.; Prevot, S.; Zupan, V.; Suffee, C.; Cao, J.D.; Benachi, A.; De Luca, D. Transplacental transmission of SARS-CoV-2 infection. Nat. Commun. 2020, 11, 3572. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.; Lu, L.; Cao, W.; Li, T. Hypothesis for potential pathogenesis of SARS-CoV-2 infection–a review of immune changes in patients with viral pneumonia. Emerg. Microbes Infect. 2020, 9, 727–732. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Centers for Disease Control and Prevention. Available online: https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/people-with-medical-conditions.html (accessed on 9 September 2020).
- Centers for Disease Control and Prevention. Available online: https://www.cdc.gov/coronavirus/2019-ncov/covid-data/investigations-discovery/assessing-risk-factors.html (accessed on 9 September 2020).
- Guan, W.-J.; Liang, W.-H.; Zhao, Y.; Liang, H.-R.; Chen, Z.-S.; Li, Y.-M.; Liu, X.-Q.; Chen, R.-C.; Tang, C.-L.; Wang, T.; et al. Comorbidity and its impact on 1590 patients with COVID-19 in China: A nationwide analysis. Eur. Respir. J. 2020, 55, 2000547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jain, V.; Yuan, J.-M. Predictive symptoms and comorbidities for severe COVID-19 and intensive care unit admission: A systematic review and meta-analysis. Int. J. Public Health 2020, 1–14. [Google Scholar] [CrossRef]
- Rokni, M.; Ghasemi, V.; Tavakoli, Z. Immune responses and pathogenesis of SARS-CoV -2 during an outbreak in Iran: Comparison with SARS and MERS. Rev. Med Virol. 2020, 30, 2107. [Google Scholar] [CrossRef] [Green Version]
- Li, G.; Fan, Y.; Lai, Y.; Han, T.; Li, Z.; Zhou, P.; Pan, P.; Wang, W.; Hu, D.; Liu, X.; et al. Coronavirus infections and immune responses. J. Med Virol. 2020, 92, 424–432. [Google Scholar] [CrossRef]
- Cox, R.J.; Brokstad, K.A. Not just antibodies: B cells and T cells mediate immunity to COVID-19. Nat. Rev. Immunol. 2020, 1–2. [Google Scholar] [CrossRef]
- Technology Networks. Available online: https://www.technologynetworks.com/immunology/news/sars-cov-2-immunity-likely-to-be-higher-than-antibody-testing-has-shown-336861 (accessed on 11 September 2020).
- Biorxiv. Available online: https://www.biorxiv.org/content/10.1101/2020.06.29.174888v1 (accessed on 11 September 2020).
- Chen, Z.; Wherry, E.J. T cell responses in patients with COVID-19. Nat. Rev. Immunol. 2020, 20, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Mason, R.J. Pathogenesis of COVID-19 from a cell biology perspective. Eur. Respir. J. 2020, 55, 2000607. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, H.; Liu, L.; Zhang, D.; Xu, J.; Dai, H.; Tang, N.; Su, X.; Cao, B. SARS-CoV-2 and viral sepsis: Observations and hypotheses. Lancet 2020, 395, 1517–1520. [Google Scholar] [CrossRef]
- To, K.K.-W.; Hung, I.F.-N.; Ip, J.D.; Chu, A.W.-H.; Chan, W.-M.; Tam, A.R.; Fong, C.H.-Y.; Yuan, S.; Tsoi, H.-W.; Ng, A.C.-K.; et al. COVID-19 re-infection by a phylogenetically distinct SARS-coronavirus-2 strain confirmed by whole genome sequencing. Clin. Infect. Dis. 2020, 1275. [Google Scholar] [CrossRef] [PubMed]
- Adhikari, S.P.; Meng, S.; Wu, Y.-J.; Mao, Y.-P.; Ye, R.-X.; Wang, Q.-Z.; Sun, C.; Sylvia, S.; Rozelle, S.; Raat, H.; et al. Epidemiology, causes, clinical manifestation and diagnosis, prevention and control of coronavirus disease (COVID-19) during the early outbreak period: A scoping review. Infect. Dis. Poverty 2020, 9, 12–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Available online: https://apps.who.int/iris/handle/10665/332196 (accessed on 5 September 2020).
- World Health Organization. Available online: https://apps.who.int/iris/handle/10665/333752 (accessed on 5 September 2020).
- Castagnoli, R.; Votto, M.; Licari, A.; Brambilla, I.; Bruno, R.; Perlini, S.; Rovida, F.; Baldanti, F.; Marseglia, G.L. Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Infection in Children and Adolescents: A Systematic Review. JAMA Pediatr 2020, 174, 882–889. [Google Scholar] [CrossRef] [Green Version]
- Sharma, A.; Tiwari, S.; Deb, M.K.; Marty, J.L. Severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2): A global pandemic and treatment strategies. Int. J. Antimicrob. Agents 2020, 56, 106054. [Google Scholar] [CrossRef]
- Zheng, J. SARS-CoV-2: An Emerging Coronavirus that Causes a Global Threat. Int. J. Biol. Sci. 2020, 16, 1678–1685. [Google Scholar] [CrossRef] [Green Version]
- Morawska, L.; Cao, J. Airborne transmission of SARS-CoV-2: The world should face the reality. Environ. Int. 2020, 139, 105730. [Google Scholar] [CrossRef]
- World Health Organization. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public (accessed on 5 August 2020).
- Jin, Y.-H.; Cai, L.; Cheng, Z.-S.; Cheng, H.; Deng, T.; Fan, Y.-P.; Fang, C.; Huang, D.; Huang, L.-Q.; Huang, Q.; et al. A rapid advice guideline for the diagnosis and treatment of 2019 novel coronavirus (2019-nCoV) infected pneumonia (standard version). Mil. Med Res. 2020, 7, 1–23. [Google Scholar] [CrossRef] [Green Version]
- Mahase, E. Covid-19: What is the R number? BMJ 2020, 369, m1891. [Google Scholar] [PubMed]
- Anderson, R.M.; Heesterbeek, H.; Klinkenberg, D.; Hollingsworth, T.D. How will country-based mitigation measures influence the course of the COVID-19 epidemic? Lancet 2020, 395, 931–934. [Google Scholar] [CrossRef]
- E Kretzschmar, M.; Rozhnova, G.; Bootsma, M.C.J.; Van Boven, M.; Van De Wijgert, J.H.H.M.; Bonten, M.J.M. Impact of delays on effectiveness of contact tracing strategies for COVID-19: A modelling study. Lancet Public Health 2020, 5, e452–e459. [Google Scholar] [CrossRef]
- World Health Organization. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public/myth-busters?gclid=EAIaIQobChMIyIXp8rTU6wIVmKztCh1SbAm9EAAYASAAEgKEbvD_BwE#climate (accessed on 6 September 2020).
- Sanyaolu, A.; Okorie, C.; Marinkovic, A.; Patidar, R.; Younis, K.; Desai, P.; Hosein, Z.; Padda, I.; Mangat, J.; Altaf, M. Comorbidity and its Impact on Patients with COVID-19. SN Compr. Clin. Med. 2020, 2, 1069–1076. [Google Scholar] [CrossRef]
- Bhatraju, P.K.; Ghassemieh, B.J.; Nichols, M.; Kim, R.; Jerome, K.R.; Nalla, A.K.; Greninger, A.L.; Pipavath, S.; Wurfel, M.M.; Evans, L.; et al. Covid-19 in Critically Ill Patients in the Seattle Region—Case Series. N. Engl. J. Med. 2020, 382, 2012–2022. [Google Scholar] [CrossRef]
- Andersen, P.I.; Ianevski, A.; Lysvand, H.; Vitkauskiene, A.; Oksenych, V.; Bjørås, M.; Telling, K.; Lutsar, I.; Dumpis, U.; Irie, Y.; et al. Discovery and development of safe-in-man broad-spectrum antiviral agents. Int. J. Infect. Dis. 2020, 93, 268–276. [Google Scholar] [CrossRef]
- Yang, C.-W.; Peng, T.-T.; Hsu, H.-Y.; Lee, Y.-Z.; Wu, S.-H.; Lin, W.-H.; Ke, Y.-Y.; Hsu, T.-A.; Yeh, T.-K.; Huang, W.-Z.; et al. Repurposing old drugs as antiviral agents for coronaviruses. Biomed. J. 2020. [Google Scholar] [CrossRef]
- Sayad, B.; Sobhani, M.; Khodarahmi, R. Sofosbuvir as Repurposed Antiviral Drug Against COVID-19: Why Were We Convinced to Evaluate the Drug in a Registered/Approved Clinical Trial? Arch. Med Res. 2020, 51, 577–581. [Google Scholar] [CrossRef]
- Mahmoud, D.B.; Shitu, Z.; Mostafa, A. Drug repurposing of nitazoxanide: Can it be an effective therapy for COVID-19? J. Genet. Eng. Biotechnol. 2020, 18, 1–10. [Google Scholar] [CrossRef]
- Guo, G.; Ye, L.; Pan, K.; Chen, Y.; Xing, D.; Yan, K.; Chen, Z.; Ding, N.; Li, W.; Huang, H.; et al. New Insights of Emerging SARS-CoV-2: Epidemiology, Etiology, Clinical Features, Clinical Treatment, and Prevention. Front. Cell Dev. Biol. 2020, 8, 1–22. [Google Scholar] [CrossRef]
- Cinatl, J., Jr.; Michaelis, M.; Hoever, G.; Preiser, W.; Doerr, H.W. Development of antiviral therapy for severe acute respiratory syndrome. Antivir. Res. 2005, 66, 81–97. [Google Scholar] [CrossRef] [PubMed]
- Cao, B.; Wang, Y.; Wen, D.; Liu, W.; Wang, J.; Fan, G.; Ruan, L.; Song, B.; Cai, Y.; Wei, M.; et al. A Trial of Lopinavir–Ritonavir in Adults Hospitalized with Severe Covid-19. N. Engl. J. Med. 2020, 382, 1787–1799. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.; Cao, R.; Zhang, L.; Yang, X.; Liu, J.; Xu, M.; Shi, Z.; Hu, Z.; Zhong, W.; Xiao, G. Remdesivir and chloroquine effectively inhibit the recently emerged novel coronavirus (2019-nCoV) in vitro. Cell Res. 2020, 30, 269–271. [Google Scholar] [CrossRef] [PubMed]
- U.S. Food & Drug Administration. Available online: https://www.fda.gov/news-events/press-announcements/covid-19-update-fda-broadens-emergency-use-authorization-veklury-remdesivir-include-all-hospitalized (accessed on 28 September 2020).
- Sheahan, T.P.; Sims, A.C.; Graham, R.L.; Menachery, V.D.; Gralinski, L.E.; Case, J.B.; Leist, S.R.; Pyrc, K.; Feng, J.Y.; Trantcheva, I.; et al. Broad-spectrum antiviral GS-5734 inhibits both epidemic and zoonotic coronaviruses. Sci. Transl. Med. 2017, 9, eaal3653. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jean, S.-S.; Lee, P.-I.; Hsueh, P.-R. Treatment options for COVID-19: The reality and challenges. J. Microbiol. Immunol. Infect. 2020, 53, 436–443. [Google Scholar] [CrossRef]
- Sheahan, T.P.; Sims, A.C.; Leist, S.R.; Schäfer, A.; Won, J.; Brown, A.J.; Montgomery, S.A.; Hogg, A.; Babusis, D.; Clarke, M.O.; et al. Comparative therapeutic efficacy of remdesivir and combination lopinavir, ritonavir, and interferon beta against MERS-CoV. Nat. Commun. 2020, 11, 14–222. [Google Scholar] [CrossRef] [Green Version]
- Hung, I.F.-N.; Lung, K.-C.; Tso, E.Y.-K.; Liu, R.; Chung, T.W.-H.; Chu, M.-Y.; Ng, Y.-Y.; Lo, J.; Chan, J.; Tam, A.R.; et al. Triple combination of interferon beta-1b, lopinavir–ritonavir, and ribavirin in the treatment of patients admitted to hospital with COVID-19: An open-label, randomised, phase 2 trial. Lancet 2020, 395, 1695–1704. [Google Scholar] [CrossRef]
- De Clercq, E. New Nucleoside Analogues for the Treatment of Hemorrhagic Fever Virus Infections. Chem. Asian J. 2019, 14, 3962–3968. [Google Scholar] [CrossRef]
- Cai, Q.; Yang, M.; Liu, D.; Chen, J.; Shu, D.; Xia, J.; Liao, X.; Gu, Y.; Cai, Q.; Yang, Y.; et al. Experimental Treatment with Favipiravir for COVID-19: An Open-Label Control Study. Engineering 2020. [Google Scholar] [CrossRef]
- Delang, L.; Neyts, J. Medical treatment options for COVID-19. Eur. Hear. J. Acute Cardiovasc. Care 2020, 9, 209–214. [Google Scholar] [CrossRef]
- Lai, C.-C.; Shih, T.-P.; Ko, W.-C.; Tang, H.-J.; Hsueh, P.-R. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and corona virus disease-2019 (COVID-19): The epidemic and the challenges. Int. J. Antimicrob. Agents 2020, 55, 105924. [Google Scholar] [CrossRef] [PubMed]
- Ferner, R.E.; Aronson, J.K. Chloroquine and hydroxychloroquine in covid-19. BMJ 2020, 369, m1432. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- British Broadcasting Corporation. Available online: https://www.bbc.com/news/51980731 (accessed on 5 August 2020).
- U.S. Food & Drug Administration. Available online: https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-revokes-emergency-use-authorization-chloroquine-and (accessed on 28 September 2020).
- World Heallth Organization. Available online: https://www.who.int/publications/m/item/targeted-update-safety-and-efficacy-of-hydroxychloroquine-or-chloroquine-for-treatment-of-covid-19 (accessed on 6 September 2020).
- Jeevaratnam, K. Chloroquine and hydroxychloroquine for COVID-19: Implications for cardiac safety. Eur. Hear. J. Cardiovasc. Pharmacother. 2020, 6, 256–257. [Google Scholar] [CrossRef] [PubMed]
- U.S. Food & Drug Administration. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2013/021226s038lbl.pdf (accessed on 10 September 2020).
- Drugs.com. Available online: https://www.drugs.com/pregnancy/ritonavir.html (accessed on 10 September 2020).
- Li, L.; Wang, X.; Wang, R.; Hu, Y.; Jiang, S.; Lu, X. Antiviral Agent Therapy Optimization in Special Populations of COVID-19 Patients. Drug Des. Dev. Ther. 2020, 14, 3001–3013. [Google Scholar] [CrossRef] [PubMed]
- Graci, J.D.; Cameron, C.E. Mechanisms of action of ribavirin against distinct viruses. Rev. Med Virol. 2005, 16, 37–48. [Google Scholar] [CrossRef] [PubMed]
- Guardigni, V.; Badia, L.; Conti, M.; Rinaldi, M.; Mancini, R.; Viale, P.; Verucchi, G. Liver decompensation predicts ribavirin overexposure in hepatitis C virus patients treated with direct-acting antivirals. World J. Hepatol. 2017, 9, 1270–1277. [Google Scholar] [CrossRef]
- Khalili, J.S.; Zhu, H.; Mak, N.S.A.; Yan, Y.; Zhu, Y. Novel coronavirus treatment with ribavirin: Groundwork for an evaluation concerning COVID-19. J. Med Virol. 2020, 92, 740–746. [Google Scholar] [CrossRef] [Green Version]
- Roberts, S.S. Assessing Ribavirin Exposure during Pregnancy: The ribavirin pregnancy registry. Gastroenterol. Nurs. 2008, 31, 413–417. [Google Scholar] [CrossRef]
- Sinclair, S.M.; Jones, J.K.; Miller, R.K.; Greene, M.F.; Kwo, P.Y.; Maddrey, W.C. The Ribavirin Pregnancy Registry: An Interim Analysis of Potential Teratogenicity at the Mid-Point of Enrollment. Drug Saf. 2017, 40, 1205–1218. [Google Scholar] [CrossRef]
- Beauverd, Y.; Radia, D.; Cargo, C.; Knapper, S.; Drummond, M.; Pillai, A.; Harrison, C.; E Robinson, S. Pegylated interferon alpha-2a for essential thrombocythemia during pregnancy: Outcome and safety. A case series. Haematol. 2016, 101, e182–e184. [Google Scholar] [CrossRef] [Green Version]
- Rheem, J.; Sundaram, V.; Saab, S. Antiviral Therapy in Elderly Patients with Hepatitis C Virus Infection. Gastroenterol. Hepatol. 2015, 11, 294–346. [Google Scholar]
- U.S. Food & Drug Administration. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/006002s044lbl.pdf (accessed on 2 October 2020).
- U.S. Food & Drug Administration. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/009768s037s045s047lbl.pdf (accessed on 2 October 2020).
- U.S. Food & Drug Administration. Available online: https://www.fda.gov/news-events/press-announcements/fda-issues-emergency-use-authorization-convalescent-plasma-potential-promising-covid-19-treatment (accessed on 28 September 2020).
- MedRXiv. Available online: https://www.medrxiv.org/content/10.1101/2020.02.12.20021386v1 (accessed on 5 August 2020).
- Ye, M.; Fu, D.; Ren, Y.; Wang, F.; Wang, D.; Zhang, F.; Xia, X.; Lv, T.-F. Treatment with convalescent plasma for COVID-19 patients in Wuhan, China. J. Med Virol. 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, Q.; He, Y. Challenges of Convalescent Plasma Therapy on COVID-19. J. Clin. Virol. 2020, 127, 104358. [Google Scholar] [CrossRef] [PubMed]
- Health.mil. Available online: https://www.health.mil/News/Articles/2020/06/19/Understanding-the-potential-of-COVID-19-convalescent-plasma (accessed on 5 September 2020).
- Zhang, W.; Zhao, Y.; Zhang, F.; Wang, Q.; Li, T.; Liu, Z.; Wang, J.; Qin, Y.; Zhang, X.; Yan, X.; et al. The use of anti-inflammatory drugs in the treatment of people with severe coronavirus disease 2019 (COVID-19): The Perspectives of clinical immunologists from China. Clin. Immunol. 2020, 214, 108393. [Google Scholar] [CrossRef]
- World Health Organization. Available online: https://www.who.int/publications/m/item/scientific-brief-on-the-use-of-non-steroidal-anti-inflammatory-drugs-(nsaid)-in-patients-with-covid-19 (accessed on 6 September 2020).
- Moore, N.; Carleton, B.; Blin, P.; Bosco-Levy, P.; Droz, C. Does ibuprofen worsen COVID-19? Drug Saf. 2020, 43, 611–614. [Google Scholar] [CrossRef]
- Capuano, A.; Scavone, C.; Racagni, G.; Scaglione, F.; Pharmacology, I.S.O. NSAIDs in patients with viral infections, including Covid-19: Victims or perpetrators? Pharmacol. Res. 2020, 157, 104849. [Google Scholar] [CrossRef]
- Mattos-Silva, P.; Felix, N.S.; Silva, P.L.; Robba, C.; Battaglini, D.; Pelosi, P.; Rocco, P.R.M.; Cruz, F.F. Pros and cons of corticosteroid therapy for COVID-19 patients. Respir. Physiol. Neurobiol. 2020, 280, 103492. [Google Scholar] [CrossRef]
- The RECOVERY Collaborative Group; Horby, P.; Lim, W.S.; Emberson, J.R.; Mafham, M.; Bell, J.L.; Linsell, L.; Staplin, N.; Brightling, C.; Ustianowski, A.; et al. Dexamethasone in Hospitalized Patients with Covid-19—Preliminary Report. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef]
- Rawson, T.M.; Moore, L.S.P.; Zhu, N.; Ranganathan, N.; Skolimowska, K.; Gilchrist, M.; Satta, G.; Cooke, G.; Holmes, A. Bacterial and Fungal Coinfection in Individuals with Coronavirus: A Rapid Review To Support COVID-19 Antimicrobial Prescribing. Clin. Infect. Dis. 2020, 530. [Google Scholar] [CrossRef]
- Atallah, B.; Mallah, S.I.; Almahmeed, W. Anticoagulation in COVID-19. Eur. Hear. J. Cardiovasc. Pharmacother. 2020. [Google Scholar] [CrossRef]
- Barnes, G.D.; Burnett, A.; Allen, A.; Blumenstein, M.; Clark, N.P.; Cuker, A.; Dager, W.E.; Deitelzweig, S.B.; Ellsworth, S.; Garcia, D.; et al. Thromboembolism and anticoagulant therapy during the COVID-19 pandemic: Interim clinical guidance from the anticoagulation forum. J. Thromb. Thrombolysis 2020, 50, 72–81. [Google Scholar] [CrossRef] [PubMed]
- Kollias, A.; Kyriakoulis, K.G.; Dimakakos, E.; Poulakou, G.; Stergiou, G.S.; Syrigos, K. Thromboembolic risk and anticoagulant therapy in COVID-19 patients: Emerging evidence and call for action. Br. J. Haematol. 2020, 189, 846–847. [Google Scholar] [CrossRef] [PubMed]
- Connors, J.M.; Levy, J.H. COVID-19 and its implications for thrombosis and anticoagulation. Blood 2020, 135, 2033–2040. [Google Scholar] [CrossRef] [PubMed]
- Karande, P.; Mitragotri, S. Transcutaneous Immunization: An Overview of Advantages, Disease Targets, Vaccines, and Delivery Technologies. Annu. Rev. Chem. Biomol. Eng. 2010, 1, 175–201. [Google Scholar] [CrossRef]
- Ventola, C.L. The Antibiotic Resistance Crisis. Part 1: Causes and threats. Pharm. Ther. 2015, 40, 277–283. [Google Scholar]
- Findlater, A.R.; Bogoch, I.I. Human Mobility and the Global Spread of Infectious Diseases: A Focus on Air Travel. Trends Parasitol. 2018, 34, 772–783. [Google Scholar] [CrossRef]
- Hui, E.K.-W. Reasons for the increase in emerging and re-emerging viral infectious diseases. Microbes Infect. 2006, 8, 905–916. [Google Scholar] [CrossRef]
- Zhang, J.; Zeng, H.; Gu, J.; Li, H.-B.; Zheng, L.; Zou, Q.-M. Progress and Prospects on Vaccine Development against SARS-CoV-2. Vaccines 2020, 8, 153. [Google Scholar] [CrossRef] [Green Version]
- Shereen, M.A.; Khan, S.; Kazmi, A.; Bashir, N.; Siddique, R. COVID-19 infection: Origin, transmission, and characteristics of human coronaviruses. J. Adv. Res. 2020, 24, 91–98. [Google Scholar] [CrossRef]
- Salvatori, G.; Luberto, L.; Maffei, M.; Aurisicchio, L.; Roscilli, G.; Palombo, F.; Marra, E. SARS-CoV-2 SPIKE PROTEIN: An optimal immunological target for vaccines. J. Transl. Med. 2020, 18, 1–3. [Google Scholar] [CrossRef]
- Ou, X.; Liu, Y.; Lei, X.; Li, P.; Mi, D.; Ren, L.; Guo, L.; Guo, R.; Chen, T.; Hu, J.; et al. Characterization of spike glycoprotein of SARS-CoV-2 on virus entry and its immune cross-reactivity with SARS-CoV. Nat. Commun. 2020, 11, 1612–1620. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lan, J.; Ge, J.; Yu, J.; Shan, S.; Zhou, H.; Fan, S.; Zhang, Q.; Shi, X.; Wang, Q.; Zhang, L.; et al. Structure of the SARS-CoV-2 spike receptor-binding domain bound to the ACE2 receptor. Nature 2020, 581, 215–220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muthumani, K.; Falzarano, D.; Reuschel, E.L.; Tingey, C.; Flingai, S.; Villarreal, D.O.; Wise, M.; Patel, A.; Izmirly, A.; Aljuaid, A.; et al. A synthetic consensus anti–spike protein DNA vaccine induces protective immunity against Middle East respiratory syndrome coronavirus in nonhuman primates. Sci. Transl. Med. 2015, 7, 301ra132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adney, D.R.; Wang, L.; Van Doremalen, N.; Shi, W.; Zhang, Y.; Kong, W.-P.; Miller, M.R.; Bushmaker, T.J.; Scott, D.; De Wit, E.; et al. Efficacy of an Adjuvanted Middle East Respiratory Syndrome Coronavirus Spike Protein Vaccine in Dromedary Camels and Alpacas. Viruses 2019, 11, 212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lan, J.; Yao, Y.; Deng, Y.; Chen, H.; Lu, G.; Wang, W.; Bao, L.; Deng, W.; Wei, Q.; Gao, G.F.; et al. Recombinant Receptor Binding Domain Protein Induces Partial Protective Immunity in Rhesus Macaques Against Middle East Respiratory Syndrome Coronavirus Challenge. EBioMedicine 2015, 2, 1438–1446. [Google Scholar] [CrossRef] [Green Version]
- Tian, X.; Li, C.; Huang, A.; Xia, S.; Lu, S.; Shi, Z.-L.; Lu, L.; Jiang, S.; Yang, Z.; Wu, Y.; et al. Potent binding of 2019 novel coronavirus spike protein by a SARS coronavirus-specific human monoclonal antibody. Emerg. Microbes Infect. 2020, 9, 382–385. [Google Scholar] [CrossRef] [Green Version]
- Lei, C.; Qian, K.; Li, T.; Zhang, S.; Fu, W.; Ding, M.; Hu, S. Neutralization of SARS-CoV-2 spike pseudotyped virus by recombinant ACE2-Ig. Nat. Commun. 2020, 11, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Kewan, T.; Covut, F.; Al–Jaghbeer, M.J.; Rose, L.; Gopalakrishna, K.; Akbik, B. Tocilizumab for treatment of patients with severe COVID–19: A retrospective cohort study. EClinicalMedicine 2020, 24, 100418. [Google Scholar] [CrossRef]
- Morena, V.; Milazzo, L.; Oreni, L.; Bestetti, G.; Fossali, T.; Bassoli, C.; Torre, A.; Cossu, M.V.; Minari, C.; Ballone, E.; et al. Off-label use of tocilizumab for the treatment of SARS-CoV-2 pneumonia in Milan, Italy. Eur. J. Intern. Med. 2020, 76, 36–42. [Google Scholar] [CrossRef]
- Xu, X.; Han, M.; Li, T.; Sun, W.; Wang, D.; Fu, B.; Zhou, Y.; Zheng, X.; Yang, Y.; Li, X.; et al. Effective treatment of severe COVID-19 patients with tocilizumab. Proc. Natl. Acad. Sci. USA 2020, 117, 10970–10975. [Google Scholar] [CrossRef]
- Chen, Y.; Lu, S.; Jia, H.; Deng, Y.; Zhou, J.; Huang, B.; Yu, Y.; Lan, J.; Wang, W.; Lou, Y.; et al. A novel neutralizing monoclonal antibody targeting the N-terminal domain of the MERS-CoV spike protein. Emerg. Microbes Infect. 2017, 6, e37. [Google Scholar] [CrossRef] [PubMed]
- Yoshimoto, F.K. The Proteins of Severe Acute Respiratory Syndrome Coronavirus-2 (SARS CoV-2 or n-COV19), the Cause of COVID-19. Protein J. 2020, 39, 198–216. [Google Scholar] [PubMed]
- Minor, P.D. Live attenuated vaccines: Historical successes and current challenges. Virology 2015, 479, 379–392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, N.; Shang, J.; Jiang, S.; Du, L. Subunit Vaccines against Emerging Pathogenic Human Coronaviruses. Front. Microbiol. 2020, 11, 298. [Google Scholar] [CrossRef]
- GSK. Available online: https://www.gsk.com/en-gb/media/press-releases/sanofi-and-gsk-initiate-phase-12-clinical-trial-of-covid-19-adjuvanted-recombinant-protein-based-vaccine-candidate/ (accessed on 9 September 2020).
- Sanofi. Available online: https://www.sanofi.com/en/media-room/press-releases/2020/2020-04-14-13-00-00 (accessed on 9 September 2020).
- Pardi, N.; Hogan, M.J.; Porter, F.W.; Weissman, D. mRNA vaccines—A new era in vaccinology. Nat. Rev. Drug Discov. 2018, 17, 261–279. [Google Scholar] [CrossRef] [Green Version]
- Liu, M.A. DNA vaccines: A review. J. Intern. Med. 2003, 253, 402–410. [Google Scholar] [CrossRef] [Green Version]
- Pachuk, C.J.; McCallus, D.E.; Weiner, D.B.; Satishchandran, C. DNA vaccines—Challenges in delivery. Curr. Opin. Mol. Ther. 2000, 2, 188–198. [Google Scholar]
- Lim, M.; Badruddoza, A.Z.M.; Firdous, J.; Azad, M.; Mannan, A.; Al-Hilal, T.A.; Cho, C.-S.; Islam, M.A. Engineered Nanodelivery Systems to Improve DNA Vaccine Technologies. Pharmaceutics 2020, 12, 30. [Google Scholar] [CrossRef] [Green Version]
- Zeng, C.; Zhang, C.; Walker, P.G.; Dong, Y. Formulation and Delivery Technologies for mRNA Vaccines. In Current Topics in Microbiology and Immunology; Springer: Berlin/Heidelberg, Germany, 2020. [Google Scholar]
- Zhang, C.; Maruggi, G.; Shan, H.; Li, J. Advances in mRNA Vaccines for Infectious Diseases. Front. Immunol. 2019, 10, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Karikó, K.; Muramatsu, H.; A Welsh, F.; Ludwig, J.; Kato, H.; Akira, S.; Weissman, D. Incorporation of Pseudouridine Into mRNA Yields Superior Nonimmunogenic Vector With Increased Translational Capacity and Biological Stability. Mol. Ther. 2008, 16, 1833–1840. [Google Scholar] [CrossRef]
- Pardi, N.; Hogan, M.J.; Naradikian, M.S.; Parkhouse, K.; Cain, D.W.; Jones, L.; Moody, M.A.; Verkerke, H.P.; Myles, A.; Willis, E.; et al. Nucleoside-modified mRNA vaccines induce potent T follicular helper and germinal center B cell responses. J. Exp. Med. 2018, 215, 1571–1588. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.-S.; Hsiao, Y.-S.; Lin, H.-H.; Liu, Y.; Chen, Y.-L. CpG-Modified Plasmid DNA Encoding Flagellin Improves Immunogenicity and Provides Protection against Burkholderia pseudomallei Infection in BALB/c Mice. Infect. Immun. 2006, 74, 1699–1705. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cui, Z. DNA vaccine. Adv. Genet. 2005, 54, 257–289. [Google Scholar] [CrossRef] [PubMed]
- Smith, H.A. Regulatory considerations for nucleic acid vaccines. Vaccine 1994, 12, 1515–1519. [Google Scholar] [CrossRef]
- Jackson, L.A.; Anderson, E.J.; Rouphael, N.G.; Roberts, P.C.; Makhene, M.; Coler, R.N.; McCullough, M.P.; Chappell, J.D.; Denison, M.R.; Stevens, L.J.; et al. An mRNA Vaccine against SARS-CoV-2—Preliminary Report. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef]
- Corbett, K.S.; Flynn, B.; Foulds, K.E.; Francica, J.R.; Boyoglu-Barnum, S.; Werner, A.P.; Flach, B.; O’Connell, S.; Bock, K.W.; Minai, M.; et al. Evaluation of the mRNA-1273 Vaccine against SARS-CoV-2 in Nonhuman Primates. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef]
- Keech, C.; Albert, G.; Cho, I.; Robertson, A.; Reed, P.; Neal, S.; Plested, J.S.; Zhu, M.; Cloney-Clark, S.; Zhou, H.; et al. Phase 1–2 trial of a SARS-CoV-2 recombinant spike protein nanoparticle vaccine. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef]
- World Health Organization. Available online: https://www.who.int/publications/m/item/draft-landscape-of-covid-19-candidate-vaccines (accessed on 13 September 2020).
- Ewer, K.J.; Sebastian, S.; Spencer, A.J.; Gilbert, S.C.; Hill, A.V.; Lambe, T. Chimpanzee adenoviral vectors as vaccines for outbreak pathogens. Hum. Vaccines Immunother. 2017, 13, 3020–3032. [Google Scholar] [CrossRef]
- Zhang, C.; Zhou, N. Adenoviral vector-based strategies against infectious disease and cancer. Hum. Vaccines Immunother. 2016, 12, 2064–2074. [Google Scholar] [CrossRef] [Green Version]
- Lee, C.S.; Bishop, E.S.; Zhang, R.; Yu, X.; Farina, E.M.; Yan, S.; Zhao, C.; Zeng, Z.; Shu, Y.; Wu, X.; et al. Adenovirus-mediated gene delivery: Potential applications for gene and cell-based therapies in the new era of personalized medicine. Genes Dis. 2017, 4, 43–63. [Google Scholar] [CrossRef]
- Alharbi, N.K.; Padron-Regalado, E.; Thompson, C.P.; Kupke, A.; Wells, D.; Sloan, M.A.; Grehan, K.; Temperton, N.J.; Lambe, T.; Warimwe, G.; et al. ChAdOx1 and MVA based vaccine candidates against MERS-CoV elicit neutralising antibodies and cellular immune responses in mice. Vaccine 2017, 35, 3780–3788. [Google Scholar] [CrossRef] [PubMed]
- Zhu, F.-C.; Guan, X.-H.; Li, Y.-H.; Huang, J.-Y.; Jiang, T.; Hou, L.-H.; Li, J.-X.; Yang, B.-F.; Wang, L.; Wang, W.-J.; et al. Immunogenicity and safety of a recombinant adenovirus type-5-vectored COVID-19 vaccine in healthy adults aged 18 years or older: A randomised, double-blind, placebo-controlled, phase 2 trial. Lancet 2020, 396, 479–488. [Google Scholar] [CrossRef]
- Folegatti, P.M.; Ewer, K.J.; Aley, P.K.; Angus, B.; Becker, S.; Belij-Rammerstorfer, S.; Bellamy, D.; Bibi, S.; Bittaye, M.; Clutterbuck, E.A.; et al. Safety and immunogenicity of the ChAdOx1 nCoV-19 vaccine against SARS-CoV-2: A preliminary report of a phase 1/2, single-blind, randomised controlled trial. Lancet 2020. [Google Scholar] [CrossRef]
- Xu, R.; Shi, M.; Li, J.; Song, P.; Li, N. Construction of SARS-CoV-2 virus-like particles by mammalian expression system. Front. Bioeng. Biotechnol. 2020, 8, 1–6. [Google Scholar] [CrossRef]
- Griffith University. Available online: https://news.griffith.edu.au/2020/04/23/griffith-university-researchers-on-the-road-to-covid-19-vaccine/ (accessed on 6 August 2020).
- UPMC. Available online: https://www.upmc.com/media/news/040220-falo-gambotto-sars-cov2-vaccine (accessed on 6 August 2020).
- Businesswire. Available online: https://www.businesswire.com/news/home/20200619005016/en/Clover-Biopharmaceuticals-Initiates-Phase-1-Clinical-Trial (accessed on 13 September 2020).
- Novavax. Available online: https://ir.novavax.com/news-releases/news-release-details/novavax-announces-positive-phase-1-data-its-covid-19-vaccine (accessed on 14 September 2020).
- Technology Networks. Available online: https://www.technologynetworks.com/biopharma/news/phase-1-clinical-trial-of-university-of-queensland-covid-19-vaccine-begins-337387#:~:text=UQ’s%20vaccine%20is%20the%20seventh,testing%20as%20quickly%20as%20possible (accessed on 14 September 2020).
- National Institutes of Health. Available online: https://www.nih.gov/news-events/news-releases/phase-3-clinical-trial-investigational-vaccine-covid-19-begins (accessed on 14 September 2020).
- Pharmaceutical Technology. Available online: https://www.pharmaceutical-technology.com/news/inovio-covid-19-vaccine-preclinical/ (accessed on 14 September 2020).
- Immunomic Therapeutics. Available online: https://www.immunomix.com/immunomic-therapeutics-forms-collaboration-with-epivax-and-pharmajet-to-develop-novel-vaccine-candidate-against-covid-19-using-its-investigational-unite-platform/ (accessed on 6 August 2020).
- Pharmaceutical Technology. Available online: https://www.pharmaceutical-technology.com/news/uga-covid-19-vaccine-candidate/ (accessed on 6 August 2020).
- Herzog, C. Influence of parenteral administration routes and additional factors on vaccine safety and immunogenicity: A review of recent literature. Expert Rev. Vaccines 2014, 13, 399–415. [Google Scholar] [CrossRef] [PubMed]
- Tseng, C.-T.; Sbrana, E.; Iwata-Yoshikawa, N.; Newman, P.C.; Garron, T.; Atmar, R.L.; Peters, C.J.; Couch, R.B. Immunization with SARS coronavirus vaccines leads to pulmonary immunopathology on challenge with the SARS virus. PLoS ONE 2012, 7, e35421. [Google Scholar] [CrossRef]
- Volz, A.; Kupke, A.; Song, F.; Jany, S.; Fux, R.; Shams-Eldin, H.; Schmidt, J.; Becker, C.; Eickmann, M.; Becker, S.; et al. Protective Efficacy of Recombinant Modified Vaccinia Virus Ankara Delivering Middle East Respiratory Syndrome Coronavirus Spike Glycoprotein. J. Virol. 2015, 89, 8651–8656. [Google Scholar] [CrossRef] [Green Version]
- Du, L.; Tai, W.; Zhou, Y.; Jiang, S. Vaccines for the prevention against the threat of MERS-CoV. Expert Rev. Vaccines 2016, 15, 1123–1134. [Google Scholar] [CrossRef]
- Bal, S.M.; Ding, Z.; Van Riet, E.; Jiskoot, W.; Bouwstra, J. Advances in transcutaneous vaccine delivery: Do all ways lead to Rome? J. Control. Release 2010, 148, 266–282. [Google Scholar] [CrossRef]
- Pielenhofer, J.; Sohl, J.; Windbergs, M.; Langguth, P.; Radsak, M.P. Current Progress in Particle-Based Systems for Transdermal Vaccine Delivery. Front. Immunol. 2020, 11, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Ali, R.; Mehta, P.; Arshad, M.S.; Kucuk, I.; Chang, M.-W.; Ahmad, Z. Transdermal Microneedles—A Materials Perspective. AAPS PharmSciTech 2019, 21, 12. [Google Scholar] [CrossRef] [PubMed]
- Li, N.; Peng, L.-H.; Chen, X.; Nakagawa, S.; Gao, J.-Q. Transcutaneous vaccines: Novel advances in technology and delivery for overcoming the barriers. Vaccine 2011, 29, 6179–6190. [Google Scholar] [CrossRef] [PubMed]
- Mitragotri, S. Devices for overcoming biological barriers: The use of physical forces to disrupt the barriers. Adv. Drug Deliv. Rev. 2013, 65, 100–103. [Google Scholar] [CrossRef] [PubMed]
- Sardesai, N.Y.; Weiner, D.B. Electroporation delivery of DNA vaccines: Prospects for success. Curr. Opin. Immunol. 2011, 23, 421–429. [Google Scholar] [CrossRef] [Green Version]
- Ita, K. Perspectives on Transdermal Electroporation. Pharmaceutics 2016, 8, 9. [Google Scholar] [CrossRef]
- Bernelin-Cottet, C.; Urien, C.; McCaffrey, J.; Collins, D.; Donadei, A.; McDaid, D.; Jakob, V.; Barnier-Quer, C.; Collin, N.; Bouguyon, E.; et al. Electroporation of a nanoparticle-associated DNA vaccine induces higher inflammation and immunity compared to its delivery with microneedle patches in pigs. J. Control. Release 2019, 308, 14–28. [Google Scholar] [CrossRef]
- Arshad, M.S.; Fatima, S.; Nazari, K.; Ali, R.; Farhan, M.; Muhammad, S.A.; Abbas, N.; Hussain, A.; Kucuk, I.; Chang, M.-W.; et al. Engineering and characterisation of BCG-loaded polymeric microneedles. J. Drug Target. 2019, 28, 525–532. [Google Scholar] [CrossRef]
- Arshad, M.S.; Zafar, S.; Tehreem Zahra, A.; Zaman, M.H.; Akhtar, A.; Kucuk, I.; Farhan, M.; Chang, M.-W.; Ahmad, Z. Fabrication and characterisation of self-applicating heparin sodium microneedle patches. J. Drug. Target. 2020, 1–22. [Google Scholar] [CrossRef]
- Marshall, S.; Sahm, L.J.; Moore, A.C. The success of microneedle-mediated vaccine delivery into skin. Hum. Vaccines Immunother. 2016, 12, 2975–2983. [Google Scholar] [CrossRef] [Green Version]
- Donnelly, R.F.; Douroumis, D. Microneedles for drug and vaccine delivery and patient monitoring. Drug Deliv. Transl. Res. 2015, 5, 311–312. [Google Scholar] [CrossRef] [Green Version]
- Vrdoljak, A.; McGrath, M.G.; Carey, J.B.; Draper, S.J.; Hill, A.V.; O’Mahony, C.; Crean, A.M.; Moore, A.C. Coated microneedle arrays for transcutaneous delivery of live virus vaccines. J. Control. Release 2012, 159, 34–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mönkäre, J.; Pontier, M.; Van Kampen, E.E.; Du, G.; Leone, M.; Romeijn, S.; Nejadnik, M.R.; O’Mahony, C.; Slütter, B.; Jiskoot, W.; et al. Development of PLGA nanoparticle loaded dissolving microneedles and comparison with hollow microneedles in intradermal vaccine delivery. Eur. J. Pharm. Biopharm. 2018, 129, 111–121. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.; Erdos, G.; Huang, S.; Kenniston, T.W.; Balmert, S.C.; Carey, C.D.; Raj, V.S.; Epperly, M.W.; Klimstra, W.B.; Haagmans, B.L.; et al. Microneedle array delivered recombinant coronavirus vaccines: Immunogenicity and rapid translational development. EBioMedicine 2020, 55, 102743. [Google Scholar] [CrossRef] [PubMed]
- Corthésy, B.; Bioley, G. Lipid-Based Particles: Versatile Delivery Systems for Mucosal Vaccination against Infection. Front. Immunol. 2018, 9, 1–20. [Google Scholar] [CrossRef]
- British Society for Immunology. Available online: https://www.immunology.org/public-information/bitesized-immunology/vaccines-and-therapeutics/mucosal-vaccination (accessed on 12 August 2020).
- Kang, S.H.; Hong, S.J.; Lee, Y.-K.; Cho, S. Oral Vaccine Delivery for Intestinal Immunity-Biological Basis, Barriers, Delivery System, and M Cell Targeting. Polymers 2018, 10, 948. [Google Scholar] [CrossRef] [Green Version]
- Russell-Jones, G. Oral vaccine delivery. J. Control. Release 2000, 65, 49–54. [Google Scholar] [CrossRef]
- Funk, C.D.; Laferrière, C.; Ardakani, A. A Snapshot of the Global Race for Vaccines Targeting SARS-CoV-2 and the COVID-19 Pandemic. Front. Pharmacol. 2020, 11, 1–17. [Google Scholar] [CrossRef]
- Zaman, M.; Chandrudu, S.; Toth, I. Strategies for intranasal delivery of vaccines. Drug Deliv. Transl. Res. 2012, 3, 100–109. [Google Scholar] [CrossRef] [Green Version]
- Du, L.; Zhao, G.; Lin, Y.; Sui, H.; Chan, C.; Ma, S.; He, Y.; Jiang, S.; Wu, C.; Yuen, K.-Y.; et al. Intranasal Vaccination of Recombinant Adeno-Associated Virus Encoding Receptor-Binding Domain of Severe Acute Respiratory Syndrome Coronavirus (SARS-CoV) Spike Protein Induces Strong Mucosal Immune Responses and Provides Long-Term Protection against SARS-CoV Infection1. J. Immunol. 2008, 180, 948–956. [Google Scholar] [CrossRef]
- Lu, N.; Hickey, A.J. Pulmonary vaccine delivery. Expert Rev. Vaccines 2007, 6, 213–226. [Google Scholar] [CrossRef]
- ONdrugDELIVERY. Available online: https://www.ondrugdelivery.com/inhaled-and-nasal-covid-19-vaccine-progress/ (accessed on 12 August 2020).


| Patient Condition | Symptoms |
|---|---|
| Asymptomatic | RT-PCR test positive but no symptoms and chest imaging is normal |
| Mild | Digestive (diarrhoea, nausea/vomiting, abdominal discomfort) and acute upper respiratory tract infection (cough, fever, sore throat, fatigue, sneeze, myalgia and nasal congestion) symptoms |
| Moderate | Pneumonia without hypoxemia |
| Severe | Pneumonia with hypoxemia (SpO2 < 90% on room air) or respiratory rate >30 breaths/minute |
| Critical | ARDS, other symptoms include respiratory failure, cardiac injury, sepsis, septic shock, acute kidney injury and coagulation abnormality |
| Type of Vaccine | Platform | Current Stage and Trial ID | Manufacturer | References |
|---|---|---|---|---|
| Inactivated | Inactivated | Phase 3 (ChiCTR2000034780) Phase 1/2(ChiCTR2000032459) | Beijing Institute of Biological Products and Sinopharm | [134] |
| Inactivated | Inactivated | Phase 3 (NCT04456595) (669/UN6.KEP/EC/2020) Phase 1/2 (NCT04383574) (NCT04352608) | Sinovac | [134] |
| Whole-virion (inactivated) | Inactivated | Phase 1/2 (NCT04471519) | Bharat Biotech | [134] |
| Codon deoptimized live attenuated vaccine | Live attenuated virus | Pre-clinical | Indian Immunologicals and Griffith University | [142] |
| Microneedle patch (S1 subunit) | Protein subunit | Pre-clinical | University of Pittsburgh | [143] |
| Trimeric subunit (S protein) | Protein subunit | Phase 1 (NCT04405908) | Clover Biopharmaceuticals, GSK and Dynavax | [144] |
| Recombinant SARS-CoV-2 nanoparticle vaccine (full length glycoprotein) with/without matrix M as adjuvant | Protein subunit | Phase 2 b (NCT04533399) Phase 1/2 (NCT04368988) | Novavax | [145] |
| RBD protein fused with IgG (Fc region) in combination with an adjuvant | Protein subunit | Pre-clinical | Chulalongkorn University and GPO, Thailand | [134] |
| Molecular clamp stabilized S protein + MF59 adjuvant | Protein subunit | Phase 1 (ACTRN12620000674932p) | University of Queensland, CSL and Seqirus | [146] |
| Recombinant protein (RBD-dimer) with an adjuvant | Protein subunit | Phase 2 (NCT04466085) Phase 1(NCT04445194) | Anhui Zhifei Longcom Biopharmaceutical and Institute of Microbiology, Chinese Academy of Sciences | [134] |
| Recombinant protein, nanoparticles (containing S-protein and other epitopes) | Protein subunit | Pre-clinical | Saint-Petersburg scientific research institute of vaccines and serums | [134] |
| LNP-based peptide antigens | Protein subunit | Pre-clinical | IMV Inc | [134] |
| 3 LNP-mRNAs | RNA | Phase 3 (NCT04368728) Phase 1/2 (2020-001038-36) (ChiCTR2000034825) (NCT04537949) | BioNTech, Pfizer and Fosun Pharma | [134] |
| LNP-encapsulated mRNA | RNA | Phase 3 (NCT04470427) Phase 2 (NCT04405076) Phase 1 (NCT04283461) | Moderna and NIAID | [147] |
| DNA plasmid vaccine (intradermal, followed by electroporation) | DNA | Phase 1/2 (NCT04447781) (NCT04336410) | Inovio Pharmaceuticals and International Vaccine Institute | [148] |
| Plasmid DNA (needle-free delivery) | DNA | Pre-clinical | Immunomic Therapeutics, EpiVax and PharmaJet | [149] |
| DNA plasmid vaccine with an adjuvant | DNA | Phase 1/2 (NCT04463472) (NCT04527081) | Osaka University, AnGes and Takara Bio | [134] |
| Para-influenza virus 5-based vaccine manifesting the S protein | Non-replicating viral vector | Pre-clinical | University of Georgia and University of Iowa | [150] |
| Intranasal recombinant vaccine based on Influenza A virus, for SARS-Cov-2 infection | Replicating viral vector | Pre-clinical | FBRI SRC VB VECTOR, Rospotrebnadzor and Koltsovo | [134] |
| Adenovirus type 5 vector | Non-replicating viral vector | Phase 3 (NCT04526990) (NCT04540419) Phase 2 (ChiCTR2000031781) Phase 1 (ChiCTR2000030906) | CanSino Biological and Beijing Institute of Biotechnology | [139] |
| ChAdOx1-S | Non-replicating viral vector | Phase 3 (ISRCTN89951424) (NCT04516746) Phase 2 (2020-001228-32) Phase 1/2 (PACTR202006922165132) (2020-001072-15) | University of Oxford and AstraZeneca | [140] |
| Enveloped virus-like particle | VLP | Pre-clinical | VBI Vaccines Inc. | [134] |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zafar, S.; Arshad, M.S.; Fatima, S.; Ali, A.; Zaman, A.; Sayed, E.; Chang, M.-W.; Ahmad, Z. COVID-19: Current Developments and Further Opportunities in Drug Delivery and Therapeutics. Pharmaceutics 2020, 12, 945. https://doi.org/10.3390/pharmaceutics12100945
Zafar S, Arshad MS, Fatima S, Ali A, Zaman A, Sayed E, Chang M-W, Ahmad Z. COVID-19: Current Developments and Further Opportunities in Drug Delivery and Therapeutics. Pharmaceutics. 2020; 12(10):945. https://doi.org/10.3390/pharmaceutics12100945
Chicago/Turabian StyleZafar, Saman, Muhammad Sohail Arshad, Sameen Fatima, Amna Ali, Aliyah Zaman, Elshaimaa Sayed, Ming-Wei Chang, and Zeeshan Ahmad. 2020. "COVID-19: Current Developments and Further Opportunities in Drug Delivery and Therapeutics" Pharmaceutics 12, no. 10: 945. https://doi.org/10.3390/pharmaceutics12100945