Safety and Local Efficacy of Laser Ablation for the Extrahepatic Metastasis of Hepatocellular Carcinoma: An Available Treatment Strategy

Abstract
:1. Introduction
2. Materials and Methods
2.1. LA Procedure
2.2. Follow-Up
2.3. Statistical Analysis
3. Results
3.1. Baseline Clinical Characteristics
3.2. LA Response and Complications
3.3. Factors Associated with ICA
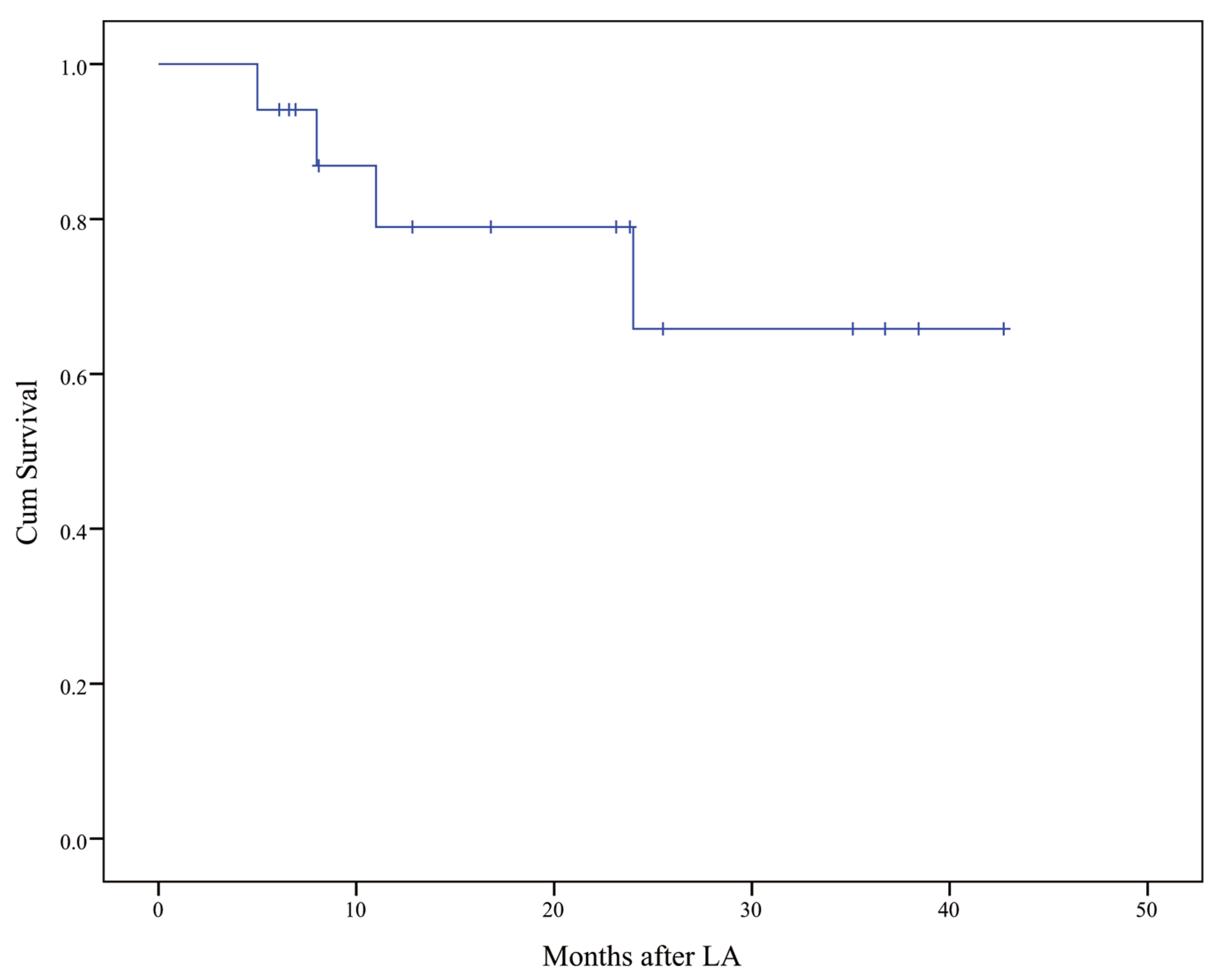
3.4. Follow-Up
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 2015, 136, E359–E386. [Google Scholar] [CrossRef] [PubMed]
- Erratum: Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2020, 70, 313. [CrossRef] [PubMed] [Green Version]
- Forner, A.; Reig, M.; Bruix, J. Hepatocellular carcinoma. Lancet 2018, 391, 1301–1314. [Google Scholar] [CrossRef]
- Hasegawa, K.; Kokudo, N.; Makuuchi, M.; Izumi, N.; Ichida, T.; Kudo, M.; Ku, Y.; Sakamoto, M.; Nakashima, O.; Matsui, O.; et al. Comparison of resection and ablation for hepatocellular carcinoma: A cohort study based on a Japanese nationwide survey. J. Hepatol. 2013, 58, 724–729. [Google Scholar] [CrossRef]
- Peng, Z.; Chen, S.; Wei, M.; Lin, M.; Jiang, C.; Mei, J.; Li, B.; Wang, Y.; Li, J.; Xie, X.; et al. Advanced Recurrent Hepatocellular Carcinoma: Treatment with Sorafenib Alone or in Combination with Transarterial Chemoembolization and Radiofrequency Ablation. Radiology 2018, 287, 705–714. [Google Scholar] [CrossRef] [Green Version]
- Faivre, S.; Rimassa, L.; Finn, R.S. Molecular therapies for HCC: Looking outside the box. J. Hepatol. 2020, 72, 342–352. [Google Scholar] [CrossRef] [Green Version]
- Kudo, M.; Finn, R.S.; Qin, S.; Han, K.H.; Ikeda, K.; Piscaglia, F.; Baron, A.; Park, J.W.; Han, G.; Jassem, J.; et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: A randomised phase 3 non-inferiority trial. Lancet 2018, 391, 1163–1173. [Google Scholar] [CrossRef] [Green Version]
- Cheng, A.L.; Hsu, C.; Chan, S.L.; Choo, S.P.; Kudo, M. Challenges of combination therapy with immune checkpoint inhibitors for hepatocellular carcinoma. J. Hepatol. 2020, 72, 307–319. [Google Scholar] [CrossRef] [Green Version]
- Zongyi, Y.; Xiaowu, L. Immunotherapy for hepatocellular carcinoma. Cancer Lett. 2020, 470, 8–17. [Google Scholar] [CrossRef]
- Bouattour, M.; Mehta, N.; He, A.R.; Cohen, E.I.; Nault, J.C. Systemic treatment for advanced hepatocellular carcinoma. Liver Cancer 2019, 8, 341–358. [Google Scholar] [CrossRef]
- Choi, G.H.; Shim, J.H.; Kim, M.J.; Ryu, M.H.; Ryoo, B.Y.; Kang, Y.K.; Shin, Y.M.; Kim, K.M.; Lim, Y.S.; Lee, H.C. Sorafenib alone versus sorafenib combined with transarterial chemoembolization for advanced-stage hepatocellular carcinoma: Results of propensity score analyses. Radiology 2013, 269, 603–611. [Google Scholar] [CrossRef] [PubMed]
- Yuan, H.; Lan, Y.; Li, X.; Tang, J.; Liu, F. Large hepatocellular carcinoma with local remnants after transarterial chemoembolization: Treatment by sorafenib combined with radiofrequency ablation or sorafenib alone. Am. J. Cancer Res. 2019, 9, 791–799. [Google Scholar] [PubMed]
- Carrafiello, G.; Laganà, D.; Ianniello, A.; Nicotera, P.; Fontana, F.; Dizonno, M.; Cuffari, S.; Fugazzola, C. Radiofrequency thermal ablation for pain control in patients with single painful bone metastasis from hepatocellular carcinoma. Eur. J. Radiol. 2009, 71, 363–368. [Google Scholar] [CrossRef]
- Kashima, M.; Yamakado, K.; Takaki, H.; Kaminou, T.; Tanigawa, N.; Nakatsuka, A.; Takeda, K. Radiofrequency ablation for the treatment of bone metastases from hepatocellular carcinoma. AJR Am. J. Roentgenol. 2010, 194, 536–541. [Google Scholar] [CrossRef]
- Doreille, A.; N’Kontchou, G.; Halimi, A.; Bouhafs, F.; Coderc, E.; Sellier, N.; Seror, O. Percutaneous treatment of extrahepatic recurrence of hepatocellular carcinoma. Diagn. Interv. Imaging 2016, 97, 1117–1123. [Google Scholar] [CrossRef] [PubMed]
- Mu, L.; Sun, L.; Pan, T.; Lyu, N.; Li, S.; Li, X.; Wang, J.; Xie, Q.; Deng, H.; Zheng, L.; et al. Percutaneous CT-guided radiofrequency ablation for patients with extrahepatic oligometastases of hepatocellular carcinoma: Long-term results. Int. J. Hyperth. 2018, 34, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Xie, X.; Lin, J.; Wang, W.; Zhang, X.; Liu, M.; Li, X.; Huang, G.; Liu, B.; Xie, X. Percutaneous radiofrequency ablation of adrenal metastases from hepatocellular carcinoma: A single-center experience. Cancer Imaging 2019, 19, 44. [Google Scholar] [CrossRef] [Green Version]
- Pacella, C.M.; Bizzarri, G.; Magnolfi, F.; Cecconi, P.; Caspani, B.; Anelli, V.; Bianchini, A.; Valle, D.; Pacella, S.; Manenti, G.; et al. Laser thermal ablation in the treatment of small hepatocellular carcinoma: Results in 74 patients. Radiology 2001, 221, 712–720. [Google Scholar] [CrossRef] [Green Version]
- Ritz, J.P.; Lehmann, K.S.; Mols, A.; Frericks, B.; Knappe, V.; Buhr, H.J.; Holmer, C. Laser-induced thermotherapy for lung tissue—Evaluation of two different internally cooled application systems for clinical use. Lasers Med. Sci. 2008, 23, 195–202. [Google Scholar] [CrossRef]
- Caspani, B.; Ierardi, A.M.; Motta, F.; Cecconi, P.; Fesce, E.; Belli, L. Small nodular hepatocellular carcinoma treated by laser thermal ablation in high risk locations: Preliminary results. Eur. Radiol. 2010, 20, 2286–2292. [Google Scholar] [CrossRef]
- Orlacchio, A.; Bolacchi, F.; Chegai, F.; Bergamini, A.; Costanzo, E.; Del Giudice, C.; Angelico, M.; Simonetti, G. Comparative evaluation of percutaneous laser and radiofrequency ablation in patients with HCC smaller than 4 cm. Radiol. Med. 2014, 119, 298–308. [Google Scholar] [CrossRef] [PubMed]
- Teratani, T.; Yoshida, H.; Shiina, S.; Obi, S.; Sato, S.; Tateishi, R.; Mine, N.; Kondo, Y.; Kawabe, T.; Omata, M. Radiofrequency ablation for hepatocellular carcinoma in so-called high-risk locations. Hepatology 2006, 43, 1101–1108. [Google Scholar] [CrossRef] [PubMed]
- Francica, G.; Petrolati, A.; Di Stasio, E.; Pacella, S.; Stasi, R.; Pacella, C.M. Effectiveness, safety, and local progression after percutaneous laser ablation for hepatocellular carcinoma nodules up to 4 cm are not affected by tumor location. AJR Am. J. Roentgenol. 2012, 199, 1393–1401. [Google Scholar] [CrossRef]
- Di Costanzo, G.G.; D’Adamo, G.; Tortora, R.; Zanfardino, F.; Mattera, S.; Francica, G.; Pacella, C.M. A novel needle guide system to perform percutaneous laser ablation of liver tumors using the multifiber technique. Acta Radiol. 2013, 54, 876–881. [Google Scholar] [CrossRef] [PubMed]
- Mou, Y.; Zhao, Q.; Zhong, L.; Chen, F.; Jiang, T. Preliminary results of ultrasound-guided laser ablation for unresectable metastases to retroperitoneal and hepatic portal lymph nodes. World J. Surg. Oncol. 2016, 14, 165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, T.A.; Deng, Z.; Tian, G.; Chen, F.; Bao, H.; Li, J.; Wang, W. Percutaneous laser ablation: A new contribution to unresectable high-risk metastatic retroperitoneal lesions? Oncotarget 2017, 8, 2413–2422. [Google Scholar] [CrossRef]
- Lu, Z.-H.; Shen, F.; Yan, Z.-L.; Li, J.; Yang, J.-H.; Zong, M.; Shi, L.-H.; Wu, M.-C. Treatment of portal vein tumor thrombus of hepatocellular carcinoma with percutaneous laser ablation. J. Cancer Res. Clin. Oncol. 2009, 135, 783–789. [Google Scholar] [CrossRef]
- Johnson, P.J.; Berhane, S.; Kagebayashi, C.; Satomura, S.; Teng, M.; Reeves, H.L.; O’Beirne, J.; Fox, R.; Skowronska, A.; Palmer, D.; et al. Assessment of liver function in patients with hepatocellular carcinoma: A new evidence-based approach-the ALBI grade. J. Clin. Oncol. 2015, 33, 550–558. [Google Scholar] [CrossRef]
- Lam, V.W.-T.; Ng, K.K.; Chok, K.S.-H.; Cheung, T.-T.; Yuen, J.; Tung, H.; Tso, W.-K.; Fan, S.-T.; Poon, R.T.P. Incomplete ablation after radiofrequency ablation of hepatocellular carcinoma: Analysis of risk factors and prognostic factors. Ann. Surg. Oncol. 2008, 15, 782–790. [Google Scholar] [CrossRef]
- Dindo, D.; Demartines, N.; Clavien, P.-A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef]
- Omary, R.A.; Bettmann, M.A.; Cardella, J.F.; Bakal, C.W.; Schwartzberg, M.S.; Sacks, D.; Rholl, K.S.; Meranze, S.G.; Lewis, C.A. Quality improvement guidelines for the reporting and archiving of interventional radiology procedures. J. Vasc. Interv. Radiol. 2002, 13, 879–881. [Google Scholar] [CrossRef]
- Tian, G.; Jiang, T.A. US-guided percutaneous laser ablation of refractory metastatic retroperitoneal lesions: A care-compliant case report. Medicine (Baltimore) 2017, 96, e6597. [Google Scholar] [CrossRef] [PubMed]
- Giorgio, A.; Tarantino, L.; de Stefano, G.; Farella, N.; Catalano, O.; Cusati, B.; Del Viscovo, L.; Alaia, A.; Caturelli, E. Interstitial laser photocoagulation under ultrasound guidance of liver tumors: Results in 104 treated patients. Eur. J. Ultrasound 2000, 11, 181–188. [Google Scholar] [CrossRef]
- Eichler, K.; Mack, M.G.; Straub, R.; Engelmann, K.; Zangos, S.; Woitaschek, D.; Vogl, T.J. Oligonodular hepatocellular carcinoma (HCC): MR-controlled laser-induced thermotherapy. Radiologe 2001, 41, 915–922. [Google Scholar] [CrossRef]
- Pacella, C.M.; Bizzarri, G.; Francica, G.; Bianchini, A.; De Nuntis, S.; Pacella, S.; Crescenzi, A.; Taccogna, S.; Forlini, G.; Rossi, Z.; et al. Percutaneous laser ablation in the treatment of hepatocellular carcinoma with small tumors: Analysis of factors affecting the achievement of tumor necrosis. J. Vasc. Interv. Radiol. 2005, 16, 1447–1457. [Google Scholar] [CrossRef]
- Zhou, K.; Pan, J.; Yang, N.; Shi, H.-F.; Cao, J.; Li, Y.-M.; Zhang, H.-Z.; Wang, K.-F.; Chen, S.-H. Effectiveness and safety of CT-guided percutaneous radiofrequency ablation of adrenal metastases. Br. J. Radiol. 2018, 91, 20170607. [Google Scholar] [CrossRef]
- Hasegawa, T.; Yamakado, K.; Nakatsuka, A.; Uraki, J.; Yamanaka, T.; Fujimori, M.; Miki, M.; Sasaki, T.; Sakuma, H.; Sugimura, Y. Unresectable Adrenal Metastases: Clinical Outcomes of Radiofrequency Ablation. Radiology 2015, 277, 584–593. [Google Scholar] [CrossRef]
- Zhang, Y.-R.; Fang, L.-Y.; Yu, C.; Sun, Z.-X.; Huang, Y.; Chen, J.; Guo, T.; Xiang, F.-X.; Wang, J.; Lu, C.-F.; et al. Laser-induced interstitial thermotherapy via a single-needle delivery system: Optimal conditions of ablation, pathological and ultrasonic changes. J. Huazhong Univ. Sci. Technol. Med. Sci. 2015, 35, 579–584. [Google Scholar] [CrossRef]
- Head, H.W.; Dodd, G.D. Thermal ablation for hepatocellular carcinoma. Gastroenterology 2004, 127, S167–S178. [Google Scholar] [CrossRef]
- Wang, T.; Lu, X.J.; Chi, J.C.; Ding, M.; Zhang, Y.; Tang, X.Y.; Li, P.; Zhang, L.; Zhang, X.Y.; Zhai, B. Microwave ablation of hepatocellular carcinoma as first-line treatment: Long term outcomes and prognostic factors in 221 patients. Sci. Rep. 2016, 6, 32728. [Google Scholar] [CrossRef]
- Liang, H.Y.; Guo, Q.Y.; Sun, W.; Mao, X.N.; Wen, F.; Shan, M.; Zhao, G.; Wang, X.H.; Lu, Z.M. Sequential Use of Transhepatic Arterial Chemoembolization and Bipolar Radiofrequency Ablation in the Clinical Therapy of Hepatocellular Carcinoma. Cancer Biother. Radiopharm. 2015, 30, 427–432. [Google Scholar] [CrossRef]
- Ayav, A.; Germain, A.; Marchal, F.; Tierris, I.; Laurent, V.; Bazin, C.; Yuan, Y.; Robert, L.; Brunaud, L.; Bresler, L. Radiofrequency ablation of unresectable liver tumors: Factors associated with incomplete ablation or local recurrence. Am. J. Surg. 2010, 200, 435–439. [Google Scholar] [CrossRef]
- Lee, J.M.; Lee, Y.H.; Kim, Y.K.; Kim, S.W.; Kim, C.S. Combined therapy of radiofrequency ablation and ethanol injection of rabbit liver: An in vivo feasibility study. Cardiovasc. Intervent. Radiol. 2004, 27, 151–157. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.-J.; Liang, H.-H.; Chen, M.-S.; Guo, R.-P.; Li, J.-Q.; Zheng, Y.; Zhang, Y.-Q.; Lau, W.Y. Hepatocellular carcinoma treated with radiofrequency ablation with or without ethanol injection: A prospective randomized trial. Radiology 2007, 244, 599–607. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Z.X.; Liao, M.H.; Wang, X.X.; Huang, J.W. Radiofrequency ablation with or without ethanol injection for hepatocellular carcinoma: A systematic review and meta-analysis. Minerva Med. 2016, 107, 381–391. [Google Scholar] [PubMed]
- Li, Z.; Zhang, K.; Lin, S.-M.; Mi, D.-H.; Cao, N.; Wen, Z.-Z.; Li, Z.-X. Radiofrequency ablation combined with percutaneous ethanol injection for hepatocellular carcinoma: A systematic review and meta-analysis. Int. J. Hyperth. 2017, 33, 237–246. [Google Scholar] [CrossRef]
- Zou, X.; Liu, Q.; Zhou, X.; He, G.; Yu, M.; Han, Z.; Meng, X.; Su, H. Ultrasound-guided percutaneous laser and ethanol ablation of rabbit VX2 liver tumors. Acta Radiol. 2013, 54, 181–187. [Google Scholar] [CrossRef]
- Hao, Y.; Numata, K.; Ishii, T.; Fukuda, H.; Maeda, S.; Nakano, M.; Tanaka, K. Rate of local tumor progression following radiofrequency ablation of pathologically early hepatocellular carcinoma. World J. Gastroenterol. 2017, 23, 3111–3121. [Google Scholar] [CrossRef]
- Lee, M.W.; Kang, D.; Lim, H.K.; Cho, J.; Sinn, D.H.; Kang, T.W.; Song, K.D.; Rhim, H.; Cha, D.I.; Lu, D.S.K. Updated 10-year outcomes of percutaneous radiofrequency ablation as first-line therapy for single hepatocellular carcinoma < 3 cm: Emphasis on association of local tumor progression and overall survival. Eur. Radiol. 2020, 30, 2391–2400. [Google Scholar] [CrossRef]
- Kim, Y.-S.; Lee, W.J.; Rhim, H.; Lim, H.K.; Choi, D.; Lee, J.Y. The minimal ablative margin of radiofrequency ablation of hepatocellular carcinoma (> 2 and < 5 cm) needed to prevent local tumor progression: 3D quantitative assessment using CT image fusion. AJR Am. J. Roentgenol. 2010, 195, 758–765. [Google Scholar] [CrossRef]
- Yoon, J.H.; Lee, J.M.; Klotz, E.; Woo, H.; Yu, M.H.; Joo, I.; Lee, E.S.; Han, J.K. Prediction of Local Tumor Progression after Radiofrequency Ablation (RFA) of Hepatocellular Carcinoma by Assessment of Ablative Margin Using Pre-RFA MRI and Post-RFA CT Registration. Korean J. Radiol. 2018, 19, 1053–1065. [Google Scholar] [CrossRef] [PubMed]
- Kono, M.; Inoue, T.; Kudo, M.; Chishina, H.; Arizumi, T.; Takita, M.; Kitai, S.; Yada, N.; Hagiwara, S.; Minami, Y.; et al. Radiofrequency ablation for hepatocellular carcinoma measuring 2 cm or smaller: Results and risk factors for local recurrence. Dig. Dis. 2014, 32, 670–677. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.H.; Lee, J.M.; Lee, J.Y.; Kim, S.H.; Yoon, J.H.; Kim, Y.J.; Han, J.K.; Choi, B.I. Radiofrequency ablation of hepatocellular carcinoma as first-line treatment: Long-term results and prognostic factors in 162 patients with cirrhosis. Radiology 2014, 270, 900–909. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | n = 17 |
|---|---|
| Age (year) | 54.1 ± 14.6 |
| Gender | |
| Male | 13 |
| Female | 4 |
| Etiology | |
| HBV 1 | 12 |
| HCV 2 | 2 |
| others | 3 |
| Initial treatment of liver tumor | |
| Surgical resection | 13 |
| Ablation | 4 |
| Intent of LA3 | |
| Curative | 12 |
| Palliative | 5 |
| Child–Pugh classification | |
| A | 17 |
| B | 0 |
| Child–Pugh score | |
| 5 | 16 |
| 6 | 1 |
| ALBI grade4 | |
| 1 | 11 |
| 2 | 6 |
| Biochemical tests | |
| AFP (μg/L) 5 | 4.5 (1.7–360.1) |
| ALB (g/L) 6 | 40.3 ± 5.5 |
| TBIL (μmol/L) 7 | 13.0 ± 4.7 |
| PLT account (×109/L) 8 | 180 ± 56 |
| Tumor number | |
| Solitary | 10 |
| Multiple | 7 |
| Size (cm) | 2.2 ± 1.1 |
| Volume (cm3) | 7.2 (5.6–19.5) |
| Characteristics | n = 28 |
|---|---|
| Tumor size (cm) | 2.2 ± 1.1 |
| Tumor volume (cm3) | 7.2 (5.6–19.5) |
| Location | |
| Abdominal wall | 3 |
| Abdominal lymph nodes | 4 |
| Intraabdominal seeding | 1 |
| Hepatic surface | 4 |
| Adrenal gland | 1 |
| Diaphragm | 1 |
| Hilar lymph nodes | 3 |
| Retroperitoneal lymph nodes | 7 |
| Subcutaneous chest wall | 4 |
| Number of fibers | 3 (1–4) |
| Power (J) | 3600 (640–5813) |
| Combination with ethanol injection | |
| Yes | 5 |
| No | 23 |
| Efficacy | |
| CA 1 | 20 |
| ICA 2 | 8 |
| Characteristics | CA 1 Lesion (n = 20) | ICA 2 Lesion (n = 8) | p-Value |
|---|---|---|---|
| Diameter of lesion (cm) | 1.84 ± 0.85 | 3.04 ± 1.10 | 0.005 |
| Volume of lesion (cm3) | 6.6 (4.5–12.3) | 23.8 (9.5–71.8) | 0.008 |
| Combination with ethanol injection | |||
| Yes | 2 | 3 | 0.123 |
| No | 18 | 5 | – |
| Number of fibers | 2 (1–3) | 4 (2.5–4) | 0.119 |
| Energy (J) | 3600 (2760–4750) | 5475 (2950–6500) | 0.281 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Long, H.; Zhuang, B.; Huang, G.; Li, X.; Lin, M.; Long, J.; Xie, X.; Liu, B. Safety and Local Efficacy of Laser Ablation for the Extrahepatic Metastasis of Hepatocellular Carcinoma: An Available Treatment Strategy. Coatings 2020, 10, 951. https://doi.org/10.3390/coatings10100951
Long H, Zhuang B, Huang G, Li X, Lin M, Long J, Xie X, Liu B. Safety and Local Efficacy of Laser Ablation for the Extrahepatic Metastasis of Hepatocellular Carcinoma: An Available Treatment Strategy. Coatings. 2020; 10(10):951. https://doi.org/10.3390/coatings10100951
Chicago/Turabian StyleLong, Haiyi, Bowen Zhuang, Guangliang Huang, Xiaoju Li, Manxia Lin, Jianting Long, Xiaoyan Xie, and Baoxian Liu. 2020. "Safety and Local Efficacy of Laser Ablation for the Extrahepatic Metastasis of Hepatocellular Carcinoma: An Available Treatment Strategy" Coatings 10, no. 10: 951. https://doi.org/10.3390/coatings10100951