Enterococcus faecalis Endocarditis and Outpatient Treatment: A Systematic Review of Current Alternatives

 ,
,
Abstract
:1. Introduction
2. Results
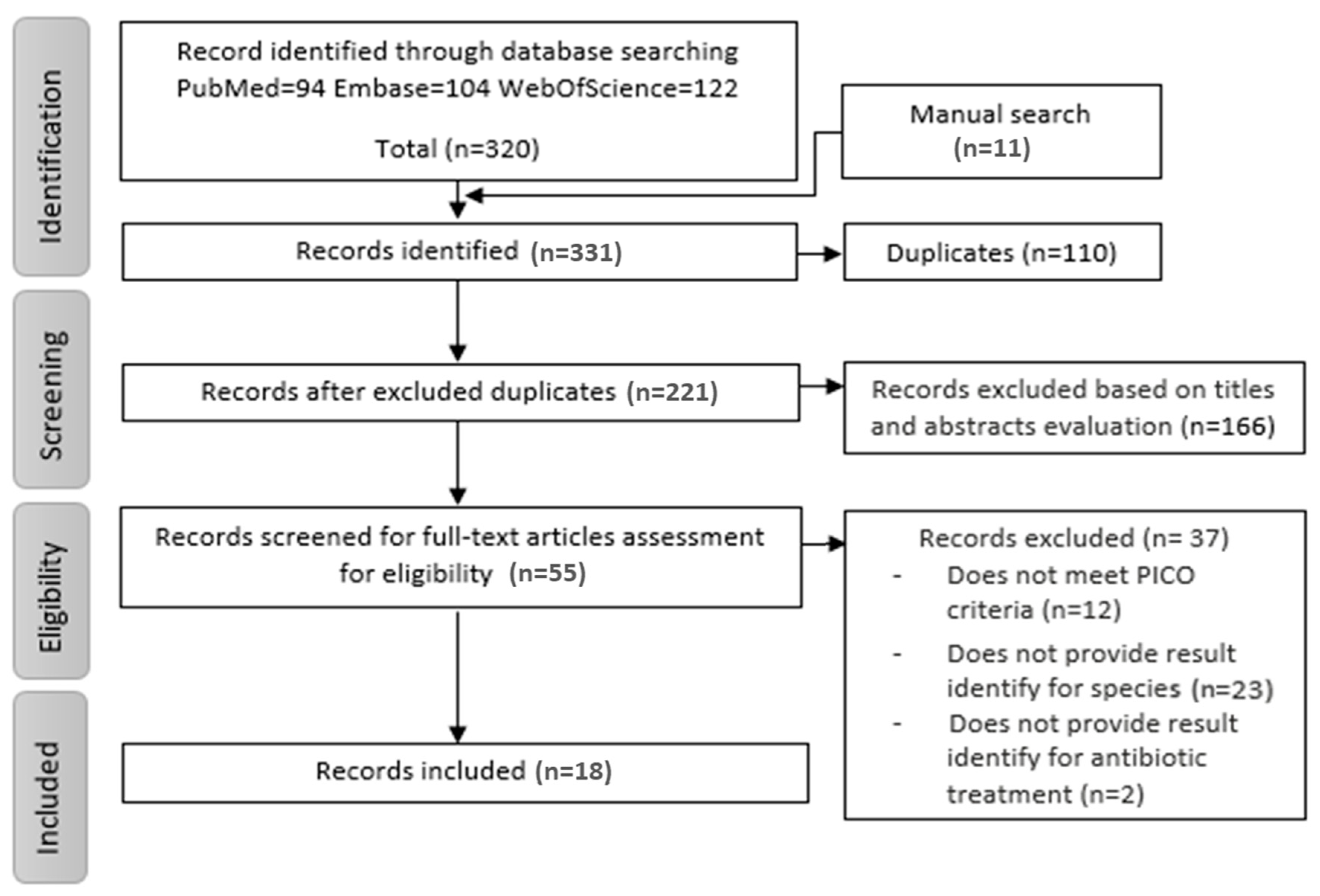
2.1. Search Results
2.2. Overview of the Studies
2.3. Quality of the Studies
2.4. Therapeutic Alternatives
2.4.1. Aminoglycosides Based Regimens
2.4.2. Dual β-Lactam Regimens
2.4.3. Teicoplanin-Based Regimens
2.4.4. Daptomycin Based Regimens
2.4.5. Dalbavancin Regimens
2.4.6. Oral Therapy
3. Discussion
4. Materials and Methods
4.1. Search Strategy
4.2. Eligibility Criteria
4.3. Selection of Studies
4.4. Quality Assessment
4.5. Data Extraction and Synthesis
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Baddour, L.M.; Wilson, W.R.; Bayer, A.S.; Fowler, V.; Tleyjeh, I.M.; Rybak, M.J.; Barsic, B.; Lockhart, P.B.; Gewitz, M.H.; Levison, M.E.; et al. Infective Endocarditis in Adults: Diagnosis, Antimicrobial Therapy, and Management of Complications. Circulation 2015, 132, 1435–1486. [Google Scholar] [CrossRef] [PubMed]
- Habib, G.; Lancellotti, P.; Antunes, M.J.; Bongiorni, M.G.; Casalta, J.-P.; Del Zotti, F.; Dulgheru, R.; El Khoury, G.; Erba, P.A.; Iung, B.; et al. 2015 ESC Guidelines for the management of infective endocarditis. Eur. Heart J. 2015, 36, 3075–3128. [Google Scholar] [CrossRef] [PubMed]
- Olmos, C.; Vilacosta, I.; Fernandez-Perez, C.; Bernal, J.L.; Ferrera, C.; García-Arribas, D.; Pérez-García, C.N.; Román, J.A.S.; Maroto, L.; Macaya, C.; et al. The Evolving Nature of Infective Endocarditis in Spain. J. Am. Coll. Cardiol. 2017, 70, 2795–2804. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Hidalgo, N.; Mas, P.T. Epidemiology of Infective Endocarditis in Spain in the Last 20 Years. Rev. Española Cardiol. (Engl. Ed.) 2013, 66, 728–733. [Google Scholar] [CrossRef]
- Beganovic, M.; Luther, M.K.; Rice, L.B.; Arias, C.A.; Rybak, M.J.; Laplante, K.L. A Review of Combination Antimicrobial Therapy for Enterococcus faecalis Bloodstream Infections and Infective Endocarditis. Clin. Infect. Dis. 2018, 67, 303–309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- García-Solache, M.; Rice, L.B. The Enterococcus: A Model of Adaptability to Its Environment. Clin. Microbiol. Rev. 2019, 32, e00058-18. [Google Scholar] [CrossRef] [Green Version]
- Rosa, R.; Creti, R.; Venditti, M.; D’Amelio, R.; Arciola, C.R.; Montanaro, L.; Baldassarri, L. Relationship between biofilm formation, the enterococcal surface protein (Esp) and gelatinase in clinical isolates of Enterococcus faecalis and Enterococcus faecium. FEMS Microbiol. Lett. 2006, 256, 145–150. [Google Scholar] [CrossRef] [Green Version]
- Cercenado, E. Enterococcus: Resistencias fenotípicas y genotípicas y epidemiología en España. Enferm. Infecc. Microbiol. Clin. 2011, 29, 59–65. [Google Scholar] [CrossRef]
- Pericà, J.M.; Llopis, J.; González-Ramallo, V.; Goenaga, M.Á.; Muñoz, P.; García-Leoni, M.E.; Fariñas, M.C.; Pajarón, M.; Ambrosioni, J.; Luque, R.; et al. Outpatient Parenteral Antibiotic Treatment for Infective Endocarditis: A Prospective Cohort Study From the GAMES Cohort. Clin. Infect. Dis. 2019, 69, 1690–1700. [Google Scholar] [CrossRef]
- Shah, A.B.; Norris, A.H. Handbook of Outpatient Parenteral Antimicrobial Therapy for Infectious Diseases, 3rd ed.; CRG Publishing, a Division of The Curry Rockefeller Group, LLC, and the Infectious Diseases Society of America: New York, NY, USA, 2016. [Google Scholar]
- López-Azkarreta, Í.; Martínez, A.M.; De Mandojana, M.F.M.; Martín, N.; Gil Bermejo, M.; Aznar, J.S.; Bruguera, E.V.; Cantero, M.J.P.; Gentil, P.R.; Vicente, M.D.; et al. Executive summary of outpatient parenteral antimicrobial therapy: Guidelines of the Spanish Society of Clinical Microbiology and Infectious Diseases and the Spanish Domiciliary Hospitalisation Society. Enferm. Infecc. Microbiol. Clin. 2019, 37, 405–409. [Google Scholar] [CrossRef]
- Iversen, K.; Ihlemann, N.; Gill, S.U.; Madsen, T.; Elming, H.; Jensen, K.T.; Bruun, N.E.; Høfsten, D.E.; Fursted, K.; Christensen, J.J.; et al. Partial Oral versus Intravenous Antibiotic Treatment of Endocarditis. N. Engl. J. Med. 2019, 380, 415–424. [Google Scholar] [CrossRef] [PubMed]
- Brown, E.; Gould, F.K. Oral antibiotics for infective endocarditis: A clinical review. J. Antimicrob. Chemother. 2020. [Google Scholar] [CrossRef] [PubMed]
- Norris, A.H.; Shrestha, N.; Allison, G.M.; Keller, S.C.; Bhavan, K.P.; Zurlo, J.J.; Hersh, A.L.; A Gorski, L.; A Bosso, J.; Rathore, M.H.; et al. 2018 Infectious Diseases Society of America Clinical Practice Guideline for the Management of Outpatient Parenteral Antimicrobial Therapya. Clin. Infect. Dis. 2018, 68, e1–e35. [Google Scholar] [CrossRef] [PubMed]
- Chapman, A.L.N.; Seaton, R.A.; Cooper, M.A.; Hedderwick, S.; Goodall, V.; Reed, C.; Sanderson, F.; Nathwani, D. On behalf of the BSAC/BIA OPAT Project Good Practice Recommendations Working Group Good practice recommendations for outpatient parenteral antimicrobial therapy (OPAT) in adults in the UK: A consensus statement. J. Antimicrob. Chemother. 2012, 67, 1053–1062. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andrews, M.-M.; Von Reyn, C.F. Patient Selection Criteria and Management Guidelines for Outpatient Parenteral Antibiotic Therapy for Native Valve Infective Endocarditis. Clin. Infect. Dis. 2001, 33, 203–209. [Google Scholar] [CrossRef] [Green Version]
- Rehm, S.J. Outpatient Intravenous Antibiotic Therapy for Endocarditis. Infect. Dis. Clin. N. Am. 1998, 12, 879–901. [Google Scholar] [CrossRef]
- Oliveira, P.R.; Carvalho, V.C.; Cimerman, S.; Lima, A.L.L.M. Recommendations for outpatient parenteral antimicrobial therapy in Brazil. Braz. J. Infect. Dis. 2017, 21, 648–655. [Google Scholar] [CrossRef]
- Gil-Navarro, M.V.; López-Azkarreta, Í.; Luque-Marquez, R.; Gálvez, J.; De Alarcon-Gonzalez, A. Outpatient parenteral antimicrobial therapy inEnterococcus faecalisinfective endocarditis. J. Clin. Pharm. Ther. 2017, 43, 220–223. [Google Scholar] [CrossRef]
- Cerón, I.; Bermejo, J.; Bouza, E.; Eworo, A.; Cruz, A.F.; Cuerpo, G.; Robles, J.A.G.; Vecchio, M.G.-D.; Mansilla, A.G.; González-Ramallo, V.; et al. Efficacy of daptomycin in the treatment of enterococcal endocarditis: A 5 year comparison with conventional therapy. J. Antimicrob. Chemother. 2014, 69, 1669–1674. [Google Scholar] [CrossRef] [Green Version]
- Tobudic, S.; Forstner, C.; Burgmann, H.; Lagler, H.; Ramharter, M.; Steininger, C.; Vossen, M.G.; Winkler, S.; Thalhammer, F. Dalbavancin as Primary and Sequential Treatment for Gram-Positive Infective Endocarditis: 2-Year Experience at the General Hospital of Vienna. Clin. Infect. Dis. 2018, 67, 795–798. [Google Scholar] [CrossRef]
- Escolà-Vergé, L.; Fernández-Hidalgo, N.; Rodríguez-Pardo, D.; Pigrau, C.; González-López, J.J.; Bartolomé, R.; Almirante, B. Teicoplanin for treating enterococcal infective endocarditis: A retrospective observational study from a referral centre in Spain. Int. J. Antimicrob. Agents 2019, 53, 165–170. [Google Scholar] [CrossRef] [PubMed]
- De Nadaï, T.; François, M.; Sommet, A.; Dubois, D.; Metsu, D.; Grare, M.; Marchou, B.; Delobel, P.; Martin-Blondel, G. Efficacy of teicoplanin monotherapy following initial standard therapy in Enterococcus faecalis infective endocarditis: A retrospective cohort study. Infectction 2019, 47, 463–469. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, H.; Carlson, J.R.; Matsumoto, E. Treatment of Enterococcus faecalis infective endocarditis with penicillin G plus ceftriaxone. Infect. Dis. (Auckl.) 2019, 52, 135–138. [Google Scholar] [CrossRef] [PubMed]
- Tritle, B.J.; Timbrook, T.T.; A Fisher, M.; Spivak, E.S. Penicillin as a Potential Agent for Dual Beta-lactam Therapy for Enterococcal Endocarditis. Clin. Infect. Dis. 2019, 2019, 1–2. [Google Scholar] [CrossRef]
- Gavaldà, J.; Len, O.; Miró, J.M.; Muñoz, P.; Montejo, M.; Alarcón, A.; De La Torre-Cisneros, J.; Peña, C.; Martínez-Lacasa, X.; Sarriá, C.; et al. Brief Communication: Treatment of Enterococcus faecalis Endocarditis with Ampicillin plus Ceftriaxone. Ann. Intern. Med. 2007, 146, 574–579. [Google Scholar] [CrossRef] [PubMed]
- Pericas, J.M.; Cervera, C.; Del Rio, A.; Moreno, A.; De La Maria, C.G.; Almela, M.; Falces, C.; Ninot, S.; Castaneda, X.; Armero, Y.; et al. Changes in the treatment of Enterococcus faecalis infective endocarditis in Spain in the last 15 years: From ampicillin plus gentamicin to ampicillin plus ceftriaxone. Clin. Microbiol. Infect. 2014, 20, O1075–O1083. [Google Scholar] [CrossRef] [Green Version]
- Carugati, M.; Bayer, A.S.; Miró, J.M.; Park, L.P.; Guimarães, A.C.; Skoutelis, A.; Fortes, C.Q.; Durante-Mangoni, E.; Hannan, M.M.; Nacinovich, F.; et al. High-Dose Daptomycin Therapy for Left-Sided Infective Endocarditis: A Prospective Study from the International Collaboration on Endocarditis. Antimicrob. Agents Chemother. 2013, 57, 6213–6222. [Google Scholar] [CrossRef] [Green Version]
- Pericas, J.M.; Cervera, C.; Moreno, A.; García-De-La-Mària, C.; Almela, M.; Falces, C.; Quintana, E.; Vidal, B.; Llopis, J.; Fuster, D.; et al. Outcome of Enterococcus faecalis infective endocarditis according to the length of antibiotic therapy: Preliminary data from a cohort of 78 patients. PLoS ONE 2018, 13, e0192387. [Google Scholar] [CrossRef] [Green Version]
- El Rafei, A.; DeSimone, D.C.; Narichania, A.D.; Sohail, M.R.; Vikram, H.R.; Li, Z.; Steckelberg, J.M.; Wilson, W.R.; Baddour, L.M. Comparison of Dual β-Lactam therapy to penicillin-aminoglycoside combination in treatment of Enterococcus faecalis infective endocarditis. J. Infect. 2018, 77, 398–404. [Google Scholar] [CrossRef]
- Fernández-Hidalgo, N.; Almirante, B.; Gavaldà, J.; Gurgui, M.; Peña, C.; De Alarcón, A.; Ruiz, J.; Vilacosta, I.; Montejo, M.; Vallejo, N.; et al. Ampicillin Plus Ceftriaxone Is as Effective as Ampicillin Plus Gentamicin for TreatingEnterococcus faecalisInfective Endocarditis. Clin. Infect. Dis. 2013, 56, 1261–1268. [Google Scholar] [CrossRef] [Green Version]
- Bassetti, M.; Russo, A.; Givone, F.; Ingani, M.; Graziano, E.; Bassetti, M. Should High-dose Daptomycin be an Alternative Treatment Regimen for Enterococcal Endocarditis? Infect. Dis. Ther. 2019, 8, 695–702. [Google Scholar] [CrossRef] [Green Version]
- Dahl, A.; Rasmussen, R.V.; Bundgaard, H.; Hassager, C.; Bruun, L.E.; Lauridsen, T.K.; Moser, C.; Sogaard, P.; Arpi, M.; Bruun, N.E. Enterococcus faecalis Infective Endocarditis. Circulation 2013, 127, 1810–1817. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hidalgo-Tenorio, C.; Vinuesa, D.; Plata, A.; Dávila, P.M.; Iftime, S.; Sequera, S.; Loeches, B.; López-Azkarreta, Í.; Fariñas, M.C.; Fernández-Roldan, C.; et al. DALBACEN cohort: Dalbavancin as consolidation therapy in patients with endocarditis and/or bloodstream infection produced by gram-positive cocci. Ann. Clin. Microbiol. Antimicrob. 2019, 18, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Presterl, E.; Graninger, W.; Georgopoulos, A. The efficacy of teicoplanin in the treatment of endocarditis caused by Gram-positive bacteria. J. Antimicrob. Chemother. 1993, 31, 755–766. [Google Scholar] [CrossRef]
- Lebeaux, D.; Fernández-Hidalgo, N.; Pilmis, B.; Tattevin, P.; Mainardi, J.-L. Aminoglycosides for infective endocarditis: Time to say goodbye? Clin. Microbiol. Infect. 2019. [Google Scholar] [CrossRef]
- Olaison, L. Enterococcal Endocarditis in Sweden, 1995–1999: Can Shorter Therapy with Aminoglycosides Be Used? Clin. Infect. Dis. 2002, 34, 159–166. [Google Scholar] [CrossRef] [Green Version]
- Maher, M.; Jensen, K.J.; Lee, D.; Nix, D.E. Stability of Ampicillin in Normal Saline and Buffered Normal Saline. Int. J. Pharm. Compd. 2016, 20, 338–342. [Google Scholar]
- Kang, M.A.; Kang, J.-S. Stability Test of Ampicillin Sodium Solutions in the Accufuser® Elastomeric Infusion Device Using HPLC: UV Method. Pharmacol. Pharm. 2012, 3, 462–467. [Google Scholar] [CrossRef] [Green Version]
- Herrera-Hidalgo, L.; López-Cortes, L.E.; Luque-Márquez, R.; Gálvez-Acebal, J.; De Alarcón, A.; Gutiérrez-Valencia, A.; Gil-Navarro, M.V.; López-Cortes, L.F. Ampicillin and Ceftriaxone Solution Stability at Different Temperatures in Outpatient Parenteral Antimicrobial Therapy. Antimicrob. Agents Chemother. 2020, 64, 1–7. [Google Scholar] [CrossRef]
- Gavaldà, J.; Torres, C.; Tenorio, C.; López, P.; Zaragoza, M.; Capdevila, J.A.; Almirante, B.; Ruiz, F.; Borrell, N.; Gomis, X.; et al. Efficacy of Ampicillin plus Ceftriaxone in Treatment of Experimental Endocarditis Due to Enterococcus faecalis Strains Highly Resistant to Aminoglycosides. Antimicrob. Agents Chemother. 1999, 43, 639–646. [Google Scholar] [CrossRef] [Green Version]
- Liao, C.-H.; Huang, Y.-T.; Tsai, H.-Y.; Hsueh, P.-R. In vitro synergy of ampicillin with gentamicin, ceftriaxone and ciprofloxacin against Enterococcus faecalis. Int. J. Antimicrob. Agents 2014, 44, 85–86. [Google Scholar] [CrossRef]
- Spellberg, B.; Chambers, H.F.; Musher, D.M.; Walsh, T.L.; Bayer, A.S. Evaluation of a Paradigm Shift From Intravenous Antibiotics to Oral Step-Down Therapy for the Treatment of Infective Endocarditis. JAMA Intern. Med. 2020, 180, 769–777. [Google Scholar] [CrossRef]
- Kobayashi, T.; Ando, T.; Streit, J.; Sekar, P. Current Evidence on Oral Antibiotics for Infective Endocarditis: A Narrative Review. Cardiol. Ther. 2019, 8, 167–177. [Google Scholar] [CrossRef] [Green Version]
- Colli, A.; Campodonico, R.; Gherli, T. Early Switch From Vancomycin to Oral Linezolid for Treatment of Gram-Positive Heart Valve Endocarditis. Ann. Thorac. Surg. 2007, 84, 87–91. [Google Scholar] [CrossRef] [PubMed]
- Muñoz, P.; Rodríguez-Creixems, M.; Moreno, M.; Marin, M.; González-Ramallo, V.; Bouza, E.; GAME Study Group; Garcia-Pavia, P. Linezolid therapy for infective endocarditis. Clin. Microbiol. Infect. 2007, 13, 211–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernández-Hidalgo, N.; Escolà-Vergé, L.; Pericas, J.M. Enterococcus faecalis endocarditis: What’s next? Future Microbiol. 2020, 15, 349–364. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, U.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, 332–336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schünemann, H.J.; Tugwell, P.; Reeves, B.C.; Akl, E.A.; Santesso, N.; Spencer, F.A.; Shea, B.; Wells, G.; Helfand, M. Non-randomized studies as a source of complementary, sequential or replacement evidence for randomized controlled trials in systematic reviews on the effects of interventions. Res. Synth. Methods 2013, 4, 49–62. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Altman, U.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.C.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355. [Google Scholar] [CrossRef] [Green Version]
- NIH Study Quality Assessment Tools n.d. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 31 October 2019).
- Ryan, R. Group Cochrane Consumers and Communication Review. Cochrane Consumers and Communication Review Group: Data synthesis and analysis n.d. Available online: https://cccrg.cochrane.org/ (accessed on 31 October 2019).



{kind=link}
{kind=link}
| Ref | Study Design/Setting | Endocarditis Type and Definition | Follow-Up Period | Dose Regimen | EFIE/Total Patients | Surgical Treatment | Adverse Events | Clinical Outcomes | Key Finding | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mortality | Relapses | Others | |||||||||
| Aminoglycoside based regimen | |||||||||||
| [28] | Prospective cohort study with comparator/Inpatient | LS-NVE 28/43 LS-PVE 15/43 Modified Duke criteria | 6 months | Initial therapy A/V plus G | 43/149 | 26/43 (60.5%) | ND | Overall 15/43 (35%) In hospital 6/43 (14%) | ND | Days of bacteriemia 3.0 (1.5–5.0) b | High-dose daptomycin may be a valid alternative to standard therapy for left-side E. faecalis IE |
| [29] | Retrospective cohort study with comparator/Inpatient | NVE 9/9 Modified Duke criteria | 1 year | Initial therapy A 2 g/4 h plus G 3 mg/kg/day for 4 weeks | 9/9 | 2/9 (22.2%) | 2/9 (22%) | 1-year 3/9 (33%) In hospital 3/9 (33%) | 1/9 (11%) | Discontinuation of AB therapy 2/9 (22%) | The suitability of a short course of antibiotic treatment for uncomplicated E. faecalis IE should be readdressed. |
| NVE 14/23 PVE 9/23 Modified Duke criteria | Initial therapy A 2 g/4 h plus G 3 mg/kg/day for 6 weeks | 23/23 | 14/23 (60.8%) | 2/23 (8%) | 1-year 7/23 (30%) In hospital 6/23 (26%) | 1/23 (4%) | Discontinuation of AB therapy 9/23 (39.1%) | ||||
| [33] | Retrospective cohort study with comparator/Inpatient | LSE ND | 1 year | Initial therapy PG/A for 4–6 weeks plus G 3 mg/kg/day for 2 weeks | 43/43 | 15/43 | eGFR change −1 (−13 to 4) b mL/min | In hospital 2/43 (5%) | 2/43 (5%) | 1 year evento-free survival 27/43 (69%) | G treatment for 2 weeks, rather than 4–6 weeks, seems adequate and preferable in susceptible E. faecalis IE |
| Initial therapy PG/A plus G 3 mg/kg/day for 4–6 weeks | 41/41 | 14/41 (34.1%) | eGFR change −11(−25 to−3) b mL/min | In hospital 4/41 (10%) | 3/41 (7%) | 1 year evento-free survival 27/41 (66%) | |||||
| [30] | Retrospective cohort study with comparator/Inpatient | All types (ND) Modified Duke criteria | 1 year | Initial therapy A 2 g/4 h plus G 3 mg/kg/day for 4–6 weeks | 67/67 | 24/67 (35.8%) | 20/67 (66%) | 1-year 11/67 (17%) 3 months 9/67 (14%) | 1/67 (3%) | Fail to complete therapy 30/67 (49%) | AC is a safe alternative to AG for treating E. faecalis IE |
| [27] | Retrospective cohort study with comparator/Inpatient | NVE 20/30 PVE 9/30 CDRE 1/30 Modified Duke criteria | 392 (118.5–792.0) b days | Initial therapy A 2 g/4 h plus G 3 mg/kg/day for 4–6 weeks | 30/30 | 15/30 (50%) | Renal failure 19/30 (64%) | 1-year 9/30 (30%) In hospital 8/30 (27%) | 2/30 (3%) | Discontinuation due to toxicity 13/30 (43%) | The efficacy of 6 weeks treatment with AC appears similar and safer than 4–6 weeks treatment with AG |
| [31] | Prospective cohort study with comparator/Inpatient | NVE 57/87 PVE 30/87 Modified Duke criteria | 11.1 (4.4–22.5) b months | Initial therapy A 2 g/4 h plus G 3 mg/kg/day for 4–6 weeks | 87/87 | 35/87 (40.2%) | 38/87 (44%) | Overall 22/87 (25%) During treatment 8/87 (21%) | 3/87 (3.4%) | Treatment change 2/87 (2%) | AC combination was as effective as AG, with less adverse events. |
| Dual β-lactam regimens | |||||||||||
| [20] | Retrospective cohort study with comparator/Inpatient and outpatient | LS-NVE 10/21 LS-PVE 9/21 RSE 2/21 Modified Duke criteria | During antibiotic therapy | Initial treatment A 2 g/6 h + C 2 g/12 h | 21/21 | 4/21 (19%) | 0% | 9/21 (43%) | ND | Treatment change 0/21 (0%) Days of bacteraemia 1 (1–6) b | Daptomycin treatment for enterococcal endocarditis lead to worse outcomes than AC therapy |
| [19] | Case series study without comparator/Outpatient | LS-NVE 4/4 ND | 365 (221–406) b days | Continuation therapy A 2 g/4 h plus C 4 g/24 h for 6 weeks antibiotic therapy | 4/4 | 3/4(75%) | 0/4(0%) | 0/4 (0%) | 0/4(0%) | Treatment change 0/4(0%) | A high single daily dose of C plus A could be an option as a continuation therapy in an OPAT program for E. faecalis IE. |
| [29] | Retrospective cohort study with comparator/Inpatient | NVE 14/14 Modified Duke criteria | 1 year | Initial therapy A 2 g/4 h plus C 2 g/12 h for 4 weeks | 14/14 | 3/14 (21.4%) | 2/14 (14%) | 1-year 3/14 (21%) In hospital 2/14 (14%) | 2/14 (14%) | Discontinuation of AB therapy 1/14 (7.1%) | The suitability of a short course of antibiotic treatment for uncomplicated EFIE should be readdressed. |
| NVE 14/32 PVE 18/32 Modified Duke criteria | Initial therapy A 2 g/4 h plus C 2 g/12 h for 6 weeks | 32/32 | 14/32 (43.7%) | 1/32 (3%) | 1-year 8/32 (25%) In hospital 8/32 (25%) | 0/32 (0%) | Discontinuation of AB therapy 1/32 (3.1%) | ||||
| [30] | Retrospective cohort study with comparator/Inpatient | All types (ND) Modified Duke criteria | 1 year | Initial therapy A 2 g/4 h plus C 2 g/12 h for 4–6 weeks | 18/18 | 3/18 (16.6%) | 1/18 (20%) | 1-year 3/18 (17%) 3 months 3/18 (17%) | 1/18 (14%) | Fail to complete therapy 5/18 (28%) | AC is a safe alternative to AG for treating E. faecalis IE |
| [27] | Retrospective cohort study with comparator/Inpatient | NVE 25/39 PVE 13/39 CDRE 1/39 Modified Duke criteria | 392 (118.5–792.0) b days | Initial therapy A 2 g/4 h plus C 2 g/12 h for 4–6 weeks | 39/39 | 15/39 (39%) | Renal failure 13/39 (34%) | In-hospital 9/39 (23%) 1-year 10/39 (26%) | 3/39 (8%) | Discontinuation due to toxicity 1/39 (3%) | The efficacy of 6 weeks treatment with AC appears similar and safer than 4–6 weeks treatment with AG |
| [31] | Prospective cohort study with comparator/Inpatient | NVE 98/159 PVE 59/159 CDRE 2/159 Modified Duke criteria | 11.1 (4.4–22.5) b months | Initial therapy A 2 g/4 h plus C 2 g/12 h for 4–6 weeks | 159/159 | 53/159 (33.3%) | 14/159 (9%) | Overall 42/159 (26%) During treatment 35/159 (22%) | 3/159 (1.8%) | Treatment change 2/159 (1%) | AC combination was as effective as AG, with less adverse events. |
| [26] | Non randomized clinical trial without comparator/Inpatient | All types(ND) Modified Duke criteria | 3 months | Initial therapy A 2 g/4 h plus C 2 g/12 h for 42 (5–48)b days | 43/43 | 7/43 (16.3%) | 2/43 (4.6%) | Overall 12/43 (28%) During treatment 10/43 (23%) | 2/43 (4.6%) | ND | AC may be a treatment option for E. faecalis endocarditis |
| [24] | Case series study without comparator/Outpatient | NVE 3/4 PVE 1/4 Modified Duke criteria | 6 months | Continuation therapy PG 24 million U PC/24 h plus C 2 g/12 h for 6–8 weeks antibiotic treatment | 4/4 | 0/4 (0%) | 1/4 (25%) | 0/4 (0%) | 0/4 (0%) | ND | PG plus C would be effective in the treatment of E. faecalis IE |
| [25] | Case series study without comparator/Outpatient | ND | 3 months | PG 18–24 million U PC/24 h plus C 2 g/12 h for 6 weeks antibiotic therapy | 3/3 | ND | 0/3 (0%) | 0/3 (0%) | 0/3 (0%) | Treatment change 0/3 (0%) | PG plus C maybe an alternative for the treatment of E. faecalis IE |
| Teicoplanin based regimens | |||||||||||
| [22] | Retrospective cohort study without comparator/ Inpatient and outpatient | NVE 16/22 PVE 5/22 Non valvular E 1/22 Modified Duke criteria | 3 months | First- line (1/14) Salvage therapy (13/14) LD + 10 (10–10.8) b mg/kg/day for 43.5 (38.8–56.3) days b | 14/22 | 3/14 (21.4%) | 2/14 (14%) | During treatment 1/14 (7.1%) 3 months 2/14 (14%) | 0/14 (0%) | Treatment change 2/14 (14%) | Teicoplanin can be used in E. faecalis IE as a sequential treatment |
| [23] | Retrospective cohort study with comparator/Inpatient and outpatient | NVE 21/37 PVE 16/37 Modified Duke criteria | 783 (126–1227) b days | Continuation therapy LD + 5.8 mg/kg/day 39 (25–34) b days antibiotic therapy | 37/37 | 11/37 (30%) | ND | Global 14/37 (38%) IE-related 3/37 (8%) | 3/37 (8%) | Patients who did not die from E. faecalis IE or experience relapses 33/37 (89%) | Teicoplanin sequential treatment appears to be effective in selected patients |
| [35] | Case series study without comparator/Inpatient | All type ND | 6 months | Initial therapy 600 mg/day for 5–6 weeks | 5/26 | ND | ND | 0/5 (0%) | ND | ND | Teicoplanin initial treatment was effective for E. faecalis IE |
| Daptomycin based regimens | |||||||||||
| [20] | Retrospective cohort study with comparator/Inpatient and outpatient | LS-NVE 4/6 LS-PVE 1/6 CDRE 1/6 Modified Duke criteria | During antibiotic therapy | Initial therapy (1/5) Salvage (4/5) 8.5 (6–10) mg/kg/day | 5/6 | 3/6 (50%) | 0% | 1/6 (16.7%) | ND | Treatment change 4/5 (80%) a Days of bacteriemia 6 (1–13) b | Daptomycin treatment for enterococcal endocarditis lead to worse outcomes than AC therapy |
| [28] | Prospective cohort study with comparator/Inpatient | LS-NVE 7/9 RS-NVE 2/9 Modified Duke criteria | 6 months | Initial (8/9) or salvage (1/9) 8.3 (7.1–9.4) b mg/kg for 28.5 (22.0–42.5)b alone or in combination | 9/29 | 4/9 (44.4%) | 0/9 (0%) | Overall 2/9 (22%) In-hospital 1/9 (11.1%) | ND | Days of bacteriemia 2.0 (1.5–3.0) b | High-dose daptomycin may be a valid alternative to standard therapy for left-side E. faecalis IE |
| [32] | Retrospective cohort study with comparator/Inpatient | NVE 8/12 PVE 4/12 Modified Duke criteria | 30 days | First-line or salvage therapy with daptomycin-based regimen 10.125 (8–12) b mg/kg for 45 ± 21.1 days | 12/16 | 7/16 (43.7%) | ND | 30-days 0/12 (0%) | 2/12 (0%) | Treatment failure 0/12 (0%) | Daptomycin could be an alternative treatment option for enterococcal NVE and PVE. |
| Dalbavancin based regimen | |||||||||||
| [21] | Case series study without comparator/Inpatient and outpatient | NVE 3/4 PVE 1/4 Modified Duke criteria | 6 months | Initial, salvage or continuation therapy LD (1000–1500 mg) plus 500–1000 mg once or twice weekly for 1 to >6 weeks | 4/27 | ND | 0/4 (0%) | 1/4 (25%) | ND | Treatment failure 1/4 (25%) | Dalbavancin is effective and safe for prolonged treatment. |
| [34] | Retrospective cohort study without comparator/Outpatient | NVE 2/3 PVE 1/3 Modified Duke criteria | 1 year | Continuation therapy 500–1500 mg between 1 and 4 doses | 3/34 | 12/34 | 0/3 | 0/3 | 0/3 | Cure of infection 3/3 | Dalbavancin is an effective consolidation antibiotic therapy in clinically stabilized patients with IE |
| Oral therapy | |||||||||||
| [12] | Randomized clinical trial with comparator/Outpatient | LSE Modified Duke criteria | 6 months | Continuation therapy with oral antibiotics with amoxicillin alone or plus moxifloxacin/linezolid/rifampicin/ciprofloxacin or moxifloxacin plus linezolid for 17 (14–25) days b | 51/201 | 15/51 (29.4%) | 10/201 (5%) | All-cause 1/51 (1.9%) | 3/51 (5.8%) | AB route change 4/201 (1.9%) Composite endpoint c 4/51 (7.8%) | Continuation therapy with oral antibiotics is non-inferior than intravenous therapy |
| Study | Risk of Bias Due To | ||||||||||
| Tool | Confounding | Selection of Participants | Classification of Interventions | Deviations from Intended Interventions | Missing Data | Measurement of Outcomes | Selection of the Reported Result | Overall Bias | |||
| [20] | Robins | S | L | L | M | L | M | M | S | ||
| [21] | S | L | L | S | M | M | L | S | |||
| [22] | M | L | L | L | L | L | L | M | |||
| [23] | M | L | L | L | M | L | M | M | |||
| [29] | M | L | L | NI | L | M | M | M | |||
| [33] | M | L | L | L | L | L | L | M | |||
| [28] | M | L | L | L | NI | L | L | M | |||
| [30] | M | L | L | M | L | L | L | M | |||
| [27] | M | L | L | M | L | L | L | M | |||
| [26] | L | L | L | NI | L | L | L | L | |||
| [31] | M | L | L | M | L | L | L | M | |||
| [32] | M | L | M | NI | NI | L | L | M | |||
| [34] | M | L | M | NI | L | L | L | M | |||
| Study | Tool | Randomization Process | Deviations from Intended Interventions | Missing Data | Measurement of Outcomes | Selection of the Reported Result | Overall Bias | ||||
| [12] | ROB-2 | L | SC | L | L | SC | SC | ||||
| Study | Tool | Study Question | Population | Consecutive | Cases Comparable | Intervention | Measurement of Outcomes | Length of Follow Up | Statistical Methods | Results | Overall |
| [19] | SQAT | Y | Y | Y | Y | Y | Y | Y | NA | Y | GOOD |
| [35] | Y | Y | NR | Y | Y | Y | Y | NR | Y | GOOD | |
| [24] | Y | Y | Y | Y | Y | Y | Y | NA | Y | GOOD | |
| [25] | Y | Y | Y | Y | Y | N | Y | NA | N | POOR | |
| Inclusion Criteria | Exclusion Criteria | |
|---|---|---|
| Design | Randomized controlled trials, non-randomized trials and observational studies | Case report, in vivo studies, in vitro studies and non-primary sources |
| Population | Patients suffering from E. faecalis IE | Non-human studies |
| Intervention/comparator | Antibiotic treatment alternatives | Non-medical approaches (e.g., Surgery) |
| Context | Outpatient setting * or continuation treatment | - |
| Outcome | Mortality, relapses, clinical cure, microbiological cure | Any outcome identify by antibiotic treatment and causative microorganism |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Herrera-Hidalgo, L.; de Alarcón, A.; López-Cortes, L.E.; Luque-Márquez, R.; López-Cortes, L.F.; Gutiérrez-Valencia, A.; Gil-Navarro, M.V. Enterococcus faecalis Endocarditis and Outpatient Treatment: A Systematic Review of Current Alternatives. Antibiotics 2020, 9, 657. https://doi.org/10.3390/antibiotics9100657
Herrera-Hidalgo L, de Alarcón A, López-Cortes LE, Luque-Márquez R, López-Cortes LF, Gutiérrez-Valencia A, Gil-Navarro MV. Enterococcus faecalis Endocarditis and Outpatient Treatment: A Systematic Review of Current Alternatives. Antibiotics. 2020; 9(10):657. https://doi.org/10.3390/antibiotics9100657
Chicago/Turabian StyleHerrera-Hidalgo, Laura, Arístides de Alarcón, Luis E. López-Cortes, Rafael Luque-Márquez, Luis F. López-Cortes, Alicia Gutiérrez-Valencia, and María V. Gil-Navarro. 2020. "Enterococcus faecalis Endocarditis and Outpatient Treatment: A Systematic Review of Current Alternatives" Antibiotics 9, no. 10: 657. https://doi.org/10.3390/antibiotics9100657