Hospitalization for Acute Respiratory Tract Infection in a Low-Antibiotic-Prescribing Setting: Cross-Sectional Data from General Practice

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Trial Design
- Being insured with the German statutory health insurance company AOK, the provider of data. Within a typical primary care setting of the participating regional areas, at least 40% of all patients are insured with AOK. Despite some socio-economic differences, research showed that AOK data is adequate for analyzing patterns of health care utilization [19].
- A minimum age of 3 months, though children and teenagers up to 17 years of age were excluded from this analysis.
- A physician consultation visit due to an episode of ARTI according to the ICD classes J00-J04, J06, J13, J20, J22, whilst being otherwise healthy.
2.2. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Butler, C.C.; Hood, K.; Verheij, T.; Little, P.; Melbye, H.; Nuttall, J.; Kelly, M.J.; Mölstad, S.; Godycki-Cwirko, M.; Almirall, J.; et al. Variation in antibiotic prescribing and its impact on recovery in patients with acute cough in primary care: Prospective study in 13 countries. BMJ 2009, 338, b2242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goossens, H.; Ferech, M.; Vander Stichele, R.; Elseviers, M.; ESAC Project Group. Outpatient antibiotic use in Europe and association with resistance: A cross-national database study. Lancet 2005, 365, 579–587. [Google Scholar] [CrossRef]
- Little, P.; Stuart, B.; Moore, M.; Coenen, S.; Butler, C.C.; Godycki-Cwirko, M.; Mierzecki, A.; Chlabicz, S.; Torres, A.; Almirall, J.; et al. Amoxicillin for acute lower-respiratory-tract infection in primary care when pneumonia is not suspected: A 12-country, randomised, placebo-controlled trial. Lancet Infect. Dis. 2013, 13, 123–129. [Google Scholar] [CrossRef]
- Coenen, S.; Ferech, M.; Haaijer-Ruskamp, F.M.; Butler, C.C.; Vander Stichele, R.H.; Verheij, T.J.M.; Monnet, D.L.; Little, P.; Goossens, H. European Surveillance of Antimicrobial Consumption (ESAC): Quality indicators for outpatient antibiotic use in Europe. Qual. Saf. Health Care 2007, 16, 440–445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Centre for Disease Prevention and Control. Summary of the Latest Data on Antibiotic Consumption in EU: 2017; European Centre for Disease Prevention and Control: Stockholm, Sweden, 2017. [Google Scholar]
- WHO. Antimicrobial Resistance: Global Report on Surveillance; WHO: Geneva, Switzerland, 2014. [Google Scholar]
- Adriaenssens, N.; Coenen, S.; Versporten, A.; Muller, A.; Minalu, G.; Faes, C.; Vankerckhoven, V.; Aerts, M.; Hens, N.; Molenberghs, G.; et al. European Surveillance of Antimicrobial Consumption (ESAC): Outpatient antibiotic use in Europe (1997–2009). J. Antimicrob. Chemother. 2011, 66, vi3–vi12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silverman, M.A.; Konnikova, L.; Gerber, J.S. Impact of Antibiotics on Necrotizing Enterocolitis and Antibiotic-Associated Diarrhea. Gastroenterol. Clin. N. Am. 2017, 46, 61–76. [Google Scholar] [CrossRef] [Green Version]
- Kenealy, T.; Arroll, B. Antibiotics for the common cold and acute purulent rhinitis. Cochrane Database Syst. Rev. 2013, 6. [Google Scholar] [CrossRef] [PubMed]
- Butler, C.C.; Rollnick, S.; Pill, R.; Maggs-Rapport, F.; Stott, N. Understanding the culture of prescribing: Qualitative study of general practitioners’ and patients’ perceptions of antibiotics for sore throats. BMJ 1998, 317, 637–642. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gonzales, R.; Steiner, J.F.; Sande, M.A. Antibiotic prescribing for adults with colds, upper respiratory tract infections, and bronchitis by ambulatory care physicians. JAMA 1997, 278, 901–904. [Google Scholar] [CrossRef] [PubMed]
- Himmel, W.; Lippert-Urbanke, E.; Kochen, M.M. Are patients more satisfied when they receive a prescription? The effect of patient expectations in general practice. Scand. J. Prim. Health Care 1997, 15, 118–122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coxeter, P.; Del Mar, C.B.; McGregor, L.; Beller, E.M.; Hoffmann, T.C. Interventions to facilitate shared decision making to address antibiotic use for acute respiratory infections in primary care. Cochrane Database Syst. Rev. 2015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Köchling, A.; Löffler, C.; Reinsch, S.; Hornung, A.; Böhmer, F.; Altiner, A.; Chenot, J.-F. Reduction of antibiotic prescriptions for acute respiratory tract infections in primary care: A systematic review. Implement. Sci. 2018, 13, 47. [Google Scholar] [CrossRef] [PubMed]
- Gulliford, M.C.; Moore, M.V.; Little, P.; Hay, A.D.; Fox, R.; Prevost, A.T.; Juszczyk, D.; Charlton, J.; Ashworth, M. Safety of reduced antibiotic prescribing for self limiting respiratory tract infections in primary care: Cohort study using electronic health records. BMJ 2016, 354, i3410. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Price, D.B.; Honeybourne, D.; Little, P.; Mayon-White, R.T.; Read, R.C.; Thomas, M.; Wale, M.C.; FitzGerald, P.; Weston, A.R.; Winchester, C.C. Community-acquired pneumonia mortality: A potential link to antibiotic prescribing trends in general practice. Respir. Med. 2004, 98, 17–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Little, P.; Stuart, B.; Smith, S.; Thompson, M.J.; Knox, K.; van den Bruel, A.; Lown, M.; Moore, M.; Mant, D. Antibiotic prescription strategies and adverse outcome for uncomplicated lower respiratory tract infections: Prospective cough complication cohort (3C) study. BMJ 2017, 357, j2148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Altiner, A.; Berner, R.; Diener, A.; Feldmeier, G.; Köchling, A.; Löffler, C.; Schröder, H.; Siegel, A.; Wollny, A.; Kern, W.V. Converting habits of antibiotic prescribing for respiratory tract infections in German primary care-the cluster-randomized controlled CHANGE-2 trial. BMC Fam. Pract. 2012, 13, 124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jaunzeme, J.; Eberhard, S.; Geyer, S. Wie „repräsentativ“ sind GKV-Daten? [How “representative” are SHI (statutory health insurance) data?]. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 2013, 56, 447–454. [Google Scholar] [CrossRef] [PubMed]
- The R Core Team. A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2018. [Google Scholar]
- Osterloh, F. Medizinische Versorgungszentren: Eine Alternative, keine Konkurrenz. Dtsch. Arztebl. 2017, 114. A1901/B-1613/C-1579. [Google Scholar]
- Smith, S.M.; Fahey, T.; Smucny, J.; Becker, L.A. Antibiotics for Acute Bronchitis. Cochrane Database Syst. Rev. 2017. [Google Scholar] [CrossRef] [PubMed]
- Spurling, G.K.P.; Del Mar, C.B.; Dooley, L.; Foxlee, R.; Farley, R. Delayed antibiotic prescriptions for respiratory infections. Cochrane Database Syst. Rev. 2017. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Variables | n | % |
|---|---|---|
| LRTI (bronchitis) | 711 | 19.4 |
| Pneumonia | 34 | 0.9 |
| Viral infection | 436 | 11.9 |
| Breathlessness | 65 | 1.8 |
| Severity of disease | ||
| Mild or moderate mild | 2466 | 67.2 |
| Moderate severe or severe | 1203 | 32.8 |
| Type of practice | ||
| Single-handed | 2938 | 80.1 |
| Group practice | 731 | 19.9 |
| Physician specialization | ||
| General practitioner | 3228 | 88.0 |
| Primary care internist | 441 | 12.0 |
| Antibiotic prescription within initial consultation | 569 | 15.5 |
| Condition | Number |
|---|---|
| ARTI directly related (e.g., pneumonia) | 18 |
| Antibiotic prescribing related (e.g., enterocolitis due to Clostridium difficile) | 1 |
| Sepsis | 1 |
| Gastrointestinal diseases | 4 |
| Cardiovascular diseases | 10 |
| Musculoskeletal disorders and fractures | 7 |
| Other | 30 |
| Total | 71 |
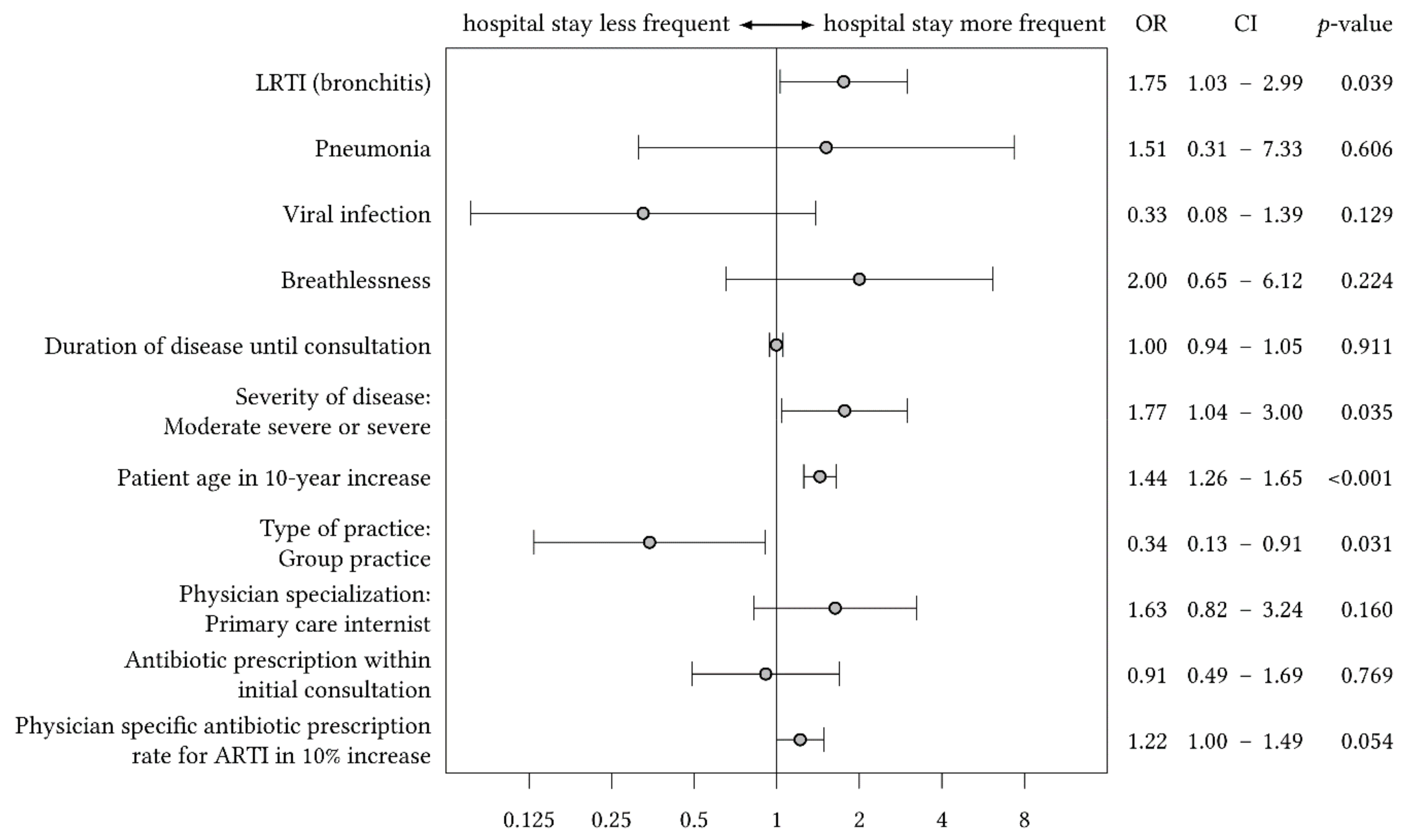
| Variable | OR | 2.5% CI | 97.5% CI | p-Value |
|---|---|---|---|---|
| LRTI (bronchitis) | 1.75 | 1.03 | 2.99 | 0.039 |
| Pneumonia | 1.51 | 0.31 | 7.33 | 0.606 |
| Viral infection | 0.33 | 0.08 | 1.39 | 0.129 |
| Breathlessness | 2.00 | 0.66 | 6.12 | 0.224 |
| Duration of disease until consultation | 1.00 | 0.94 | 1.05 | 0.911 |
| Severity of disease | ||||
| Mild or moderate mild | 1 | |||
| Moderate severe or severe | 1.77 | 1.04 | 3.00 | 0.035 |
| Patient age in 10-year increase | 1.44 | 1.26 | 1.65 | <0.001 |
| Type of practice | ||||
| Single-handed | 1 | |||
| Group practice | 0.34 | 0.13 | 0.91 | 0.031 |
| Physician specialization | ||||
| General practitioner | 1 | |||
| Primary care internist | 1.63 | 0.83 | 3.24 | 0.160 |
| Antibiotic prescription within initial consultation | 0.91 | 0.49 | 1.69 | 0.769 |
| Physician specific antibiotic prescription rate for ARTI in 10% increase | 1.22 | 1.00 | 1.49 | 0.054 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Löffler, C.; Altiner, A.; Diener, A.; Berner, R.; Feldmeier, G.; Helbig, C.; Kern, W.V.; Köchling, A.; Schmid, M.; Schön, G.; et al. Hospitalization for Acute Respiratory Tract Infection in a Low-Antibiotic-Prescribing Setting: Cross-Sectional Data from General Practice. Antibiotics 2020, 9, 653. https://doi.org/10.3390/antibiotics9100653
Löffler C, Altiner A, Diener A, Berner R, Feldmeier G, Helbig C, Kern WV, Köchling A, Schmid M, Schön G, et al. Hospitalization for Acute Respiratory Tract Infection in a Low-Antibiotic-Prescribing Setting: Cross-Sectional Data from General Practice. Antibiotics. 2020; 9(10):653. https://doi.org/10.3390/antibiotics9100653
Chicago/Turabian StyleLöffler, Christin, Attila Altiner, Annette Diener, Reinhard Berner, Gregor Feldmeier, Christian Helbig, Winfried V. Kern, Anna Köchling, Michaela Schmid, Gerhard Schön, and et al. 2020. "Hospitalization for Acute Respiratory Tract Infection in a Low-Antibiotic-Prescribing Setting: Cross-Sectional Data from General Practice" Antibiotics 9, no. 10: 653. https://doi.org/10.3390/antibiotics9100653