Prediction of Sudden Cardiac Death Risk with a Support Vector Machine Based on Heart Rate Variability and Heartprint Indices




Abstract
:1. Introduction
2. Materials and Methods
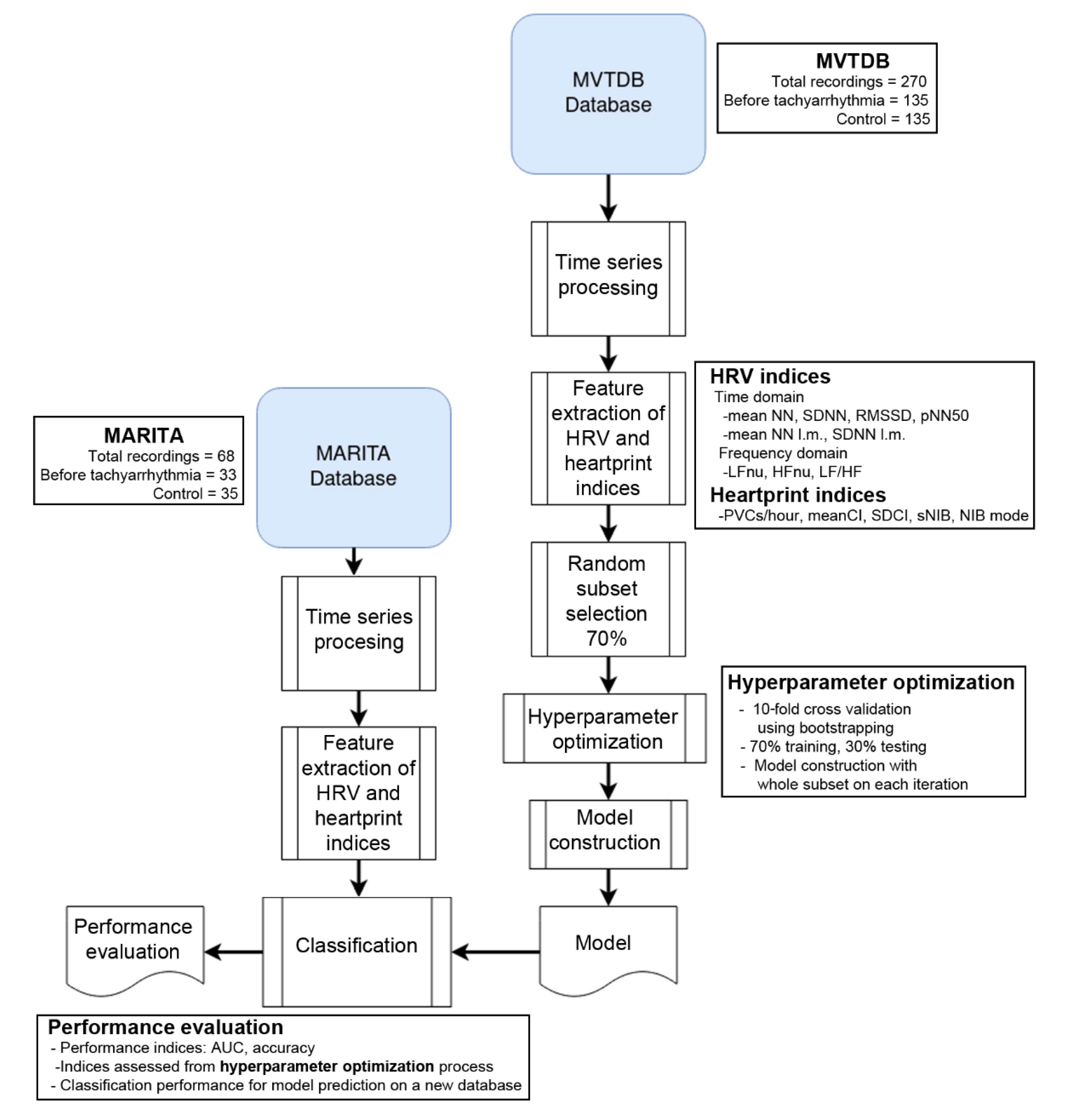
2.1. Data
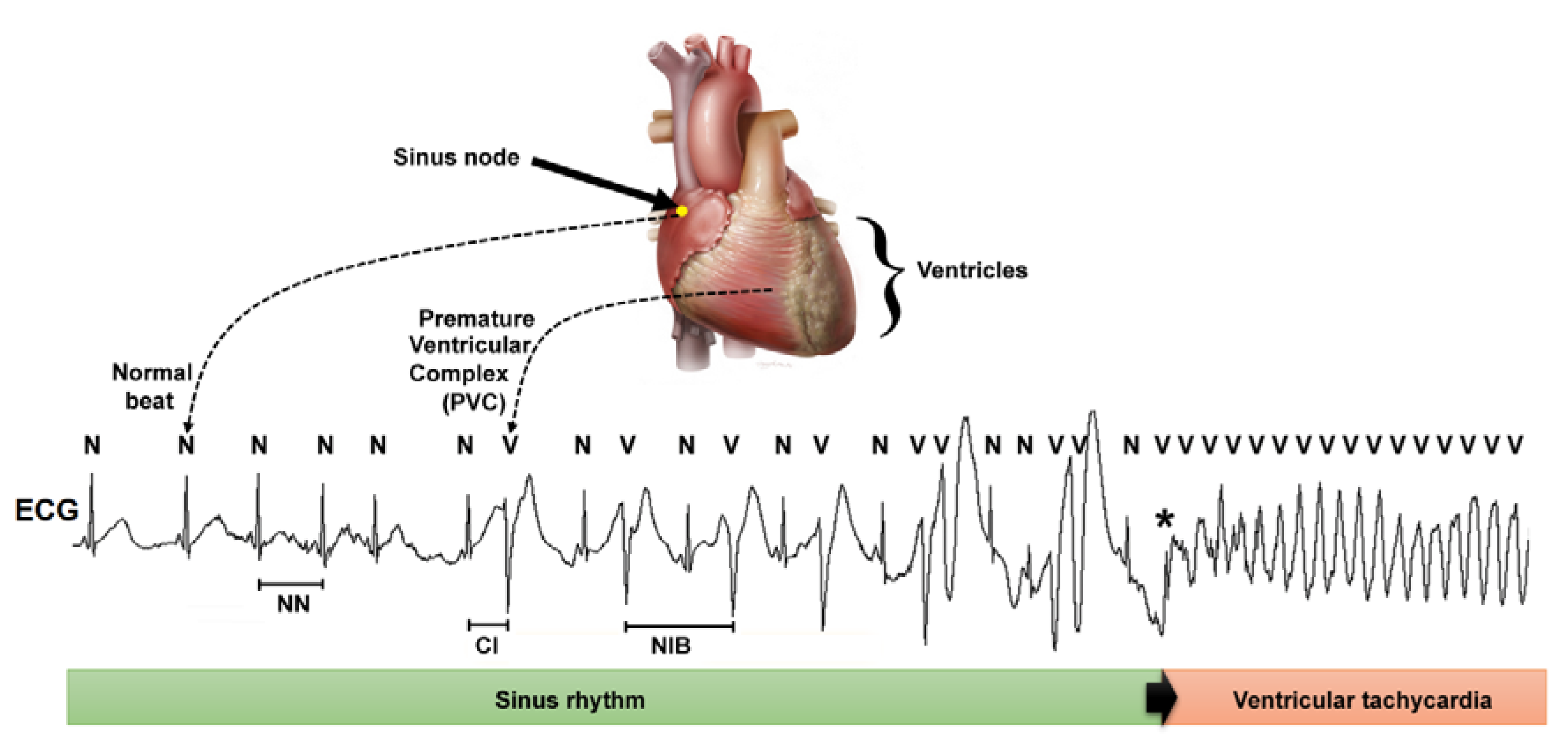
2.2. Time Series Processing
2.3. Feature Extraction of HRV and Heartprint Indices
2.4. Classification
2.5. Statistical Analysis
3. Results
3.1. Conventional Statistical Analysis of Heart Rate Variability and Heartprint Indices
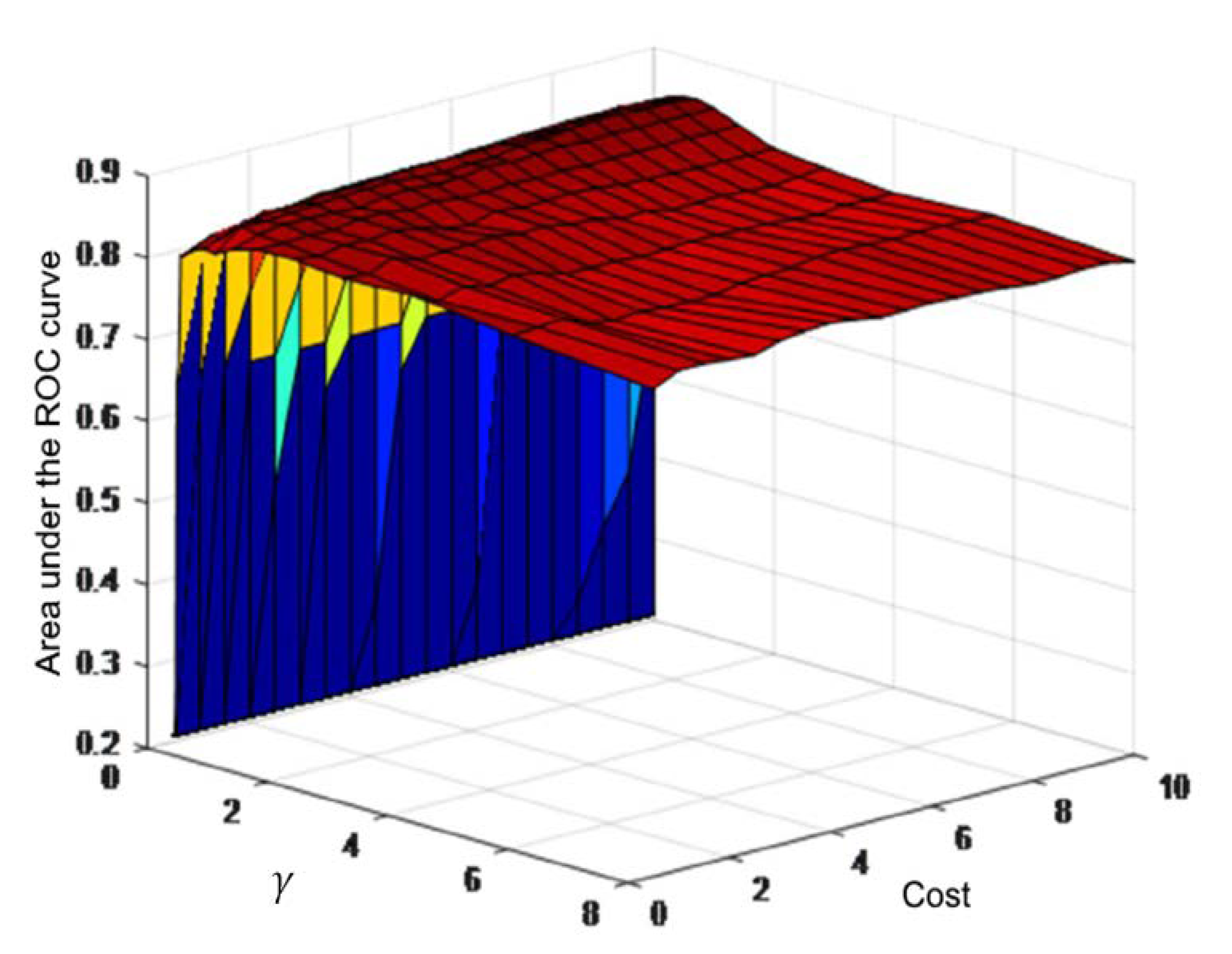
3.2. Definition and Validation of the Support Vector Machine
3.3. Support Vector Machine Training and Performance Tests
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Deyell, M.W.; Krahn, A.D.; Goldberger, J.J. Sudden cardiac death risk stratification. Circ. Res. 2015, 116, 1907–1918. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lerma, C.; Glass, L. Predicting the risk of sudden cardiac death. J. Physiol. 2016, 594, 2445–2458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mehra, R. Global public health problem of sudden cardiac death. J. Electrocardiol. 2007, 40, S118–S122. [Google Scholar] [CrossRef] [PubMed]
- Malik, M.; Bigger, J.T.; Camm, A.J.; Kleiger, R.E.; Malliani, A.; Moss, A.J.; Schwartz, P.J. Heart rate variability. Standards of measurement, physiological interpretation, and clinical use. Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Eur. Heart J. 1996, 17, 354–381. [Google Scholar] [CrossRef] [Green Version]
- Au-Yeung, W.-T.M.; Reinhall, P.G.; Poole, J.E.; Anderson, J.; Johnson, G.; Fletcher, R.D.; Moore, H.J.; Mark, D.B.; Lee, K.L.; Bardy, G.H. SCD-HeFT: Use of R-R interval statistics for long-term risk stratification for arrhythmic sudden cardiac death. Hear. Rhythm 2015, 12, 2058–2066. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huikuri, H.V.; Raatikainen, M.J.P.; Moerch-Joergensen, R.; Hartikainen, J.; Virtanen, V.; Boland, J.; Anttonen, O.; Hoest, N.; Boersma, L.V.A.; Platou, E.S.; et al. Prediction of fatal or near-fatal cardiac arrhythmia events in patients with depressed left ventricular function after an acute myocardial infarction. Eur. Heart J. 2009, 30, 689–698. [Google Scholar] [CrossRef] [PubMed]
- Skinner, J.E.; Meyer, M.; Dalsey, W.C.; Nester, B.A.; Ramalanjaona, G.; O’Neil, B.J.; Mangione, A.; Terregino, C.; Moreyra, A.; Weiss, D.N.; et al. Risk stratification for arrhythmic death in an emergency department cohort: A new method of nonlinear PD2i analysis of the ECG. Ther. Clin. Risk Manag. 2008, 4, 689–697. [Google Scholar] [CrossRef] [Green Version]
- Skinner, J.E.; Meyer, M.; Nester, B.A.; Geary, U.; Taggart, P.; Mangione, A.; Ramalanjaona, G.; Terregino, C.; Dalsey, W.C. Comparison of linear-stochastic and nonlinear-deterministic algorithms in the analysis of 15-minute clinical ECGs to predict risk of arrhythmic death. Ther. Clin. Risk Manag. 2009, 5, 671–682. [Google Scholar] [CrossRef] [Green Version]
- Ong, M.E.H.; Lee Ng, C.H.; Goh, K.; Liu, N.; Koh, Z.X.; Shahidah, N.; Zhang, T.T.; Fook-Chong, S.; Lin, Z. Prediction of cardiac arrest in critically ill patients presenting to the emergency department using a machine learning score incorporating heart rate variability compared with the modified early warning score. Crit. Care 2012, 16, R108. [Google Scholar] [CrossRef] [Green Version]
- Fujita, H.; Acharya, U.R.; Sudarshan, V.K.; Ghista, D.N.; Sree, S.V.; Eugene, L.W.J.; Koh, J.E.W. Sudden cardiac death (SCD) prediction based on nonlinear heart rate variability features and SCD index. Appl. Soft Comput. 2016, 43, 510–519. [Google Scholar] [CrossRef]
- Martínez-Alanis, M.; Ruiz-Velasco, S.; Lerma, C. Quantitative analysis of ventricular ectopic beats in short-term RR interval recordings to predict imminent ventricular tachyarrhythmia. Int. J. Cardiol. 2016, 225, 226–233. [Google Scholar] [CrossRef] [PubMed]
- Carrim, Z.I.; Khan, A.A. Mean frequency of premature ventricular complexes as predictor of malignant ventricular arrhythmias. Mt. Sinai J. Med. 2005, 72, 374–380. [Google Scholar]
- Schulte-Frohlinde, V.; Ashkenazy, Y.; Goldberger, A.L.; Ivanov, P.C.; Costa, M.; Morley-Davies, A.; Stanley, H.E.; Glass, L. Complex patterns of abnormal heartbeats. Phys. Rev. E. Stat. Nonlin. Soft Matter Phys. 2002, 66, 031901. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lerma, C.; Gorelick, A.; Ghanem, R.N.; Glass, L.; Huikuri, H.V. Patterns of ectopy leading to increased risk of fatal or near-fatal cardiac arrhythmia in patients with depressed left ventricular function after an acute myocardial infarction. Europace 2013, 15, 1304–1312. [Google Scholar] [CrossRef] [PubMed]
- Joo, S.; Choi, K.J.; Huh, S.J. Prediction of spontaneous ventricular tachyarrhythmia by an artificial neural network using parameters gleaned from short-term heart rate variability. Expert Syst. Appl. 2012, 39, 3862–3866. [Google Scholar] [CrossRef]
- Goldberger, A.L.; Amaral, L.A.N.; Glass, L.; Hausdorff, J.M.; Ivanov, P.C.; Mark, R.G.; Mietus, J.E.; Moody, G.B.; Peng, C.-K.; Stanley, H.E. PhysioBank, PhysioToolkit, and PhysioNet. Circulation 2000, 101, E215–E220. [Google Scholar] [CrossRef] [Green Version]
- Schirdewan, A.; Meyerfeldt, U.; Wessel, N.; Bondke, H.J.; Schreiber, P.; Sadowski, R.; Kamke, W.; Wiedemann, M. 1091–211 Heart rate dynamics before the onset of ventricular tachyarrhythmias: Results of the cardioverter defibrillator registry MARITA. J. Am. Coll. Cardiol. 2004, 43, A125–A126. [Google Scholar] [CrossRef] [Green Version]
- Wessel, N.; Voss, A.; Malberg, H.; Ziehmann, C.; Voss, H.U.; Schirdewan, A.; Meyerfeldt, U.; Kurths, J. Nonlinear analysis of complex phenomena in cardiological data. Herzschrittmachertherapie Elektrophysiologie 2000, 11, 159–173. [Google Scholar] [CrossRef]
- Lerma, C.; Wessel, N.; Schirdewan, A.; Kurths, J.; Glass, L. Ventricular arrhythmias and changes in heart rate preceding ventricular tachycardia in patients with an implantable cardioverter defibrillator. Med. Biol. Eng. Comput. 2008, 46, 715–727. [Google Scholar] [CrossRef]
- Lerma, C.; Lee, C.F.; Glass, L.; Goldberger, A.L. The rule of bigeminy revisited: Analysis in sudden cardiac death syndrome. J. Electrocardiol. 2007, 40, 78–88. [Google Scholar] [CrossRef]
- Hastie, T.; Tibshirani, R.; Friedman, J. The Elements of Statistical Learning; Springer Series in Statistics; Springer: New York, NY, USA, 2009; ISBN 978-0-387-84857-0. [Google Scholar]
- Rubio, J.D.J. SOFMLS: Online self-organizing fuzzy modified least-squares network. IEEE Trans. Fuzzy Syst. 2009, 17, 1296–1309. [Google Scholar] [CrossRef]
- Chiang, H.-S.; Chen, M.-Y.; Huang, Y.-J. Wavelet-Based EEG Processing for Epilepsy Detection Using Fuzzy Entropy and Associative Petri Net. IEEE Access 2019, 7, 103255–103262. [Google Scholar] [CrossRef]
- Elias, I.; de Jesús Rubio, J.; Martinez, D.I.; Vargas, T.M.; Garcia, V.; Mujica-Vargas, D.; Meda-Campaña, J.A.; Pacheco, J.; Gutierrez, G.J.; Zacarias, A. Genetic algorithm with radial basis mapping network for the electricity consumption modeling. Appl. Sci. 2020, 10, 4239. [Google Scholar] [CrossRef]
- Chang, C.-C.; Lin, C.-J. LIBSVM. ACM Trans. Intell. Syst. Technol. 2011, 2, 1–27. [Google Scholar] [CrossRef]
- Huikuri, H.V.; Exner, D.V.; Kavanagh, K.M.; Aggarwal, S.G.; Mitchell, L.B.; Messier, M.D.; Becker, D.; Sheldon, R.S.; Bloch Thomsen, P.-E.; CARISMA and REFINE Investigators. Attenuated recovery of heart rate turbulence early after myocardial infarction identifies patients at high risk for fatal or near-fatal arrhythmic events. Hear. Rhythm 2010, 7, 229–235. [Google Scholar] [CrossRef] [PubMed]
- Meyerfeldt, U.; Wessel, N.; Schütt, H.; Selbig, D.; Schumann, A.; Voss, A.; Kurths, J.; Ziehmann, C.; Dietz, R.; Schirdewan, A. Heart rate variability before the onset of ventricular tachycardia: Differences between slow and fast arrhythmias. Int. J. Cardiol. 2002, 84, 141–151. [Google Scholar] [CrossRef]
- Sosnowski, M.; Skrzypek-Wańha, J.; Korzeniowska, B.; Tendera, M. Increased variability of the coupling interval of premature ventricular beats may help to identify high-risk patients with coronary artery disease. Int. J. Cardiol. 2004, 94, 53–59. [Google Scholar] [CrossRef]
- Leclercq, J.F.; Maisonblanche, P.; Cauchemez, B.; Coumel, P. Respective role of sympathetic tone and of cardiac pauses in the genesis of 62 cases of ventricular fibrillation recorded during Holter monitoring. Eur. Heart J. 1988, 9, 1276–1283. [Google Scholar] [CrossRef]
- Zimmermann, M. Sympathovagal balance prior to onset of repetitive monomorphic idiopathic ventricular tachycardia. Pacing Clin. Electrophysiol. 2005, 28, S163–S167. [Google Scholar] [CrossRef]
- Billman, G.E. The LF/HF ratio does not accurately measure cardiac sympatho-vagal balance. Front. Physiol. 2013, 4, 26. [Google Scholar] [CrossRef] [Green Version]
- Li, Q.; Rajagopalan, C.; Clifford, G.D. Ventricular fibrillation and tachycardia classification using a machine learning approach. IEEE Trans. Biomed. Eng. 2014, 61, 1607–1613. [Google Scholar] [PubMed]
- Ganesh Kumar, R.; Kumaraswamy, Y.S. Investigation of Support Vector Machine To Assess Cardiac Arrhythmia. Int. Conf. Adv. Comput. Electr. Eng. 2012, 1, 98–102. [Google Scholar]
- Moridani, M.K.; Setarehdan, S.K.; Nasrabadi, A.M.; Hajinasrollah, E. New algorithm of mortality risk prediction for cardiovascular patients admitted in intensive care unit. Int. J. Clin. Exp. Med. 2015, 8, 8916–8926. [Google Scholar]
- Yaghouby, F.; Ayatollahi, A. An arrhythmia classification method based on selected features of heart rate variability signal and support vector machine-based classifier. IFMBE Proc. 2009, 25, 1928–1931. [Google Scholar]
- Bloch Thomsen, P.E.; Jons, C.; Raatikainen, M.J.P.; Moerch Joergensen, R.; Hartikainen, J.; Virtanen, V.; Boland, J.; Anttonen, O.; Gang, U.J.; Hoest, N.; et al. Long-term recording of cardiac arrhythmias with an implantable cardiac monitor in patients with reduced ejection fraction after acute myocardial infarction: The Cardiac Arrhythmias and Risk Stratification After Acute Myocardial Infarction (CARISMA) study. Circulation 2010, 122, 1258–1264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bishop, C.M. Pattern Recognition and Machine Learning, 1st ed.; Springer: New York, NY, USA, 2006; ISBN 9780387310732. [Google Scholar]
- Kheder, G.; Kachouri, A.; Samet, M. HRV analysis using wavelet package transform and least square support vector machine. Int. J. Circuits, Syst. Signal Process. 2008, 2, 18. [Google Scholar]
- Acharya, U.R.; Fujita, H.; Sudarshan, V.K.; Sree, V.S.; Eugene, L.W.J.; Ghista, D.N.; Tan, R.S. An integrated index for detection of Sudden Cardiac Death using Discrete Wavelet Transform and nonlinear features. Knowl. Based Syst. 2015, 83, 149–158. [Google Scholar] [CrossRef]
- Aquino, G.; Zacarias, A.; Rubio, J.D.J.; Pacheco, J.; Gutierrez, G.J.; Ochoa, G.; Balcazar, R.; Cruz, D.R.; Garcia, E.; Novoa, J.F. Novel Nonlinear Hypothesis for the Delta Parallel Robot Modeling. IEEE Access 2020, 8, 46324–46334. [Google Scholar] [CrossRef]
- Meda-Campaña, J.A. On the estimation and control of nonlinear systems with parametric uncertainties and noisy outputs. IEEE Access 2018, 6, 31968–31973. [Google Scholar] [CrossRef]
- Hernández, G.; Zamora, E.; Sossa, H.; Téllez, G.; Furlán, F. Hybrid neural networks for big data classification. Neurocomputing 2020, 390, 327–340. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| MVTDB (N = 78) | MARITA (N = 13) | p-Value | |
|---|---|---|---|
| Age (years) | 62 (53–69) | 62 (57–69) | 0.669 |
| Sex | 0.312 | ||
| Male | 63 | 12 | |
| Female | 15 | 1 | |
| Diagnosed cardiac disease | |||
| Dilated cardiomyopathy | 26 (33%) | 1 (8%) | 0.061 |
| Ischemic cardiomyopathy | 49 (63%) | 11 (85%) | 0.125 |
| Left ventricular ejection fraction (%) | 25 (20–35) | 40 (33–45) | 0.006 |
| New York Heart Association class | 0.068 | ||
| I or II | 65 (83%) | 8 (62%) | |
| III or IV | 13 (17%) | 5 (38%) | |
| Medication | |||
| Beta-blocker | 27 (35%) | 12 (92%) | <0.001 |
| Digoxin | 23 (29%) | 5 (38%) | 0.516 |
| Antiarrhythmic drug | 26 (33%) | 4 (31%) | 0.856 |
| Others | 9 (12%) | 13 (100%) | <0.001 |
| None | 19 (24%) | 0 (0%) | 0.045 |
| Number of recordings per patient | |||
| Before tachyarrhythmia | 1 (1–2) | 3 (1–3) | 0.059 |
| Total before tachyarrhythmia | 135 | 33 | |
| Control | 1 (1–2) | 2 (1–3) | 0.221 |
| Total control | 135 | 35 |
| MARITA | MVTDB | |||
|---|---|---|---|---|
| Before VT/VF (N = 33) | Control (N = 35) | Before VT/VF (N = 135) | Control (N = 135) | |
| meanNN (ms) | 705 (610–784) | 759 (678–873) * | 676 (607–819) | 787 (707–898) * |
| SDNN (ms) | 46 (28–71) | 41 (30–78) | 49 (34–77) | 50 (27–78) |
| RMSSD (ms) | 15 (11–24) | 15 (12–20) | 18 (13–31) | 20 (13–35) |
| pNN50 (%) | 2.00 (0.50–6.71) | 1.00 (0.40–3.50) | 0.49 (12.38–2.09) | 2.75 (0.49–2.75) |
| LFnu | 49.4 (42.2–63.2) | 56.5 (52.7–67.5) & | 45.2 (33.5–56.2) | 50.1 (39.3–60.6) * |
| HFnu | 25.7 (20.3–32.5) | 16.9 (12.1–32.5) & | 31.3 (21.5–42.9) | 29.6 (20.0–38.7) |
| LF/HF | 1.6 (1.0–3.1) & | 2.7 (2.0–3.9) *,& | 1.2 (0.7–2.4) | 1.6 (0.9–2.3) * |
| meanNN l.m. (ms) | 625 (560–801) | 764 (676–823) *,& | 625 (532–734) | 803 (726–954) * |
| SDNN l.m. (ms) | 19 (13–35) & | 22 (15–31) | 65 (39–90) | 24 (13–38) * |
| PVCs/hour ¶ | 154 (63–500) | 79 (11–181) * | 159 (42–433) | 71 (11–351) * |
| meanCI (ms) ¶ | 485 (444–522) | 493 (446–553) & | 520 (446–592) | 575 (509–636) * |
| SDCI (ms) ¶ | 41 (32–71) | 59 (30–75) | 63 (46–78) | 57 (37–88) |
| sNIB ¶ | 14 (2–36) | 4 (1–9) | 9 (3–25) | 5 (1–22) |
| NIB mode ¶ | 2 (1–3) | 2 (1–8) | 1 (0–4) | 2 (0–7) |
| Combination | Indices |
|---|---|
| 2 indices | meanNN l.m., SDCI * |
| 3 indices | meanNN l.m., SDCI *, meanNN |
| 4 indices | meanNN l.m., SDCI *, meanNN, meanCI * |
| 5 indices | meanNN l.m., SDCI *, meanNN, meanCI *, LF/HF |
| 6 indices | meanNN l.m., SDCI *, meanNN, meanCI *, LF/HF, SDNN l.m. |
| 7 indices | meanNN l.m., SDCI *, meanNN, meanCI *, LF/HF, SDNN l.m., LFnu |
| 8 indices | meanNN l.m., SDCI *, meanNN, meanCI *, LF/HF, SDNN l.m., LFnu, NIBmax * |
| 9 indices | meanNN l.m., SDCI *, meanNN, meanCI *, LF/HF, SDNN l.m., LFnu, NIBmax *, RMSsd |
| 10 indices | meanNN l.m., SDCI *, meanNN, meanCI *, LF/HF, SDNN l.m., LFnu, NIBmax *, RMSsd, HFnu |
| 11 indices | meanNN l.m., SDCI *, meanNN, meanCI *, LF/HF, SDNN l.m., LFnu, NIBmax *, RMSsd, HFnu, sNIB * |
| 12 indices | meanNN l.m., SDCI *, meanNN, meanCI *, LF/HF, SDNN l.m., LFnu, NIBmax *, RMSsd, HFnu, sNIB *, SDNN |
| 13 indices | meanNN l.m., SDCI *, meanNN, meanCI *, LF/HF, SDNN l.m., LFnu, NIBmax *, RMSsd, HFnu, sNIB *, SDNN, PVCs/hour |
| 14 indices | meanNN l.m., SDCI *, meanNN, meanCI *, LF/HF, SDNN l.m., LFnu, NIBmax *, RMSsd, HFnu, sNIB *, SDNN, PVCs/hour, pNN50 |
| Combination | AUC | Accuracy | C Value | r Value |
|---|---|---|---|---|
| 2 indices | 0.8339 ± 0.0655 | 82.14 ± 8.18 | 7.5 | 0.1250 |
| 3 indices | 0.8433 ± 0.0827 | 84.55 ± 7.25 | 9.0 | 1.0000 |
| 4 indices | 0.8557 ± 0.0799 | 85.80 ± 6.71 & | 5.0 | 8.0000 |
| 5 indices | 0.8578 ± 0.0768 * | 84.64 ± 6.61 | 8.5 | 0.7071 |
| 6 indices | 0.8403 ± 0.0716 | 85.27 ± 5.06 | 8.5 | 0.7071 |
| 7 indices | 0.8397 ± 0.0811 | 84.02 ± 5.13 | 2.0 | 0.7071 |
| 8 indices | 0.8534 ± 0.0700 | 83.75 ± 9.09 | 8.0 | 0.1250 |
| 9 indices | 0.8379 ± 0.0671 | 81.34 ± 5.65 | 8.0 | 0.7071 |
| 10 indices | 0.8421 ± 0.0708 | 82.77 ± 5.91 | 1.5 | 1.0000 |
| 11 indices | 0.8378 ± 0.1001 | 84.20 ± 8.91 | 6.0 | 0.1768 |
| 12 indices | 0.8271 ± 0.0841 | 81.25 ± 6.13 | 8.0 | 0.2500 |
| 13 indices | 0.7972 ± 0.0705 | 79.55 ± 6.24 | 10.0 | 0.1250 |
| 14 indices | 0.8022 ± 0.1060 | 80.27 ± 10.25 | 2.0 | 0.7071 |
| Training | Testing | |||
|---|---|---|---|---|
| Combination | AUC | Accuracy | AUC | Accuracy |
| 4 indices | 0.892 (0.852–0.931) | 82.593 | 0.678 (0.550–0.806) | 67.647 |
| 5 indices | 0.858 (0.812–0.903) | 77.407 | 0.646 (0.515–0.777) | 63.235 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martinez-Alanis, M.; Bojorges-Valdez, E.; Wessel, N.; Lerma, C. Prediction of Sudden Cardiac Death Risk with a Support Vector Machine Based on Heart Rate Variability and Heartprint Indices. Sensors 2020, 20, 5483. https://doi.org/10.3390/s20195483
Martinez-Alanis M, Bojorges-Valdez E, Wessel N, Lerma C. Prediction of Sudden Cardiac Death Risk with a Support Vector Machine Based on Heart Rate Variability and Heartprint Indices. Sensors. 2020; 20(19):5483. https://doi.org/10.3390/s20195483
Chicago/Turabian StyleMartinez-Alanis, Marisol, Erik Bojorges-Valdez, Niels Wessel, and Claudia Lerma. 2020. "Prediction of Sudden Cardiac Death Risk with a Support Vector Machine Based on Heart Rate Variability and Heartprint Indices" Sensors 20, no. 19: 5483. https://doi.org/10.3390/s20195483