The Impact of the COVID-19 Confinement on the Habits of PA Practice According to Gender (Male/Female): Spanish Case

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Instrument
2.3. Procedure
2.4. Data Analysis
3. Results
4. Discussion
Limitations and Future Research Lines
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
- Gender: Man/Woman
- Age (years)
- Province (selection of the corresponding Spanish province)
- Education level (no education/Primary Ed./Secondary Ed./Higher Ed.)
- 5.
- Physical activity intensity (1. None/2. Smooth/3. Moderate/4. Intense)
- 6.
- Weekly hours of physical activity (1. None (cero)/2. Few (<3 h)/3. Some (between 3h and 5h59′)/4. Enough (between 6h and 8h59′)/5. A lot (over 9h))
- 7.
- To what extent (1. None/2. Few/3. Some/4. Enough/5. A lot) did you practice the following activities? (cycling, swimming, outdoor sports, racket sports, gym sports, smooth gymnastics, e-sports)
References
- WHO. Cronología de la Respuesta de la OMS a la COVID-19. Centro de prensa. Available online: https://www.who.int/es/news-room/detail/29-06-2020-covidtimeline (accessed on 4 August 2020).
- Boletín Oficial del Estado. Real Decreto 463/2020, de 14 de Marzo, por el que se declara el Estado de Alarma para la gestión de la situación de crisis sanitaria ocasionada por el COVID-19. Available online: https://www.boe.es/eli/es/rd/2020/03/14/463 (accessed on 30 June 2020).
- Boletín Oficial del Estado. Real Decreto 555/2020, de 5 de Junio, por el que se prorroga el Estado de Alarma declarado por el Real Decreto 463/2020, de 14 de Marzo, por el que se declara el Estado de Alarma para la gestión de la situación de crisis sanitaria ocasionada por el COVID-19. Available online: https://www.boe.es/eli/es/rd/2020/06/05/555 (accessed on 4 August 2020).
- Boletín Oficial del Estado. Orden SND/380/2020, de 30 de Abril, sobre las Condiciones en las que se puede realizar actividad física no Profesional al aire libre durante la situación de crisis sanitaria ocasionada por el COVID-19. Available online: https://www.boe.es/eli/es/o/2020/04/30/snd380 (accessed on 30 June 2020).
- Martín, L. España Roza Los 4 Millones de Afectados Por ERTEs. Eonomía Digital. Available online: https://www.economiadigital.es/directivos-y-empresas/espana-roza-los-4-millones-de-afectados-por-ertes-por-coronavirus_20053920_102.html (accessed on 4 August 2020).
- INE. INEbase/Economía/Cuentas Económicas/Contabilidad Nacional Trimestral de España: Principales Agregados (CNTR)/Últimos datos. Available online: https://www.ine.es/dyngs/INEbase/es/operacion.htm?c=Estadistica_C&cid=1254736164439&menu=ultiDatos&idp=1254735576581 (accessed on 4 August 2020).
- Frontiers. Coronavirus Disease (COVID-19): Psychoeducational Variables Involved in the Health Emergency|Frontiers Research Topic. Available online: https://www.frontiersin.org/research-topics/13709/coronavirus-disease-covid-19-psychoeducational-variables-involved-in-the-health-emergency?utm_campaign=sub-cov-rt-fpsyg-psychoeducational-variables&utm_medium=cvlp&utm_source=fweb (accessed on 4 August 2020).
- Borja, M. Siete de Cada Diez Mujeres se Sienten Mucho Más Cansadas y Estresadas Que Antes de la Pandemia de Coronavirus. 20minutos. Salud. Available online: https://www.20minutos.es/noticia/4339673/0/7-de-cada-10-mujeres-se-sienten-mucho-mas-cansadas-y-estresadas-que-antes-del-coronavirus/?autoref=true (accessed on 31 July 2020).
- Bosch, J.; García, J.; Murillo, C. El sector del Deporte: Un Paciente Económico del Coronavirus Con un Diagnóstico Muy Incierto a Fecha de Hoy. 2020. Available online: https://seed-deporte.es/el-sector-del-deporte-un-paciente-economico-del-coronavirus-con-un-diagnostico-muy-incierto-a-fecha-de-hoy/ (accessed on 30 June 2020).
- De Guerreiro, R.C.; Silva, A.; de Andrade, H.A.; Biasibetti, I.G.; Vital, R.; da Silva, H.G.V.; da Silva, F.R.; de Mello, M.T. Was postponing the Tokyo 2020 Olympic and Paralympic Games a correct decision? Rev. Bras. Med. Esporte 2020, 26, 191–195. [Google Scholar] [CrossRef]
- TOKYO2020. Olympic Games Postponed to 2021. TOKYO2020. News. General. Available online: https://tokyo2020.org/en/news/joint-statement-from-international-olympic-committee-and-tokyo2020 (accessed on 31 July 2020).
- Mena, F. Mapa Coronavirus Deporte: Más de 250 Competiciones Afectadas. RTVE. Coronavirus en el deporte. 2020. Available online: https://www.rtve.es/noticias/20200724/mapa-coronavirus-deporte/2010083.shtml (accessed on 31 July 2020).
- García-Tascón, M. COVID-19 y el Otro Gran Invisible del Deporte: El Equipamiento Deportivo. FAGDE, Deporte y Covid-19. 2020. Available online: https://www.fagde.org/es/post/878/covid-19-y-el-otro-gran-invisible-del-deporte-el-equipamiento-deportivo/ (accessed on 30 June 2020).
- Maugeri, G.; Castrogiovanni, P.; Battaglia, G.; Pippi, R.; D’Agata, V.; Palma, A.; di Rosa, M.; Musumeci, G. The impact of physical activity on psychological health during Covid-19 pandemic in Italy. Heliyon 2020, 6, e04315. [Google Scholar] [CrossRef]
- Lesser, I.A.; Nienhuis, C.P. The Impact of COVID-19 on Physical Activity Behavior and Well-Being of Canadians. Int. J. Environ. Res. Public Health 2020, 17, 3899. [Google Scholar] [CrossRef] [PubMed]
- Palco23. Administración y Gimnasios Buscan Fórmulas para Compensar el Cierre de Centros Deportivos|Palco23. Palco23. Available online: https://www.palco23.com/fitness/administracion-y-gimnasios-buscan-formulas-para-compensar-el-cierre-de-centros-deportivos.html (accessed on 30 June 2020).
- Palco23. Los Gimnasios Españoles Asumen Que el Cierre Durará Como Mínimo dos meses|Palco23. PALCO23. Available online: https://www.palco23.com/fitness/los-gimnasios-espanoles-asumen-que-el-cierre-durara-como-minimo-dos-meses.html (accessed on 30 June 2020).
- IOC. What goes into postponing the Olympic Games? Olympic News. IOC NEWS. Available online: https://www.olympic.org/news/what-goes-into-postponing-the-olympic-games (accessed on 31 July 2020).
- Jiménez Gutiérrez, A.; Mayo Mauriz, X.; López Valenciano, A.; Ardanuy Pizarro, M. Estudio de Evaluaciόn del Impacto de la Pandemia del COVID-19 Sobre el Ecosistema del Deporte en ESPAŇA. 2020. Available online: https://deporteespana.es/es/noticia/4985/-estudio-del-impacto-del-covid-19-sobre-el-ecosistema-del-deporte-espanol-documento-completo/ (accessed on 30 June 2020).
- Taku, K.; Arai, H. Impact of COVID-19 on Athletes and Coaches, and Their Values in Japan: Repercussions of Postponing the Tokyo 2020 Olympic and Paralympic Games. J. Loss Trauma 2020, 25, 623–630. [Google Scholar] [CrossRef]
- Muñiz, J. El sector del Fitness Prevé Pérdidas Superiores a los 1.100 Millones Por el Coronavirus|Deporte y Negocio. Expansión, Deporte y Negocio, Marketing Deportivo. 2020. Available online: https://www.expansion.com/directivos/deporte-negocio/2020/06/17/5eea0c57468aeb722f8b4612.html (accessed on 10 July 2020).
- Barnes, S.J. Information management research and practice in the post-COVID-19 world. Int. J. Inf. Manag. 2020, in press. [Google Scholar] [CrossRef]
- Moreno, M.A. Una “Reconversión digital” Para Los Gimnasios Ante el Coronavirus. La Vanguardia. Deportes. Available online: https://www.lavanguardia.com/deportes/20200417/48569692286/una-reconversion-digital-para-los-gimnasios-ante-el-coronavirus.html (accessed on 4 August 2020).
- Piedra, J. Redes sociales en tiempos del COVID-19. Sociol. Deport. 2020, 1, 41–43. [Google Scholar] [CrossRef]
- CSD, Consejo COLEF. YoMeMuevoEnCasa. Ùltimas noticias. Available online: https://www.csd.gob.es/es/la-campana-yomemuevoencasa-del-csd-y-el-consejo-colef-recuerda-la-importancia-de-mantener-un-estilo-de-vida-activo-durante (accessed on 1 July 2020).
- Varea, V.; González-Calvo, G. Touchless classes and absent bodies: Teaching physical education in times of Covid-19. Sport. Educ. Soc. 2020, AHEAD-OF-PRINT. 1–15. [Google Scholar] [CrossRef]
- Irazusta Astiazarán, J.; Ara Roy, I. Actividad Física en la Población Universitaria Durante el Confinamiento Por Covid-19: Determinantes y Consecuencias Sobre el Estado de Salud y la Calidad de Vida. 2020. Available online: https://www.csd.gob.es/sites/default/files/media/files/2020-06/Resumen%20Ejecutivo%20Proyecto%20AF%20confinamiento%20universitarios%20200605_FINAL%20....pdf (accessed on 29 June 2020).
- Hammami, A.; Harrabi, B.; Mohr, M.; Krustrup, P. Physical activity and coronavirus disease 2019 (COVID-19): Specific recommendations for home-based physical training. Manag. Sport Leis. 2020, 1–6. [Google Scholar] [CrossRef]
- Magaz-González, A.M.; García-Tascón, M. Resultados Preliminares del “Estudio Sobre el Confinamiento en Relación con la Actividad Física y el Uso de Las TIC”–SEED. 2020. Available online: https://seed-deporte.es/resultados-preliminares-del-estudio-sobre-el-confinamiento-en-relacion-con-la-actividad-fisica-y-el-uso-de-las-tic/ (accessed on 30 June 2020).
- Puyana, M.G.; Jesús, S.O.A.; Jerónimo, G.F. Organizaciones de Gestión de los Gimnasios Españoles [Management Organizations of Spanish Gyms]. Apunt. Educ. Física Deport. 2018, 3, 7–19. Available online: https://www.raco.cat/index.php/ApuntsEFD/article/view/340449 (accessed on 16 September 2020). [CrossRef]
- Fitbit Staff. The Impact of Coronavirus on Global Activity. Fitbit News 2020. Available online: https://blog.fitbit.com/covid-19-global-activity (accessed on 20 June 2020).
- IBV. Actividad Física en Tiempos COVID-19. Informe de Resultados. 2020. Available online: http://munideporte.com/imagenes/documentacion/ficheros/03E3FDFD.pdf (accessed on 1 July 2020).
- ACSM. ACSMs Guidelines for Exercise Testing and Prescription, 10th ed.; Riebe, D., Ed.; Wolters Kluwer Health: Philadelphia, PA, USA, 2018; Available online: https://www.acsm.org/read-research/books/acsms-guidelines-for-exercise-testing-and-prescription (accessed on 4 August 2020).
- Brown, W.J.; Bauman, A.; Bull, F.C.; Burton, N.W. Development of Evidence-Based Physical Activity Recommendations for Adults (18–64 Years). 2013. Available online: https://www1.health.gov.au/internet/main/publishing.nsf/Content/health-pubhlth-strateg-phys-act-guidelines/$File/DEB-PAR-Adults-18-64years.pdf (accessed on 23 June 2020).
- Garber, C.E.; Blissmer, B.; Deschenes, M.R.; Franklin, B.A.; Lamonte, M.J.; Lee, I.-M.; Nieman, D.C.; Swain, D.P. Quantity and Quality of Exercise for Developing and Maintaining Cardiorespiratory, Musculoskeletal, and Neuromotor Fitness in Apparently Healthy Adults. Med. Sci. Sport Exerc. 2011, 43, 1334–1359. [Google Scholar] [CrossRef]
- WHO. Recomendaciones Mundiales Sobre Actividad Física para la Salud. 2010. Available online: https://apps.who.int/iris/bitstream/handle/10665/44441/9789243599977_spa.pdf?ua=1 (accessed on 4 August 2020).
- Bravo-Cucci, S.; Kosakowski, H.; Núñez-Cortés, R.; Sánchez-Huamash, C.; Ascarruz-Asencios, J. La Actividad Física en el Contexto de Aislamiento social Por COVID-19. GICOS 2020, 5, 6–22. Available online: http://erevistas.saber.ula.ve/index.php/gicos/article/view/16117 (accessed on 31 July 2020).
- Biswas, A.; Oh, P.I.; Faulkner, G.E.; Bajaj, R.R.; Silver, M.A.; Mitchell, M.S.; Alter, D.A. Sedentary Time and Its Association With Risk for Disease Incidence, Mortality, and Hospitalization in Adults. Ann. Intern. Med. 2015, 162, 123. [Google Scholar] [CrossRef] [PubMed]
- Jakicic, J.M.; Clark, K.; Coleman, E.; Donnelly, J.E.; Foreyt, J.; Melanson, E.; Volek, J.; Volpe, S.L. Appropriate Intervention Strategies for Weight Loss and Prevention of Weight Regain for Adults. Med. Sci. Sport. Exerc. 2001, 33, 2145–2156. Available online: https://journals.lww.com/acsm-msse/Fulltext/2001/12000/Appropriate_Intervention_Strategies_for_Weight.26.aspx (accessed on 1 July 2020). [CrossRef]
- WHO. OMS|10 datos sobre la actividad física. WHO. 2017. Available online: http://www.who.int/features/factfiles/physical_activity/es/ (accessed on 20 July 2020).
- García-González, D.; Pérez-Bilbao, T.; de la Torre-Luque, A.; López Ramírez, E.; García-Foncillas López, J.F.; San Juan, A. Ejercicio individualizado como herramienta protectora en la rehabilitación cardio-oncológica: Revisión narrativa. Arch. Med. Deport. 2020, 37, 125–135. Available online: http://archivosdemedicinadeldeporte.com/summary.php?articulo=1761 (accessed on 4 August 2020).
- Da Silveira, M.P.; da Silva Fagundes, K.K.; Bizuti, M.R.; Starck, É.; Rossi, R.C.; de Resende e Silva, D.T. Physical exercise as a tool to help the immune system against COVID-19: An integrative review of the current literature. Clin. Exp. Med. 2020, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Ávila, M.P.W.; Corrêa, J.C.; Lucchetti, G.; Lucchetti, G. The Role of Physical Activity in the Association between Resilience and Mental Health in Older Adults. J. Aging Phys. Act. 2018, 26, 248–253. [Google Scholar] [CrossRef]
- Barbosa-Granados, H.; Urrea Cuéllar, M.Á. Influencia del deporte y la actividad física en el estado de salud físico y mental: Una revisión bibliográfica. Katharsis 2018, 25, 155–173. [Google Scholar] [CrossRef]
- Dunstan, D.W.; Howard, B.; Healy, G.N.; Owen, N. Too much sitting—A health hazard. Diabetes Res. Clin. Pract. 2012, 97, 368–376. [Google Scholar] [CrossRef]
- Owen, N.; Healy, G.N.; Matthews, C.E.; Dunstan, D.W. Too Much Sitting: The Population Health Science of Sedentary Behavior. Exerc. Sport Sci. Rev. 2010, 38. Available online: https://journals.lww.com/acsm-essr/Fulltext/2010/07000/Too_Much_Sitting__The_Population_Health_Science_of.3.aspx (accessed on 5 August 2020). [CrossRef]
- ACSM. Progression Models in Resistance Training for Healthy Adults. Med. Sci. Sports Exerc. 2009, 41, 687–708. [Google Scholar] [CrossRef]
- Nelson, M.E.; Rejeski, W.J.; Blair, S.N.; Duncan, P.W.; Judge, J.O.; King, A.C.; Macera, C.A.; Castaneda-Sceppa, C. Physical activity and public health in older adults: Recommendation from the American College of Sports Medicine and the American Heart Association. Med. Sci. Sports Exerc. 2007, 39, 1435–1445. [Google Scholar] [CrossRef] [Green Version]
- Manson, J.E.; Greenland, P.; Lacroix, A.Z.; Stefanick, M.L.; Mouton, C.P.; Oberman, A.; Perri, M.G.; Sheps, D.S.; Pettinger, M.B.; Siscovick, D.S. Walking Compared with Vigorous Exercise for the Prevention of Cardiovascular Events in Women. N. Engl. J. Med. 2002, 347, 716–725. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Instituto Nacional de Estadística (INE). Mujeres y Hombres en España. Salud. Esperanza de Vida. 2020. Available online: https://www.ine.es/ss/Satellite?L=es_ES&c=INESeccion_C&cid=1259926378861&p=1254735110672&pagename=ProductosYServicios%2FPYSLayout¶m1=PYSDetalle¶m3=1259926137287 (accessed on 4 September 2020).
- Ministerio de Sanidad C y BS. ENSE. Encuesta Nacional de Salud España 2017. 2018. Available online: https://www.mscbs.gob.es/estadEstudios/estadisticas/encuestaNacional/encuestaNac2017/ENSE17_pres_web.pdf (accessed on 4 September 2020).
- Nuzzo, J.L. Men’s health in the United States: A national health paradox. Aging Male 2019, 23, 42–52. [Google Scholar] [CrossRef]
- WHO. Uneven Access to Health Services Drives Life Expectancy Gaps: WHO. 2019. Available online: https://www.who.int/news-room/detail/04-04-2019-uneven-access-to-health-services-drives-life-expectancy-gaps-who (accessed on 8 September 2020).
- WHO. Stay Physically Active during Self-Quarantine. 2020. Available online: https://www.euro.who.int/en/health-topics/health-emergencies/coronavirus-covid-19/technical-guidance/stay-physically-active-during-self-quarantine (accessed on 4 August 2020).
- ACSM. Staying Active during the Coronavirus Pandemic. Exercise is Medicine; 2020. Available online: https://www.cdc.gov/ (accessed on 3 August 2020).
- Rosales, C.K.; Erazo, P.V.; Valderrama, J.F.; Gonzalez, J.B.; Terneus, D.H.; Stagno, R.U.; Sarquis, F.J.; Reyes, A.S.; Miranda, F.V.; Plaza, R.S.; et al. Orientaciones Deporte y COVID-19: Recomendaciones sobre el retorno a la actividad física y deportes de niños niñas y adolescentes. Rev. Chil. Pediatría 2020, 91, 1–16. [Google Scholar] [CrossRef]
- Wenham, C.; Smith, J.; Morgan, R. COVID-19: The gendered impacts of the outbreak. Lancet 2020, 395, 846–848. [Google Scholar] [CrossRef] [Green Version]
- Smith, J. Overcoming the ‘tyranny of the urgent’: Integrating gender into disease outbreak preparedness and response. Gend. Dev. 2019, 27, 355–369. [Google Scholar] [CrossRef]
- Azevedo, M.R.; Araújo, C.L.P.; Reichert, F.F.; Siqueira, F.V.; Da Silva, M.C.; Hallal, P.C. Gender differences in leisure-time physical activity. Int. J. Public Health 2007, 52, 8–15. [Google Scholar] [CrossRef] [Green Version]
- Hands, B.; Parker, H.; Larkin, D.; Cantell, M.; Rose, E. Male and Female Differences in Health Benefits Derived from Physical Activity: Implications for Exercise Prescription. J. Womens Health Issues Care 2016, 5. [Google Scholar] [CrossRef] [Green Version]
- Arriscado, D.; Knox, E.C.L.; Zabala, M.; Zurita-Ortega, F.; Dalmau, J.M.; Muros, J.J. Different healthy habits between northern and southern Spanish school children. J. Public Health (Bangkok) 2017, 25, 653–660. [Google Scholar] [CrossRef] [Green Version]
- Van Hecke, L.; Loyen, A.; Verloigne, M.; Van Der Ploeg, H.P.; Lakerveld, J.; Brug, J.; De Bourdeaudhuij, I.; Ekelund, U.; Donnelly, A.E.; Hendriksen, I.; et al. Variation in population levels of physical activity in European children and adolescents according to cross-European studies: A systematic literature review within DEDIPAC. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 70. [Google Scholar] [CrossRef] [Green Version]
- Van Uffelen, J.G.; Khan, A.; Burton, N.W. Gender differences in physical activity motivators and context preferences: A population-based study in people in their sixties. BMC Public Health 2017, 17, 624. [Google Scholar] [CrossRef] [PubMed]
- European Commission. Special Eurobarometer 472, Sport and Physical Activity; Directorate-General for Communication: Brussels, Belgium, 2018. [Google Scholar]
- Eurostat. Health-enhancing Physical Activity Statistics. Eurostat. Statistics Explained. 2018. Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Health-enhancing_physical_activity_statistics (accessed on 1 July 2020).
- Subdirección General de Estadística y Estudios. Encuesta de Hábitos Deportivos en España, 2015. 2015. Available online: http://www.culturaydeporte.gob.es/dam/jcr:398d6e55-7bc5-4b8e-b0f3-95dd49c4997f/Encuesta_de_Habitos_Deportivos_2015.pdf (accessed on 22 May 2020).
- Ministerio de Sanidad y Consumo. Encuesta Nacional de Salud ENSE, España 2017 Serie Informes Monográficos 2-Actividad Física, Descanso y Ocio. 2017. Available online: https://www.mscbs.gob.es/estadEstudios/estadisticas/encuestaNacional/encuesta2017.htm (accessed on 4 August 2020).
- Instituto Nacional de Estadística (INE). Avance de La Estadística Del Padrón Continuo a 1 de Enero de 2020-Datos Provisionales. 2020. Available online: https://www.ine.es/prensa/pad_2020_p.pdf (accessed on 8 September 2020).
- Pérez Santamaría, F.J.; Rodríguez Testal, J.F.; Romero de Loera, B.; Ruvalcaba Coyaso, F.J. Preferencias por formatos de respuesta en cuestionarios para encuestas. Metodol. Encuestas 2002, 4, 63–74. Available online: http://casus.usal.es/pkp/index.php/MdE/article/view/913 (accessed on 30 June 2020).
- Skjong, R.; Wentworth, B. Expert Judgement and risk perception. 2000. Available online: http://research.dnv.com/skj/Papers/SkjWen.pdf (accessed on 4 August 2020).
- Colás, M.P.; Buendía, L. Investigación Educativa, 3rd ed.; Alfar: Sevilla, Spain, 2012. [Google Scholar]
- World Medical Association (WMA). WMA Declaration of Helsinki–Ethical Principles for Medical Research Involving Human Subjects–WMA–The World Medical Association. 2013. Available online: https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/ (accessed on 4 August 2020).
- Jiménez-Pavón, D.; Carbonell-Baeza, A.; Lavie, C.J. Physical exercise as therapy to fight against the mental and physical consequences of COVID-19 quarantine: Special focus in older people. Prog. Cardiovasc. Dis. 2020, 63, 386–388. [Google Scholar] [CrossRef] [PubMed]
- López-Bueno, R.; Calatayud, J.; Casaña, J.; Casajús, J.A.; Smith, L.; Tully, M.A.; Andersen, L.L.; López-Sánchez, G.F. COVID-19 Confinement and Health Risk Behaviors in Spain. Front. Psychol. 2020, 11. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Rio, J.; Cecchini, J.A.; Mendez-Gimenez, A.; Carriedo, A. Weight changes during the COVID-19 home confinement. Effects on psychosocial variables. Obes. Res. Clin. Pract. 2020. [Google Scholar] [CrossRef] [PubMed]
- Balluerka Lasa, N.; Gómez Benito, J.; Hidalgo Montesinos, M.D.; Gorostiaga Manterola, A.; Espada Sánchez, J.P.; Padilla García, J.L.; Santed Germán, M.A. Las Consecuencias Psicológicas de La COVID-19 y El Confinamiento. Informe de Investigación. 2020. Available online: https://canal.ugr.es/wp-content/uploads/2020/05/Consecuencias-psicologicas-COVID-19.pdf (accessed on 29 June 2020).
- MAMifit. La Práctica de Ejercicio Físico Entre Mujeres Aumenta Durante el Confinamiento. Agencia EFE. 2020. Available online: https://www.efe.com/efe/espana/practicodeporte/la-practica-de-ejercicio-fisico-entre-mujeres-aumenta-durante-el-confinamiento/50000944-4227909 (accessed on 5 August 2020).
- Rodríguez García, G. Actitudes y hábitos conductuales hacia la práctica deportiva en el medio rural en function del género. J. Sport Health Res. 2016, 8, 103–114. [Google Scholar]
- Alonso Fernández, D.; Mujeres, Hombres y Práctica Físico-Deportiva: Aproximación al Sector de los Centros Deportivos y Gimnasios Mediante la Segmentación Por Sexos. EFDeportes. 2012. Available online: https://www.efdeportes.com/efd175/practica-deportiva-segmentacion-por-sexos.htm (accessed on 4 September 2020).
- Ministerio de Educación C. yD. (MECD). Anuario de Estadísticas Deportivas 2020. 2020. Available online: http://www.culturaydeporte.gob.es/dam/jcr:47414879-4f95-4cae-80c4-e289b3fbced9/anuario-de-estadisticas-deportivas-2020.pdf (accessed on 30 June 2020).
- Eurostat (European Commission). Quality of Life. Facts and Views; Statistical books; Publications Office of the European Union: Luxembourg, 2015. [Google Scholar] [CrossRef]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Worldwide trends in insufficient physical activity from 2001 to 2016: A pooled analysis of 358 population-based surveys with 1·9 million participants. Lancet Glob. Health 2018, 6, e1077–e1086. [Google Scholar] [CrossRef] [Green Version]
- Peake, J.M.; Neubauer, O.; Walsh, N.P.; Simpson, R.J. Recovery of the immune system after exercise. J. Appl. Physiol. 2017, 122, 1077–1087. [Google Scholar] [CrossRef]
- Reimers, C.D.; Knapp, G.; Reimers, A.K. Does Physical Activity Increase Life Expectancy? A Review of the Literature. J. Aging Res. 2012, 2012, 243958. [Google Scholar] [CrossRef] [Green Version]
- UN. COVID-19, Women, Girls and Sport: Build Back Better. 2020. Available online: https://www.unwomen.org/-/media/headquarters/attachments/sections/library/publications/2020/brief-covid-19-women-girls-and-sport-en.pdf?la=en&vs=2629 (accessed on 5 August 2020).



{kind=link}
{kind=link}
| Type | Intensity | Frequency | Duration | Quantity | Examples |
|---|---|---|---|---|---|
| Cardiorespiratory exercise | Moderate | ≥5 d·wk | ≥30 min·d Sessions of at least 10 min | ≥150 min·wk Additional health benefits are obtained with 300 min ∙ wk | Rhythm, aerobic exercises involving large muscle groups |
| Vigorous | ≥3 d·wk | ≥20 min·d | ≥75 min·wk To be more effective increase to 150 min· wk | ||
| Or a combination of moderate and vigorous exercise on ≥3–5 d·wk | |||||
| Muscular fitness (muscular strength, endurance and power) | Should be tailored to the individual’s experience | 2–3 d·wks with at least 48 h separating the exercise training sessions for the same muscle group | A reasonable rest interval | 2–4 sets 8–12 repetitions per set 8–10 exercises for session | Training involving each major muscle group. Multi-joint exercises (stair climbing, carrying bags of groceries). |
| Flexibility exercise | Stretch to the point of tightness or slight discomfort | ≥2–3 times·wk Most effective when performed daily | 30–60 s/ex Series 10–30 s Adjusting time/duration and repetitions according to individual needs | 2–4 series | Exercises targeting the major muscle tendon units should be performed (postural stability and flexibility exercises) |
| Neuromotor exercise | Not determined | ≥2–3 d·wk | ≥20–30 min· d | ≥60 min·wk | Involving balance, agility, coordination, gait |
| Recommendations of Physical Activity during Quarantine according to WHO and ACSM |
|---|
| 150–300 min per week of moderate-intensity aerobic physical activity and 2 sessions per week of muscle strength training |
| Walk briskly around the house. Dance. Jump rope. Walk up and down the stairs |
| 7-Minute Workout app |
| Yoga |
| Simple muscle strengthening exercises around your house: squats or sit-to-stands from a sturdy chair, push-ups against a wall, the kitchen counter or the floor, lunges or single leg step-ups on stairs |
| Do not sit all day |
| Relaxation techniques |
| M | SD | Wilcoxon W | Z | Sig. | ||
|---|---|---|---|---|---|---|
| Female (n = 538) | ||||||
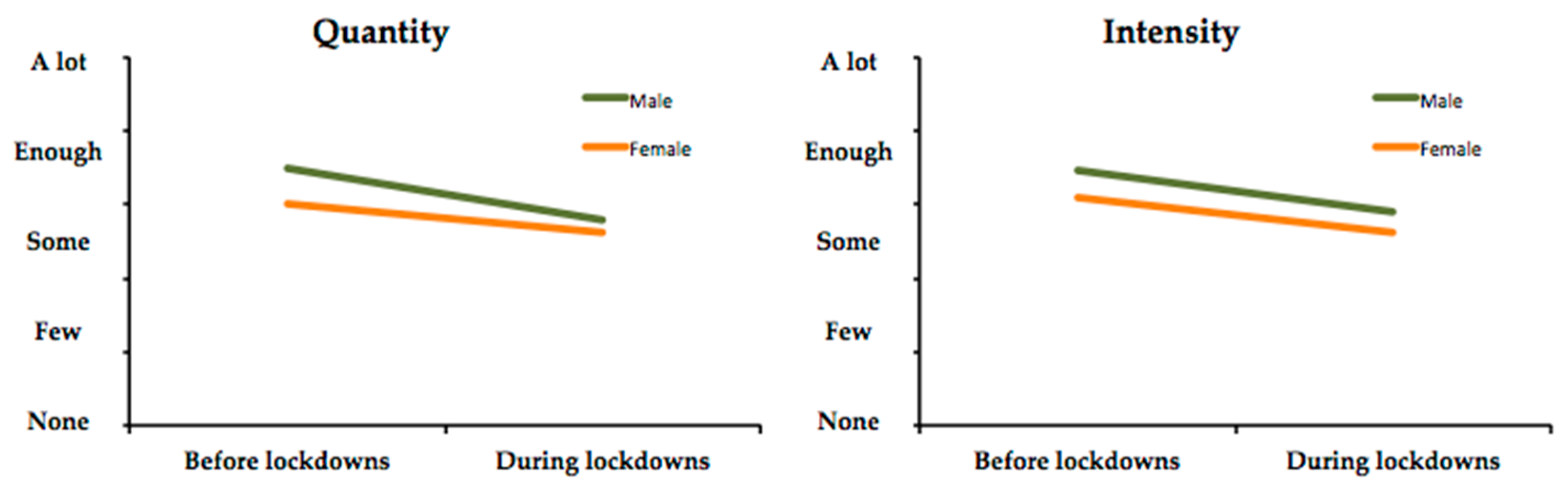
| Quantity | Before | 3.02 | 1.16 | 17,850.000 | −7.458 | 0.000 |
| During | 2.62 | 1.01 | ||||
| Intensity | Before | 3.08 | 0.81 | 8629.500 | −10.729 | 0.000 |
| During | 2.62 | 0.81 | ||||
| Male (n = 508) | ||||||
| Quantity | Before | 3.50 | 1.30 | 9049.000 | −11.283 | 0.000 |
| During | 2.79 | 1.17 | ||||
| Intensity | Before | 3.45 | 0.77 | 4676.500 | −11.655 | 0.000 |
| During | 2.90 | 0.92 | ||||
| BEFORE | DURING | |||
|---|---|---|---|---|
| Female | Male | Female | Male | |
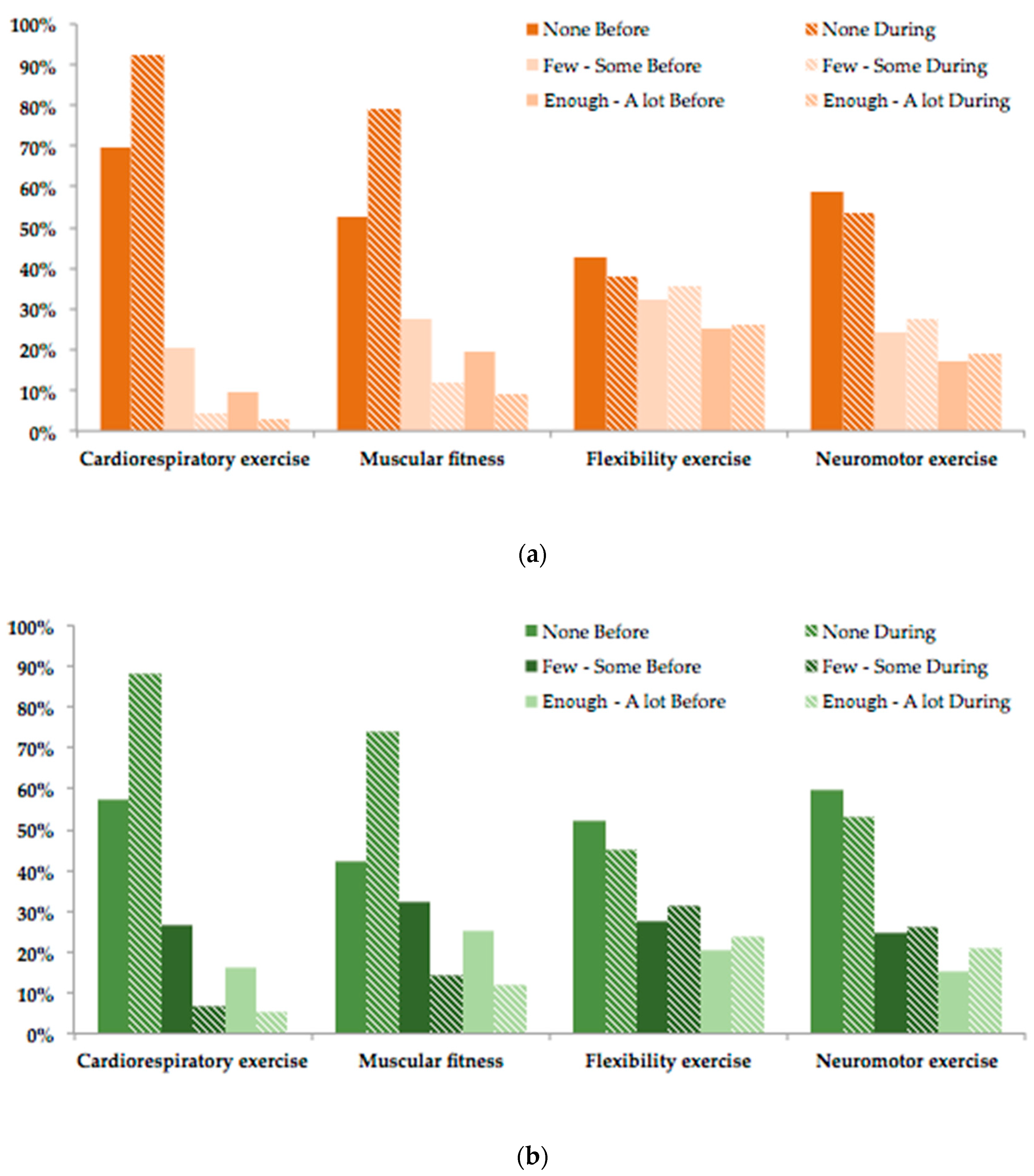
| Cardiorespiratory exercise (1) | ||||
| None | 69.89% | 57.58% | 92.43% | 88.04% |
| Few–Some (<6 h) | 20.45% | 26.38% | 4.55% | 6.84% |
| Enough-A lot (>6 h) | 9.67% | 16.04% | 3.02% | 5.12% |
| Muscular fitness (2) | ||||
| None | 52.86% | 42.44% | 79.03% | 73.94% |
| Few-Some (<6 h) | 27.58% | 32.40% | 11.93% | 14.06% |
| Enough–A lot (>6 h) | 19.55% | 25.16% | 9.03% | 12.01% |
| Flexibility exercise (3) | ||||
| None | 42.75% | 51.97% | 38.10% | 44.98% |
| Few-Some (<6 h) | 32.25% | 27.56% | 35.69% | 31.20% |
| Enough–A lot (>6 h) | 25.00% | 20.47% | 26.21% | 23.82% |
| Neuromotor exercise (4) | ||||
| None | 58.74% | 59.78% | 53.47% | 52.95% |
| Few–Some (<6 h) | 24.29% | 24.80% | 27.51% | 26.25% |
| Enough–A lot (>6 h) | 16.98% | 15.42% | 19.02% | 20.80% |
| Female = 538 Male = 508 | Group | M | SD | Mann–Whitney U | Wilcoxon W | Z | Sig. |
|---|---|---|---|---|---|---|---|
| Quantity_ Variation | Female | −0.40 | 1.21 | 154.937 | 299.928 | 3.883 | 0.000 |
| Male | −0.71 | 1.25 | |||||
| Intensity_ Variation | Female | −0.46 | 0.87 | 141.996 | 286.987 | 1.174 | 0.241 |
| Male | −0.55 | 0.91 |
| None | Few–Some | Enough–A lot | ||||
|---|---|---|---|---|---|---|
| Female | Male | Female | Male | Female | Male | |
| DURING-BEFORE Cardiorespiratory exercise | 22.54% | 30.46% | −15.89% | −19.54% | −6.64% | −10.93% |
| Muscular fitness | 26.17% | 31.50% | −15.65% | −18.35% | −10.52% | −13.15% |
| Flexibility exercise | −4.65% | −6.99% | 3.44% | 3.64% | 1.21% | 3.35% |
| Neuromotor exercise | −5.27% | −6.82% | 3.22% | 1.44% | 2.04% | 5.38% |
| M | SD | Wilcoxon W | Z | Sig. | ||
|---|---|---|---|---|---|---|
| Female (n = 38) | Before | 1.00 | 0.00 | 21.000 | 4.042 | 0.000 |
| During | 1.80 | 0.85 | ||||
| Male (n = 16) | Before | 1.00 | 0.00 | 28.000 | 2.530 | 0.011 |
| During | 1.50 | 0.63 |
| N = 1046 Female = 538 Male = 508 | Group | M | SD | Mann–Whitney U Test | |||
|---|---|---|---|---|---|---|---|
| Mann–Whitney | Wilcoxon W | Z | Sig. | ||||
| (1) | Female | 3.18 | 1.41 | 119.721 | 264.712 | −3567 | 0.000 |
| Male | 3.58 | 1.42 | |||||
| (2) | Female | 2.81 | 1.56 | 179.875 | 324.866 | 9385 | 0.000 |
| Male | 1.94 | 1.31 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
García-Tascón, M.; Sahelices-Pinto, C.; Mendaña-Cuervo, C.; Magaz-González, A.M. The Impact of the COVID-19 Confinement on the Habits of PA Practice According to Gender (Male/Female): Spanish Case. Int. J. Environ. Res. Public Health 2020, 17, 6961. https://doi.org/10.3390/ijerph17196961
García-Tascón M, Sahelices-Pinto C, Mendaña-Cuervo C, Magaz-González AM. The Impact of the COVID-19 Confinement on the Habits of PA Practice According to Gender (Male/Female): Spanish Case. International Journal of Environmental Research and Public Health. 2020; 17(19):6961. https://doi.org/10.3390/ijerph17196961
Chicago/Turabian StyleGarcía-Tascón, Marta, César Sahelices-Pinto, Cristina Mendaña-Cuervo, and Ana María Magaz-González. 2020. "The Impact of the COVID-19 Confinement on the Habits of PA Practice According to Gender (Male/Female): Spanish Case" International Journal of Environmental Research and Public Health 17, no. 19: 6961. https://doi.org/10.3390/ijerph17196961