Fatherhood and Smoking Problems in Indonesia: Exploration of Potential Protective Factors for Men Aged 18–49 Years from the United Nations Multi-Country Study on Men and Violence


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Measures
2.3. Statistical Analysis
3. Results
3.1. Characteristics Study Participants by Current Smoking and CPD
3.2. Factors Associated with Current Smoking
3.3. Factors Associated with CPD
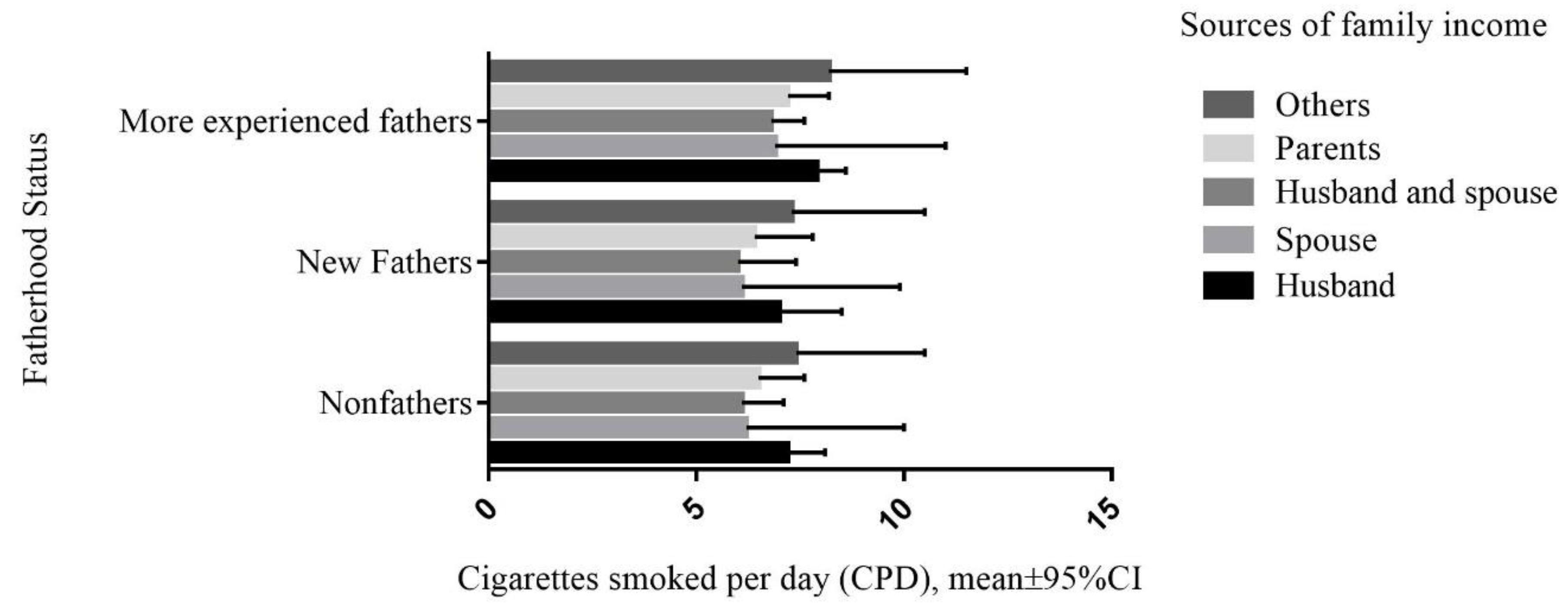
3.4. CPD by Different Fatherhood Status and Sources of Family Income
4. Discussion
4.1. Smoking and Sociodemographic Factors
4.2. Smoking and New Fathers
4.3. Smoking and More Experienced Fathers
4.4. Smoking, Fatherhood and Breadwinner
4.5. Public Health Implications and Recommendations
4.6. Strengths and Limitations of the Study
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ng, M.; Freeman, M.K.; Fleming, T.D.; Robinson, M.; Dwyer-Lindgren, L.; Thomson, B.; Wollum, A.; Sanman, E.; Wulf, S.; Lopez, A.D.; et al. Smoking prevalence and cigarette consumption in 187 countries, 1980–2012. JAMA 2014, 311, 183–192. [Google Scholar] [CrossRef] [Green Version]
- GBD 2015 Tobacco Collaborators. Smoking prevalence and attributable disease burden in 195 countries and territories, 1990–2015: A systematic analysis from the Global Burden of Disease Study 2015. Lancet 2017, 289, 1885–1906. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. WHO Global Report: Mortality Attributable to Tobacco; WHO: Geneva, Switzerland, 2012. [Google Scholar]
- Öberg, M.; Jaakkola, M.S.; Woodward, A.; Peruga, A.; Prüss-Ustün, A. Worldwide burden of disease from exposure to second-hand smoke: A retrospective analysis of data from 192 countries. Lancet 2011, 377, 139–146. [Google Scholar] [CrossRef]
- Kimmel, M.S. The Gendered Society, 4th ed.; Oxford University Press: Oxford, UK, 2011. [Google Scholar]
- Kimmel, M.S.; Hearn, J.; Connell, R.W. Handbook of Studies on Men and Masculinities; Sage Publications: Thousand Oaks, CA, USA, 2005. [Google Scholar]
- Kodriati, N.; Pursell, L.; Hayati, E.N. A scoping review of men, masculinities, and smoking behavior: The importance of settings. Glob. Health Action 2018, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. WHO Report on the Global Tobacco Epidemic 2015: Raising Taxes on Tobacco; WHO: Geneva, Switzerland, 2015. [Google Scholar]
- Tan, Y.L.; Dorotheo, U. The Tobacco Control Atlas: ASEAN Region; Publishing of Suetawan Co., Ltd.: Bangkok, Thailand, 2016. [Google Scholar]
- Eriksen, M.; Mackay, J.; Schluger, N.; Islami, F.; Drope, J. The Tobacco Atlas; American Cancer Society: Atlanta, GA, USA, 2015. [Google Scholar]
- Roberts, B.B. The “Marlboro Men” of the Early Seventeenth Century: Masculine Role Models for Dutch Youths in the Golden Age. Men Masc. 2006, 9, 76–94. [Google Scholar] [CrossRef]
- Nichter, M.; Padmawati, S.; Danardono, M.; Ng, N.; Prabandari, Y.; Mark, N. Reading culture from tobacco advertisements in Indonesia. Tob. Control 2009, 18, 98–107. [Google Scholar] [CrossRef] [Green Version]
- Connell, R. Masculinities; Polity Press: Cambridge, UK, 2005. [Google Scholar]
- Evans, J.; Frank, B.; Oliffe, J.L.; Gregory, D. Health, illness, men, and masculinities (HIMM): A theoretical framework for understanding men and their health. JMH 2011, 8, 7–15. [Google Scholar] [CrossRef] [Green Version]
- Priyatna, C.C. The Invisible Cigarette: The Production of Smoking Culture and Identity in Indonesia; Monash University: Melbourne, Australia, 2013. [Google Scholar]
- Nilan, P. Contemporary masculinities and young men in Indonesia. Indones. Malay World 2009, 37, 327–344. [Google Scholar] [CrossRef]
- Kodriati, N.; Hayati, E.N.; Santosa, A.; Pursell, L. Perceived social benefits versus perceived harms of smoking among Indonesian boys aged 12–16 years: A secondary analysis of Global Youth Tobacco Survey 2014. Tob. Prev. Cessat. 2020, 6. [Google Scholar] [CrossRef] [PubMed]
- Ng, N.; Weinehall, L.; Ohman, A. ‘If I don’t smoke, I’m not a real man’--Indonesian teenage boys’ views about smoking. Health Educ. Res. 2007, 22, 794–804. [Google Scholar] [CrossRef] [Green Version]
- Bottorff, J.L.; Radsma, J.; Kelly, M.; Oliffe, J.L. Fathers’ narratives of reducing and quitting smoking. Sociol. Health Illn. 2009, 31, 185–200. [Google Scholar] [CrossRef] [PubMed]
- Nelson, D.L.; Burke, R.J. (Eds.) Gender, Work, Stress, and Health; American Psychological Association: Washington, DC, USA, 2002. [Google Scholar]
- Gough, B.; Robertson, S. Men, Masculinities, and Health; Palgrave Macmillan: London, UK, 2010. [Google Scholar]
- Lamb, M.E. (Ed.) The Role of the Father in Child Development, 4th ed.; John Wiley & Sons, Inc: Hoboken, NJ, USA, 2004. [Google Scholar]
- Greaves, L.; Oliffe, J.L.; Ponic, P.; Kelly, M.T.; Bottorff, J.L. Unclean fathers, responsible men: Smoking, stigma and fatherhood. Health Sociol. Rev. 2010, 19, 522–533. [Google Scholar] [CrossRef]
- Everett, K.D.; Bullock, L.; Longo, D.R.; Gage, J.; Madsen, R. Men’s tobacco and alcohol use during and after pregnancy. Am. J. Men’s Health 2007, 1, 317–325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blackburn, C.; Bonas, S.; Spencer, N.; Dolan, A.; Coe, C.; Moy, R. Smoking behaviour change among fathers of new infants. Soc. Sci. Med. 2005, 61, 517–526. [Google Scholar] [CrossRef] [PubMed]
- Kwon, J.Y.; Oliffe, J.L.; Bottorff, J.L.; Kelly, M.T. Masculinity and Fatherhood: New Fathers’ Perceptions of Their Female Partners’ Efforts to Assist Them to Reduce or Quit Smoking. Am. J. Men’s Health 2014, 9, 332–339. [Google Scholar] [CrossRef] [Green Version]
- Marsiglio, W. (Ed.) Fatherhood: Contemporary Theory, Research, and Social Policy; Sage: Thousand Oaks, CA, USA, 1995. [Google Scholar]
- Souralová, A.; Fialová, H. Where have all the fathers gone? Remarks on feminist research on transnational fatherhood. NORMA 2017, 12, 159–174. [Google Scholar] [CrossRef]
- Sahabat Keluarga Kementrian Pendidikan dan Kebudayaan. Sejarah Peringatan Hari Ayah di Indonesia. Available online: https://sahabatkeluarga.kemdikbud.go.id/laman/index.php?r=tpost/xview&id=3638 (accessed on 8 January 2020).
- Government of Indonesia. Indonesia labor law no 13 2003. Available online: https://www.ilo.org/dyn/natlex/natlex4.detail?p_lang=en&p_isn=64764&p_country=IDN&p_count=611&p_classification=01&p_classcount=81 (accessed on 8 January 2020).
- Hayati, E.N.; Kodriati, N.; Saeroni; Masud, S.I.; Warner, X.; Roselli, T. Men Experiences of Violence against Women in Indonesia: And How We Can Begin to Prevent It. 2015. Available online: http://www.partners4prevention.org/resource/mens-experiences-violence-against-women-indonesia-and-how-we-can-begin-prevent-it (accessed on 1 September 2020).
- SVRI. UN Multi-Country Study on Men and Violence. Available online: https://www.svri.org/what-we-do/research-support/un-multi-country-study-men-and-violence#:~:text=The%20UN%20Multi%2DCountry%20Study,perpetration%20of%20violence%20against%20women (accessed on 4 September 2020).
- Amalia, B.; Cadogan, S.L.; Prabandari, Y.S.; Filippidis, F.T. Socio-demographic inequalities in cigarette smoking in Indonesia, 2007 to 2014. Prev. Med. 2019, 123, 27–33. [Google Scholar] [CrossRef]
- Tee, G.H. Social determinants of health and tobacco use in five low and middle-income countries-results from the Global Adult Tobacco Survey (GATS), 2011–2012. Asian Pac. J. Cancer Prev. 2016, 17, 1269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sreeramareddy, C.T.; Pradhan, P.M.S.; Mir, I.A.; Sin, S. Smoking and smokeless tobacco use in nine South and Southeast Asian countries: Prevalence estimates and social determinants from Demographic and Health Surveys. Popul. Health Metr. 2014, 12, 22. [Google Scholar] [CrossRef]
- Pemerintah Republik Indonesia. Undang—undang Republik Indonesia nomor 13 tahun 2003 tentang ketenagakerjaan. Available online: https://www.ilo.org/dyn/natlex/docs/ELECTRONIC/64764/71554/F1102622842/IDN64764.pdf (accessed on 8 January 2020).
- Barclay, L.; Lupton, D. The experiences of new fatherhood: A socio-cultural analysis. J. Adv. Nurs. 1999, 29, 1013–1020. [Google Scholar] [CrossRef]
- St John, W.; Cameron, C.; McVeigh, C. Meeting the challenge of new fatherhood during the early weeks. J Obs. Gynecol. Neonatal. Nurs. 2005, 34. [Google Scholar] [CrossRef]
- Juhari, R.; Yaacob, S.N.; Talib, M.A. Father involvement among Malay Muslims in Malaysia. J. Fam. Issues 2013, 34, 210–229. [Google Scholar] [CrossRef]
- Hossain, Z.; Roopnarine, J.L. Mothers’ and fathers’ childcare involvement with young children in rural families in Malaysia. Int. J. Psy. 2005, 40, 385–394. [Google Scholar] [CrossRef] [Green Version]
- Everett, K.D.; Gage, J.; Bullock, L.; Longo, D.R.; Geden, E.; Madsen, R.W. A pilot study of smoking and associated behaviors of low-income expectant fathers. Nicotine Tob. Res. Off. J. Soc. Res. Nicotine Tob. 2005, 7, 269–276. [Google Scholar] [CrossRef] [PubMed]
- Stanton, W. Randomised control trial of a smoking cessation intervention directed at men whose partners are pregnant. Prev. Med. 2004, 38, 6–9. [Google Scholar] [CrossRef] [PubMed]
- Wakefield, M.; Reid, Y.; Roberts, L.; Mullins, R.; Gillies, P. Smoking and smoking cessation among men whose partners are pregnant_a qualitative study. Soc. Sci. Med. 1998, 47, 657–664. [Google Scholar] [CrossRef]
- O’Brien, R.; Hunt, K.; Hart, G. ’The average Scottish man has a cigarette hanging out of his mouth, lying there with a portion of chips’: Prospects for change in Scottish men’s constructions of masculinity and their health-related beliefs and behaviours. Crit. Public Health 2009, 19, 363–381. [Google Scholar] [CrossRef] [Green Version]
- Oliffe, J.L.; Bottorff, J.L.; Sarbit, G. Supporting fathers’ efforts to be smoke free_program principles. Can. J. Nurs. Res. 2012, 44, 64–82. [Google Scholar]
- JHUCCP. Mobilizing for Impact: Indonesia’s SIAGA Campaign Promotes Shared Responsibility; JHPIEGO: Baltimore, MD, USA, 2004. [Google Scholar]


{kind=link}
| Characteristics (n = 2540) | Current Smoking n (%) 1 | CPD 2 Mean ± SD 3 |
|---|---|---|
| Overall | 1695 (66.7) | 7.3 ± 7.8 |
| Age group | p-value = 0.238 | p-value = 0.002 * |
| 18–24 | 424 (64.1) | 6.5 ± 7.2 |
| 25–34 | 561 (68.2) | 7.7 ± 7.8 |
| 35–49 | 710 (67.2) | 7.6 ± 8.1 |
| Education level | p-value < 0.001 * | p-value < 0.008 * |
| Low | 769 (75.6) | 7.7 ± 7.4 |
| Medium | 804 (63.3) | 7.3 ± 7.9 |
| High | 122 (48.4) | 6 ± 8.6 |
| Job category | p-value < 0.001 * | p-value < 0.001 * |
| Never worked/student | 160 (51.8) | 4.8 ± 6.5 |
| Nonmanual | 675 (62.6) | 7.5 ± 8.4 |
| Manual | 860 (74.6) | 7.9 ± 7.4 |
| Partnership status | p-value < 0.005 * | p-value < 0.001 * |
| Single | 502 (62.4) | 6.4 ± 7.1 |
| Married/cohabitated | 1163 (68.9) | 7.7 ± 8.0 |
| Divorced/widowed | 30 (65.2) | 10.9 ± 10.7 |
| Main sources of income | p-value < 0.009 * | p-value < 0.001 * |
| Husband | 1029 (68.4) | 8.0 ± 8.2 |
| Spouse | 12 (70.6) | 7.2 ± 9.3 |
| Both equally | 291 (69.4) | 6.9 ± 7.09 |
| Parents | 345 (60.6) | 5.9 ± 6.7 |
| Others | 18 (60.0) | 7 ± 7.9 |
| Variables | OR of Current Smoking | RR of CPD |
|---|---|---|
| (95% CI) | (95% CI) | |
| Fatherhood (Ref. Nonfather) | ||
| New fathers | 2.28 * (1.09–4.79) | 0.85 (0.70–1.02) |
| More experienced fathers | 1.53 * (1.08–2.17) | 1.01 (0.89–1.15) |
| Age group (Ref. 18–24 years) | ||
| 25–34 years | 0.8 (0.61–1.08) | 1.05 (0.95–1.17) |
| 35–49 years | 0.64 * (0.46–0.88) | 1.02 (0.90–1.15) |
| Education level (Ref. low) | ||
| Medium | 0.63 * (0.52–0.76) | 1.08 (1.01–1.15) |
| High | 0.36 * (0.27–0.49) | 1.14 (0.99–1.31) |
| Job category (Ref. Never worked/student) | ||
| Nonmanual | 1.68 * (1.21–2.33) | 1.19 * (1.03–1.37) |
| Manual | 2.38 * (1.70–3.34) | 1.07 (0.93–1.23) |
| Partnership status (Ref. single) | ||
| Married/cohabitated | 0.83 (0.56–1.24) | 1.00 (0.87–1.16) |
| Divorced/widowed | 0.82 (0.40–1.67) | 1.51* (1.21–1.87) |
| Main sources of income (Ref. husband) | ||
| Spouse | 1.05 (0.36–3.02) | 0.93 (0.55–1.55) |
| Both equally | 1.08 (0.85–1.37) | 0.87 * (0.79–0.95) |
| Parents | 0.96 (0.69–1.33) | 0.89 * (0.79–0.99) |
| Others | 0.73 (0.32–1.65) | 0.97 (0.71–1.32) |
| Inflated Current smoking a | ||
| Current smoker | −29.8 * (−30.3; −29.3) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kodriati, N.; Hayati, E.N.; Santosa, A.; Pursell, L. Fatherhood and Smoking Problems in Indonesia: Exploration of Potential Protective Factors for Men Aged 18–49 Years from the United Nations Multi-Country Study on Men and Violence. Int. J. Environ. Res. Public Health 2020, 17, 6965. https://doi.org/10.3390/ijerph17196965
Kodriati N, Hayati EN, Santosa A, Pursell L. Fatherhood and Smoking Problems in Indonesia: Exploration of Potential Protective Factors for Men Aged 18–49 Years from the United Nations Multi-Country Study on Men and Violence. International Journal of Environmental Research and Public Health. 2020; 17(19):6965. https://doi.org/10.3390/ijerph17196965
Chicago/Turabian StyleKodriati, Nurul, Elli Nur Hayati, Ailiana Santosa, and Lisa Pursell. 2020. "Fatherhood and Smoking Problems in Indonesia: Exploration of Potential Protective Factors for Men Aged 18–49 Years from the United Nations Multi-Country Study on Men and Violence" International Journal of Environmental Research and Public Health 17, no. 19: 6965. https://doi.org/10.3390/ijerph17196965