A Qualitative Research Study Which Explores Humanitarian Stakeholders’ Views on Healthcare Access for Refugees in Greece

Abstract
:1. Introduction
1.1. Refugees in Greece Since the EU–Turkey Deal
1.2. Rhetoric and Reality Concerning Access to Healthcare for Refugees in Greece
- What are the key barriers or facilitators for healthcare access for refugees in Greece (from the perspective of healthcare providers);
- What challenges are faced by providers of healthcare for refugees in Greece when delivering their services;
- The evolution of the health response for refugees in Greece between 2015 and March 2018.
2. Materials and Methods
2.1. Sampling and Participant Recruitment
2.2. Key Informant Interviews
2.3. Data Management and Storage
2.4. Thematic Analysis
2.5. Ethics
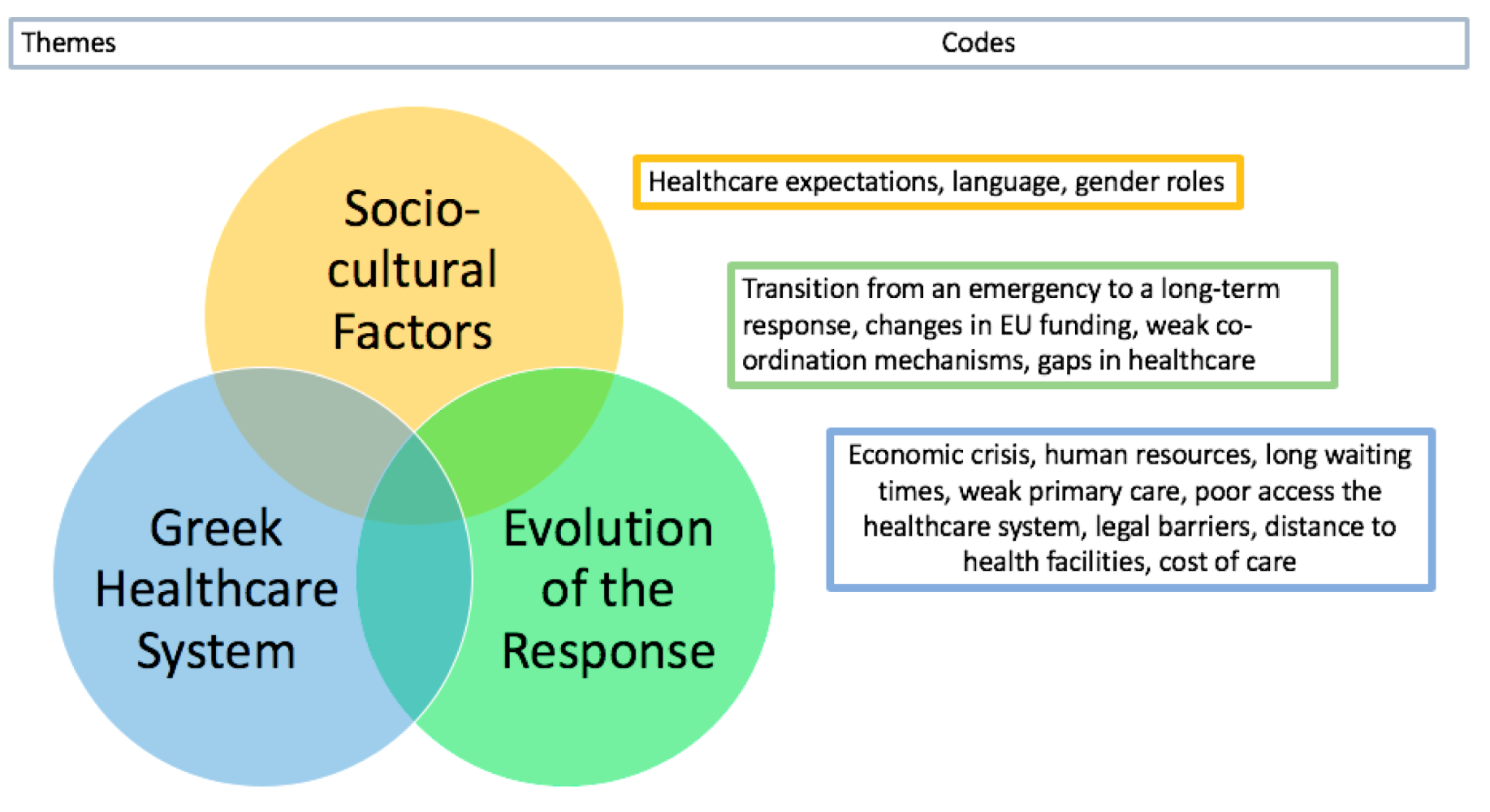
3. Results
3.1. Socio-Cultural Factors
3.1.1. Gender and Cultural Sensitivity of Care Provision
Many of the doctors and other staff are not used to working [with] such a multi-cultural, multi-national patient load so they have not been trained on how to do culturally sensitive medicine. This is another barrier for both of them to communicate effectively.—KI 9
Very frequently there are women who are reluctant to be examined by a male physician or there are men who are reluctant to be examined by a female. Also, for some women, the fact that the decision of whether they access healthcare is made by the male member of the family may restrict their access.—KI 9
3.1.2. Language
With translators our team can see around one hundred patients per day. But without, it can be as low as 20 per day.—KI 1
If sent by themselves with no translator, they [refugee patients] don’t know what’s going on and may find it difficult to transfer medical records back. Therefore, you lose a lot of valuable information. They also don’t know how to interact with the system effectively and advocate for their own needs.—KI 2
3.1.3. Healthcare Expectations
They did not like seeing a primary health care physician; they would rather see a specialist as this was the system they were used to before the war. If you had chest pain, you would see a cardiologist. There was no GP system.—KI 1
Some of the refugees are very used to increased antibiotic prescriptions and although in Greece more antibiotics are prescribed than other European countries, they are still not satisfied if they do not get priority. For some of them, they are used to getting medications such as injections—in Greece injections are not very popular with doctors. So some are not satisfied for reasons of different medical cultures.—KI 9
3.2. The Greek Health System
3.2.1. Greece’s Economic Crisis
Not everyone has access, you are not always able to find the speciality you want, it can take months to get an appointment, there is a big waiting list.—KI 5
3.2.2. Human Resources for Health
It was hard to find people that were willing to go to particular areas. Obviously, people want to live in big cities, but it is hard to get people to relocate to an island.—KI 14
3.2.3. Insufficient Access to Primary Care
If you can do good primary healthcare, everything else becomes easier, you do not need really strong referral services to secondary care if you do good primary health care.—KI 15
3.2.4. Long Waiting Times for Secondary Care Appointments
3.2.5. Perceived Complexity of Access to Secondary Care
The main problem might be that actual healthcare services are not accessible, maybe because the Greek system is complicated. It is difficult for Greek people to access it. People have to get a paper, then get in, then go to another office, then another place. Then sometimes have to go by phone and don’t know how to do it as they can’t speak Greek. It is a complicated system in terms of accessibility. It is not that they do not have access to it.—KI 7
3.2.6. Information Exchange among Stakeholders and with Patients
Knowing where to go [for healthcare] can be challenging [for refugees]. There are a lot of different hospitals here; military hospitals for example … This is not easily navigated or explained unless they have someone to help them. This is why community clinics are good because at least it is a first step and people have set up a referral pathway for them.—KII 11
3.2.7. Legal Barriers
3.2.8. Distance to Health Facilities
In most cases, refugee camps are hidden and away from big cities and towns. They are in hiding. The implications of this is that they cannot be integrated into Greek society.—KI 10
3.2.9. Cost of Care
Working in a European country is hugely expensive compared to working in other countries where you are normally based for emergencies. Just being able to get registered is very costly and time consuming, it is quite difficult…The cost of transport is expensive. We have to rent cars like a tourist would.—KI 14
Compassion fatigue was certainly an issue. Initially it was very popular to be aware of the refugee crisis in the Middle East and in Europe and to interact with that, it was in the news and people were donating and compassionate towards the cause, which dies off very quickly when the next emergency happens or when people don’t want to be sad anymore …—KI 3
Some electronic prescriptions have a contribution fee which is not much money but for some of the patients or refugees, is a significant amount—KI 13
3.3. Evolution of Healthcare Response
…Has become much more organised, much more streamlined in its progression, more urbanised. Services now have become more centralised, based on polyclinics in towns that people can access from wherever they are living rather than [clinics] being in-camp or in refugee communities. [Services have] also been a lot more formalised and regulated—[this is a] positive thing. [There are a] lot less providers, those providers that are here have become more scrutinised, and have more targets to meet—more accountability. [There are] still a lot of issues that need to be addressed fairly urgently—KI 3
After summer 2017, when funding started going to the government, a lot of NGOs started to leave. Then an urgent need on the islands occurred as the government could not handle the situation— KI 12…The situation now is worse than it was last year. The gaps are getting wider, the population that has been there for longer is getting sicker, there is a bigger population and less actors, the mathematics of it is not looking good. We have actually scaled up our operation when they wanted to be scaling down, but they had to do the opposite—KI 15
3.3.1. Weak Co-Ordination Mechanisms
During the peak of the crisis when the awareness was at its highest, in 2015/2016, there was a lot of money flowing, a lot of services being provided, not always in a co-ordinated manner… there was a lot of service provision, perhaps even too much, there were a lot of actors offering similar services…You had 2 or 3 health actors offering services around the clock at a campsite compared to normal living situations where you don’t have 24/7 primary health care—KII 9
We wouldn’t be told that camps were closing until pretty much the day of. This make it hard to plan as an organisation, but it is also hard to reassure people if you do not know what is happening yourself. A lot of volunteers that were with them built up a good relationship, particularly those who spoke Arabic with the refugees, there was a good trust level. But then that suddenly disappears, or they promise to be there the next day but cannot go because they have been moved to another camp. That trust then immediately drops—KI 14
3.3.2. Healthcare Gaps
They often experienced many years of conflict within Syria and then also have the traumatic journey across sea. But the main traumas, in my experience, came from the borders being closed. They had in their mind that they were moving somewhere and going on so had a hope—KI 2
In Athens, a city of 5 million, there are only 2 functioning psychiatric hospitals—KI 13
3.3.3. Transition from an Emergency to a Long-Term Response
After the EU–Turkey deal, the population became “stranded” in Greece and on the islands… Some patients have been there for 2 years now, so their needs have dramatically changed—KII 15
4. Discussion
4.1. Socio-Cultural Factors
4.2. Responsiveness of Greece’s Health System
4.3. Evolution of the Health Response
4.4. Weak Coordination
4.5. Strengths and Limitations of This Study
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| EU | European Union |
| UNHCR | United Nations High Commissioner for Refugees |
| WHO | World Health Organisation |
| FYROM | Former Yugoslav Republic of Macedonia |
| NGO | Non-Governmental Organisation |
| MSF | Médecins Sans Frontières |
| MdM | Médecins du Monde |
| HS | Health System |
| PHC | Primary Health Care |
| KII | Key Informant Interview |
| KI | Key Informant |
| MoH | Ministry of Health |
| AMKA | Αριθμός Μητρώου Κοινωνικής Ασφάλισης (Greek social security number) |
| ECHO | European Civil Protection and Humanitarian Aid Operations |
| NCD | Non-Communicable Diseases |
Appendix A
Appendix A.1. Questionnaire
- (1)
- What is your role in your organisation?
- (2)
- Can you tell me what training you have and about prior experience in similar contexts?
- (3)
- How long have you worked on the Greece response?
- (4)
- Name of organisation
- (5)
- What is the role of the organisation?
- (6)
- How long has it been operational in Greece?
- (7)
- How big is it? E.g.,
- (8)
- How many people are employees in Greece?
- (9)
- How many refugees do you serve?
- (10)
- How many consultations?
- (11)
- What sectors, e.g., MHPSS/MCH/WASH/Shelter, etc. does it work in?
- (12)
- Where in Greece does it operate?
- (13)
- How has its work changed over time, e.g., scope and location?
- (14)
- Who provides primary health care and how has this changed?
- (15)
- Who provides secondary health care and how has this changed?
- (16)
- Who provides speciality care: maternal and child health/psychosocial/pre-natal/dental?
- (17)
- What are the main gaps in service provision in your opinion?
- (18)
- What are the main health issues observed among refugees in Greece? What is not adequately provided for?
- (19)
- Are refugees satisfied with what is provided in primary care?
- (20)
- Are refugees satisfied with what is provided in secondary care?
- (21)
- What are the main barriers to accessing care for refugees in Greece, e.g., Primary/secondary/emergency/maternity?
- (a)
- Physical accessibility
- (b)
- Language
- (c)
- Cultural factors determining care-seeking behaviour
- (d)
- Cost of care
- (22)
- What are the main challenges in providing health care to refugees?
- (23)
- What initiatives are adopted to overcome certain challenges?
- (24)
- How has health service provision changed during your time working in Greece?
- (25)
- What improvements do you think could be made to the provision of healthcare in Greece?
- (26)
- How have the roles of government/NGOs/International agencies changed over the period 2015–2017 and what has influenced these changes?
Appendix B
References
- UNHCR. Greece Factsheet UNHCR. Available online: https://data2.unhcr.org/en/documents/download/74134 (accessed on 21 April 2020).
- UNHCR. UNHCR—Syria Emergency. Available online: https://www.unhcr.org/uk/syria-emergency.html (accessed on 22 April 2020).
- Aburas, R.; Najeeb, A.; Baageel, L.; Mackey, T.K. The Syrian conflict: A case study of the challenges and acute need for medical humanitarian operations for women and children internally displaced persons. BMC Med. 2018, 16, 65. [Google Scholar] [CrossRef] [PubMed]
- WHO. Fake lifejackets play a role in drowning of refugees. In Bulletin of the World Health Organization; World Health Organization: Geneva, Switzerland, 2016; Volume 94, pp. 411–412. [Google Scholar]
- UNHCR. UNHCR—What Is a Refugee? Available online: https://www.unhcr.org/uk/what-is-a-refugee.html (accessed on 22 April 2020).
- Watch, H.R. Q&A: Why the EU-Turkey Migration Deal is No Blueprint|Human Rights Watch. 2016. Available online: https://www.hrw.org/news/2016/11/14/qa-why-eu-turkey-migration-deal-no-blueprint (accessed on 22 April 2020).
- Batalla Adam, L. The EU-Turkey Deal One Year On: A Delicate Balancing Act. Int. Spect. 2017, 52, 44–58. [Google Scholar] [CrossRef]
- UNHCR. Mediterranean Situation UNHCR. 2018. Available online: https://data2.unhcr.org/en/situations/mediterranean (accessed on 23 March 2018).
- Kingsley, P. Migration to Greece Is Rising, as Erdogan Warns of Still More—The New York Times. The New York Times. 2019. Available online: https://www.nytimes.com/2019/09/11/world/europe/greece-migrants-erdogan-lesbos-syria.html?auth=login-email&login=email (accessed on 22 April 2020).
- BBC. Greece Moves Thousands of Migrants from Idomeni Camp—BBC News; BBC News: 2016. Available online: https://www.bbc.co.uk/news/world-europe-36358891 (accessed on 22 April 2020).
- Kouparanis, P. Makeshift Refugee Camps in Northern Greece Evacuated|Europe|News and Current Affairs from around the Continent|DW|11.06.2016; Deutsche Welle: 2016. Available online: https://www.dw.com/en/makeshift-refugee-camps-in-northern-greece-evacuated/a-19323822 (accessed on 22 April 2020).
- UNHCR. Greece. 2019. Available online: www.unhcr.org (accessed on 22 April 2020).
- Ekathimerini. Moria Migrant Camp on Lesvos Breaks New Record with Nearly 14,000 residents|News|ekathimerini.com; Ekathimerini.com: 2019. Available online: https://www.ekathimerini.com/245523/article/ekathimerini/news/moria-migrant-camp-on-lesvos-breaks-new-record-with-nearly-14000-residents (accessed on 22 April 2020).
- Mellou, K.; Silvestros, C.; Georgakopoulou, T.; Koustenis, A.; Kokkinou, E.; Botsi, C.; Terzidis, A. Activities for Increasing Childhood Vaccination Coverage of the Refugee and Migrant Population, Greece, European Program PHILOS, 2017. Int. Sch. Sci. Res. Innov. 2018, 12. Available online: https://waset.org/pdf/books/?id=77245&pageNumber=1 (accessed on 23 May 2018).
- Ben Farhat, J.; Blanchet, K.; Juul Bjertrup, P.; Veizis, A.; Perrin, C.; Coulborn, R.M.; Mayaud, P.; Cohuet, S. Syrian refugees in Greece: Experience with violence, mental health status, and access to information during the journey and while in Greece. BMC Med. 2018, 16, 40. Available online: http://www.ncbi.nlm.nih.gov/pubmed/29530041 (accessed on 15 May 2018). [CrossRef] [PubMed]
- Arsenijević, J.; Schillberg, E.; Ponthieu, A.; Malvisi, L.; Ahmed, W.A.E.; Argenziano, S.; Zamatto, F.; Burroughs, S.; Severy, N.; Hebting, C.; et al. A crisis of protection and safe passage: Violence experienced by migrants/refugees travelling along the Western Balkan corridor to Northern Europe. Confl. Health 2017, 11, 6. [Google Scholar] [CrossRef] [PubMed]
- Christoldoulou, G.N.; Abou-Saleh, M.T. Greece and the Refugee Crisis: Mental Health Context. Available online: https://www.cambridge.org/core/services/aop-cambridge-core/content/view/5CA44CAA39B0A4930610AF212EAB0298/S2056474000001410a.pdf/div-class-title-greece-and-the-refugee-crisis-mental-health-context-div.pdf (accessed on 20 September 2020).
- Gunst, M.; Jarman, K.; Yarwood, V.; Rokadiya, S.; Capsaskis, L.; Orcutt, M.; Abbara, A. Healthcare access for refugees in Greece: Challenges and opportunities. Health Policy 2019, 123, 818–824. [Google Scholar] [CrossRef]
- Bradby, H.; Lebano, A.; Hamed, S.; Gil-Salmerón, A.; Durá-Ferrandis, E.; Garcés-Ferrer, J.; Sherlaw, W.; Chrisova, I.; Karnaki, P.; Zoata, D.; et al. Policy Makers’, NGO, and Healthcare Workers’ Accounts of Migrants’ and Refugees’ Healthcare Access Across Europe—Human Rights and Citizenship Based Claims. Front. Sociol. 2020, 5, 16. [Google Scholar] [CrossRef] [Green Version]
- Kotsiou, O.; Kotsios, P.; Srivastava, D.; Kotsios, V.; Gourgoulianis, K.; Exadaktylos, A. Impact of the refugee crisis on the Greek Healthcare System: A long road to Ithaca. Int. J. Environ. Res. Public Health 2018, 15, 1790. [Google Scholar] [CrossRef] [Green Version]
- Kousoulis, A.A.; Ioakeim-Ioannidou, M.; Economopoulos, K.P. Access to health for refugees in Greece: Lessons in inequalities. Int. J. Equity Health 2016, 15, 122. [Google Scholar] [CrossRef] [Green Version]
- European Public Health Alliance. Access to Health Is a Luxury for Stranded Refugees in Greece—EPHA; EPHA: 2020. Available online: https://epha.org/access-to-health-is-a-luxury-for-stranded-refugees-in-greece (accessed on 22 April 2020).
- Kotsiou, O.S.; Kotsios, V.S.; Gourgoulianis, K.I. Enhanced Public Interest in Response to the Refugee and Healthcare Crises in Greece. Int. J. Environ. Res. Public Health 2020, 17, 2272. [Google Scholar] [CrossRef] [Green Version]
- Moris, D.; Kousoulis, A. Refugee crisis in Greece: Healthcare and integration as current challenges. Perspect. Public Health 2017, 137, 309–310. [Google Scholar] [CrossRef] [PubMed]
- Papadimos, T.; Pappada, S.; Lyaker, M.; Papadimos, J.; Casabianca, A. Health Security and the Refugee Crisis in Greece: The Refugee Perspective; Intechopen: London, UK, 2020. [Google Scholar]
- Gale, N.K.; Heath, G.; Cameron, E.; Rashid, S.; Redwood, S. Using the framework method for the analysis of qualitative data in multi-disciplinary health research. BMC Med. Res. Methodol. 2013, 13, 117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Economou, C.; Kaitelidou, D.; Kentikelenis, A.; Maresso, A.; Sissouras, A. The Impact of the Financial Crisis on Health and the Health System in Greece. In Economic Crisis, Health Systems and Health in Europe: Country Experience; Maresso, A., Ed.; WHO/European Observatory on Health Systems and Policies: Copenhagen, Denmark, 2015; pp. 103–142. [Google Scholar]
- Woloshin, S.; Bickell, N.A.; Schwartz, L.M.; Gany, F.; Welch, H.G. Language Barriers in Medicine in the United States. JAMA J. Am. Med. Assoc. 1995, 273, 724. [Google Scholar] [CrossRef]
- Kerasidou, A.; Kingori, P.; Legido-Quigley, H. “You have to keep fighting”: Maintaining healthcare services and professionalism on the frontline of austerity in Greece. Int. J. Equity Health 2016, 15, 118. [Google Scholar] [CrossRef] [Green Version]
- Shirinzadeh, S.A.; Mahadi, T.S.T. Translators as Cultural Mediators in Transmitting Cultural Differences. Procedia Soc. Behav. Sci. 2015, 208, 167–174. [Google Scholar] [CrossRef] [Green Version]
- Deane, S. Syria’s Lost Generation: Refugee Education Provision and Societal Security in an Ongoing Conflict Emergency. IDS Bull. 2016, 47. [Google Scholar] [CrossRef]
- Bader, Y.; Bani-Ali, N. Consonantal Variation in Syrian Refugees’ Speech in Jordan. J. Appl. Linguist. Lang. Res. 2020, 7, 1–18. [Google Scholar]
- Baban, F.; Ilcan, S.; Rygiel, K. Syrian refugees in Turkey: Pathways to precarity, differential inclusion, and negotiated citizenship rights. J. Ethn. Migr. Stud. 2017, 43, 41–57. [Google Scholar] [CrossRef]
- Hémono, R.; Relyea, B.; Scott, J.; Khaddaj, S.; Douka, A.; Wringe, A. The needs have clearly evolved as time has gone on: A qualitative study to explore stakeholders’ perspectives on the health needs of Syrian refugees in Greece following the 2016 European Union-Turkey agreement. Confl. Health 2018, 12, 1–9. [Google Scholar] [CrossRef]
- NaTakallam. Available online: https://natakallam.com/ (accessed on 22 April 2020).
- İçduygu, A.; Şimşek, D. Syrian refugees in turkey: Towards integration policies. Turk. Policy Q. 2016, 15, 59–69. [Google Scholar]
- Chillingaryan, K.P.; Zvereva, E. Linguistic and cultural mediation in health care settings: An overview of Russia and Turkey. In Proceedings of the ADVED 2018—4th International Conference on Advances in Education and Social Sciences, Istanbul, Turkey, 15–17 October 2018. [Google Scholar]
- Lokot, M. ‘Blood Doesn’t Become Water’? Syrian Social Relations during Displacement. Available online: https://doi.org/10.1093/jrs/fey059 (accessed on 22 April 2020).
- Asgary, R.; Segar, N. Barriers to Health Care Access among Refugee Asylum Seekers. J. Health Care Poor Underserved 2011, 22, 506–522. [Google Scholar] [CrossRef] [PubMed]
- New Greek Primary Health Care Network Celebrates 1 Year of Operation. Available online: https://www.euro.who.int/en/countries/greece/news/news/2018/12/new-greek-primary-health-care-network-celebrates-1-year-of-operation (accessed on 15 December 2018).
- Kotsiou, O.; Srivastava, D.; Kotsios, P.; Exadaktylos, A.; Gourgoulianis, K. The Emergency Medical System in Greece: Opening Aeolus’ Bag of Winds. Int. J. Environ. Res. Public Health 2018, 15, 745. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zavras, D.; Tsiantou, V.; Pavi, E.; Mylona, K.; Kyriopoulos, J. Impact of economic crisis and other demographic and socio-economic factors on self-rated health in Greece. Eur. J. Public Health 2013, 23, 206–210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kentikelenis, A.; Karanikolos, M.; Papanicolas, I.; Basu, S.; McKee, M.; Stuckler, D. Health effects of financial crisis: Omens of a Greek tragedy. Lancet 2011, 378, 1457–1458. [Google Scholar] [CrossRef] [Green Version]
- Tountas, Y.; Karnaki, P.; Pavi, E.; Souliotis, K. The “unexpected” growth of the private health sector in Greece. Health Policy 2005, 74, 167–180. [Google Scholar] [CrossRef]
- United Nations. Sustainable Development Goals; United Nations. Available online: https://sustainabledevelopment.un.org/?menu=1300 (accessed on 22 April 2020).
- Starfield, B.; Shi, L.; Macinko, J. Contribution of Primary Care to Health Systems and Health. Milbank Q. 2005, 83, 457–502. [Google Scholar] [CrossRef]
- European Civil Protection and Humanitarian Aid Operations. 2018. Available online: http://ec.europa.eu/echo/files/aid/countries/factsheets/greece_en.pdf (accessed on 9 May 2018).
- Lopes Cardozo, B.; Gotway Crawford, C.; Eriksson, C.; Zhu, J.; Sabin, M.; Ager, A.; Foy, D.; Snider, L.; Shcholte, W.; Kiaser, R.; et al. Psychological Distress, Depression, Anxiety, and Burnout among International Humanitarian Aid Workers: A Longitudinal Study. PLoS ONE 2012, 7, e44948. [Google Scholar] [CrossRef] [Green Version]
- Dyer, A. 49.4 Building Resilience in Humanitarian Workers Responding to the Refugee Crisis in Greece. J. Am. Acad. Child Adolesc. Psychiatry 2017, 56, S73. [Google Scholar]
- Managing Migration EU Financial Support to Greece. February 2019. Available online: https://ec.europa.eu/home-affairs/sites/homeaffairs/files/what-we-do/policies/european-agenda-migration/201902_managing-migration-eu-financial-support-to-greece_en.pdf (accessed on 19 September 2020).
- Nianias, H. Refugees in Lesbos: Are There too Many NGOs on the Island?|Global Development Professionals Network|The Guardian. Available online: https://www.theguardian.com/global-development-professionals-network/2016/jan/05/refugees-in-lesbos-are-there-too-many-ngos-on-the-island (accessed on 22 April 2020).
- Rantsiou, F. Refugee Response in Greece: A Flawed System|Comment|Ekathimerini.com; Ekathiminerini.com: 2016. Available online: https://www.ekathimerini.com/214403/opinion/ekathimerini/comment/refugee-response-in-greece-a-flawed-system (accessed on 22 April 2020).
- Jervelund, S.S.; Nordheim, O.; Stathopoulou, T.; Eikemo, T.A. Non-communicable Diseases among Refugee Claimants in Greek Refugee Camps: Are Their Health-care Needs Met? J. Refug. Stud. 2019, 32, i36–i51. [Google Scholar] [CrossRef]
- Jefee-Bahloul, H.; Bajbouj, M.; Alabdullah, J.; Hassan, G.; Barkil-Oteo, A. Mental health in Europe’s Syrian refugee crisis. Lancet Psychiatry 2016, 3, 315–317. [Google Scholar] [CrossRef]
- Reindorp, N.; Wiles, P. Humanitarian Coordination: Lessons from Recent Field Experience; Overseas Development Institute: London, UK, 2001. [Google Scholar]


{kind=link}
| Location | N = 16 | % |
|---|---|---|
| London, England | 2 | 13 |
| Athens, Greece | 7 | 44 |
| Skype/Phone | 7 | 44 |
| Gender | ||
| Male | 7 | 44 |
| Female | 9 | 56 |
| Age | ||
| <30 | 4 | 25 |
| 30–39 | 8 | 50 |
| 40–49 | 3 | 19 |
| >50 | 1 | 6 |
| Number of years working on Greece response | ||
| <1 year | 2 | 13 |
| 1–2 years | 6 | 38 |
| >2 year | 8 | 50 |
| Organisation | ||
| NGOs * (local and international) | 11 | 69 |
| International organisations * | 5 | 31 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Joseph, L.; Ismail, S.A.; Gunst, M.; Jarman, K.; Prior, D.; Harris, M.; Abbara, A. A Qualitative Research Study Which Explores Humanitarian Stakeholders’ Views on Healthcare Access for Refugees in Greece. Int. J. Environ. Res. Public Health 2020, 17, 6972. https://doi.org/10.3390/ijerph17196972
Joseph L, Ismail SA, Gunst M, Jarman K, Prior D, Harris M, Abbara A. A Qualitative Research Study Which Explores Humanitarian Stakeholders’ Views on Healthcare Access for Refugees in Greece. International Journal of Environmental Research and Public Health. 2020; 17(19):6972. https://doi.org/10.3390/ijerph17196972
Chicago/Turabian StyleJoseph, Liz, Sharif A. Ismail, Meghan Gunst, Kate Jarman, Dina Prior, Matthew Harris, and Aula Abbara. 2020. "A Qualitative Research Study Which Explores Humanitarian Stakeholders’ Views on Healthcare Access for Refugees in Greece" International Journal of Environmental Research and Public Health 17, no. 19: 6972. https://doi.org/10.3390/ijerph17196972