Clinical Application of Mindfulness-Oriented Meditation: A Preliminary Study in Children with ADHD

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
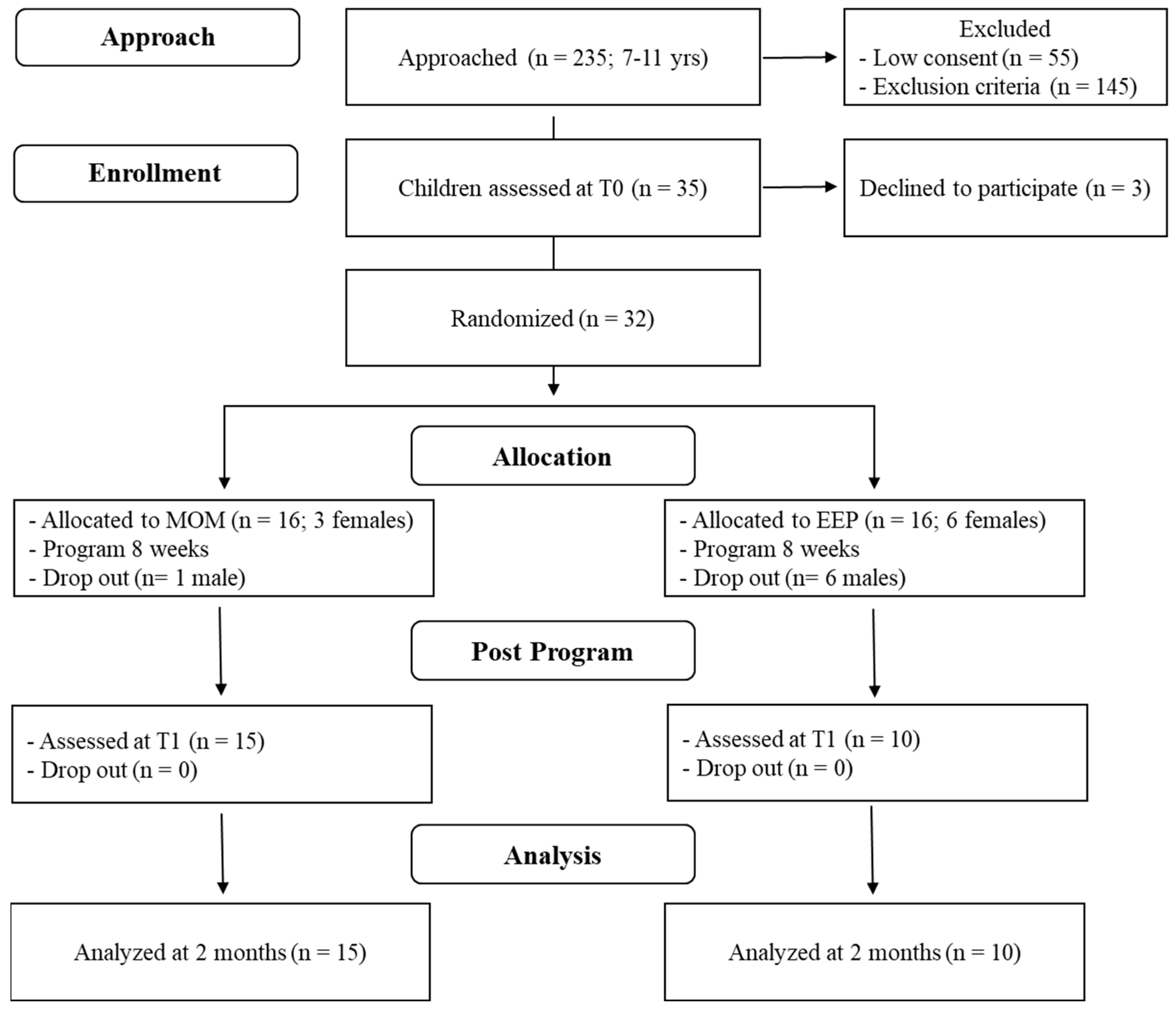
2.1. Participants
2.2. Procedure
2.3. Mindfulness-Oriented Meditation Training
2.4. Emotion Education Program
3. Measures
3.1. Neuropsychological Measures
3.2. Parent and Self-Report Questionnaires
3.3. Academic Skills
4. Results
Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Rowland, A.S.; Skipper, B.J.; Umbach, D.M.; Rabiner, D.L.; Campbell, R.A.; Naftel, A.J.; Sandler, D.P. The prevalence of ADHD in a population-based sample. J. Atten. Disord. 2015, 19, 741–754. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; (DSM-5); American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Kessler, R.C.; Adler, L.; Barkley, R.; Biederman, J.; Conners, C.K.; Demler, O.; Faraone, S.V.; Greenhill, L.L.; Howes, M.J.; Secnik, K.; et al. The prevalence and correlates of adult ADHD in the United States: Results from the national comorbidity survey replication. Am. J. Psychiatry 2006, 163, 716–723. [Google Scholar] [CrossRef]
- Willcutt, E.G.; Doyle, A.E.; Nigg, J.T.; Faraone, S.; Pennington, B.F. Validity of the executive function theory of attention-deficit/hyperactivity disorder: A meta-analytic review. Biol. Psychol. 2005, 57, 1336–1346. [Google Scholar] [CrossRef]
- Singh, A.; Yeh, C.J.; Verma, N.; Das, A.K. Overview of attention deficit/ hyperactivity disorder in young children. Health Psychol. Res. 2015, 3, 23–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pennington, B.F.; Ozonoff, S. Executive functions and developmentalpsychopathology. J. Child Psychol. Psychiatry 1996, 37, 51–87. [Google Scholar] [CrossRef]
- Barkley, R.A. Behavioral inhibition, sustained attention, and executive functions: Constructing a unifying theory of ADHD. Psychol. Bull. 1997, 121, 65–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rubia, K.; Taylor, E.; Smith, H.; Oksannen, H.; Overmeyer, S.; Newman, S. Neuropsychological analyses of impulsiveness in childhood hyperactivity. Br. J. Psychiatry 2001, 179, 138–143. [Google Scholar] [CrossRef] [Green Version]
- Castellanos, F.X.; Tannock, R. Neuroscience of attention-deficit/hyperactivity disorder: The search for endophenotypes. Nat. Rev. Neurosci. 2002, 3, 617–628. [Google Scholar] [CrossRef]
- Martinussen, R.; Hayden, J.; Hogg-Johnson, S.; Tannock, R. A meta-analysis of working memory impairments in children with attention-deficit/hyperactivity disorder. J. Am. Acad. Child Adolesc. Psychiatry 2005, 44, 377–384. [Google Scholar] [CrossRef]
- Nigg, J.T.; Stavro, G.; Ettenhofer, M.; Hambrick, D.Z.; Miller, T.; Henderson, J.M. Executive functions and ADHD in adults: Evidence for selective effects on ADHD symptom domains. J. Abnorm. Psychol. 2005, 114, 706–717. [Google Scholar] [CrossRef] [Green Version]
- Doyle, A.E. Executive functions in attention-deficit/hyperactivity disorder. J. Clin. Psychiatry 2006, 67, 21–26. [Google Scholar] [PubMed]
- Seidman, L.J.; Valera, E.M.; Makris, N.; Monuteaux, M.C.; Boriel, D.L.; Kelkar, K.; Kennedy, D.N.; Caviness, V.S.; Bush, G.; Aleardi, M.; et al. Dorsolateral prefrontal and anterior cingulated cortex volumetric abnormalities in adults with attention-deficit/hyperactivity disorder identified by magnetic resonance imaging. Biol. Psychiatry 2006, 60, 1071–1080. [Google Scholar] [CrossRef] [PubMed]
- Barkley, R.A.; Murphy, K.R. Impairment in occupational functioning and adult ADHD: The predictive utility of executive function (EF) rating versus EF tests. Arch. Clin. Neuropsychol. 2010, 25, 157–173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rubia, K.; Halari, R.; Cubillo, A.; Mohammad, A.M.; Scott, S.; Brammer, M. Disorder-specific inferior prefrontal hypofunction in boys with pure attention-deficit/hyperactivity disorder compared to boys with pure conduct disorder during cognitive flexibility. Hum. Brain Mapp. 2010, 31, 1823–1833. [Google Scholar] [CrossRef] [PubMed]
- Nigg, J.T. Attention-deficit/hyperactivity disorder and adverse health outcomes. Clin. Psychol. Rev. 2012, 33, 215–228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hinshaw, S.P.; Arnold, L.E.; MTA Cooperative Group. Attention-deficit hyperactivity disorder, multimodal treatment, and longitudinal outcome: Evidence, paradox, and challenge. Wiley Interdiscip. Rev. Cogn. Sci. 2015, 6, 39–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Institute for Health and Care Excellence. Clinical Guideline 72 [CG72]. Attention Deficit Hyperactivity Disorder: Diagnosis and Management of ADHD in Children, Young People and Adults; Scope NICE: London, UK, 2008. [Google Scholar]
- National Institute for Health and Care Excellence. NICE Guideline 87 [NG87]. Attention Deficit Hyperactivity Disorder: Diagnosis and Management; Scope NICE: London, UK, 2018. [Google Scholar]
- MTA Cooperative Group. Moderators and mediators of treatment response for children with attention-deficit/hyperactivity disorder: The multimodal treatment study of children with attention-deficit/hyperactivity disorder. Arch. Gen. Psychiatry 1999, 56, 1088–1096. [Google Scholar] [CrossRef] [PubMed]
- American Academy Child and Adolescent Psychiatry. Practice parameters for the use of stimulant medication in children, adolescent and adults. J. Am. Acad. Child. Adolesc. Psychiatry 2002, 41, 26S–49S. [Google Scholar] [CrossRef]
- Cairncross, M.; Miller, C.J. The effectiveness of mindfulness-based therapies for ADHD: A meta-analytic review. J. Atten. Disord. 2016, 20, 1–17. [Google Scholar] [CrossRef]
- Zhang, J.; Díaz-Román, A.; Cortese, S. Meditation-based therapies for attention-deficit/hyperactivity disorder in children, adolescents, and adults: A systematic review and meta-analysis. Evid. Based Ment. Health 2018, 21, 87–94. [Google Scholar] [CrossRef]
- Brown, K.W.; Ryan, R.M. The benefits of being present: Mindfulness and its role in psychological well-being. J. Pers. Soc. Psychol. 2003, 84, 822–848. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kabat-Zinn, J. Mindfulness-based interventions in context: Past, present, and future. Clin. Psychol. 2003, 10, 144–156. [Google Scholar] [CrossRef]
- Bishop, S.R.; Lau, M.; Shapiro, S.; Carlson, L.; Anderson, N.; Carmody, J.; Segal, Z.; Abbey, S.; Speca, M.; Velting, D.; et al. Mindfulness: A proposed operational definition. Clin. Psychol. 2004, 11, 230–241. [Google Scholar] [CrossRef]
- Hölzel, B.K.; Lazar, S.W.; Gard, T.; Schuman-Olivier, Z.; Vago, D.R.; Ott, U. How does mindfulness meditation work? Proposing mechanisms of action from a conceptual and neural perspective. Perspect. Psychol. Sci. 2011, 6, 537–559. [Google Scholar] [CrossRef]
- Malinowski, P. Neural mechanisms of attentional control in mindfulness meditation. Neuroscience 2013, 7, 8. [Google Scholar] [CrossRef] [Green Version]
- Evans, S.; Ling, M.; Hill, B.; Rinehart, N.; Austin, D.; Sciberras, E. Systematic review of meditation-based interventions for children with ADHD. Eur. Child Adolesc. Psychiatry 2017, 27, 9–27. [Google Scholar] [CrossRef]
- Carsley, D.; Khoury, B.; Heath, N.L. Effectiveness of mindfulness interventions for mental health in Schools: A comprehensive meta-analysis. Mindfulness 2018, 9, 693–707. [Google Scholar] [CrossRef]
- Dunning, D.L.; Griffiths, K.; Kuyken, W.; Crane, C.; Foulkes, L.; Parker, J.; Dalgleish, T. Research review: The effects of mindfulness-based interventions on cognition and mental health in children and adolescents—A meta-analysis of randomized controlled trials. J. Child Psychol. Psychiatry 2019, 60, 244–258. [Google Scholar] [CrossRef] [Green Version]
- Biegel, G.M.; Brown, K.W.; Shapiro, S.L.; Schubert, C.M. Mindfulness-based stress reduction for the treatment of adolescent psychiatric outpatients: A randomized clinical trial. J. Consult. Clin. Psychol. 2009, 77, 855–866. [Google Scholar] [CrossRef] [Green Version]
- Burke, C.A. Mindfulness-based approaches with children and adolescents: A preliminary review of current research in an emergent field. J. Child Fam. Stud. 2010, 19, 133–144. [Google Scholar] [CrossRef]
- Flook, L.; Smalley, S.L.; Kitil, M.J.; Galla, B.M.; Kaiser-Greenland, S.; Locke, J.; Ishijima, E.; Kasari, C. Effects of mindful awareness practices on executive functions in elementary school children. J. Appl. Sch. Psychol. 2010, 26, 70–95. [Google Scholar] [CrossRef]
- Semple, R.J.; Lee, J.; Rosa, D.; Miller, L.F. A randomized trial of mindfulness-based cognitive therapy for children: Promoting mindful attention to enhance social-emotional resiliency in children. J. Child Fam. Stud. 2010, 19, 218–229. [Google Scholar] [CrossRef]
- Thompson, M.; Gauntlett-Gilbert, J. Mindfulness with children and adolescents: Effective clinical application. Clin. Child Psychol. Psychiatry 2008, 13, 395–407. [Google Scholar] [CrossRef] [PubMed]
- Allen, N.B.; Chambers, R.; Knight, W.; Melbourne Academic Mindfulness Interest Group. Mindfulness-based psychotherapies: A review of conceptual foundations, empirical evidence and practical considerations. Aust. N. Z. J. Psychiatry 2016, 40, 285–294. [Google Scholar]
- Beauchemin, J.; Hutchins, T.L.; Patterson, F. Mindfulness meditation may lessen anxiety, promote social skills, and improve academic performance among adolescents with learning disabilities. J. Evid. Based Integr. Med. 2008, 13, 34–45. [Google Scholar] [CrossRef] [Green Version]
- Broderick, P.C.; Metz, S. Learning to BREATHE: A pilot trial of a mindfulness curriculum for adolescents. Adv. Sch. Ment. Health Promot. 2009, 2, 35–46. [Google Scholar] [CrossRef]
- Zoogman, S.; Goldberg, S.B.; Hoyt, W.T.; Miller, L. Mindfulness interventions with youth: A meta-analysis. Mindfulness 2014, 6, 290–302. [Google Scholar] [CrossRef]
- Napoli, M.; Krech, P.R.; Holley, L.C. Mindfulness training for elementary school students: The attention academy. J. Appl. Sch. Psychol. 2005, 21, 99–125. [Google Scholar] [CrossRef]
- Geronimi, E.M.; Arellano, B.; Woodruff-Borden, J. Relating mindfulness and executive function in children. Clin. Child. Psychol. Psychiatry 2020, 25, 1–11. [Google Scholar] [CrossRef]
- Van Dam, N.T.; van Vugt, M.K.; Vago, D.R.; Schmalzl, L.; Saron, C.D.; Olendzki, A.; Meissner, T.; Lazar, S.W.; Kerr, C.E.; Gorchov, J.; et al. Mind the hype: A critical evaluation and prescriptive agenda for research on mindfulness and meditation. Perspect. Psychol. Sci. 2018, 13, 36–61. [Google Scholar] [CrossRef]
- Fabbro, F.; Muratori, F. La mindfulness: Un nuovo approccio psicoterapeutico in età evolutiva. G. Ital. Di Neuropsichiatr. Dell’età Evol. 2012, 32, 248–259. [Google Scholar]
- Gunaratana, H. Mindfulness in Plain; English Wisdom Publications: Somerville, MA, USA, 2002. [Google Scholar]
- Kabat-Zinn, J. An outpatient program in behavioral medicine for chronic pain patients based on the practice of mindfulness meditation: Theoretical considerations and preliminary results. Gen. Hosp. Psychiatry 1982, 4, 33–47. [Google Scholar] [CrossRef]
- Kabat-Zinn, J. Full Catastrophe Living: The Program of the Stress Reduction Clinic at the University of Massachusetts Medical Center; Dell: New York, NY, USA, 1990. [Google Scholar]
- Haydicky, J.; Wiener, C.; Badali, P.; Milligan, K.; Ducharme, J.M. Evaluation of a mindfulness-based intervention for adolescents with learning disability and co-occurring ADHD and anxiety. Mindfulness 2012, 3, 151–164. [Google Scholar] [CrossRef]
- Crescentini, C.; Capurso, V.; Furlan, S.; Fabbro, F. Mindfulness-oriented meditation for primary school children: Effects on attention and psychological well-being. Front Psychol. 2016, 7, 805. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Viechtbauer, W.; Smits, L.; Kotz, D.; Budé, L.; Spigt, M.; Serroyen, J.; Crutzen, R. A simple formula for the calculation of sample size in pilot studies. J. Clin. Epidemiol. 2015, 68, 1375–1379. [Google Scholar] [CrossRef] [Green Version]
- Kaufman, J.; Birmaher, B.; Brent, D.; Rao, U. Schedule for affective disorders and schizophrenia for school-age children-present lifetime version (K-SADS-PL): Initial reliability and validity data. J. Am. Acad. Child Adolesc. Psychiatry 1997, 36, 980–988. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th ed.; (DSM-IV-TR); American Psychiatric Association: Washington, DC, USA, 2000. [Google Scholar]
- Shaffer, D.; Gould, M.S.; Brasic, J.; Ambrosini, P.; Fisher, P.; Bird, H.; Aluwahlia, S. A children’s Global Assessment Scale (C-GAS). Arch. Gen. Psychiatry 1983, 40, 1228–1231. [Google Scholar] [CrossRef]
- Orsini, A.; Pezzuti, L.; Picone, L. WISC-IV: Contributo Alla Taratura Italiana; (Italian Edition); Giunti, O.S., Ed.; Organizzazioni Speciali: Firenze, Italy, 2012. [Google Scholar]
- Raven, J.C. Coloured Progressive Matrices-CPM, Series A, AB, B; (Italian Adaptation); Giunti, O.S., Ed.; Organizzazioni Speciali: Firenze, Italy, 2008. [Google Scholar]
- Campanella, F.; Crescentini, C.; Urgesi, C.; Fabbro, F. Mindfulness-oriented meditation improves self-related character scales in healthy individuals. Compr. Psychiatry 2014, 55, 1269–1278. [Google Scholar] [CrossRef]
- Crescentini, C.; Matiz, A.; Fabbro, F. Improving personality/character traits in individuals with alcohol dependence: The influence of mindfulness-oriented meditation. J. Addict. Dis. 2015, 34, 75–87. [Google Scholar] [CrossRef]
- Crescentini, C.; Menghini, D. La Mindfulness per l’ADHD e i Disturbi del Neurosviluppo. Applicazione Clinica Della Meditazione Orientata alla Mindfulness—MOM; Centro Studi Erickson: Trento, Italy, 2019. [Google Scholar]
- MacCoon, D.G.; Imel, Z.E.; Rosenkranz, M.A.; Sheftel, J.G.; Weng, H.Y.; Sullivan, J.C.; Lutz, A. The validation of an active control intervention for mindfulness based stress reduction (MBSR). Behav. Res. 2012, 50, 3–12. [Google Scholar] [CrossRef] [Green Version]
- Corallo, R. Sei Folletti Nel Mio Cuore (Six Pixies in My Heart); Centro Studi Erickson: Trento, Italy, 2011. [Google Scholar]
- Conners, C.K.; MHS Staff. Conners’ Continuous Performance Test-II 5th Version (CPT-II V.5). Technical Guide and Software Manual; Multi Health System: North Tonawanda, NY, USA, 2004. [Google Scholar]
- Golden, C.J.; Freshwater, S.M. The Stroop Color and Word Test: A Manual for Clinical and Experimental Uses; Stoelting: Chicago, IL, USA, 2002. [Google Scholar]
- Townsend, J.T.; Ashby, F.G. Methods of modeling capacity in simple processing systems. In Cognitive Theory; Castellan, J.N.J., Restle, F., Eds.; Lawrence Erlbaum Associates: New York, NY, USA, 1978; Volume 3, pp. 199–239. [Google Scholar]
- Logan, G.D.; Cowan, W.B. On the ability to inhibit thought and action: A theory of an act of control. Psychol. Rev. 1984, 91, 295–327. [Google Scholar] [CrossRef]
- Marcos, E.; Pani, P.; Brunamonti, E.; Deco, G.; Ferraina, S.; Verschure, P. Neural variability in premotor cortex is modulated by trial history and predicts behavioral performance. Neuron 2013, 78, 249–255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pani, P.; Menghini, D.; Napolitano, C.; Calcagni, M.; Armando, M.; Sergeant, J.A.; Vicari, S. Proactive and reactive control of movement are differently affected in attention deficit hyperactivity disorder children. Res. Dev. Disabil. 2013, 34, 3104–3111. [Google Scholar] [CrossRef] [PubMed]
- Menghini, D.; Armando, M.; Calcagni, M.; Napolitano, C.; Pasqualetti, P.; Sergeant, J.A.; Pani, P.; Vicari, S. The influence of generalized anxiety disorder on executive functions in children with ADHD. Eur. Arch. Psychiatry Clin. Neurosci. 2017, 268, 349–357. [Google Scholar] [CrossRef] [PubMed]
- Conners, C.K. Conners’ Rating Scales–Revised; (Italian adaptation); Giunti, O.S., Ed.; Organizzazioni Speciali: Firenze, Italy, 1997. [Google Scholar]
- Achenbach, T.M.; Rescorla, L.A. Manual for the ASEBA School-Age Forms and Profiles; University of Vermont, Research Center for Children, Youth and Families: Burlington, VT, USA, 2001. [Google Scholar]
- March, J.S.; Parker, J.D.A.; Sullivan, K.; Stallings, P.; Conners, C.K. The Multidimensional Anxiety Scale for Children (MASC): Factor structure, reliability, and validity. J. Am. Acad. Child Adolesc. Psychiatry 1997, 36, 554–565. [Google Scholar] [CrossRef]
- Kovacs, M. Children’s Depression Inventory—CDI; (Italian Adaptation); Giunti, O.S., Ed.; Organizzazioni Speciali: Firenze, Italy, 1982. [Google Scholar]
- Greco, L.A.; Baer, R.A.; Smith, G.T. Assessing mindfulness in children and adolescents: Development and validation of the child and adolescent mindfulness measure (CAMM). Psychol. Assess 2011, 23, 606–614. [Google Scholar] [CrossRef]
- Abidin, R.R. The Parenting Stress Index-Short Form. Test Manual Pediatric; Psychology Press: Charlottesville, VA, USA, 1990. [Google Scholar]
- Abidin, R.R. Parenting Stress Index: Professional Manual, 3rd ed.; Psychological Assessment Resources: Odessa, FL, USA, 1995. [Google Scholar]
- Guarino, A.; Di Blasio, P.; D’Alessio, M.; Camisasca, E.; Serantoni, G. Parenting Stress Index—Short Form; Giunti, O.S., Ed.; Organizzazioni Speciali: Firenze, Italy, 2008. [Google Scholar]
- Cornoldi, C.; Colpo, G. Prove di Lettura MT-2 per la Scuola Primaria; Giunti, O.S., Ed.; Organizzazioni Speciali: Firenze, Italy, 2007. [Google Scholar]
- Biancardi, A.; Nicoletti, C. Batteria per la Discalculia Evolutiva (BDE); Edizioni Omega: Torino, Italy, 2004. [Google Scholar]
- Cornoldi, C.; Lucangeli, D.; Bellina, M. Test AC-MC 6-11. Test di Valutazione delle Abilità di Calcolo; Centro Studi Erickson: Trento, Italy, 2012. [Google Scholar]
- Holas, P.; Jankowski, T. A cognitive perspective on mindfulness. Int. J. Psychol. 2013, 48, 232–243. [Google Scholar] [CrossRef]
- Chambers, R.; Lo, B.C.L.; Allen, N.B. The impact of intensive mindfulness training on attentional control, cognitive style, and affect. Cogn. Res. 2008, 32, 303–322. [Google Scholar] [CrossRef]
- Lyvers, M.; Makin, C.; Toms, E.; Thorberg, F.A.; Samios, C. Trait mindfulness in relation to emotional self-regulation and executive function. Mindfulness 2014, 5, 619–625. [Google Scholar] [CrossRef]
- Oberle, E.; Kimberly, A.S.C.; Molly, S.; Kimberly, C.T. Mindfulness and inhibitory control in early adolescence. J. Early Adolesc. 2012, 32, 565–588. [Google Scholar] [CrossRef]
- Riggs, N.R.; Black, D.S.; Ritt-Olson, A. Associations between dispositional mindfulness and executive function in early adolescence. J. Child Fam. Stud. 2015, 24, 2745–2751. [Google Scholar] [CrossRef]
- Quach, D.; Mano, K.E.J.; Alexander, K. A randomized controlled trial examining the effect of mindfulness meditation on working memory capacity in adolescents. J. Adolesc. Health. 2016, 58, 489–496. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gallant, S.N. Mindfulness meditation practice and executive functioning: Breaking down the benefit. Conscious Cogn. 2016, 40, 116–130. [Google Scholar] [CrossRef] [PubMed]
- Xue, J.; Zhang, Y.; Huang, Y. A meta-analytic investigation of the impact of mindfulness-based interventions on ADHD symptoms. Medicine 2019, 98, e15957. [Google Scholar] [CrossRef]
- Van de Weijer-Bergsma, E.; Formsma, A.R.; de Bruin, E.I.; Bogels, S.M. The effectiveness of mindfulness training on behavioral problems and attentional functioning in adolescents with ADHD. J. Child Fam. Stud. 2012, 21, 775–787. [Google Scholar] [CrossRef] [Green Version]
- Van der Oord, S.; Bögels, S.M.; Peijnenburg, D. The effectiveness of mindfulness training for children with ADHD and mindful parenting for their parents. J. Child Fam. Stud. 2012, 21, 139–147. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| MOM G | EEP G | ||
|---|---|---|---|
| Neuropsychological Measure | Time | M (SD) | M (SD) |
| CPT-II HRT (msec) | T0 | 505.39 (73.00) | 445.37 (75.98) |
| T1 | 431.33 (52.26) | 428.21 (45.08) | |
| CPT-II HRT-SD (msec) | T0 | 348.23 (89.39) | 238.76 (94.94) |
| T1 | 222.12 (93.04) | 239.97 (65.26) | |
| STROOP IES (msec/errors) | T0 | 115.48 (47.86) | 110.76 (57.90) |
| T1 | 96.62 (41.91) | 107.26 (35.12) | |
| SSRT (msec) | T0 | 347.24 (190.72) | 279.62 (106.35) |
| T1 | 319.74 (62.14) | 271.39 (62.94) | |
| N-BACK II (% of errors) | T0 | 55.67 (23.65) | 36.40 (16.97) |
| T1 | 48.93 (14.31) | 45.50 (15.45) |
| MOM G | EEP G | ||
|---|---|---|---|
| CPRS-R:L Subscale | Time | T-Score M (SD) | T-Score M (SD) |
| Oppositional | T0 | 64.13 (14.58) | 67.90 (12.64) |
| T1 | 56.47 (10.64) b | 68.90 (14.16) | |
| Cognitive Problems/Inattention | T0 | 76.80 (12.45) | 86.20 (11.00) |
| T1 | 75.00 (11.85) | 84.00 (14.37) | |
| Hyperactivity | T0 | 69.80 (14.51) | 81.00 (12.02) |
| T1 | 62.13 (10.98) | 79.00 (13.22) | |
| Anxious-Shy | T0 | 53.40 (13.89) | 54.20 (13.07) |
| T1 | 49.73 (11.50) | 56.80 (12.85) | |
| Perfectionism | T0 | 51.93 (9.25) | 50.10 (8.37) |
| T1 | 43.47 (7.08) | 50.80 (7.54) | |
| Social Problems | T0 | 63.40 (16.05) | 64.80 (19.36) |
| T1 | 65.80 (14.63) | 61.50 (15.09) | |
| Psychosomatic Problems | T0 | 55.93 (19.64) | 60.80 (16.10) |
| T1 | 48.93 (13.62) | 64.90 (16.94) | |
| ADHD Index | T0 | 78.80 (12.70) | 83.80 (6.73) |
| T1 | 71.47 (10.13) | 80.50 (14.42) | |
| CGI Restless-Impulsive | T0 | 73.47 (14.29) | 76.90 (9.42) |
| T1 | 63.93 (10.12) a,b | 79.60 (11.17) | |
| CGI Emotional Lability | T0 | 56.20 (14.66) | 67.10 (12.74) |
| T1 | 48.73 (8.94) | 67.80 (17.67) | |
| CGI Total | T0 | 70.40 (14.83) | 76.70 (9.92) |
| T1 | 60.53 (9.88) a,b | 78.80 (13.20) | |
| DSM-IV Inattentive | T0 | 78.66 (12.02) | 84.60 (10.69) |
| T1 | 74.80 (12.04) | 84.20 (14.57) | |
| DSM-IV Hyperactive/Impulsive | T0 | 70.00 (12.45) | 77.10 (9.47) |
| T1 | 63.13 (10.49) b | 75.20 (14.77) | |
| DSM-IV Total | T0 | 77.07 (12.65) | 84.30 (9.94) |
| T1 | 71.47 (10.53) | 82.50 (14.76) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santonastaso, O.; Zaccari, V.; Crescentini, C.; Fabbro, F.; Capurso, V.; Vicari, S.; Menghini, D. Clinical Application of Mindfulness-Oriented Meditation: A Preliminary Study in Children with ADHD. Int. J. Environ. Res. Public Health 2020, 17, 6916. https://doi.org/10.3390/ijerph17186916
Santonastaso O, Zaccari V, Crescentini C, Fabbro F, Capurso V, Vicari S, Menghini D. Clinical Application of Mindfulness-Oriented Meditation: A Preliminary Study in Children with ADHD. International Journal of Environmental Research and Public Health. 2020; 17(18):6916. https://doi.org/10.3390/ijerph17186916
Chicago/Turabian StyleSantonastaso, Ornella, Vittoria Zaccari, Cristiano Crescentini, Franco Fabbro, Viviana Capurso, Stefano Vicari, and Deny Menghini. 2020. "Clinical Application of Mindfulness-Oriented Meditation: A Preliminary Study in Children with ADHD" International Journal of Environmental Research and Public Health 17, no. 18: 6916. https://doi.org/10.3390/ijerph17186916