
Abstract
Patient-reported outcome (PRO) is included in the remission criteria of rheumatoid arthritis (RA). We aimed to determine the effect of age on PRO and the subsequent achievement of clinical and functional RA remission criteria. Three hundred and one patients with non-rheumatic diseases were evaluated using the 0–10 cm visual analog scale (VAS) assessment for musculoskeletal symptoms and a functional health assessment questionnaire-disability index (HAQ-DI). These assessments were compared with those obtained from 149 patients with RA with negative tender/swollen joint counts and normal serum C-reactive levels (objective clinical remission). Of the 301 patients, 32.2%, 26.6%, and 41.2% were classified as non-elderly (< 65 years), early elderly (65–74 years), and late-elderly (≥ 75 years) patients, respectively. VAS > 1 cm and HAQ-DI ≥ 0.5 were observed in 7.3% and 14.5%, respectively, in late-elderly patients, whereas ≤ 1.0% of non-elderly and early elderly patients for the both. Among 149 RA patients in objective remission, however, > 20% and > 10% of early elderly patients (and even non-elderly patients) had VAS > 1 cm and HAQ-DI ≥ 0.5, respectively, and 34.0% and 35.8% of late-elderly patients with RA had VAS > 1 cm and HAQ-DI ≥ 0.5, respectively. Multivariate logistic analysis revealed that age and RA were associated with the non-achievement of VAS ≤ 1 cm and HAQ-DI < 0.5. Therefore, the effect of age, which was independent of the presence of RA even without any objective disease activity, on PRO and the non-achievement of clinical and functional remission criteria was demonstrated.
Similar content being viewed by others

Introduction
Patient-reported outcome (PRO) is an important clinical measure of rheumatoid arthritis (RA) disease activity, which is characterized by persistent and eventually destructive polyarthritis1,2. However, PRO measures such as the global assessment of disease activity in which the patient uses a 10-cm (100-mm) visual analog scale (VAS) may be influenced by factors other than RA disease activity such as joint damage, osteoarthritis, and psychological distress3. Patient VAS has often been reported to be a limiting factor for reaching remission4. Even for subjective symptoms of individual joints, the concordance of joint symptoms determined by ultrasound-defined synovitis was more limited than joint swelling determined by rheumatologists5, although the assessment of joint symptoms by patients themselves was sensitive, and, thus, may be useful as a screening tool for the presence of arthritis.
The above mentioned strengths and weaknesses of PRO have effects on designating the clinical remission of RA, which has been defined by the American College of Rheumatology (ACR)/The European League Against Rheumatism (EULAR). Remission criteria, whether using the Boolean-based or composite measure simplified disease activity index (SDAI) score, are composed of the following components: tender joint count (TJC), swollen joint count (SJC), patient VAS, serum C-reactive protein (CRP) levels and, in addition, a physician’s global assessment of disease activity using SDAI scores alone6. We have recently reported that ~ 50% of patients with RA achieved clinical remission as defined by the SDAI scores, and that advanced age negatively affected remission achievement irrespective of objective findings such as inflammatory joint counts7. However, a study that only included patients with RA may not be sufficient for determining the effect of age on PRO in RA. A previous report8 suggested that the majority of individuals above 50 years of age did not meet the previous version of ACR remission criteria9. The patients’ age was shown to be an important factor affecting the health assessment questionnaire-disability index (HAQ-DI) and patient VAS scores10,11. Therefore, we conducted a cross-sectional study comparing 301 patients without defined rheumatic disease with RA patients with negative joint counts and normal serum CRP levels experiencing “objective” clinical remission to further delineate the relevance of age on PRO measures such as patient VAS and HAQ-DI scores.
Results
Patient characteristics
Of the 301 patients without rheumatic diseases involved in the study, 54.8% were female (Table 1). The median age of the group that did not have rheumatic disease was 70 years, and the proportion of non-elderly (< 65 years), early elderly (65–74 years), and late-elderly (≥ 75 years) were 32.2%, 26.6%, and 41.2%, respectively. Major diagnoses of non-rheumatic diseases of the group included hypertension (40.2%), cervical atherosclerosis (25.2%), chronic gastritis (54.5%), and hyperlipidemia (48.2%).
Of the 304 patients with RA considered, 149 (49.0%) had no tender or swollen joints and normal serum CRP values (≤ 0.3 mg/dl), namely “objective clinical remission”. Of these, 73.8% were women (Supplementary Table 1). The median age of the patients with RA having negative joint counts and normal CRP values was 72 years, and the rates of non-elderly (< 65 years), early elderly (65–74 years), and late-elderly (≥ 75 years) were 32.2%, 32.2%, and 35.6%, respectively. Therefore, patients with RA had a comparable age distribution to that of non-rheumatic patients, although predominance of women patients was observed in patients with RA, as expected. Compared with the remaining patients with RA, those with negative joint counts and normal CRP possessed a lower level of radiographic damage, were less frequently seropositive for rheumatoid factor (RF) and anti-cyclic citrullinated peptide antibody (anti-CCP), and reported less usage of biologic disease-modifying antirheumatic drugs (bDMARDs) and glucocorticoids. Sex, age distribution, and methotrexate (MTX) administration were comparable between the two groups. As expected, subjective and composite remission rates defined by patient VAS ≤ 1 cm, HAQ-DI < 0.5, SDAI ≤ 3.3, and Boolean-based remission were greater in patients with RA with negative joint counts and normal CRP values than the remaining patients with RA (71.8% vs 29.2%, p < 0.0001; 78.5% vs 45.8%, p < 0.0001; 83.9% vs 16.8%, p < 0.0001; and 71.8% vs 16.1%, p < 0.0001; respectively).
Comparison of the non-achievement rates of subjective clinical or functional remission among the different age groups between non-rheumatic patients and patients with RA in “objective clinical remission”
Rates of patient VAS > 1 cm and HAQ-DI ≥ 0.5 among the non-elderly, early elderly, and late-elderly patients without rheumatic diseases were compared with those of patients with RA in “objective clinical remission.” Notably, subjective non-achievement of remission criteria was almost exclusively observed in the late-elderly patients: 7.3% for patient VAS > 1 cm and 14.5% for HAQ-DI ≥ 0.5 (0.0–1.0% in non-elderly and early elderly patients, Table 2). In contrast to the above findings, > 20% and > 10% of patients with RA with negative joint counts and normal CRP values did not meet the patient VAS ≤ 1 cm and HAQ-DI < 0.5 criteria, respectively, even in patients aged < 75 years (early elderly or non-elderly). Furthermore, 34.0% and 35.8% of late-elderly patients with RA had VAS > 1 cm and HAQ-DI ≥ 0.5, respectively, despite “objective clinical remission.” Therefore, it was demonstrated that a considerable portion of RA patients had subjective/functional disturbance even in the absence of objective findings.
Multivariate analysis of factors associated with the non-achievement of subjective remission within a combined population of non-rheumatic and patients with RA in the absence of objective findings
In order to evaluate whether age, sex, and the presence of RA is associated with the non-achievement of subjective clinical or functional remission, we combined the data from non-rheumatic patients and patients with RA with negative joint counts and normal CRP. Age showed marginal and significant impacts on non-achievement of VAS ≤ 1 cm (15.3% in late-elderly vs 9.2% in others; p = 0.051) and HAQ-DI < 0.5 (20.9% in late-elderly vs 4.8% in others; p < 0.0001), respectively. Sex was associated with HAQ-DI scores that were ≥ 0.5 (14.9% in female vs 5.1% in male patients; p = 0.0011), but not with patient VAS > 1 cm (13.5% vs 8.6%, respectively; p = 0.13). The presence of RA, even without objective findings, was significantly associated with patient VAS > 1 cm (28.2% in patients with RA without objective findings vs 3.3% in non-rheumatic patients; p < 0.0001) and HAQ-DI ≥ 0.5 (21.5% vs 6.0%, respectively; p < 0.0001). Because sex and RA are confounding (Table 1; Supplementary Table 1), a multivariate logistic analysis was subsequently performed to clarify the effects of the above parameters on the non-achievement of patient VAS ≤ 1 cm and HAQ-DI < 0.5 (Table 3). We confirmed that age and the presence of RA were significantly associated with the non-achievement of patient VAS ≤ 1 cm and HAQ-DI < 0.5, and that sex (female) was significantly associated with the non-achievement of HAQ-DI < 0.5.
Discussion
To the best of our knowledge, this is the first study that examined patient VAS values and HAQ-DI scores with respect to musculoskeletal symptoms in 301 patients without rheumatic disease to compare them with those from patients with RA lacking any objective findings such as tender/swollen joints or elevated serum CRP values. In this study, we demonstrated that advanced age clearly affected the achievement of RA remission criteria irrespective of the presence of RA. Therefore, current assessments of subjective disease activity and functional state by patient VAS and HAQ-DI may not be effective in late-elderly patients. Moreover, the presence of RA itself, without any objective disease activity, was associated with worsened patient VAS and HAQ-DI scores.
It should be noted that the age distribution for patients with RA with negative joint counts and normal CRP values and remaining patients with RA examined were similar (Table 2), while radiographic damage and seropositivity, both of which are poor prognostic factors of RA12, were significantly different between the two groups (Supplementary Table 1). Thus, the effect of advanced age on the achievement of RA remission criteria is largely subjective, as indicated previously7, and this fact is likely to be related to differences between patient VAS and physician (evaluator) VAS scores4,13. The effect of age on RA outcome has previously been identified in a cohort of patients with early RA, the ESPOIR cohort (the French multicenter prospective cohort of patients with early arthritis)14. Additionally, it is important to note the difficulty in meeting RA remission criteria for patients in a general population of elderly individuals without rheumatic diseases8, as well in patients with RA associated with comorbidities15,16,17. Therefore, the inclusion of PRO in RA disease activity measures and corresponding remission criteria can be reconsidered in the future, as its usefulness for evaluating advanced-aged patients is diminished relative to younger ones18,19,20,21.
The effect of sex on HAQ-DI but not on patient VAS in this study may be an issue requiring investigation in the future. In a separate analysis of non-rheumatic and patients with RA, patient VAS > 1 cm was observed in 3.7% of male and 3.0% of female non-rheumatic patients (p = 0.76) and in 25.6% of male and 29.1% of female patients with RA (p = 0.84), while HAQ-DI ≥ 0.5 was observed in 3.7% of male and 7.9% of female non-rheumatic patients (p = 0.15) and in 10.3% of male and 25.5% of female RA patients (p = 0.068).
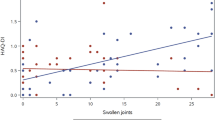
In this study, patients without rheumatic diseases completed a single global assessment of musculoskeletal symptoms (patient VAS for non-rheumatic patients), while patients with RA completed a global assessment of disease activity (patient VAS for RA patients) and a global assessment of pain (pain VAS). As expected, the pain VAS and patient VAS were strongly correlated (r2 = 0.843, p < 0.0001) even among RA patients in objective clinical remission. Therefore, our results indicate that a considerable portion of people aged ≥ 75 years without any diagnosis of rheumatic diseases suffer from musculoskeletal pain.
The limitations of our study are that the suitability of patient VAS for patients without rheumatic diseases is unknown, and the lack of CRP and radiographic joint evaluation data of those patients.
In conclusion, we clarified the importance of advanced age, which was independent of the presence of RA even without any objective disease activity, on PRO such as patient VAS and HAQ-DI scores, which should be increasingly important as human global populations are rapidly ageing.
Methods
Patients
Patients without rheumatic disease who visited a general medical clinic (Aoki Clinic) between September 2017 and December 2018 were considered. The patients gave informed consent and received a systemic, 68-joint examination to confirm the absence of an active rheumatic disease such as RA. All patients (n = 302) visiting between this time period except one, who had active arthritis, were enrolled in the study.
As a disease control, patients with RA (n = 149) with neither tender nor swollen joints and with normal serum CRP values (≤ 0.3 mg/dl), characteristics of “objective clinical remission,” were selected from the data of 304 patients with RA obtained from the Toho University Ohashi Medical Center between May 2014 and March 20157. All patients met the ACR 1987 revised criteria22 and/or the ACR/EULAR 2010 classification criteria23 for RA.
The study protocol was approved by the Ethics Committee of Toho University Ohashi Medical Center (project approval number: H17028). All methods were performed in accordance with the Declaration of Helsinki and other relevant guidelines and regulations.
Clinical assessments
Patients without rheumatic diseases completed a global assessment (0–10 cm visual analog scale) of musculoskeletal symptoms (patient VAS for non-rheumatic patients) and an HAQ-DI functional assessment. We obtained the following medical information from the medical records of non-rheumatic patients: age, sex, and disease diagnosis. For RA patients, records of age, sex, disease duration from the onset of symptoms to study enrolment, radiographic stage, global assessment of disease activity as measured by a 10-cm patient VAS, HAQ-DI, physician-based assessments of the presence of tenderness and swelling in 68 and 66 joints, respectively, serum levels of CRP, rheumatoid factor (RF), anti-cyclic citrullinated peptide antibody (anti-CCP), and treatment regimens were obtained. Physician-based assessment of the presence of tenderness and swelling in 68 and 66 joints, respectively, was used to screen to exclude patients demonstrating active rheumatic diseases such as RA and osteoarthritis from the patient group that did not have rheumatic disease.
Statistical analysis
Statistical analysis was performed using JMP Pro (version 14.2.0, SAS Institute Japan Ltd. Tokyo, Japan). Continuous variables were summarized using the median and interquartile range (IQR) and were analyzed using the Mann–Whitney U test or the Kruskal–Wallis test. Binominal data between two or three groups were evaluated using Pearson’s chi-square test, and Fisher’s exact test was used where appropriate. A multivariate logistic regression analysis was performed to examine the conditional effects of clinical parameters on the achievement of patient VAS ≤ 1 cm or HAQ-DI < 0.5. p values < 0.05 were considered statistically significant.
Data availability
The datasets generated during the current study are available from the corresponding author on reasonable request.
References
van Tuyl, L. H. D. & Michaud, K. Patient-reported outcomes in rheumatoid arthritis. Rheum. Dis. Clin. North Am. 42, 219–237 (2016).
Felson, D. T. et al. The American College of Rheumatology preliminary core set of disease activity measures for rheumatoid arthritis clinical trials. Arthritis Rheum. 36, 729–740 (1993).
Nikiphorou, E. et al. Patient global assessment in measuring disease activity in rheumatoid arthritis: a review of the literature. Arthritis Res. Ther. 18, 251 (2016).
Studenic, P., Smolen, J. S. & Aletaha, D. Near remission of ACR/EULAR criteria for remission: effects of patient global assessment in Boolean and index-based definitions. Ann. Rheum. Dis. 71, 1702–1705 (2012).
Hirata, A. et al. Concordance between patient-reported joint symptoms, physician-examined arthritic signs and ultrasound-detected synovitis in rheumatoid arthritis. Arthritis Care Res. (Hoboken) 69, 801–806 (2017).
Felson, D. T. et al. American College of Rheumatology/European League Against Rheumatism provisional definition of remission in rheumatoid arthritis for clinical trials. Ann. Rheum. Dis. 70, 404–413 (2011).
Ito, H. et al. Global assessments of disease activity are age-dependent determinant factors of clinical remission in rheumatoid arthritis. Semin. Arthritis Rheum. 47, 310–314 (2017).
Sokka, T., Mäkinen, H., Hannonen, P. & Pincus, T. Most people over age 50 in the general population do not meet ACR remission criteria or OMERACT minimal disease activity criteria for rheumatoid arthritis. Rheumatology 46, 1020–1023 (2007).
Pinals, R. S., Masi, A. T., Larsen, R. A. & The Subcommittee for Criteria of Remission in Rheumatoid Arthritis of the American Rheumatism Association Diagnostic and Therapeutic Criteria Committee. Preliminary criteria for clinical remission in rheumatoid arthritis. Arthritis Rheum. 24, 1308–1315 (1981).
Krishnan, E., Sokka, T., Häkkinen, A., Hnbert, H. & Hannonen, P. Normative values for the health assessment questionnaire disability index. Benchmarking disability in the general population. Arthritis Rheum. 50, 953–960 (2004).
Krishnan, E., Häkkinen, A., Sokka, T. & Hannonen, P. Impact of age and comorbidities on the criteria for remission and response in rheumatoid arthritis. Ann Rheum. Dis. 64, 1350–1352 (2005).
Smolen, J. S. et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2016 update. Ann. Rheum. Dis. 76, 960–977 (2017).
Kaneko, Y., Kuwana, M., Kondo, H. & Takeuchi, T. Discordance in global assessments between patient and estimator in patients with newly diagnosed rheumatoid arthritis: associations with progressive joint destruction and functional impairment. J. Rheumatol. 41, 1061–1066 (2014).
Krams, T. et al. Effect of age at rheumatoid arthritis onset on clinical, radiographic, and functional outcomes: the ESPOIR cohort. Joint Bone Spine 83, 511–515 (2016).
Masri, K. R. et al. Validity and reliability problem with patient global as a component of the ACR/EULAR remission criteria as used in clinical practice. J. Rheumatol. 39, 1139–1145 (2012).
Thiele, K. et al. Performance of the 2011 ACR/EULAR preliminary remission criteria compared with DAS28 remission in unselected patients with rheumatoid arthritis. Ann. Rheum. Dis. 72, 1194–1199 (2013).
Ranganath, V. K. et al. Comorbidities are associated with poorer outcomes in community patients with rheumatoid arthritis. Rheumatology 52, 1809–1817 (2013).
van der Heijde, D. M. et al. Judging disease activity in clinical practice in rheumatoid arthritis: first step in the development of a disease activity score. Ann. Rheum. Dis. 49, 916–920 (1990).
Prevoo, M. L. et al. Modified disease activity scores that include twenty-eight-joint counts: development and validation in a prospective longitudinal study of patients with rheumatoid arthritis. Arthritis Rheum. 38, 44–48 (1995).
Smolen, J. S. et al. A simplified disease activity index for rheumatoid arthritis for use in clinical practice. Rheumatology 42, 244–257 (2003).
Kameda, H. et al. Development and validation of the handy rheumatoid activity score with 38 joints (HRAS38) for rheumatoid arthritis in patients receiving infliximab. Mod. Rheumatol. 16, 381–388 (2006).
Arnett, F. C. et al. The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis Rheum. 31, 315–324 (1988).
Aletaha, D. et al. 2010 Rheumatoid arthritis classification criteria: an American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheum. 62, 2569–2581 (2010).
Acknowledgements
The authors thank Editage Japan for the editing this manuscript.
Author information
Authors and Affiliations
Contributions
T.A. collected the data from non-rheumatic patients and wrote the draft. H.I. and A.H. collected the data from RA patients. T.O. and Y.N. performed the statistical analyses. H.K. designed the study. All authors reviewed and approved the manuscript.
Corresponding author
Ethics declarations
Competing interests
This work was partly supported by JSPS KAKENHI Grant Number JP15K09535, Health and Labor Sciences Research Grants for research on intractable diseases (The Research Team for Autoimmune Diseases) from the Ministry of Health, Labor and Welfare of Japan for H. K. H. K. has received consulting fees, speaking fees, and/or honoraria from AbbVie G.K., Asahi Kasei Pharma, Astellas Pharma, Bristol-Myers Squibb, Chugai Pharmaceutical Co., Ltd., Eisai Co. Ltd., Eli Lilly Japan K.K., Gilead Sciences, Janssen Pharmaceutical K.K., Mitsubishi Tanabe Pharma, Novartis Pharma K.K., and Sanofi Pharma, and has received research grants from AbbVie G.K., Asahi Kasei Pharma, Astellas Pharma Inc., Chugai Pharmaceutical Co., Ltd., Eisai Co., Ltd., Mitsubishi Tanabe Pharma, Novartis Pharma K.K. and Sanofi Pharma. T. A., H. I., T. O., A. H. and Y. N. declare no potential conflict of interest.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Aoki, T., Ito, H., Ogura, T. et al. Association of age with the non-achievement of clinical and functional remission in rheumatoid arthritis. Sci Rep 10, 15277 (2020). https://doi.org/10.1038/s41598-020-72274-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-020-72274-2
This article is cited by
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
