Article Text

Abstract
Purpose We performed a systematic review and meta-analysis to summarise the geographic distribution of age-related macular degeneration (AMD) incidence.
Methods Databases including PubMed, Embase and Web of Science were searched for publications of early and late AMD before September 2019. Studies were included if they applied a standardised photographic assessment and classification system. The proportion of participants with AMD in each eligible study was combined to obtain a pooled incidence from all studies using a random effects model. We also assessed sources of potential heterogeneity in the incidence of AMD using meta-regression analyses for both late and early AMD.
Results Twenty-four population-based studies (70 123 individuals aged 55 years or older) were included in the meta-analysis. The pooled global annual incidences of early and late AMD were 1.59% (95% CI 1.12% to 2.10%) and 0.19% (95% CI: 0.13% to 0.28%), respectively. Individuals of European descent had the highest annual incidence of both early (2.73%, 95% CI 1.63% to 4.57%) and late (0.36%, 95% CI 0.17% to 0.75%) AMD than other ethnic groups. Average age (p=0.001) at baseline, ethnicity (p=0.001), region (p=0.043) and gender (p=0.011) were predictors for incident late AMD, while only average age (p=0.01) at baseline and ethnicity (p=0.025) was associated with incidence of early AMD.
Conclusions This meta-analysis offers an up-to-date overview of AMD globally, which may provide scientific guidance for the design and implementation of public health strategies such as screening programmes for AMD in both specific geographic locations and ethnic groups, as well as worldwide.
- Epidemiology
Statistics from Altmetric.com
INTRODUCTION
Age-related macular degeneration (AMD) is a leading cause of visual impairment and blindness throughout the world.1–3 It is estimated that the number of AMD patients may increase from 9.1 million in 2010 to 17.8 million in 2050 across all scenarios.4 Although the anti-vascular endothelial growth factor (anti-VEGF) injection treatments have ushered in a new era of the clinical treatment of retinal diseases including AMD,5 its promotion is limited by its substantial economic burden, especially in countries and areas of low socioeconomic status.6 Thus, it is important to reduce the burden of visual impairment and blindness caused by AMD from a public health perspective.
While a number of reports have systematically reviewed the prevalence of AMD throughout the world,7–10 few have focused on the incidence. In epidemiology, while prevalence measures the proportion of diseases in a specific group, incidence is another important index which reflect the speed of disease development. Despite the incidence of AMD has been systematically reviewed in western countries and in whites where AMD is considered to be prevalent,11 little is known in other parts of the world and in other ethnic groups such as Asians. Recent evidence has suggested that the prevalence of AMD is about 10% in older Asians such as Chinese, which is comparable to that of whites.12 Therefore, understanding the geographic patterns and distributions of AMD incidence are crucial for clinical management and health resource allocations from a global perspective.
To address this gap, we conducted a systematic review and meta-analysis of published literature to summarise the global incidence of AMD and describe the differences by time periods, regions and study characteristics. The findings would provide valuable information towards designing and implementing eye-care strategies as well as public health measures throughout the world.
METHODS
Our systematic review was performed based on the Meta-analysis Of Observational Studies in Epidemiology (MOOSE) guidelines13 and the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) guidelines.14
Search strategy
We searched PubMed, Web of Science, and Embase for pertinent publications before September 2019. A combination of subject words and random words related to AMD and incidence constitutes the search strategy. Full search terms used for PubMed were presented as follows: ((‘age-related macular degeneration’ [All Fields] OR ‘age related macular degeneration’ [All Fields] OR ‘age-related maculopathy’ [All Fields] OR ‘age related maculopathy’ [All Fields] OR ‘macular degeneration’ [All Fields]) AND (‘incidence’ [Title/Abstract] OR ‘epidemiology’ [Title/Abstract])). The strategy identified total articles cited in previous reviews.7 8 References of identified reports were also searched manually in order to avoid missing potentially relevant studies. Publications on incidence were independently searched and scanned by two authors (MZ and PCD). Any disagreement was resolved through discussion.
Eligibility criteria
Studies were included if they were original research reports describing the incidence of AMD (including early, late and/or any AMD). Additional full-text reviews were included if they: (1) were population-based study conducted from a non-diseased condition whether in only one or both eyes at baseline; (2) reported at least a follow-up duration of 2 years with a follow-up rate of being at least 50%; (3) had a standardised classification system (either the Wisconsin age-related maculopathy grading system,15 the international classification for AMD,16 or other study-specific classification system); (4) used a standardised photographic assessment of AMD; (5) clearly described geographic area and year of survey; (6) were published in English language only; (7) included at least 100 participants at baseline.
Studies were excluded if they: (1) were not population-based (hospital audits, surveys or clinics); (2) included non-specific volunteers or particular professions with the exception of a study of American watermen17; (3) only carried out physical examination by funduscope or slit lamp for AMD diagnosis or made self-reported diagnoses; (4) performed ocular fundus examinations only in those with vision impairment (as they may represent a subgroup with disease); (5) did not report original data (eg, reviews, editorials); (6) recorded the number of eyes with AMD rather than the number of individuals.
AMD grading
On account of the Wisconsin Age-Related Maculopathy Grading System and International Classification System, early AMD was defined as the presence of large indistinct soft drusen, reticular drusen or the copresence of large distinct soft drusen and retinal pigmentary abnormalities (hyperpigmentation or depigmentation of retinal pigment epithelial cells) within the macula, in the absence of any late AMD lesions. Late AMD was defined as the presence of neovascular AMD, indicated by retinal pigment epithelial or neurosensory subretinal detachment, retinal or subretinal haemorrhage, subretinal fibrosis or old atrophic disciform scars, or photocoagulation scars with a history of neovascular AMD, or the presence of pure geographic atrophy within the macula, as described in the International Age-Related Maculopathy Classification.
Data collection and risk of bias assessment
The following information was collected from each eligible study in the analysis: geographic location, study name, first author, publication year, age range, ethnicity, follow-up duration, response rate, definition of AMD, sample size, year of baseline exam, annual incidence rates of early or late AMD cases, or both. Based on the classification of United Nations Population Division (2011), regions were divided into Asia, North America, Europe, Africa, Oceania and Latin America & Caribbean.
A modified edition of the risk of bias tool developed by Hoy and colleagues18 was employed in assessing the quality of the eligible studies (table 1). The areas assessed included seven items including study setting, study design, response rate, ascertainment of AMD, exclusion of prevalent AMD, sex subgroups and severity of incident cases. High risk, and unclear were scored as ‘1’, while low risk was scored as ‘0’ for each item. We have present risk of bias and quality scores in table 2. Based on the whole score, the study was classified as having a lower bias risk (score 0–2), a moderate bias risk (score 3–4) or a higher bias risk (score ≥5).
Studies of early and late age-related macular degeneration incidence
Risk of bias items assessed in the included studies
Considering changes in treatment strategies and efforts of public health since 2000, studies in our analysis were layered by the year of follow-up exam (before 2000 vs after 2000) to make comparisons and conclusions more credible.
Statistical analyses
Incidence was calculated as annual incidence, using the formula – ln(1−S)/t,42 where S is the cumulative incidence over t years and t is the duration of follow-up. Information on annual incidence by study location, course of AMD, photographic assessment, grading system, follow-up duration and year of baseline exam was assessed and compared. The proportion of participants with AMD in each eligible study was fully combined to obtain a pooled incidence from all studies using a random effect model. We also estimated the impact of seven categorical covariates for incidence using meta-regression analyses for both late and early AMD, including average age at baseline, ratio of sex-specific incidence, region, ethnicity, publication year, follow-up duration and classification system. The extent of heterogeneity among different studies was quantified using the I2 statistics.43 An I2 value of more than 50% or a p value of less than 0.10 denotes a significant degree of heterogeneity. The 95% CIs of incidence were presented, which represents the range into which the true value of incidence is 95% likely to fall. Evidence of publication bias was assessed by the Egger’s test.44 All these meta-analyses were accomplished using Stata 12.0.
RESULTS
We searched PubMed (1160 onward), Web of Science (1761 onward) and Embase (1226 onward) electronic databases up to September 2019, of which 101 were related to our scientific questions. After scanning full text of the articles, there were 24 publications with 70 123 participants meeting the inclusion criteria initially (figure 1). Information on the 24 cohort studies included in the systematic review is summarised in table 1.
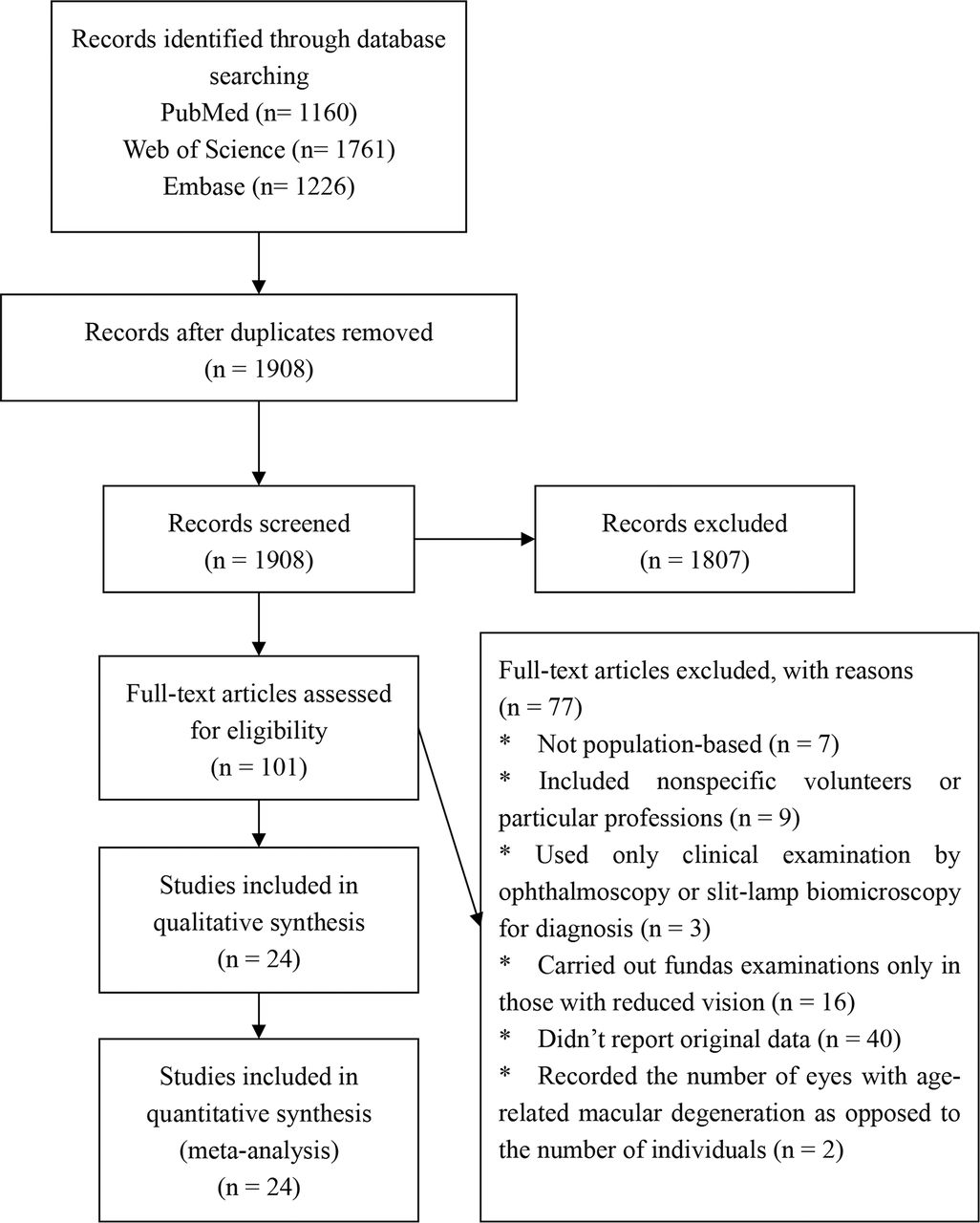
Selection process of articles in the review (n=24).
Pooled global incidence of AMD
Among the 24 studies, 5 were conducted in Asia,25 28 31 38 39 6 were conducted in North America,17 27 29 30 32 35 9 were conducted in Europe,19 20 22–24 33 36 40 41 2 were conducted in Oceania21 34 and 1 each was conducted in Latin America & Caribbean26 and Africa.37 We assessed the incidence of both early and late AMD among four major ethnic groups, namely, Whites, Blacks, Hispanics and Asians. The average baseline age of participants in each of the 24 cohort studies was more than 55 years. The sample sizes ranged from 359 in the Copenhagen study24 to 4926 in the Beaver Dam Eye Study (BDES)32 with all follow-up rates of being more than 50%. Whereas annual incidence of early AMD ranged from 0.45% in the Multi-Ethnic Study of Atherosclerosis (MESA)41 to 5.52% in the Study of Osteoporotic Fractures (SOF)29, annual incidence of late AMD was from 0% in the Thessaloniki Eye Study (TES)36 to 1.70% in the Antioxidants, Lipides Essentiels, Nutrition et Maladies Oculaires Study (ALENMOS)29 researched the incidence data of black women in North America only. All studies were of high quality (score 0–2) according to table 2. There was publication bias as indicated by Egger test (p<0.05).
Incidence of AMD by period of study
The annual incidence of AMD stratified by period of study is shown in figure 2. There was a slightly decreasing trend in the incidence of early AMD over time (after 2000 vs before 2000). Meanwhile, the late AMD incidence after 2000 is basically unchanged from those before.

Annual incidence of AMD stratified by the year of follow-up exam (%).
A, early AMD; B, late AMD.
Incidence of AMD by region
There was worldwide variation in the incidence of AMD. Geographically, the incidence of late AMD higher in Europe (0.26%, 95% CI 0.17% to 0.45%) than in other regions. Meanwhile, the lowest incidence of early AMD occurred in Asia (1.02%, 95% CI 0.81% to 1.29%). Africans had both the highest incidence of early AMD (2.85%, 95% CI 2.46% to 3.32%) and the lowest incidence of late AMD (0%).
Incidence of AMD by ethnicity
Figure 3 summarises the ethnicity-specific and pooled global incidence of AMD. The pooled global incidences of early and late AMD were 1.59% (95% CI: 1.12% to 2.10%, I2=98.5%, p<0.001) and 0.19% (95% CI: 0.13% to 0.28%, I2=96.2%, p<0.001), respectively. Whites had the highest incidence of early AMD (2.36%, 95% CI 1.61% to 3.46%), followed by Blacks (1.73%, 95% CI 0.93% to 3.21%), Asians (0.93%, 95% CI 0.72% to 1.19%) and Hispanics (0.50%, 95% CI 0.31% to 0.79%). Meanwhile, annual incidence of late AMD in studies was 0.33% (95% CI 0.20% to 0.53%) in Whites, 0.10% (95% CI 0.06% to 0.17%) in Asians, 0.08% (95% CI 0.04% to 0.18%) in Blacks and 0.05% (95% CI 0.03% to 0.10%) in Hispanics.

{kind=link}
{kind=link}
{kind=link}
Ethnic-specific and global incidence of AMD.
Meta-regression
The associations of seven categorical covariates with both late and early AMD were examined using meta-regression analyses and the results are shown in table 3. In the meta-regression analyses, average age at baseline was significantly associated with the annual incidence of early AMD (p=0.01). Ethnicity (p=0.025) was also found to be associated with annual incidence of early AMD. With regard to annual incidence of late AMD, average age at baseline (p=0.001), gender (p=0.011), region (p=0.043) and ethnicity (p=0.001) were significant associates.
Results of meta-regression analysis
DISCUSSION
In this systematic review and meta-analysis, we reported that the pooled global annual incidences of early and late AMD were 1.59% and 0.19%, respectively. The annual incidence rate of both early and late AMD was found to be highest in Europeans. Average age at baseline, ethnicity, region and gender were predictors for incident late AMD while only average age at baseline and ethnicity were associated with incident early AMD. These findings may be a useful guide for the precise projection of global burden of AMD.
Understanding the worldwide geographic distribution of incidence is crucial for developing global strategies for disease prevention. It is interesting to observe a higher incidence of early but a lower incidence of late AMD in Africa. The high incidence of early AMD in Africa may be a result of the higher UV radiation exposure,45–49 stronger genetic predisposition50 or greater susceptibility51 to inflammation. However, there were limited studies conducted in Africa and the conclusion is far from conclusive. Compared with Asia, the pooled incidence of early and late AMD was higher in Europe and Oceania, where the main residents are of white descent. Among the four major ethnic groups, the annual incidence of AMD is highest among whites, in concordance with the results of previous studies.7 9 52 53 The reasons which could explain the ethnic variations remain unclear.35 One possible explanation is that there is less protective melanin in the pigmented retinal pigment epithelium and choroid in Whites than in other ethnic groups.54–56 The melanin can act as a free radical scavenger and may also inhibit the leakage, migration or proliferation of endothelial cells. Other possible explanations involve the disparities in the frequency of genetic markers (eg, CHF(1q25-31) and ARMS2/HTRA1(10q26))55 56 and the exposure of AMD-related environmental factors.57 58
The result of meta-regression indicates that different demographic age-sex structure between regions may lead to the heterogeneity. In this way, the number of new cases could differ significantly in different regions with the same late AMD incidence. As for the gender difference in late AMD incidence, it mainly result from the higher incidence of neovascular age-related macular degeneration (NVAMD) in women than men, which has been supported by several cohort studies.21 24 29 40 59–61 We provided several explanations for this observation. With regard to gender difference, while hormonal/menopausal aetiologies may play an important role in this process,62 the relationship between NVAMD and stoke, both of which women have a higher incidence at older age, may also be an explanation.62–64 As related studies reported, NVAMD and stroke actually share common potential vascular risk factors,65 pathogenic mechanisms,63 and possibly even genetic determinants (eg, APOE genes).66–68 For example, a higher the stroke incidence could be observed in older women when NVAMD generally first occurs.69 In other words, there may be a potential unknown mechanism for this gender difference. Besides, survival bias may also lead to the gender difference on account of the finding that the reduced non-participants were more likely to be men who had already died of a stroke or had early AMD at baseline.
In our analysis, we found that there was no obvious upward or downward trend of early and late incidence of AMD over time, consistent with the data of the National Health and Nutrition Examination Survey,70 which indicated that the downward trend of AMD might be explained by the differences in methodological issues.
Our systematic review and meta-analysis updates two earlier incidence reviews which only focused in whites11 71 by summarising the incidence of AMD globally and the public health implications of the findings might be considerable. In these two previous publications, the annual incidence of late AMD was 0.35% in American whites and 0.14% in Europeans, consistent with our results of late AMD. However, apart from age, we also found that region and ethnicity were associated with the incidence of late AMD compared with these two reviews.
Our findings also suggest that counties in Europe and Oceania might need to increase the allocation of health services to visual impairment and blindness caused by AMD, because of the highest incidence of AMD in these regions. The increase of AMD incidence among developing countries also needs to be noted, as most of them residing in developing counties and have limited access to the expensive therapeutic approach such as the anti-VEGF treatment. Besides, the differences of incidences between different age and gender were also of research and epidemiological significance. From a research perspective, this finding could act as an evidence supporting that the absence of adjustment of incidence according to age-sex structure of population may result in the failure to conduct the conjoint analysis of AMD. In epidemiology, if different age and gender may lead to different numbers of incidences, could early health prevention be carried out for specific population to avoid the disease? In other words, once these problems are resolved, the present limited understanding of the etiological and risk factors of AMD is expected to flourish.
The strengths of our systematic review and meta-analysis are the use of fundus photography and standardised systems to assess AMD and the including of studies with relatively high quality. However, the review has several limitations. First of all, there were limited studies reporting the incidence of AMD in Latin America & Caribbean and Africa. Thus, the actual incidence in these areas is still unclear and more studies of high quality are warranted in these areas. In addition, annual incidence was estimated directly from aggregated data of cumulative incidence and average follow-up duration, which could make less accuracy in the estimation, extremely for populations with high rate of other morbidity and mortality and for a disease increasing non-linearly with age. The average follow-up duration was not usually given accurately in studies, which could also account for this deviation.
In summary, this systematic review offers a latest overview of the incidence of AMD globally. There is substantial evidence supporting a higher incidence of both early and late AMD in individuals of European descent. In addition, gender should be taken into full consideration when comparing the incidence of late disease among different studies. These findings provide vital guidance for the design and accomplishment of public health approaches such as screening programmes in both specific geographic locations and racial groups, as well as worldwide.
REFERENCES
Footnotes
MZ and P-CD contributed equally.
Contributors XFZ and CWP contributed substantially to the conception and design of this paper. MZ and PCD conducted the literature searches and extracted the data from published papers. MZ, PCD and JHL drafted the paper and carried out the statistical analysis.
Funding This study was supported by the Priority Academic Program Development of Jiangsu Higher Education Institutions (PAPD).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.
Linked Articles
- At a glance