
Abstract
Many towns and cities use passive samplers (diffusion tubes) to monitor nitrogen dioxide (NO2) concentration. However, literature studies have shown large horizontal and vertical concentration gradients for diffusion tubes placed over short distances, raising concerns over the representativeness of monitoring locations. This study examines variations in NO2 concentrations with height at two roadside locations along a busy urban road in Newcastle upon Tyne (UK) over an 8-month period. NO2 concentrations were passively monitored at building facades (approximately 7.0 m from the roadside) at heights of 0.7 m, 1.7 m and 2.7 m to replicate child breathing height in prams and buggies, adult breathing height and the Newcastle City Council sampling height (for 2017), respectively. Paired t tests indicated that NO2 concentrations were significantly lower at 2.7 m (4.7% lower, n = 16, p = 0.001) and 1.7 m (7.1% lower, n = 14, p = 0.007) compared with those at 0.7 m. There was no statistically significant difference between NO2 concentrations measured at 2.7 m and 1.7 m, indicating that UK local authority practice of placing diffusion tubes at higher than adult breathing height does not result in underreporting of NO2 concentrations for regulatory purposes. The results have clear public health implications as they provide evidence that young children, in an urban setting and close to busy roadways, may be exposed to higher NO2 concentrations compared with adults in the same location. We have shown that such differences might not be adequately reflected in the monitoring data from municipal authorities.
Similar content being viewed by others


Introduction
Elevated traffic-derived nitrogen dioxide (NO2) concentrations in urban areas have been linked to increased incidences of both mortality and disease (Atkinson et al. 2018; Committee on the Medical Effects of Air Pollutants 2018; Mills et al. 2016; WHO 2006). Of particular concern are the adverse health effects of NO2 on children (Esposito et al. 2014; Favarato et al. 2014; Gaffin et al. 2018), given that many schools are located in areas that breach air quality guidelines for NO2 (Guerriero et al. 2016; Salonen et al. 2019). To help protect the public against the health effects of NO2, the World Health Organization (WHO) has set guideline values of 40 μg m−3 and 200 μg m−3 for long-term (annual) and short-term (1-h) exposures respectively. The European Union and the UK use the same values (Beckwith et al. 2019). Nevertheless, there is evidence that NO2 is associated with health effects at concentrations that are well below the guideline values, even as low as 5 μg m−3 (Committee on the Medical Effects of Air Pollutants 2018).
Recent UK government statistics show that road sources contribute 34% of the total emissions of nitrogen oxides (NOx) in the UK, with energy generation; domestic and industrial sources; and other transport sources contributing 22%, 19% and 17% of the total respectively (DEFRA 2019a). At locations immediately adjacent to roads, 80% of the total NOx emissions are contributed from road sources (DEFRA 2019a). The NO2 component of the total NOx emissions comprises primary and secondary sources. Primary NO2 is the fraction of NOx emitted from a car exhaust that is already in the form of NO2. Over the last two decades, the fraction of NOx emitted in the form of primary NO2 has increased significantly, from below 0.1 for vehicles manufactured before 1998, to well over 0.3 more recently (Carslaw et al. 2019), with some studies quoting as high as 0.7 (Keuken et al. 2012).
Increased numbers of diesel vehicles on the road, with their widespread use of catalytic emission control technologies, are largely responsible for the increase in the fraction of NOx released as primary NO2 from car exhausts (Carslaw et al. 2019). Emission control by techniques such as selective catalytic reduction (SCR) oxidises NO to NO2, which is then used to oxidise the incomplete combustion products produced by the engine, i.e. CO, hydrocarbons and particulate matter, thus reducing the emission of these harmful pollutants and also increasing the amount of NO2 released (Carslaw et al. 2019). Other emission control technologies include lean NOx traps (LNT), where NOx is reduced to ammonia and water; LNT tends to produce higher NO2 emissions than SCR (Carslaw et al. 2019). Once emitted from the vehicle exhaust, NO that has not been oxidised reacts very quickly with tropospheric ozone to produce secondary NO2 (Clapp and Jenkin 2001), with a large proportion of this reaction thought to occur on the road, over a duration of a few seconds (Yang et al. 2018). Nevertheless, NOx emissions from vehicles are reducing as cleaner vehicles enter the overall vehicle stock (Carslaw et al. 2019; Keuken et al. 2012).
Municipal authorities monitor NO2 concentrations using a combination of instrumental and passive methods. Instrumental techniques, such as the reference method of chemiluminescence (Clapp and Jenkin 2001), allow accurate and precise determination of NO2 concentrations, with a high temporal resolution. Nevertheless, the high cost of such systems tends to restrict their geographical coverage (Pannullo et al. 2015). Passive techniques, such as Palmes-type diffusion tubes, allow a much more extensive spatial monitoring resolution. However, the requirement that the tubes be exposed for several weeks means that they are suitable only for monitoring against long-term ambient standards (exceedances of 1-h standards can be implied if annual average concentrations at diffusion tube locations exceed 60 μg m−3 (DEFRA 2016; Laxen and Marner 2003)). Diffusion tubes are also less precise than instrumental techniques and may have inherent biases (Heal et al. 2019).
Notwithstanding concerns over the performance of diffusion tubes, municipal authorities in many countries use them as an essential component of the local air quality management (LAQM) process (AEA Energy and Environment 2008). Typically, exposure of the tubes occurs over 4- or 5-week blocks (AEA Energy and Environment 2008) before being replaced, allowing NO2 determinations at monthly and yearly resolution.
UK Government guidance on the siting of diffusion tubes lists the following specific categories of site: kerbside (within 1 m of the kerb), roadside (between 1 and 5 m from the kerb edge, though in some circumstances, up to 15 m (DEFRA 2016)) and urban or suburban background sites (greater than 50 m from main roads) (AEA Energy and Environment 2008). The diffusion tubes are mounted on street furniture or building facades, as appropriate, with spacers used to ensure unimpeded airflow around the tube (AEA Energy and Environment 2008). Diffusion tube monitoring strategies are used to evaluate the performance of air quality management plans and will typically utilise dozens of diffusion tube locations across a city. For example, Newcastle City Council (NCC), in 2018, used 53 diffusion tube locations, as well as four automatic monitoring stations that were also capable of measuring NO2 (Newcastle City Council 2019). Having such large numbers of monitoring locations reporting NO2 concentrations year-on-year provides the spatial resolution needed to assess the effectiveness of air quality improvement measures.
Nevertheless, there is much literature debate about the variations in NO2 and other pollutant concentrations over distances as short as several metres, and the implications that this might have for representative siting of diffusion tube locations (Amato et al. 2019; Beckwith et al. 2019; Borge et al. 2016; Pannullo et al. 2015; Vardoulakis et al. 2011). For example, Borge et al. (2016) found NO2 gradients as high as 2 μg m−3 m−1 during a high spatial resolution monitoring survey at a busy roundabout in Madrid. Significant temporal variations in PM10 were also observed (as high as 55 μg m−3 min−1). Similarly, in a diffusion tube survey carried out in York, UK, Beckwith et al. (2019) found significant differences in NO2 concentrations between road stretches that were associated with acceleration, queuing or cruising. As well as the position of the monitoring location along a road with respect to junctions and pedestrian crossings etc., there is also the question of the fall-off in NO2 concentrations with distance from the kerb and the implications that this has for the reporting of representative exposure concentrations. The rate of fall-off is often reported as fitting an exponential equation (Kenagy et al. 2016) but is very much dependent on the local building infrastructure, such as the presence of street canyons (Amato et al. 2019; Borge et al. 2016). Consequently, ‘halving distances’ for NO2 concentrations have been reported to range from 25 m (± 35 m sd) for Barcelona (Amato et al. 2019) to over 100 m for Birmingham (Vardoulakis et al. 2011) and York (Beckwith et al. 2019). Of more relevance to the current study is the observation by Vardoulakis et al. (2011) that the annual mean NO2 concentrations in Birmingham were 21% higher for lamppost mounted diffusion tubes compared with those attached 5 m away on building facades.
As well as considerations over the spatial positioning of NO2 monitors, the height at which they are mounted has also been shown to have a significant influence on the reported NO2 concentration (Amato et al. 2019; Barratt et al. 2018; Cheong et al. 2012; Eeftens et al. 2019; Kenagy et al. 2016; Kohler et al. 2005; Laxen and Noordally 1987; Monn et al. 1997; Sajani et al. 2018; Scottish Government 2015; Vardoulakis et al. 2011). Most of the literature studies that have examined NO2 concentration fall-off with height have done so at different heights on multi-storey buildings, allowing an assessment of risk for residents due to pollution from the busy roads below. In most of the studies, a significant reduction in NO2 concentration is observed at the higher heights, ranging from 11% (Sajani et al. 2018) to 40% (Monn et al. 1997) for monitors placed at approximately 20 m in comparison with ground level. Nevertheless, one such study in Singapore found a more complex relationship between height and NO2 concentrations, with the middle floors of a 22-storey building recording the highest NO2 concentrations (16% higher at 17.5 m vs ground level, and then falling with increasing height thereafter) (Cheong et al. 2012). This unusual relationship was possibly due to the presence of a dense tree canopy between the road source and the building. Other factors that significantly affect the magnitude of the fall-off in NO2 concentrations with height include seasonal effects (Eeftens et al. 2019; Monn et al. 1997; Sajani et al. 2018) street infrastructure, particularly street canyons (Amato et al. 2019; Vardoulakis et al. 2011), and distance from the kerb (Kenagy et al. 2016).
For the present study, we are interested in the near-ground relationship between NO2 concentration and height, i.e. the difference in concentration at breathing heights of a child in a buggy and that of an adult. The motivation for this study is the varying practice across the UK concerning the NO2 monitoring heights used by municipal authorities and how these relate to the exposure of sensitive receptors. Ideally, diffusion tubes should be placed at ‘breathing height’, to represent the accurate exposure of the public to NO2. Nevertheless, UK guidance recommends that diffusion tubes be placed at heights of between 2 and 4 m to alleviate problems with theft and damage (AEA Energy and Environment 2008; Kenagy et al. 2016). In Newcastle upon Tyne, UK, where the current study is located, diffusion tubes used by NCC were positioned at the height of 2.7 m above ground in 2017, though this changed to 2.5 m in 2018 (Newcastle City Council 2018; Newcastle City Council 2019). Therefore, an adult at an average breathing height of 1.7 m (Kenagy et al. 2016) will experience NO2 concentrations approximately 1 m below what was being monitored and reported by NCC for 2017; this will be the case for many local authority areas across the UK. The official guidance acknowledges that tubes placed at heights above the breathing zone may ‘underestimate the actual concentrations to which the public are exposed’ (AEA Energy and Environment 2008). The average breathing height of children ranges from 0.7 to 1.5 m (Rivas et al. 2016), whereas children in prams and strollers have breathing heights of approximately 0.55 m and 0.85 m respectively (Sharma and Kumar 2018). Therefore, children will experience NO2 concentrations at heights that are as much as 2 m below what is being monitored and reported by NCC.
In this paper, we seek to examine the differences in measured NO2 concentrations as a function of height (0.7 m, 1.7 m and 2.7 m) at two separate roadside locations in the UK city of Newcastle upon Tyne. The study arose from an opportunity to incorporate additional sampling locations into the annual diffusion tube monitoring programme operated by NCC. Although such studies have been carried out in the past, notably that of Kenagy et al. (2016), who studied differences between NO2 concentrations at adult and child breathing height at roadside locations in Edinburgh, our study differs in that it is carried out at a greater distance from the road (the façade of the buildings), and for an extended period of time (8 months) and therefore for a wider range of meteorological conditions.
Methodology
The study was carried out in Heaton, a suburb of Newcastle upon Tyne, UK, approximately 3 km from the city centre. Heaton is a residential area with two primary schools, multiple shopping streets and a light railway station (part of the Tyne and Wear Metro system). We selected two locations along Chillingham Road (UK road reference: A188), which is the main shopping street for the area and has previously been identified by NCC as a ‘hotspot’ area with regard to air pollution and NO2 concentrations. Between 2008 and 2010, NCC carried out air quality monitoring, using diffusion tubes, at four locations along Chillingham Road; however, annual mean concentrations were found to be below the EU, and UK obligatory limit of 40 μg m−3 and so the monitoring was discontinued. In recent years, traffic volumes have increased, with an annual average daily traffic flow of 15,015 vehicles in 2018, representing an increase of 5% since 2008. The composition is 82% cars and taxis, 15% light goods vehicles, 1.2% buses and 1.2% heavy goods vehicles (Department for Transport 2020). There are several pedestrian crossing and traffic-lighted junctions that cause traffic to build up in stretches along the road.
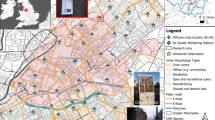
Site 1 (X 427052, Y 566421) is situated at the northern end of Chillingham Road (see Fig. 1), approximately 30 m from Ravenswood Primary School. The site is positioned approximately 75 m from the Coast Road (A1058) roundabout, which causes frequent speed changes. The site is a 2-storey end-terraced business premises. NCC previously monitored the same site between 2008 and 2010.

Location of the monitoring sites in Newcastle upon Tyne, UK
Site 2 (X 427209, Y 565727) is situated at the southern end of Chillingham Road (see Fig. 1), approximately 85 m from Chillingham Road Primary School and approximately 375 m from Chillingham Road Metro station. The site is positioned next to a busy T-junction and a pedestrian crossing which creates stop-start and idling traffic. The site is a 2-storey terraced residential property and has several business premises in close proximity. NCC previously monitored at a location 25 m from the site between 2008 and 2010.
Monitoring at the two sites was carried out with Palmes-type NO2 diffusion tubes in accordance with UK guidance (AEA Energy and Environment 2008; DEFRA 2016). The study was carried out as part of the overall monthly NCC diffusion tube monitoring programme.
Diffusion tubes use the principle of molecular diffusion to determine NO2 concentrations (AEA Energy and Environment 2008). When deployed, the cylindrical tubes are positioned vertically with one capped end (top) and one uncapped end (bottom) (see Fig. 2). Mass transfer occurs as gas molecules diffuse from an area of high concentration (uncapped end) to an area of low concentration (capped end) (AEA Energy and Environment 2008). The capped end contains two stainless steel grids coated in triethanolamine (TEA) to absorb NO2 directly from the air (AEA Energy and Environment 2008).

Schematic of a diffusion tube
The tubes were mounted at heights of 0.7, 1.7 and 2.7 m to replicate child breathing height, adult breathing height (Department for Transport 2020) and NCC sampling height (for 2017), respectively. Drainpipes located approximately 7 m from the roadside were used for mounting purposes as suitable pieces of ‘street furniture’. A spacer block measuring approximately 5 cm was placed between the tubes and the mounting surface to allow the open-ended tube to be exposed to freely circulating air. The tubes and spacer blocks were fixed to the drainpipes using a cable tie. The tubes were deployed in accordance with the diffusion tube calendar supplied by DEFRA (DEFRA 2019b). The exposure periods consisted of 4- or 5-week blocks (i.e. 28 or 35 days) over 9 months (July 2018 to February 2019 inclusive; the start and end dates of the exposure months were on Wednesdays). The tubes were changed on specific dates, as defined by the diffusion tube calendar (± 2 days).
The tubes were labelled with a unique sequentially numbered ID for logging purposes and each batch was placed in an airtight bag before and after exposure periods. The tubes were stored in a refrigerator and returned to SOCOTEC UK Limited (formerly ESG) for laboratory analysis in accordance with the standard guidance (AEA Energy and Environment 2008). At the laboratory, a colorimetric analysis technique was performed using a continuous flow auto-analyser (CFA) to determine NO2 concentrations by the quantification of the colour change in comparison with that produced by a known standard.
Diffusion tubes tend to under- or over-estimate NO2 concentrations for a variety of reasons, including variable wind flow at the tube opening, within-tube reaction of nitric oxide with ozone, and incomplete conversion of NO2 to nitrite in warm, sunny, low humidity conditions (RH < 75%) (AEA Energy and Environment 2008; Heal et al. 2019). As a result, local authorities are required to quantify the bias of their diffusion tube measurements and apply an appropriate bias adjustment factor. NCC carry out their own co-location studies in which the accuracy of the diffusion tubes is verified by exposure in conjunction with an automatic chemiluminescence analyser located at the Automatic Urban and Rural Network (AURN) station at St Mary’s Place (Newcastle City Council 2019). The NCC local bias adjustment factor was 0.90 for 2018/2019 (personal communication from NCC).
During this study, less than 1 year of NO2 diffusion tube data was obtained, and so we applied the standard seasonal adjustment approach used by local authorities in the UK (DEFRA 2016). Equation 1 was used to carry out the adjustment, where [NO2]Raw is the unadjusted NO2 concentration; [NO2]SA is the seasonally adjusted NO2 concentration; [AURNYear] is the annual average NO2 concentration measured by the chemiluminescence method at the Newcastle City Centre (Background Urban) for the year beginning July 2018; and [AURNPeriod] is the corresponding concentration for the 8-month sampling period of the study. The yearly and period averages were 30.22 μg m−3 and 30.85 μg m−3 respectively, giving a quotient in Eq.1 of 0.980.
Results and discussion
Trends in diffusion tube concentrations
The trends for the raw monthly NO2 concentrations at the three heights, for the two sites, are shown in Fig. 3, and a summary of the average concentration over the 8-month sampling period is shown in Table 1. In addition, Table 1 shows the bias-adjusted concentration at 2.7 m (the standard NCC sampling height for diffusion tube measurements for 2017) for the entire sampling period (applying a bias adjustment factor of 0.9, obtained from a co-location study), together with a seasonally adjusted concentration for the year beginning July 2018, as described in the methodology. The bias- and seasonally adjusted NO2 concentrations are both well below the 40 μg m−3 EU limit. The concentration of NO2 at site 1 is approximately 5 μg m−3 lower than that at site 2. Both sites are prone to traffic build-up and stop-start traffic, though this is more significant at site 2, given the close proximity to a T-junction and pedestrian crossing. The general trends for monthly NO2 concentrations shown in Fig. 1 are typical of the annual European pattern of NO2 concentrations, with the highest concentrations observed in winter months due to meteorological conditions such as ground-level temperature inversions and increased use of domestic heating (Hazenkamp-von Arx et al. 2004).

Monthly trends in NO2 concentration measured by diffusion tubes at two different locations: (a) site 1 and (b) site 2. Three height locations were monitored at each location, as specified in the legend. All measurements are raw data, as received from the laboratory, and are uncorrected for bias or seasonal effects
In Table 2, the differences between NO2 concentration at the three sampling heights are depicted as (a) the difference between the unadjusted mean values for the sampling period, taken from Table 1, and (b) the average difference for pairwise comparisons of raw monthly NO2 concentrations (both as μg m−3 and %). By both measures, there are differences in NO2 concentrations between the heights, with higher concentrations prevalent at the lower heights. The significance of these differences was tested using a paired sample t test analysis (two-tailed) on the raw monthly NO2 concentrations from diffusion tubes for each combination of sampling heights (2.7 m vs 1.7 m, 2.7 m vs 0.7 m and 1.7 m vs 0.7 m). The t tests were carried out on data from each site separately and for both sites combined. The combined analysis is justified because the distance of the diffusion tubes to the kerbside was the same for both sites (7 m) and the same approach was used for a similar study carried out by Kenagy et al. (2016).
For site 2, all pairwise height comparisons show that the NO2 concentration is lower at the higher of the comparison heights; however, none of the comparisons are statistically significant. For site 1 and the combined set of data, the concentration at 0.7 m is significantly higher than at both 1.7 m and 2.7 m. However, there is no statistically significant difference in concentrations between 1.7 and 2.7 m, i.e. between adult breathing height and the sampling height used by NCC. For the combined set of data, the difference in concentration between NCC sampling height and a child breathing height is 1.32 μg m−3, or 4.71%.
Comparison with other studies
Table 3 compares a range of literature studies, both for short vertical distances, as in our case, and for those that have been conducted on tall buildings, as already discussed. Of the studies listed in Table 3, only two have investigated the variation in NO2 concentrations near to the ground (Kenagy et al. 2016; Scottish Government 2015). The significantly higher NO2 concentration measured in our study at 0.7 m compared with that at 2.7 m (site 1 and the combined data set) is in agreement with research carried out by Kenagy et al. (2016). They found that tubes placed < 5 m from the kerb in a busy Edinburgh street were 8.7% lower at 2.0 m compared with that at 0.8 m. This same study found that tubes placed > 5 m from the kerb did not show a significant difference. Moreover, upon analysis of sub-groups within the < 5 m data, Kenagy et al. (2016) found that the significance in differences between heights does not extend beyond 2 m, which contradicts our results for site 1, and the combined dataset, but is in agreement with our results from site 2.
However, our findings for site 1 and the combined dataset, and those of Kenagy et al. (2016) for diffusion tubes < 5 m from the kerb, directly contradict a study published by the Scottish Government, who used a mobile road-located trolley to measure concentrations at 0.8 m and 1.68 m. The Scottish Government study found that NO2 concentrations were 15% higher in adult breathing height compared with that in children’s breathing height at busy junctions, though no significant difference was observed for low ambient concentrations (Scottish Government 2015). The discrepancy between studies is most likely explained by methodological differences, such as the siting of the monitor on the road, where the chemistry will be different. Also, the Scottish Government study used an electrochemical method (AQMesh) which has been shown to need additional correction to bring it in line with co-located measurements from reference monitors (Cordero et al. 2018). However, these contrasting findings do highlight a general difficulty in the literature about firmly establishing relationships between NO2 (and other pollutants) with height, and on setting guidance on the placement of diffusion tubes and other monitors.
Public health implications
Our study has shown that there is no significant difference in NO2 concentration between diffusion tubes placed at 1.7 m (adult breathing height) compared with that at 2.7 m. Consequently, there is no evidence that the use of locations higher than adult breathing height by many municipal authorities in the UK is likely to lead to underreporting of NO2 concentrations with respect to the guideline values. This finding is important because UK government guidance allows local authorities considerable leeway in determining the height at which diffusion tubes are placed, so as to minimise theft and damage (Kenagy et al. 2016). The variability in practice across the UK is demonstrated by Table S1 in the supplementary material, which shows typical ranges of diffusion tube heights used by local authorities, as detailed in their Annual Status Reports (Progress Reports in Scotland and Wales), which are submitted to DEFRA as part of the LAQM process in the UK (DEFRA 2016).
However, our study has provided evidence to support previous literature observations (Kenagy et al. 2016) that the standard practice of locating diffusion tubes at heights either at or above adult breathing height in the UK may lead to an underestimation of the concentration of NO2 experienced by children, either walking or in prams and buggies. These concerns have been highlighted in the literature for nitrogen dioxide, particulate matter and other pollutants (Sharma and Kumar 2018). In the present study, at site 1, we found that NO2 concentrations over an 8-month period were 5.9% lower at the NCC standard diffusion tube height (2.7 m) compared with at children’s breathing height (0.7 m). Moreover, we have shown that the zone in which these vertical concentration differences are significant may extend to at least 7 m, which is considerably further than reported by Kenagy et al. (2016). These findings have clear public health implications as they indicate that children, in an urban setting and close to busy roadways, may be exposed to higher NO2 concentrations compared with those experienced by an adult in the same location. The health effects of air pollution are amplified in vulnerable groups such as young children, especially those with pre-existing medical conditions such as asthma (Esposito et al. 2014; Favarato et al. 2014). Young children are considered vulnerable because their organs and immune systems are still developing and are therefore more susceptible to the damaging effects of air pollution (Paulin and Hansel 2016).
To emphasise the potential influence of sampling height on LAQM in Newcastle upon Tyne, we have calculated the effect of placing diffusion tubes at heights of 0.7 m instead of 2.7 m across the city. We have assumed a 4.4% increase in NO2 at all diffusion tube locations (based on the percentage increase at both sites combined), though we acknowledge the many varying factors that influence vertical NO2 profiles, as already discussed. Table 4 shows that based on 2017 data (Newcastle City Council 2018), an extra five (out of 41) diffusion tube locations would exceed the NO2 annual mean objective of 40 μg m−3 and a further five sites would potentially be in exceedance of the NO2 1-h mean objective of 200 μg m−3, as they would exceed an annual mean of 60 μg m−3, which is accepted as being indicative of an exceedance of the 1-h guideline (DEFRA 2016; Laxen and Marner 2003). For data collected during 2018, the effect is smaller with only two additional diffusion tube locations exceeding the 40 μg m−3 guideline value and one location exceeding 60 μg m−3.
Conclusions
The passive monitoring of two roadside locations for 8 months along a heavily trafficked urban roadway in Newcastle upon Tyne (UK) found that NO2 concentrations at child breathing heights (0.7 m) were significantly different to those at adult breathing heights (1.7 m) and Newcastle City Council (NCC) 2017 sampling height (2.7 m). Paired t test results showed that NO2 concentrations at child breathing heights were on average 4.71% and 7.12% lower at 2.7 m and 1.7 m respectively compared with that at 0.7 m. Nevertheless, there was variability in the results, as when analysed separately, one of the sites did not show a significant difference. The monitoring was carried out at a greater distance from the road than with previous literature studies (7 m) and suggests that the zone in which there is a significantly varying vertical NO2 concentration profile at near-ground level has a greater extent than previously thought. Modelling carried out on diffusion tube data for Newcastle upon Tyne from 2017 and 2018 indicates that if diffusion tube monitoring was carried out at 0.7 m, corresponding to the height of a child in a pram or buggy, there would be an increase in the number of monitoring locations that breached the 40 μg m−3 guideline value for NO2. Such a pattern is likely across all municipal authorities that carry out this type of monitoring, and so we should ask whether current practice adequately takes into account the most vulnerable receptors.
Data availability
All data is available within the paper.
References
AEA Energy & Environment (2008) Diffusion tubes for ambient NO2 monitoring: practical guidance for laboratories and users
Amato F, Pérez N, López M, Ripoll A, Alastuey A, Pandolfi M, Karanasiou A, Salmatonidis A, Padoan E, Frasca D, Marcoccia M, Viana M, Moreno T, Reche C, Martins V, Brines M, Minguillón MC, Ealo M, Rivas I, van Drooge B, Benavides J, Craviotto JM, Querol X (2019) Vertical and horizontal fall-off of black carbon and NO2 within urban blocks. Sci Total Environ 686:236–245. https://doi.org/10.1016/j.scitotenv.2019.05.434
Atkinson RW, Butland BK, Anderson HR, Maynard RL (2018) Long-term concentrations of nitrogen dioxide and mortality: a meta-analysis of cohort studies. Epidemiology. 29:460–472. https://doi.org/10.1097/EDE.0000000000000847
Barratt B et al (2018) A dynamic three-dimensional air pollution exposure model for Hong Kong. Res Rep Health Eff Inst:1–65
Beckwith M, Bates E, Gillah A, Carslaw N (2019) NO2 hotspots: are we measuring in the right places? Atmos Environ: X 2:100025. https://doi.org/10.1016/j.aeaoa.2019.100025
Borge R, Narros A, Artíñano B, Yagüe C, Gómez-Moreno FJ, de la Paz D, Román-Cascón C, Díaz E, Maqueda G, Sastre M, Quaassdorff C, Dimitroulopoulou C, Vardoulakis S (2016) Assessment of microscale spatio-temporal variation of air pollution at an urban hotspot in Madrid (Spain) through an extensive field campaign. Atmos Environ 140:432–445. https://doi.org/10.1016/j.atmosenv.2016.06.020
Carslaw DC, Farren NJ, Vaughan AR, Drysdale WS, Young S, Lee JD (2019) The diminishing importance of nitrogen dioxide emissions from road vehicle exhaust. Atmos Environ-X 1:100002. https://doi.org/10.1016/j.aeaoa.2018.100002
Cheong K, Tham K, Balasubramanian R, Kalaiarasan M (2012) Vertical distribution of NO2 in an urban area: exposure risk assessment in children. J Civil Environ Eng 2:1–6. https://doi.org/10.1016/j.aeaoa.2019.100025
Clapp LJ, Jenkin ME (2001) Analysis of the relationship between ambient levels of O3, NO2 and NO as a function of NOx in the UK. Atmos Environ 35:6391–6405. https://doi.org/10.1016/S1352-2310(01)00378-8
Committee on the Medical Effects of Air Pollutants (2018) Associations of long-term average concentrations of nitrogen dioxide with mortality. https://www.gov.uk/government/publications/nitrogen-dioxide-effects-on-mortality. Accessed 9th Jan 2020
Cordero JM, Borge R, Narros A (2018) Using statistical methods to carry out in field calibrations of low cost air quality sensors. Sensor Actuat B-Chem 267:245–254. https://doi.org/10.1016/j.snb.2018.04.021
DEFRA (2016) Local air quality management: technical guidance LAQM.TG(16). London
DEFRA (2019a) Clean air strategy 2019, London
DEFRA (2019b) Diffusion tube data entry system. https://laqm.defra.gov.uk/diffusion-tubes/data-entry.html. Accessed Jun 2020
Department for Transport (2020) Road traffic statistics. https://roadtraffic.dft.gov.uk/#6/55.254/-6.053/basemap-regions-countpoints. Accessed Jun 2020
Eeftens M, Odabasi D, Fluckiger B, Davey M, Ineichen A, Feigenwinter C, Tsai MY (2019) Modelling the vertical gradient of nitrogen dioxide in an urban area. Sci Total Environ 650:452–458. https://doi.org/10.1016/j.scitotenv.2018.09.039
Esposito S, Galeone C, Lelii M, Longhi B, Ascolese B, Senatore L, Prada E, Montinaro V, Malerba S, Patria MF, Principi N (2014) Impact of air pollution on respiratory diseases in children with recurrent wheezing or asthma. BMC Pulm Med 14:130. https://doi.org/10.1186/1471-2466-14-130
Favarato G, Anderson HR, Atkinson R, Fuller G, Mills I, Walton H (2014) Traffic-related pollution and asthma prevalence in children. Quantification of associations with nitrogen dioxide. Air Qual Atmos Health 7:459–466. https://doi.org/10.1007/s11869-014-0265-8
Gaffin JM, Hauptman M, Petty CR, Sheehan WJ, Lai PS, Wolfson JM, Gold DR, Coull BA, Koutrakis P, Phipatanakul W (2018) Nitrogen dioxide exposure in school classrooms of inner-city children with asthma. J Allergy Clin Immunol 141:2249–2255.e2242. https://doi.org/10.1016/j.jaci.2017.08.028
Guerriero C, Chatzidiakou L, Cairns J, Mumovic D (2016) The economic benefits of reducing the levels of nitrogen dioxide (NO2) near primary schools: the case of London. J Environ Manag 181:615–622. https://doi.org/10.1016/j.jenvman.2016.06.039
Hazenkamp-von Arx ME et al (2004) PM2. 5 and NO2 assessment in 21 European study centres of ECRHS II: annual means and seasonal differences. Atmos Environ 38:1943–1953. https://doi.org/10.1016/j.atmosenv.2004.01.016
Heal MR, Laxen DPH, Marner B (2019) Biases in the measurement of ambient nitrogen dioxide (NO2) by Palmes passive diffusion tube: a review of current understanding. Atmosphere-Basel. 10. https://doi.org/10.3390/atmos10070357
Kenagy HS, Lin C, Wu H, Heal MR (2016) Greater nitrogen dioxide concentrations at child versus adult breathing heights close to urban main road kerbside. Air Qual Atmos Health 9:589–595. https://doi.org/10.1007/s11869-015-0370-3
Keuken MP, Roemer MGM, Zandveld P, Verbeek RP, Velders GJM (2012) Trends in primary NO2 and exhaust PM emissions from road traffic for the period 2000-2020 and implications for air quality and health in the Netherlands. Atmos Environ 54:313–319. https://doi.org/10.1016/j.atmosenv.2012.02.009
Kohler M, Corsmeier U, Vogt U, Vogel B (2005) Estimation of gaseous real-world traffic emissions downstream a motorway. Atmos Environ 39:5665–5684. https://doi.org/10.1016/j.atmosenv.2004.09.088
Laxen D, Marner B (2003) Analysis of the relationship between 1-hour and annual mean nitrogen dioxide at UK roadside and kerbside monitoring sites. Available from Defra, 2006a and Defra
Laxen DPH, Noordally E (1987) Nitrogen-dioxide distribution in street canyons. Atmos Environ 21:1899–1903. https://doi.org/10.1016/0004-6981(87)90150-8
Mills IC, Atkinson RW, Anderson HR, Maynard RL, Strachan DP (2016) Distinguishing the associations between daily mortality and hospital admissions and nitrogen dioxide from those of particulate matter: a systematic review and meta-analysis. BMJ Open 6:e010751. https://doi.org/10.1136/bmjopen-2015-010751
Monn C, Carabias V, Junker M, Waeber R, Karrer M, Wanner H-U (1997) Small-scale spatial variability of particulate matter< 10 μm (PM10) and nitrogen dioxide. Atmos Environ 31:2243–2247. https://doi.org/10.1016/S1352-2310(97)00030-7
Newcastle City Council (2018) 2018 Air quality annual status report. https://www.newcastle.gov.uk/services/environment-and-waste/environmental-health-and-pollution/air-pollution/air-quality. Accessed Jun 2020
Newcastle City Council (2019) 2019 Air quality annual status report. https://www.newcastle.gov.uk/services/environment-and-waste/environmental-health-and-pollution/air-pollution/air-quality. Accessed Jun 2020
Pannullo F, Lee D, Waclawski E, Leyland AH (2015) Improving spatial nitrogen dioxide prediction using diffusion tubes: a case study in West Central Scotland. Atmos Environ 118:227–235. https://doi.org/10.1016/j.atmosenv.2015.08.009
Paulin L, Hansel N (2016) Particulate air pollution and impaired lung function. F1000Res 5. https://doi.org/10.12688/f1000research.7108.1
Rivas I, Donaire-Gonzalez D, Bouso L, Esnaola M, Pandolfi M, de Castro M, Viana M, Àlvarez-Pedrerol M, Nieuwenhuijsen M, Alastuey A, Sunyer J, Querol X (2016) Spatiotemporally resolved black carbon concentration, schoolchildren’s exposure and dose in Barcelona. Indoor Air 26:391–402. https://doi.org/10.1111/ina.12214
Sajani SZ et al (2018) Vertical variation of PM2.5 mass and chemical composition, particle size distribution, NO2, and BTEX at a high rise building. Environ Pollut 235:339–349. https://doi.org/10.1016/j.envpol.2017.12.090
Salonen H, Salthammer T, Morawska L (2019) Human exposure to NO2 in school and office indoor environments. Environ Int 130:104887. https://doi.org/10.1016/j.envint.2019.05.081
Scottish Government (2015) Air quality study: assessing variations in roadside air quality with sampling height: a mobile air quality monitoring study commissioned to assess variations in roadside air quality. https://www.gov.scot/publications/air-quality-study-scotland-assessing-variations-roadside-air-quality-sampling/pages/1/. Accessed 26th May 2020
Sharma A, Kumar P (2018) A review of factors surrounding the air pollution exposure to in-pram babies and mitigation strategies. Environ Int 120:262–278. https://doi.org/10.1016/j.envint.2018.07.038
Vardoulakis S, Solazzo E, Lumbreras J (2011) Intra-urban and street scale variability of BTEX, NO2 and O3 in Birmingham, UK: implications for exposure assessment. Atmos Environ 45:5069–5078. https://doi.org/10.1016/j.atmosenv.2011.06.038
WHO (2006) WHO air quality guidelines for particulate matter, ozone, nitrogen dioxide and sulfur dioxide - global update 2005 - summary of the risk assessment. Geneva
Yang B, Zhang KM, Xu WD, Zhang S, Batterman S, Baldauf RW, Deshmukh P, Snow R, Wu Y, Zhang Q, Li Z, Wu X (2018) On-road chemical transformation as an important mechanism of NO2 formation. Environ Sci Technol 52:4574–4582. https://doi.org/10.1021/acs.est.7b05648
Acknowledgements
We are grateful to Newcastle City Council for incorporating the two additional diffusion tube locations into their standard LAQM monitoring programme for the duration of the study.
Funding
This study was supported by Northumbria University and by Newcastle City Council (funded the diffusion tube analysis).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
ESM 1
(DOCX 16.6 kb)
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Rowell, A., Terry, M.E. & Deary, M.E. Comparison of diffusion tube–measured nitrogen dioxide concentrations at child and adult breathing heights: who are we monitoring for?. Air Qual Atmos Health 14, 27–36 (2021). https://doi.org/10.1007/s11869-020-00909-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11869-020-00909-4