Article Text

Abstract
Background and purpose Transient ischaemic attack (TIA), transient symptoms with infarction (TSI) and diffusion-weighted imaging (DWI)-negative acute ischaemic stroke (AIS) share similar aetiologies but are considered to have a rather benign prognosis. We intended to investigate the association between intracranial atherosclerotic stenosis (ICAS), extracranial atherosclerotic stenosis (ECAS) and the prognosis of patients with TIA, TSI and DWI-negative AIS.
Methods Clinical and imaging data of eligible participants were derived from the Chinese Intracranial Atherosclerosis study, according to symptom duration, acute infarction on DWI and discharge diagnosis. Based on the severity and location of arterial atherosclerosis, we categorised the study population into four groups: no or <50% ICAS and no ECAS; ≥50% ICAS but no ECAS; no or <50% ICAS with ECAS; and concurrent ≥50% ICAS and ECAS. Using multivariable Cox regression models, we analysed the relationship between the severity and distribution of large artery atherosclerosis and the prognosis of TIA, TSI and DWI-negative AIS.
Results A total of 806 patients were included, 67.3% of whom were male. The median age of the study participants was 63 years. Patients in the concurrent ≥50% ICAS and ECAS subgroup had both a significantly higher 1-year recurrence rate (adjusted HR 3.4 (95% CI 1.15 to 10.04), p=0.027) and a higher risk of composite vascular events (adjusted HR 3.82 (95% CI 1.50 to 9.72), p=0.005).
Conclusions Concurrent ICAS and ECAS is associated with a higher possibility of 1-year recurrent stroke or composite vascular events. Large artery evaluation is necessary to assess patients with transient ischaemic symptoms or DWI-negative AIS. Progress in shortening the time interval between symptom onset and large vessel evaluation is needed.
- stroke
- atherosclerosis
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
The estimated lifetime risk of stroke in China is up to 24.9%, and it is the leading cause of death nationwide.1 2 Ischaemic stroke accounts for 69.6% of all strokes in China.3 Progressing transient ischaemic symptoms were reported in 15%–30% of patients who had ischaemic stroke.4 Ischaemic symptoms of less than 24 hours in duration are usually diagnosed as transient ischaemic attack (TIA). With the wide use of brain imaging such as diffusion-weighted MRI, the definition of TIA has been revised from time to tissue basis.5 6
In daily practice, the two definitions are often combined to evaluate patients with acute ischaemic cerebrovascular disease. Acute diffusion-weighted imaging (DWI) lesions are found in 13.9%–34.3% patients with TIA, a condition known as transient symptoms with infarction (TSI).7 8 In patients initially diagnosed with acute ischaemic stroke (AIS), up to 6.8% had negative results on DWI scan.9 Although the DWI sequence of MRI is more sensitive in detecting acute infarction(s),10 it is not recommended for initial diagnosis or for planning subsequent treatment in the recent guideline for early management11 of all patients with suspected stroke. It has been recommended in selecting candidates for mechanical thrombectomy.12 Compared with patients with persistent ischaemic symptom(s) and positive DWI findings, TSI and DWI-negative AIS are considered to have milder clinical manifestations and are prone to be excluded from clinical trials.13 14
Identification of higher risk patients is crucial for customised monitoring and treatment schedule.5 Large artery atherosclerosis is one of the imaging markers that predict the prognosis of stroke or TIA independent of widely used risk stratification systems, such as the ABCD2 score.15 Routine tests of large artery were recommended for patients with suspected TIA in the 2009 American Stroke Association (ASA) scientific statement, but the applicability of these evaluations depended mainly on local availability and expertise,6 and potential gaps between the percentage of vascular evaluation in clinical practice and guideline-recommended vascular assessment, such as carotid imaging, existed.16
The Chinese Intracranial Atherosclerosis (CICAS) study was designed to investigate the prevalence and analyse the risk factors for recurrent stroke in patients with large artery occlusive disease in China.17 The CICAS study found a higher prevalence of intracranial artery atherosclerosis compared with extracranial artery atherosclerosis (46% vs 14%).
A previous study found that the coexistence of intracranial artery stenosis and the extracranial lipid-rich necrotic core was associated with a higher risk of subsequent vascular events.18 We aimed to test the hypothesis that concurrent intracranial atherosclerotic stenosis (ICAS) and extracranial atherosclerotic stenosis (ECAS) might increase the risk of stroke recurrence and composite vascular events in patients with transient ischaemic symptoms or AIS with negative DWI.
Methods
Data derivation and study population
The current study derived data from the CICAS project. Detailed protocol and results have been published previously.17 Briefly, the CICAS study is a multicentre, hospital-based, prospective cohort that included patients aged 18–80 years old who had ischaemic stroke or TIA within 7 days from symptom onset. Exclusion criteria were patients (1) who were clinically unstable; (2) with a modified Rankin Scale score (mRS) >2 before admission; (3) with a known source of cardioembolism; and (4) who were unable to cooperate during brain MRI scan.
Written informed consent was collected from all enrolled patients or their legal proxies.
Three subgroups of the CICAS study participants were included in the current analysis: (1) patients with TIA, defined as patients with a discharge diagnosis of TIA or with focal neurological symptoms or signs that lasted less than 24 hours without acute infarction on DWI sequence; (2) patients with TSI, defined as patients who had an episode of ischaemic symptoms or signs that lasted less than 24 hours with acute infarction(s) on DWI sequence; and (3) patients with DWI-negative AIS, defined as patients who had persistent focal neurological symptoms (lasted longer than 24 hours) without acute ischaemic lesion(s) on DWI sequence.
Patients with a discharge diagnosis of ischaemic stroke and positive DWI findings (acute infarction) were excluded.
Outcomes definition and assessment
The outcomes are consistent with the CICAS study.17 We focused on recurrent stroke (ischaemic or haemorrhagic) and composite vascular events (including myocardial infarction, angina pectoris, haemorrhagic events and ischaemic vascular events, including stroke or TIA) at 1 year.
The protocol for follow-up has been reported previously.17 Medical records and images of recurrent stroke or composite vascular events were reviewed by centralised adjudicators and the principal investigator.19
Imaging analysis
All patients were evaluated following a standardised test panel of conventional MRI on a 3.0 or 1.5 T MRI scanner. DWI, T1/T2-weighted imaging, fluid-attenuated inversion recovery sequences and three-dimensional time-of-flight magnetic resonance angiography (3D-TOF-MRA) were required in the standardised test sequences. Scanning parameters were demanded in the protocol.17 We used the initial MRI to identify acute infarction(s). To screen for extracranial arteries, patients underwent duplex colour Doppler ultrasound or contrast-enhanced MRA.
According to the Warfarin-Aspirin Symptomatic Intracranial Disease Study criteria,20 two experts ascertained the degree of ICAS. The following arterial segments of the intracranial arteries were included for assessment: bilateral intracranial internal carotid artery (locations of stenosis distal to the ophthalmic artery), anterior cerebral artery A1/A2, middle cerebral artery M1/M2, posterior cerebral artery P1/P2 and basilar artery.17 The extracranial part of the internal carotid artery and vertebral artery, bilateral external carotid artery, and bilateral proximal part of the arteria subclavia were assessed using the North American Symptomatic Carotid Endarterectomy Trial criteria.21
In this study, the severity of ICAS was categorised into two groups: no stenosis or <50% stenosis, ≥50% stenosis or occlusion (including 50%–69% stenosis, 70%–99% stenosis, and occlusion). The degree of ECAS was dichotomised into <50% or no stenosis and ≥50% stenosis or occlusion.
Statistical analysis
The study population was further divided into four subgroups: (1) non-stenosis group, which was defined as <50% or no ICAS without ≥50% ECAS; (2) ICAS-only group, defined as ≥50% ICAS or intracranial artery occlusion without ≥50% ECAS; (3) ECAS-only group, defined as <50% or no ICAS with ≥50% ECAS; and (4) ICAS+ECAS group, defined as ≥50% ICAS or intracranial artery occlusion with ≥50% ECAS.
Among the subgroups, we intended to compare the demographic and clinical characteristics. χ2 statistics or Fisher’s exact tests were used to compare categorical variables. The Wilcoxon rank-sum test and Mann-Whitney tests were used to compare continuous variables as appropriate.
Baseline characteristics and outcomes were also assessed among patients with different diagnoses (TIA, TSI and DWI-negative AIS).
We assessed the relationship between severity and distribution (intracranial or extracranial) of large artery atherosclerosis and prognosis of TIA, TSI and DWI-negative AIS by multivariable Cox regression method, expressed by crude and adjusted HR with 95% CI. We described the cumulative risk of subsequent stroke by drawing Kaplan-Meier curves. A two-sided p value less than 0.05 was considered to be of statistical significance. SAS V.9.4 software was used to perform all statistical analyses.
Results
Study participants and baseline characteristics
A total of 2051 patients, including 230 patients with incomplete information on symptom duration or number of infarction(s) and 1821 patients with persistent symptoms (lasting >24 hours) and infarction(s), were excluded. Among 264 patients with TIA, 91 patients with TSI, 374 patients with DWI-negative AIS, and 84 patients with a discharge diagnosis of TIA and incomplete information on symptom relief and number of infarction(s), 7 patients without complete follow-up were excluded, resulting in 806 patients fulfilling the inclusion criteria (figure 1).
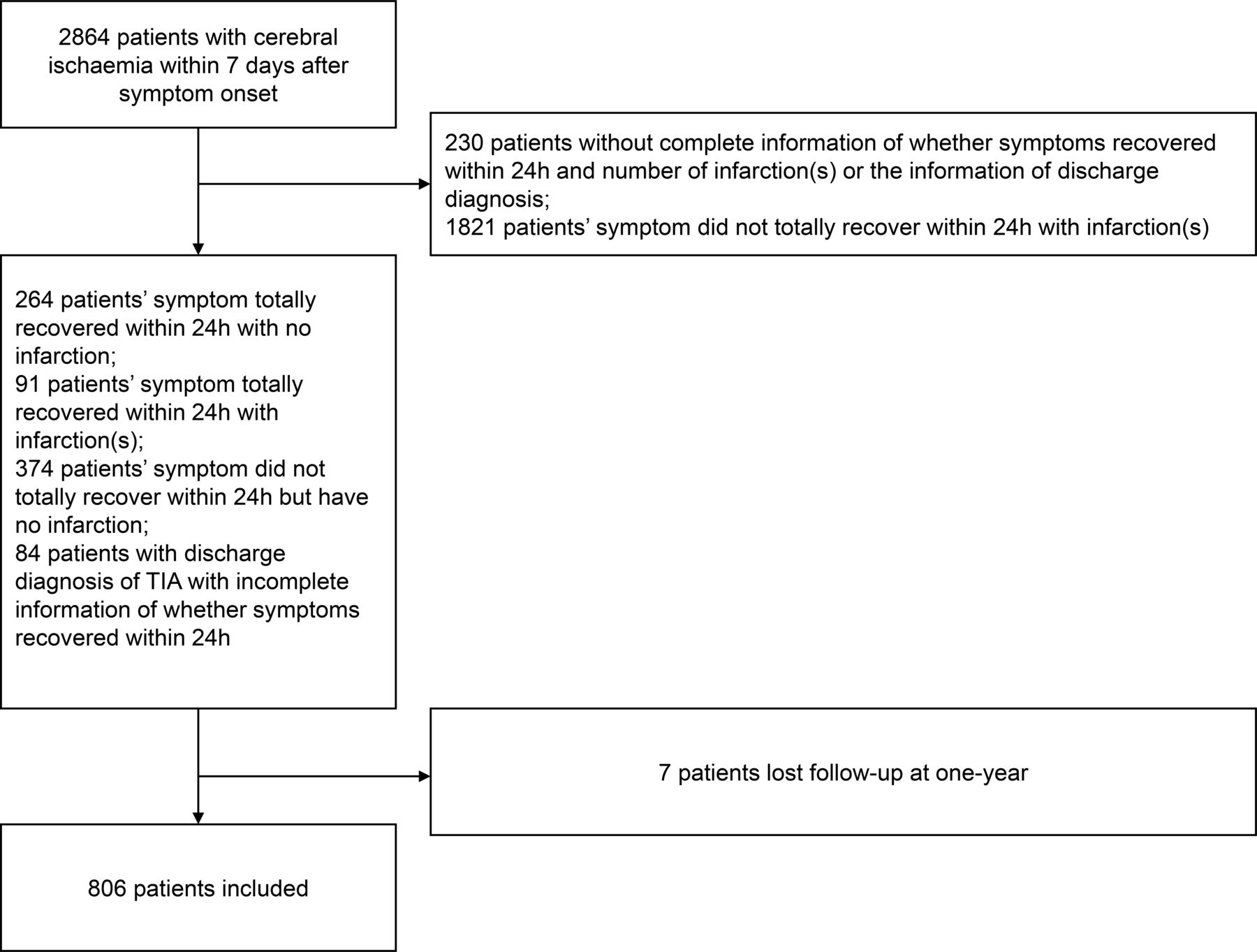
Flow chart of patient inclusion. TIA, transient ischaemic attack.
There were 542 male patients (67.3%), and the median age of the included patients was 63 years. During the 1-year follow-up, 32 patients had recurrent stroke and 37 patients had composite vascular events.
Univariable analysis among subgroups
There were 463 patients in the non-stenosis group, 233 patients in the ICAS-only group, 51 patients in the ECAS-only group and 59 patients in the concurrent ICAS and ECAS group. In the univariable analysis of baseline characteristics among subgroups categorised by severity of ICAS and ECAS, compared with the other three groups, patients with concurrent ICAS and ECAS tended to have higher mRS scores prior to the current event, with more of them having a history of ischaemic stroke as well as hypertension (table 1).
Baseline characteristics based on subgroups of stenosis
Large artery atherosclerosis and risk of recurrent stroke or composite vascular events
Patients with ICAS only had a higher risk of recurrent stroke after adjusting for age and sex (HR 2.51 (95% CI 1.12 to 5.60), p=0.023). Still, after adjusting for all confounding factors in univariate analysis, the association was not significant.
After adjusting for all confounding factors in univariate analysis, a significantly higher recurrence rate (8.5% vs 2.4% in the non-stenosis group, 5.6% in the ICAS-only group and 5.9% in the ECAS-only group) was seen in patients with concurrent ICAS and ECAS (adjusted HR 3.4 (95% CI 1.15 to 10.04), p=0.027) (table 2). As shown in figure 2, the cumulative risk of recurrent stroke was highest in the concurrent ICAS and ECAS group.

{kind=link}
{kind=link}
Cumulative incidence of recurrent stroke according to severity and location of atherosclerosis using Kaplan-Meier survival graphs at 1 year. Stroke included recurrent (ischaemic or haemorrhagic) stroke. (A) Non-stenosis, defined as <50% or no ICAS without ≥50% ECAS; (B) ICAS only, defined as ≥50% ICAS or intracranial artery occlusion without ≥50% ECAS; (C) ECAS only, defined as <50% or no ICAS with ≥50% ECAS; (D) ICAS+ECAS, defined as ≥50% ICAS or intracranial artery occlusion with ≥50% ECAS. ECAS, extracranial atherosclerotic stenosis; ICAS, intracranial atherosclerotic stenosis.
One-year outcomes stratified by severity and location of atherosclerosis
Higher risk of composite vascular events was seen in patients with concurrent ICAS and ECAS (11.9% vs 3.0% in the non-stenosis group, 5.6% in the ICAS-only group and 5.9% in the ECAS-only group) following adjustment of all factors with the difference in univariate analysis (adjusted HR 3.82 (95% CI 1.50 to 9.72), p=0.005) (table 2).
Baseline characteristics and outcomes of different diagnosis groups
Patients in the DWI-negative AIS group were more likely to have higher mRS score prior to the current event, more history of ischaemic stroke, myocardial infarction, hypertension and higher baseline National Institutes of Health Stroke Scale (NIHSS) score. Compared with other groups, patients with TSI were more likely to have ECAS. Proportions of patients who received endovascular treatment were similar among groups (online supplementary table 1).
Supplemental material
Compared with the TIA and DWI-negative AIS groups, patients with TSI had a higher risk of recurrent stroke and composite vascular events. Due to the relatively small number of events, multivariable analysis was not applicable (online supplementary table 2).
After adjusting for diagnosis and other confounding factors (demographics, medical history and essential treatment strategy), which showed statistical differences among groups of severity and location of atherosclerosis, a higher rate of recurrence (adjusted HR 3.20 (95% CI 1.03 to 9.91), p=0.044) and composite vascular events (adjusted HR 3.58 (95% CI 1.31 to 9.77), p=0.013) remained in patients with concurrent ICAS and ECAS (online supplementary table 3).
In the multivariate analysis including only patients with TIA and DWI-negative AIS, after adjusting for potential confounding factors, which showed statistical differences in the univariate analysis among groups of different severity and location of atherosclerosis (online supplementary table 4), patients with concurrent ICAS and ECAS portended the highest risk of recurrence (adjusted HR 4.95 (95% CI 1.04 to 23.64), p=0.045) and composite vascular events (adjusted HR 4.72 (95% CI 1.31 to 17.05), p=0.018) (online supplementary table 5).
Distribution of bleeding events according to treatment (dual antiplatelet or not) and diagnosis is shown in the online supplementary figure. The total number of bleeding was lower in the dual antiplatelet group, but the percentage of bleeding was higher in patients who received dual antiplatelet treatment. The association between dual antiplatelet treatment and risk of bleeding was not calculable due to the low bleeding rate. Current guideline recommends short-term dual antiplatelet treatment for patients who had minor stroke (NIHSS ≤3) or high-risk TIA (ABCD2 score ≥4),11 and further evaluation based on NIHSS and ABCD2 score is needed in a registry with larger sample size.
Supplemental material
DISCUSSION
Our study suggests that independent of other risk factors, concurrent ICAS and ECAS is a predictor of stroke recurrence and composite vascular events in patients with TIA, TSI and DWI-negative AIS.
The results supported previous findings. Intracranial artery atherosclerosis and extracranial artery atherosclerosis were prevalent in patients with TIA and predicted a higher risk of recurrent ischaemic events.15 In patients with TSI, large artery atherosclerosis was independently associated with an elevated possibility of subsequent stroke.22 Whether combined ICAS and ECAS increases the recurrence or rate of composite vascular events after TIA or TSI needs to be investigated. The relationship between large artery sclerosis and the prognosis of DWI-negative AIS needs to be elucidated.
Atherosclerotic disease is a systemic disease and affects different arterial territories with shared pathophysiological pathways and partly overlapped risk factors.23 A higher prevalence of ICAS was reported in Asian patients with ischaemic cerebrovascular disease.24 Despite guideline-recommended therapy, patients with ischaemic cerebrovascular disease with ICAS had a higher risk of subsequent stroke, composite vascular events or death.25 26 ECAS is also a predictor of recurrent stroke and vascular events in patients with ischaemic cerebrovascular disease.27 28 Although ICAS and ECAS were different phenotypes of systemic atherosclerosis, coexistence with ECAS was common in patients with ICAS.29 30 Based on a study of 7-Tesla MRI and autopsy, the burden of ICAS was associated with extracranial artery atherosclerotic lesions.31 32
Several studies have explored the impact of concurrent ICAS and ECAS on the prognosis of cerebrovascular disease. The Asymptomatic Myocardial Ischemia in Stroke and Atherosclerotic Disease study, a hospital-based, prospective, single-centre registry, enrolled 403 patients who had a stroke and assessed the atherosclerotic lesions in multiple arterial territories (intracranial arteries, extracranial carotid arteries, coronary arteries and peripheral arteries). Concurrent ECAS in patients with significant ICAS increased the risk of major adverse cardiovascular events from 9.0% to 23.4%.33 In a study focused on recent ischaemic stroke or TIA of the anterior circulation, coexisting intracranial artery atherosclerosis and extracranial carotid plaques significantly increased the rate of recurrent stroke (OR 3.16 (95% CI 1.03 to 9.71), p=0.044).34
The study participants we focused on could be excluded in clinical practice since they are presumed to have better outcomes compared with those who had ischaemic stroke. Patients with TIA or TSI presented with a focal neurological deficit but relieved within a short period, which could result in a presumption of benign prognosis. For patients with DWI-negative AIS, later risk of new ischaemic stroke was not significantly less than DWI-positive patients with AIS.8 Symptomatic intracranial artery atherosclerosis is prevalent in these patients.35 Patients with ICAS on intensive medical treatment had a low risk of recurrent stroke.36 37 Early evaluation of large artery is essential to tailor proper treatment strategy.
Although the 2009 ASA scientific statement recommended that patients with TIA should undergo neuroimaging evaluation within 24 hours after symptom onset,6 there were also gaps in adherence to the recommended time window of vascular imaging evaluation. As a hospital-based registry, the CICAS study did not adopt the ‘round-the-clock’ system of rapid assessment. In our study, the median time interval between symptom onset and MRI evaluation was 4 days. However, in the TIAregistry.org, a multinational prospective cohort study, the ‘round-the-clock’ system evaluated eligible patients on an urgent basis and allowed all necessary diagnostic tests to be completed, usually within 3 hours.15 Efforts to improve rapid access to acute care to avoid delay in diagnostic tests are called upon.38
Our study has certain advantages. This study derived data from a multicentre, hospital-based study and all enrolled patients were examined following a standard battery of intracranial/extracranial artery evaluations. We centrally interpreted imaging data, and events adjudication reduced potential bias induced by intercentre differences.
Our study has certain limitations. First, dependent on the vascular flow intensity signal, 3D-TOF-MRA could exaggerate the degree of luminal stenosis. Double confirmation of stenosis severity and stable intrarater/inter-rater agreement minimised the influence of the inherent disadvantage of MRA evaluation. Second, we used ultrasonographic or contrast-enhanced MRA to detect extracranial artery atherosclerotic stenosis. Recent studies emphasised the prognostic value of imaging markers other than luminal stenosis of extracranial arteries, including high-risk non-stenotic carotid plaque,39 calcification40 or inflammation.27 Further study using techniques with a higher spatial resolution to detect the composition of plaques or changes of vessel walls would help distinguish the progress of atherosclerosis. Third, the sample size of our subgroup analysis was relatively small due to our special focus based both on symptom duration and DWI positivity, which could result in limited statistical power. Larger scale analysis will be needed before generalising the results of our study. Fourth, we observed a similar risk of recurrent stroke and composite vascular events in patients with ICAS only, compared with patients with ECAS only. Since we discussed ICAS and ECAS degree by luminal stenosis, further studies on more imaging biomarkers of plaque characteristics and vessel wall changes are needed to distinguish the influence of ICAS from that of ECAS on the prognosis of patients with transient ischaemic symptoms or negative-DWI ischaemic stroke.
CONCLUSIONS
In summary, combined intracranial artery atherosclerosis and extracranial artery atherosclerosis increased the 1-year risk of recurrent stroke and composite vascular events (including myocardial infarction, angina pectoris, haemorrhagic events and ischaemic vascular events other than stroke or TIA) in patients with TIA, TSI and DWI-negative AIS. Early and thorough screening of intracranial/extracranial artery for atherosclerotic lesions is necessary to triage patients and target treatment. Progress in shortening the time interval between symptom onset and large vessel evaluation is needed.
Acknowledgments
We appreciate all study participants and their relatives for the constant support given to the CICAS study. We also appreciate the hard work and dedication of all relevant clinicians, statisticians, coordinators and imaging technicians who participated in the study.
References
Footnotes
Twitter @yilong
Contributors YJW had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. YJW designed the study. YS, JJ and YSP collected the data. YS wrote the manuscript. WC, HZ, HL, YHP, LL, XZ, YLW and XM reviewed, edited and approved the final version.
Funding This study is supported by grants from the National Natural Science Foundation of China (81971091 and 81901177), Beijing Hospitals Authority Youth Programme (QML20190501), Ministry of Science and Technology of the People’s Republic of China (2016YFC0901002, 2016YFC0901001, 2017YFC1310901, 2017YFC1310902, 2017YFC1307905, 2018YFC1311700 and 2018YFC1311706), Beijing Municipal Administration of Hospitals (SML20150502), Beijing Municipal Science & Technology Commission (D171100003017002 and D151100002015003), National Science and Technology Major Project (2017ZX09304018), and Beijing Tiantan Hospital (2018-YQN-1).
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The ethics committee of Beijing Tiantan Hospital (IRB approval number: (2007) Hospital Ethical Approval No. 27) gave ethical approval for the study protocol.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. Please contact China National Clinical Research Center for Neurological Diseases.