
Abstract
Stigma regarding HIV pre-exposure prophylaxis (PrEP) is commonly implicated as a factor limiting the scale-up of this highly effective HIV prevention modality. To quantify and characterize PrEP stigma, we developed and validated a brief HIV PrEP Stigma Scale (HPSS) among a group of 279 men who have sex with men (MSM). Scale development was informed by a theoretical model to enhance content validity. We assessed two scale versions, Semantic Differential and Likert, randomizing the order in which scales were presented to participants. Both scales demonstrated high internal consistency. The Likert scale had substantially better construct validity and was selected as the preferred option. Scale scores demonstrated construct validity through association with constructs of interest: healthcare distrust, HIV knowledge, perceived proportion of friends/partners on PrEP, perceived community evaluation of PrEP, and perceived effectiveness of PrEP. The scale accounted for 25% of the total variance in reported willingness to be on PrEP, indicating the substantial role PrEP stigma may have on decisions to initiate PrEP. Given increased efforts to roll-out PrEP, having a valid tool to determine the level and types of PrEP stigma in individuals, groups, and communities can help direct implementation plans, identify goals for stigma reduction, and monitor progress over time.
Resumen
El estigma relacionado con la profilaxis pre-exposición para la prevención del VIH (PrEP, por sus siglas en inglés) ha sido identificado como un factor que limita la implementación a gran escala de esta efectiva modalidad de prevención del VIH. Para poder cuantificar y caracterizar el estigma relacionado al PrEP, desarrollamos y validamos una breve Escala de Estigma al PrEP (HPSS, por sus siglas en inglés) con un grupo de 279 hombres que tienen sexo con hombres. El desarrollo de la escala se basó en un modelo teórico para optimizar la validez de contenido. Evaluamos dos versiones de la escala, Diferencial Semántico y Likert, alternando aleatoriamente el orden en que se presentaron las escalas a los participantes. Ambas escalas demostraron alta consistencia interna. La escala Likert tuvo una mejor validez de constructo y fue seleccionada como la opción preferencial. Los puntajes de la escala demostraron validez de constructo a través de su asociación con las siguientes construcciones de interés: desconfianza en el sistema de salud, conocimiento acerca del VIH, percepción de la proporción de amigos/compañeros que toman PrEP, percepción de la evaluación comunitaria acerca del PrEP, y percepción de la efectividad del PrEP. La escala representó el 25% de la varianza total de la disposición a tomar PrEP, lo que indica el importante rol que el estigma asociado al PrEP puede tener en la decisión de empezar a tomar PrEP. Dado el aumento de los esfuerzos para implementar PrEP, el contar con una herramienta válida para determinar el nivel y los tipos de estigma relacionado al PrEP en individuos, grupos y comunidades puede ayudar a dar dirección a los planes de implementación, a identificar objetivos para la reducción del estigma y a monitorear el progreso a lo largo del tiempo.
Similar content being viewed by others


Introduction
The use of oral emtricitabine/tenofovir disoproxil fumarate for HIV pre-exposure prophylaxis (PrEP) for men who have sex with men (MSM) has high clinical trial efficacy, providing over 90% protection when the medication is used [1, 2]. Mathematical modeling indicates the promise of PrEP, with one model finding that half of all new HIV infections over a ten-year period could be averted in a population of MSM in the United States if 60% of persons indicated for PrEP were taking the medication with high adherence [3]. Encouragingly, the population-level impact of PrEP is now visible in some settings. In New South Wales, Australia, there was a population-wide 25% decline in new HIV diagnoses after PrEP was made widely and freely available [4].
In the United States, estimates range from 12,000–200,000 individuals taking PrEP in 2017 [5, 6]. Recent gains in increasing PrEP prescriptions may be leveling off, [5] far short of the 1.1 Mio. persons the Centers for Disease Control and Prevention (CDC) estimates are indicated for PrEP [6]. Progress in scaling up PrEP has not been uniform. One metric, the PrEP-to-need ratio, describes disparities in PrEP scale-up by comparing the number of new PrEP prescriptions relative to the number of new HIV diagnoses; the metric identified women, younger persons, and the Southern US region as having low PrEP-to-need ratios [5, 7]. Structural barriers contribute to these disparities; for instance, counties with higher concentrations of residents living in poverty are less likely to have a PrEP-prescribing clinic [9]. Social factors have also been identified as key components limiting PrEP uptake, including relationships with partners, family, and HIV and PrEP stigma [8, 9].
Stigma has been seminally defined by Goffman as a discrediting attribute that leads to “a whole and usual person” to be considered “tainted (and) discounted [10].”Two recent reviews and one meta-analysis identified the stigmatization of PrEP use (hereafter referred to as PrEP stigma) as a barrier to PrEP scale-up [11,12,13]. Individuals that endorsed beliefs stigmatizing PrEP, such as it being “for people who are promiscuous,” were less likely to be interested in taking PrEP [14]. Numerous qualitative studies have identified stigma as a major barrier to accessing and staying on PrEP [8, 15,16,17,18,19].
To best understand PrEP stigma and the ways in which it impacts PrEP decision-making, standardized and validated measurement tools are needed. Past quantitative measurements of PrEP stigma have predominantly consisted of individual belief statements, with each belief statement then assessed for association with PrEP-related outcomes such as willingness to take PrEP [14, 20, 21]. Such items are diverse in content and wording, as well as response format, with some using semantic differential options (unpleasant ….. pleasant) [22] and others using Likert scale options (strongly disagree, disagree, neutral, agree, strongly agree). With known differences in participant preferences, time and cognitive burden, and impact on psychometric properties, [23,24,25,26,27,28,29,30,31] response option types used in items and scales assessing PrEP stigma are also important to consider.
Given that stigma may be a substantial barrier to the expanded use of PrEP, there is a need for a validated stigma scale. Based on a stigma theory [32] and with attention to an optimal response option strategy, we developed and evaluated a brief measure of PrEP Stigma- the HIV PrEP Stigma Scale (HPSS).
Methods
Participants
Eligible participants were aged 18 or older, male at birth, HIV negative by self-report, and had anal sex with a man in the last 12 months. To prevent fraudulent completions, IP addresses were used to remove duplicate survey responses. Participants were recruited with online banner advertisements on Facebook, a method that does not produce substantially more biased recruitment for MSM than alternative recruitment methods such as venue-based, time–space sampling [33]. Banner advertisements were clicked by 4,137 persons, 1,186 of whom consented to be screened. After completing the eligibility form, 408 were eligible to participate. Among the 393 individuals that consented to participate, 279 completed the survey and were included in the analysis dataset. Consent, screening, and survey activities were conducted on an electronic, HIPAA-compliant survey platform. The study was approved by the Emory University Institutional Review Board, Protocol Number 00,092,291.
Measures
Scale Development
To develop the HPSS, we reviewed literature regarding PrEP stigma and identified key sources for items: a study of stigma as a multidimensional barrier, [34] studies of barriers and facilitators to PrEP acceptability, [35, 36] measures from the Adolescent Medicine HIV Trials Network for HIV/AIDS Interventions (ATN) U19 Scale It Up, [37, 38] and measures from an HIV Prevention Trials Network Study, HPTN082 [39, 40]. We sought to include studies representing a broad range of characteristics; in total, there were 1586 participants in these studies, including 402 men, 1171 women, and 7 transgender men; 824 heterosexual, 140 bisexual, and 154 gay/homosexual persons; 666 Black, 250 White, 184 Latino, and 13 Asian; and 400 participants from international settings. These numbers do not represent the full range of the data because not all variables were reported, and not all studies have initiated or completed data collection. Each study reported age differently, yet there was a wide range of ages, with some studies focused on adolescent participation and others on adult participation.
In assessing HPSS measures across these sources, we identified three predominant themes: shame regarding PrEP use, character judgements of people on PrEP, and perceived social support for taking PrEP. In order to develop a diverse set of items, we adapted existing items to address the domains of a stigma framework, comprising internal, anticipated, and experienced stigma [32]. Within each domain, we sought to have at least one item represent one of three attributes of PrEP stigma we discovered in the literature: shame regarding PrEP use, character judgements of people on PrEP, and perceived social support for taking PrEP (Supplement 1). We limited the total number of items on the scale to a small number to facilitate use of the scale in a broad range of settings such as implementation science, program evaluation, and clinical trials research.
Variables Hypothesized to Correlate with PrEP
To assess construct validity, we tested a set of a priori hypotheses that the Semantic Differential and Likert HPSS would correlate with each of six constructs. Higher levels of PrEP stigma were anticipated to positively correlate with healthcare distrust and negatively correlate with HIV knowledge, willingness to be on PrEP, proportion of friends/partners on PrEP, community evaluation of PrEP, and perceived PrEP effectiveness. The full text of the survey instrument, including all demographic items and constructs detailed below, are provided in Supplement 2.
Healthcare distrust was measured with the Health Care System Distrust scale, a 10-item validated instrument that assesses domains such as perceptions of healthcare system honesty and competence [41].
HIV knowledge was measured using an 8-item scale from the SHIPP study, developed to incorporate more current understandings of HIV prevention [42]. Questions included more traditional items such as, “the risk for getting HIV is very low when having oral sex” as well as less traditional knowledge items such as, “Nearly all HIV transmission comes from having lots of boyfriends or hook-ups.”
Willingness to be on PrEP was measured with an item from the ATN, “How likely would you be to take PrEP in the future?” with Likert response options ranging from very unlikely to very likely [43].
Perceived proportion of friends/partners on PrEP was a measure created for this study, assessed by taking the mean of two slider-scale items with a response range of 0–100%: “What proportion of your (‘friends’ OR ‘current and past sexual partners’) are currently taking PrEP?”.
Community evaluation of PrEP was assessed with an item developed for this study: “In general, does your community have a positive attitude toward PrEP?” with response options of “Yes”, “No,” and “Unsure.”
Perceived PrEP effectiveness was measured with an item from the American Men’s Internet Survey (AMIS): “How effective is PrEP at preventing HIV infection if a person takes their pills every day?” with response options of > 90%, 75–89%, 50–74%, 35–49%, 20–34%, and < 20% [44].
We classified individuals as being eligible for PrEP based on an abbreviation of CDC eligibility criteria we have used previously [45, 46]: HIV negative status and meeting at least one of criteria (1, 2, or 3): (1) had sex with men (not in a monogamous relationship with an HIV-negative partner) and (a) has been diagnosed with an STI and/or (b) had condomless anal sex in the last 6 months, (2) is in an ongoing sexual relation with an HIV-positive partner, and/or (3) injected drugs and (a) shared injection or drug preparation equipment and/or (b) participated in methadone, buprenorphine, or suboxone treatment program in the last 6 months.
Statistical Analyses
Descriptive statistics of the study sample are presented, followed by an exploratory factor analysis based on maximum likelihood with Promax rotation to determine whether the Semantic Differential HPSS or the Likert HPSS had latent constructs. A cut-off of < 0.4 was adopted to indicate poor factor loadings. Scree plots of Eigenvalues were used to determine the number of factors in each scale. Cronbach’s alpha was used to assess internal consistency reliability of the overall scale. For analyses of scale performance, only participants completing at least 50% of scale items were included. This approach to missing data resulted in excluding a small number of participants for Likert scale assessments (n = 15, 5%) and a larger number of participants for Semantic Differential scale assessments (n = 79, 28%). A number of sensitivity analyses were conducted to determine the impact of missing data (Supplements 5–7), finding no substantial changes in study conclusions. In Table 3, Pearson’s correlation coefficients (r) were used to assess construct validity of the Likert HPSS. Table 4 displays the mean, standard deviation, and beta estimates from bivariate and multiple linear regression models of the Likert HPSS score predicted by a number of socio-demographic and other PrEP-related characteristics. All analyses were performed in SAS 9.4
Results
From June 8th 2018 to June 14th 2018, 279 participants were enrolled in the study, and their demographic data are presented in Table 1, stratified by the randomized order in which they received the two scale versions. Participants were from 40 different states across the United States, with median 4 participants per state and range 1 to 21 (Supplement 3). Participants were predominantly white (85%), with fewer identifying as Latino (8%), Black (2%), Asian (2%), or multiracial/other (4%). The majority identified as gay (80%). Participants were 13% aged 18–24, 15% aged 25–34, 18% aged 35–49, and 53% aged 50 and above. Over half had college education or higher (61%), and earned greater than $50,000 annually (57%). A minority of participants (9%) were currently taking PrEP.
Factor analysis of each scale indicated unidimensionality, based on scree plots of Eigenvalues (Supplement 4). Each scale had a single item with a factor loading below 0.4, indicating poor item fit; these two items were removed from all subsequent analyses (Table 2). All remaining items had factor loadings and item-rest correlations above the commonly used threshold of 0.4 [47]. Cronbach’s alpha values indicated high internal consistency, with Semantic Differential 0.88 and Likert 0.82.
Overall, the sample reported low- to moderate-levels of PrEP stigma (Table 2). Scales were coded such that higher values equate to higher levels of stigma. Most participants completed at least half of Semantic Differential items (200/279, 72%), but a greater proportion completed at least half of Likert items (264/279, 95%). Randomization order did not significantly influence rates of item completion; for full detail regarding missingness by item, see Supplements 5 and 6. The overall mean Semantic Differential score was 2.97 on a 7-point scale, approximately 15% (1-point) below the midpoint of the range. The overall Likert scale mean was 2.59 on a 5-point scale, equating to a value slightly closer to neutral (3) than to disagree (2), approximately 8% (0.41/5.0 scale points) below the midpoint.
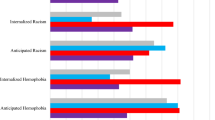
Figure 1 shows the percent distribution of participants’ responses to Likert scale items. Notably, for the majority of items, less than 15% of individuals had responses categorized as stigmatizing. Conversely, many agreed that individuals on PrEP receive praise (65%), are taking care of their health (89%), and that their friends would be supportive (69%). In fact, half would feel proud to take PrEP. Yet substantial minorities held stigmatizing views: being ashamed to take PrEP in front of others (13%) or anticipating problems with sex partners (17%), being seen by others as slutty (21%) or negative judgment (31%). The mixed views regarding PrEP stigma is perhaps best demonstrated by neutral being the most commonly-selected scale category for stigmatizing statements.

Participant agreement with HIV PrEP Stigma Scale (HPSS) items. *Green indicates non-stigmatizing responses, red indicates stigmatizing responses (Color figure online)
The Semantic Differential HPSS was correlated with 2 out of 6 hypothesized variables: willingness to be on PrEP and perceived PrEP effectiveness (Table 3). Both relationships were correlated in the expected direction. The strength of these relationships, based on Cohen’s guidance for interpreting correlation coefficients, was small [48]. The Likert HPSS was correlated with 5 out of 6 hypothesized variables, each in the expected direction. Mistrust in the health care system was correlated with Likert HPSS responses in the expected direction, but was not statistically significant. The strength of the statistically significant correlations with hypothesized variables was small for 1, moderate for 3, and strong for 1. The scale accounted for 25% of the overall variance for the strongly correlated construct, willingness to be on PrEP. A sensitivity analysis in Supplement 7 varied missing data criteria assumptions for Table 3, but identified no substantial differences.
We assessed whether the Likert HPSS correlated with demographic or other sexual behavior variables and found few associations (Table 4). In unadjusted models, sexual orientation, PrEP use (current or past), and recent STI diagnosis were associated with PrEP stigma. In adjusted models, the same set of variables and income were associated with PrEP stigma. Participants who reported PrEP use had lower PrEP stigma scores by 0.52 and 0.53 points, respectively, compared to those who did not.
Discussion
We developed and validated a PrEP stigma scale, the HPSS. In an assessment of Semantic Differential and Likert HPSS versions, both demonstrated face validity by covering key domains in the literature, indicated internal consistency through high Cronbach’s alpha values, and had unidimensionality. The Likert HPSS substantially outperformed the Semantic Differential scale in terms of construct validity, correlating with 5 out of 6 variables hypothesized to be associated with PrEP stigma. It also performed better in terms of completion rates, likely indicating higher acceptability. Of particular relevance to public health programs, the scale accounted for 25% of the variance in participants’ willingness to be on PrEP and 17% of the variance in participants’ perceptions of community attitudes towards PrEP. The strength of these associations indicates that further research regarding PrEP stigma is merited, particularly to better understand the relation between PrEP stigma and willingness to initiate PrEP. This call for further research to develop stigma reduction interventions has been echoed in several recent reviews of PrEP stigma [11,12,13].
Overall, PrEP stigma was low-moderate in the sample, with the average median HPSS item response slightly closer to neutral than to disagree for the Likert responses, in which higher values indicated more stigma. A slight majority of participants indicated they would be proud to take PrEP, and strong majorities anticipated support from their friends and families for taking PrEP. Yet a minority of participants anticipated negative consequences, such as being perceived negatively by doctors, experiencing negative judgements, or having problems with sex partners. Despite the relatively moderate levels of overt PrEP stigma, having higher stigma score was strongly associated with lower willingness to take PrEP. Similarly, in a recent study, believing that ‘PrEP is for promiscuous people’ was found to be associated with lower interest in PrEP among black and white MSM in the Southeastern US [14].
The majority of previously published work identified no difference between performance of Semantic Differential and Likert scales, [25,26,27,28,29,30] yet some studies found Semantic labeling increased performance [23, 24, 30] There are several possible reasons that the Likert scale in our study items outperformed the Semantic Differential scale. First, it was difficult to translate more complex logic of Likert items into the simplified Semantic Differential format we were using. Second, we selected a transformation of items from Likert to Semantic that required greater changes to item wording than some prior studies. These prior studies used nearly identical wording for both scales, changing only the response format. We opted for a more condensed Semantic scale, using a single stem for all items (People taking PrEP are …). Higher completion rates for Likert items relative to Semantic Differential items may indicate that such items are more acceptable or interpretable, which conforms to previous findings that participants prefer Likert scale formats [31]. Last, it is possible that the performance across different response formats depends on the specific domains of assessment. Regardless of the reason for the difference, the substantial performance difference identified in this study argues for more use of head-to-head comparisons of scale response formatting.
HPSS was designed based on a stigma framework with three domains (internal, anticipated, and experienced stigma) and on three attributes abstracted from PrEP stigma literature (shame, character judgments, social support), yet our factor analysis revealed a unidimensional scale. The three dimension stigma framework has been validated for HIV stigma for people living with HIV [49, 50] and for substance abuse stigma for people who have substance abuse histories [51]. There are several notable differences between this study and past research. PrEP is a protective behavior, rather than a disease or disorder, potentially influencing scale dimensionality. The HPSS was designed to accommodate both those using and not using PrEP, so responses may be formulated based on various sources: personal experience on PrEP, observed experiences of others on PrEP, discussion among friends/community, online information/discussions, or even supposition. In a sample solely consisting of individuals possessing the stigmatizing trait (PrEP users), responses would likely be primarily based on personal experience and might be multidimensional. Our sample did not include a sufficient number of PrEP users (n = 25) to perform a separate validation with that group. Future work with PrEP users should be conducted to determine if unique subscales emerge and relate to other important outcomes. Regardless of latent constructs, using the stigma framework to structure development of the scale held substantial value by facilitating content validity: ensuring that our items covered diverse topics from different vantages. We found utility for each scale item, with item-rest correlations well above a threshold indicating irrelevance (0.3) and well below a threshold indicating excessive overlap with other items (0.9).
A recently published study among MSM in Chicago developed a PrEP stigma scale and found that Black participants and participants in geographic areas with higher concentrations of HIV incidence had higher levels of PrEP stigma [52]. The scale developed for the Chicago study was published after data collection finished for the present study. There are, however, some key benefits of the scale presented in our study. Most importantly, our study thoroughly assessed construct validity and determined the scale to perform well based on that assessment; the prior scale had no stated assessment of validity. The current study also assessed scale performance across two versions, with findings leading to identification of a scale that substantially outperformed its competitor. It is important to note that there was considerable overlap in item topics across the two scales, including promiscuity, responsibility, and daily use, indicating face validity for each instrument. Future studies may be useful to further assess the relative performance of the two scales.
This study has a number of limitations. First, the sample was majority White and older, and only included MSM; the scale may not perform similarly in other settings. This concern is partially mitigated by the diverse source of studies that provided items that comprise the scale. These studies totaled over 1500 participants, and represented substantial diversity across age, gender, sexual orientation, race, and nationality. We anticipate that the scale will likely perform well across diverse settings, however, future research is needed to provide additional validation across other groups and settings. We are currently investigating how the scale will perform in a study that targets recruitment of over 190 Black MSM in urban areas, [53] and also in a study that targets recruitment of over 120 Latino MSM or Black MSM in rural areas [54]. It is important to note that for the present study, although we did not observe significant differences in mean scale scores by race/ethnicity, we did not have sufficient sample size to adequately assess potential areas of difference. Last, the sample size did not allow for conduct of confirmatory factor analysis: a future assessment should consider confirmatory factor analysis of the scale.
We developed and validated a PrEP stigma scale that is strongly correlated with willingness to be on PrEP. Having a uniform and validated measurement tool, such as the one presented here, can facilitate improved assessment of the impact of PrEP stigma on PrEP initiation and maintenance in care. Moreover, such measurement can help track trends across populations. Goffman notes that, “an attribute that stigmatizes one type of possessor can confirm the usualness of another … stigma then is a relationship between attribute and stereotype.” [10] PrEP is an excellent example of this: PrEP use (attribute) is stigmatized in some communities (negative stereotype), but considered beneficial (positive stereotype) in others [15]. Ongoing assessment of PrEP stigma may help us better understand its influence on PrEP adoption, a potentially vital step in bringing PrEP to scale to dramatically reduce new HIV infections.
References
Grant RM, Lama JR, Anderson PL, et al. Preexposure chemoprophylaxis for HIV prevention in men who have sex with men. N Engl J Med. 2010;363(27):2587–99.
Anderson PL, Glidden DV, Liu A, et al. Emtricitabine-tenofovir concentrations and pre-exposure prophylaxis efficacy in men who have sex with men. Sci Transl Med. 2012;4(151):151ra125–ra125.
Jenness SM, Goodreau SM, Rosenberg E, et al. Impact of the Centers for Disease Control's HIV Preexposure Prophylaxis Guidelines for Men Who Have Sex With Men in the United States. J Infect Dis. 2016;214(12):1800–7.
Grulich AE, Guy R, Amin J, et al. Population-level effectiveness of rapid, targeted, high-coverage roll-out of HIV pre-exposure prophylaxis in men who have sex with men: the EPIC-NSW prospective cohort study. The lancet HIV. 2018;5(11):e629–e637637.
Sullivan PS, Mera Giler R, Mouhanna F, et al. Trends in active prescriptions of emtricitabine/tenofovir disoproxil fumarate for pre-exposure prophylaxis against HIV infections, United States, 2012–2016. Ann Epidemiol. 2018;28(12):833–40.
Smith DK, Van Handel M, Grey J. Estimates of adults with indications for HIV pre-exposure prophylaxis by jurisdiction, transmission risk group, and race/ethnicity, United States, 2015. Ann Epidemiol. 2018;28(12):850–857.e859.
Siegler AJ, Mouhanna F, Giler RM, et al. The prevalence of pre-exposure prophylaxis use and the pre-exposure prophylaxis-to-need ratio in the fourth quarter of 2017, United States. Ann Epidemiol. 2018;28(12):841–9.
Arnold T, Brinkley-Rubinstein L, Chan P, et al. Social, structural, behavioral and clinical factors influencing retention in Pre-Exposure Prophylaxis (PrEP) care in Mississippi. PLoS ONE. 2017;12(2):e0172354.
Lockard A, Rosenberg ES, Sullivan PS, et al. Contrasting self-perceived need and guideline-based indication for HIV pre-exposure prophylaxis among young, black men who have sex with men offered pre-exposure prophylaxis in Atlanta. Georgia AIDS Patient Care STDS. 2019;33(3):112–9.
Goffman E. Stigma: notes on the management of spoiled identity. New York: Simon and Schuster; 2009.
Golub SA. PrEP Stigma: implicit and explicit drivers of disparity. Curr HIV/AIDS Rep. 2018;15(2):190–7.
Calabrese SK, Underhill K. How stigma surrounding the use of HIV preexposure prophylaxis undermines prevention and pleasure: a call to destigmatize "truvada whores". Am J Public Health. 2015;105(10):1960–4.
Peng P, Su S, Fairley CK, et al. A global estimate of the acceptability of pre-exposure prophylaxis for HIV among men who have sex with men: a systematic review and meta-analysis. AIDS Behav. 2018;22(4):1063–74.
Eaton LA, Kalichman SC, Price D, Finneran S, Allen A, Maksut J. Stigma and conspiracy beliefs related to pre-exposure prophylaxis (PrEP) and interest in Using PrEP among black and white men and transgender women who have sex with men. AIDS Behav. 2017;21(5):1236–46.
Grace D, Jollimore J, MacPherson P, Strang MJP, Tan DHS. The Pre-exposure prophylaxis-stigma paradox: learning from Canada's first wave of PrEP users. AIDS Patient Care STDS. 2018;32(1):24–30.
Cahill S, Taylor SW, Elsesser SA, Mena L, Hickson D, Mayer KH. Stigma, medical mistrust, and perceived racism may affect PrEP awareness and uptake in black compared to white gay and bisexual men in Jackson, Mississippi and Boston, Massachusetts. AIDS Care. 2017;29(11):1351–8.
Franks J, Hirsch-Moverman Y, Loquere AS Jr, et al. Sex, PrEP, and stigma: experiences with HIV Pre-exposure prophylaxis among new York city MSM participating in the HPTN 067/ADAPT study. AIDS Behav. 2018;22(4):1139–49.
Schwartz J, Grimm J. Stigma communication surrounding PrEP: the experiences of a sample of men who have sex with men. Health communication. 2019;34(1):84–90.
Brooks RA, Landrian A, Nieto O, Fehrenbacher A. Experiences of anticipated and enacted pre-exposure prophylaxis (PrEP) stigma among Latino MSM in Los Angeles. AIDS Behav. 2019;23:1964.
Lelutiu-Weinberger C, Golub SA. Enhancing PrEP access for Black and Latino men who have sex with men. JAIDS J Acquir Immune Defic Syndr. 2016;73(5):547–55.
Biello KB, Oldenburg CE, Mitty JA, et al. The "safe sex" conundrum: anticipated stigma from sexual partners as a barrier to PREP use among substance using MSM engaging in transactional sex. AIDS Behav. 2017;21(1):300–6.
Dawes J. Do data characteristics change according to the number of scale points used? An experiment using 5-point, 7-point and 10-point scales. International journal of market research. 2008;50(1):61–104.
Friborg O, Martinussen M, Rosenvinge JH. Likert-based vs semantic differential-based scorings of positive psychological constructs: a psychometric comparison of two versions of a scale measuring resilience. Personality and Individual Difference. 2006;40(5):873–84.
McLeod A, Pippin S, Wong JA. Revisiting the likert scale: can the fast form approach improve survey research? Int J Behav Account Financ. 2011;2(3–4):310–27.
Schibeci R. Measuring student attitudes: semantic differential or likert instruments? Sci Educ. 1982;66(4):565–70.
Dixon PN, Bobo M, Stevick RA. Response differences and preferences for all-category-defined and end-defined Likert formats. Educ Psychol Measur. 1984;44(1):61–6.
Krosnick JA, Fabrigar LR. Designing rating scales for effective measurement in surveys. Survey Meas Proc Qual. 1997;1997:141–64.
Menezes D, Elbert NF. Alternative semantic scaling formats for measuring store image: an evaluation. J Mark Res. 1979;16(1):80–7.
Matz-Costa C, James JB, Ludlow L, Brown M, Besen E, Johnson C. The meaning and measurement of productive engagement in later life. Soc Indic Res. 2014;118(3):1293–314.
Chin WW, Johnson N, Schwarz A. A fast form approach to measuring technology acceptance and other constructs. MIS Quart. 2008;32(4):687–703.
Herek GM, Cogan JC, Gillis JR, Glunt EK. Correlates of internalized homophobia in a community sample of lesbians and gay men. J Gay Lesbian Med Assoc. 1997;2:17–25.
Earnshaw VA, Chaudoir SR. From conceptualizing to measuring HIV stigma: a review of HIV stigma mechanism measures. AIDS Behav. 2009;13(6):1160–77.
Hernandez-Romieu AC, Sullivan PS, Sanchez TH, et al. The comparability of men who have sex with men recruited from venue-time-space sampling and facebook: a cohort study. JMIR Res Protoc. 2014;3(3):e37.
Calabrese SK, Dovidio JF, Tekeste M, et al. HIV pre-exposure prophylaxis stigma as a multidimensional barrier to uptake among women who attend planned parenthood. J Acquir Immune Defic Syndr. 2018;79(1):46–53.
Golub SA, Gamarel KE, Rendina HJ, Surace A, Lelutiu-Weinberger CL. From efficacy to effectiveness: facilitators and barriers to PrEP acceptability and motivations for adherence among MSM and transgender women in New York City. AIDS Patient Care STDs. 2013;27(4):248–54.
Whiteside YO, Harris T, Scanlon C, Clarkson S, Duffus W. Self-perceived risk of HIV infection and attitudes about preexposure prophylaxis among sexually transmitted disease clinic attendees in South Carolina. AIDS Patient Care STDS. 2011;25(6):365–70.
Naar S, Parsons JT, Stanton BF. Adolescent trials network for HIV-AIDS scale it up program: protocol for a rational and overview. JMIR Res Protoc. 2019;8(2):e11204.
Parsons JT, Starks T, Gurung S, Cain D, Marmo J, Naar S. Clinic-Based Delivery of the Young Men's Health Project (YMHP) Targeting HIV risk reduction and substance use among young men who have sex with men: protocol for a type 2, hybrid implementation-effectiveness trial. JMIR Res Protoc. 2019;8(5):e11184.
Celum C, Delany-Moretlwe S, Hosek S, et al. Risk behavior, perception, and reasons for PrEP among young African women in HPTN 082. Age. 2018;21:25.
Velloza J. The influence of HIV-related stigma on PrEP disclosure and adherence over time among AGYW in HPTN 082. International conference on HIV treatment and prevention Adherence; June 18, 2019; Miami, Florida, USA.
Rose A, Peters N, Shea JA, Armstrong K. Development and testing of the health care system distrust scale. J Gen Intern Med. 2004;19(1):57–63.
US Centers for Disease Control and Prevention Foundation. (2019) Sustainable Health Center Implementation PrEP Pilot (SHIPP) Study: NCT02074891. https://www.cdcfoundation.org/what/program/sustainable-health-center-implementation-prep-pilot-shipp-study. Accessed June 24, 2019.
Gamarel KE, Darbes LA, Hightow-Weidman L, Sullivan P, Stephenson R. The development and testing of a relationship skills intervention to improve HIV prevention uptake among young gay, bisexual, and other men who have sex with men and their primary partners (We Prevent): research protocol (ATN 157). JMIR Res Protoc. 2019;8:e10370.
Zlotorzynska M, Sullivan P, Sanchez T. The annual american men's internet survey of behaviors of men who have sex with men in the united states: 2016 key indicators report. JMIR Public Health Surveill. 2019;5(1):e11313.
Centers for Disease Control and Prevention. US Public Health Service: Preexposure prophylaxis for the prevention of HIV infection in the United States—2017 Update: a clinical practice guideline. 2018.
Bratcher A, Schlueter Wirtz S, Siegler AJ. Users of a national directory of PrEP service providers: beliefs, self-efficacy, and progress toward prescription. JAIDS J Acquir Immune Defic Syndr. 2018;78(4):e28–e30.
Loiacono ET, Watson RT, Goodhue DL. WebQual: a measure of website quality. Market Theory Appl. 2002;13(3):432–8.
Cohen J. Statistical power analysis for the behavioral sciences. London: Routledge; 2013.
Reinius M, Wiklander M, Wettergren L, Svedhem V, Eriksson LE. The relationship between stigma and health-related quality of life in people living with HIV who have full access to antiretroviral treatment: an assessment of earnshaw and chaudoir's HIV stigma framework using empirical data. AIDS Behav. 2018;22(12):3795–806.
Earnshaw VA, Smith LR, Chaudoir SR, Amico KR, Copenhaver MM. HIV stigma mechanisms and well-being among PLWH: a test of the HIV stigma framework. AIDS Behav. 2013;17(5):1785–95.
Smith LR, Earnshaw VA, Copenhaver MM, Cunningham CO. Substance use stigma: reliability and validity of a theory-based scale for substance-using populations. Drug Alcohol Depend. 2016;162:34–433.
Mustanski B, Ryan DT, Hayford C, Phillips G 2nd, Newcomb ME, Smith JD. Geographic and individual associations with PrEP stigma: results from the RADAR cohort of diverse young men who have sex with men and transgender women. AIDS Behav. 2018;22(9):3044–56.
Clinicaltrials.gov. (2019) Pre-exposure Prophylaxis (PrEP) at Home (PrEP@Home): NCT03569813. https://clinicaltrials.gov/ct2/show/NCT03569813. Accessed March 19, 2019.
Siegler AJ, Brock JB, Hurt CB, et al. An electronic pre-exposure prophylaxis initiation and maintenance home care system for nonurban young men who have sex with men: protocol for a randomized controlled trial. JMIR Res Protoc. 2019;8(6):e13982.
Acknowledgements
The authors would like to thank all study participants, who generously gave their time and efforts for this research. The research reported in this publication was supported by the National Institute of Mental Health R01MH114692 and by the Eunice Kennedy Shriver National Institute of Child Health and Human Development of the NIH (Grant No. U19HD089881), under ATN protocol 159. The research was facilitated by the Emory Center for AIDS Research (Grant No. P30AI050409). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Siegler, A.J., Wiatrek, S., Mouhanna, F. et al. Validation of the HIV Pre-exposure Prophylaxis Stigma Scale: Performance of Likert and Semantic Differential Scale Versions. AIDS Behav 24, 2637–2649 (2020). https://doi.org/10.1007/s10461-020-02820-6
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10461-020-02820-6