Covariates and Spatial Interpolation of HIV Screening in Mozambique: Insight from the 2015 AIDS Indicator Survey

 , , , ,
, , , ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Study Sample
2.2. Measures
2.2.1. Outcome
2.2.2. Explanatory Variables
2.3. Data Analysis
2.3.1. Spatial Interpolation of HIV Prevalence
2.3.2. Ethical Consideration
3. Results
3.1. Sample Characteristics
3.2. Chi-Square Test of Independence between the Covariates and the Outcome
3.3. Sociodemographic and Sexual Behavioural Factors Regressed on HIV Screening Status
3.4. Gender Modifies the Association between Each Covariate and HIV Screening
3.5. Drivers of HIV Testing in a Gender-Stratified Multivariate Model
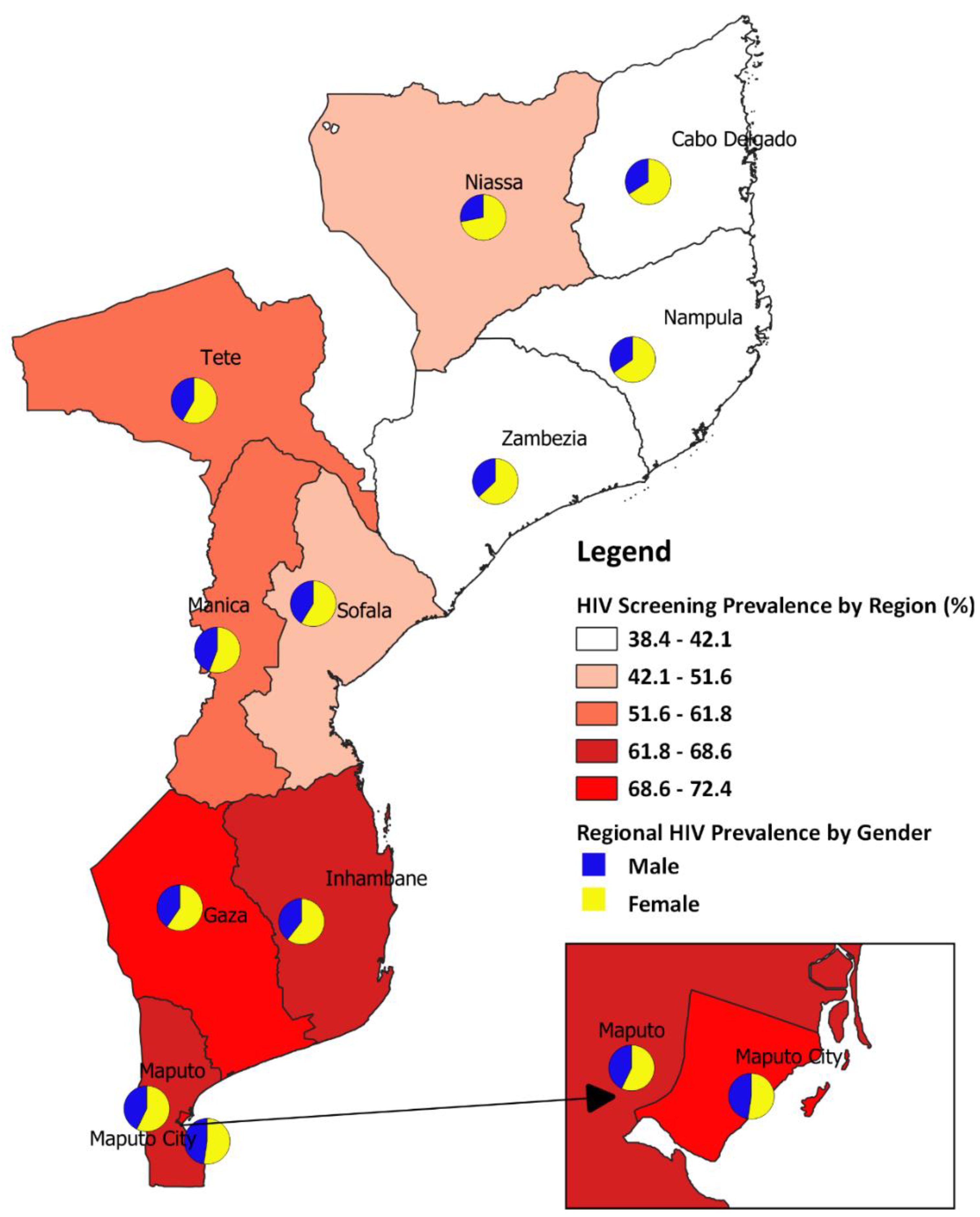
3.6. Spatial Map of Mozambique Showing Provincial HIV Screening Prevalence by Gender
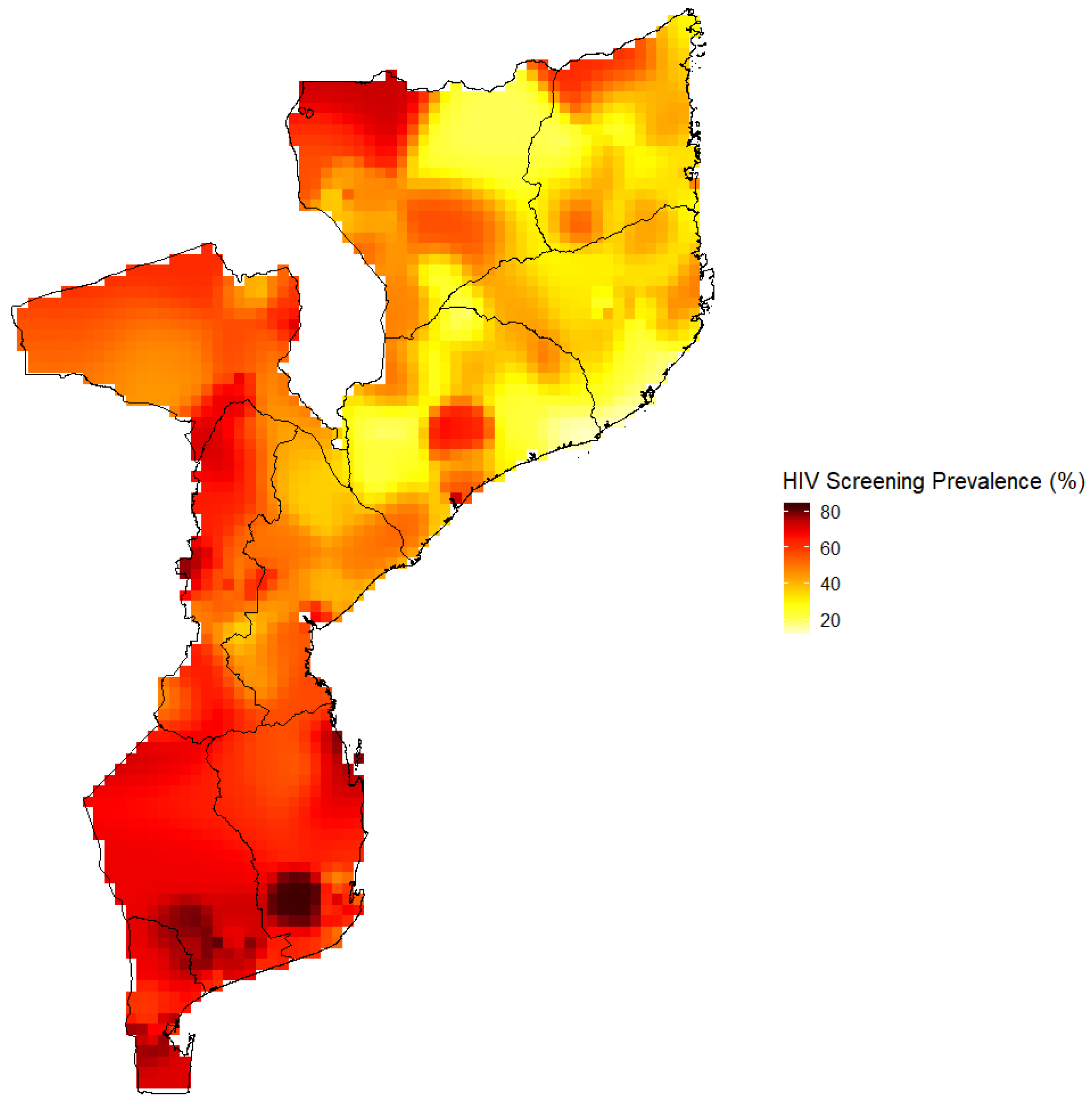
3.7. HIV Screening Prevalence in Mozambique Estimated by the Kernel Estimator Approach
4. Discussion
5. Strengths and Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- UNAIDS. UNAIDS Data 2018. Available online: https://www.unaids.org/en/resources/documents/2018/unaids-data-2018 (accessed on 10 January 2020).
- World Health Organization. HIV/AIDS: Data and Statistics. Available online: https://www.who.int/hiv/data/en/ (accessed on 10 August 2019).
- World Health Organization. HIV/AIDS Fact Sheet. Available online: https://www.who.int/en/news-room/fact-sheets/detail/hiv-aids (accessed on 25 November 2019).
- UNAIDS. Global HIV & AIDS Statistics—2019 Fact Sheet. Available online: https://www.unaids.org/en/resources/fact-sheet (accessed on 16 June 2020).
- Bovbjerg, M.L. Foundations of Epidemiology; Open Text Library: Corvallis, OR, USA, 2019. [Google Scholar]
- Shearer, F.M.; Moss, R.; McVernon, J.; Ross, J.V.; McCaw, J.M. Infectious disease pandemic planning and response: Incorporating decision analysis. PLoS Med. 2020, 17, e1003018. [Google Scholar] [CrossRef]
- Macicame, I.; Bhatt, N.; Matavele Chissumba, R.; Eller, L.A.; Viegas, E.; Araújo, K.; Nwoga, C.; Li, Q.; Milazzo, M.; Hills, N.K. HIV prevalence and risk behavior among male and female adults screened for enrolment into a vaccine preparedness study in Maputo, Mozambique. PLoS ONE 2019, 14, e0221682. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joint Untied Nations Programme on HIV/AIDS (UNAIDS). 90-90-90 an Ambitious Treatment Target to Help End the AIDS Epidemic. 2014. Available online: https://www.unaids.org/sites/default/files/media_asset/90-90-90_en.pdf (accessed on 10 December 2019).
- Levi, J.; Raymond, A.; Pozniak, A.; Vernazza, P.; Kohler, P.; Hill, A. Can the UNAIDS 90-90-90 target be achieved? A systematic analysis of national HIV treatment cascades. BMJ Glob. Health 2016, 1, e000010. [Google Scholar] [CrossRef] [Green Version]
- Martins-Fonteyn, E.; Loquiha, O.; Baltazar, C.; Thapa, S.; Boothe, M.; Raimundo, I.; Hens, N.; Aerts, M.; Meulemans, H.; Degomme, O. Factors influencing risky sexual behaviour among Mozambican miners: A socio-epidemiological contribution for HIV prevention framework in Mozambique. Int. J. Equity Health 2017, 16, 179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Audet, C.M.; Burlison, J.; Moon, T.D.; Sidat, M.; Vergara, A.E.; Vermund, S.H. Sociocultural and epidemiological aspects of HIV/AIDS in Mozambique. BMC Int. Health Hum. Rights 2010, 10, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Korenromp, E.L.; Gobet, B.; Fazito, E.; Lara, J.; Bollinger, L.; Stover, J. Impact and cost of the HIV/AIDS national strategic plan for Mozambique, 2015–2019—Projections with the Spectrum/Goals Model. PLoS ONE 2015, 10, e0142908. [Google Scholar] [CrossRef]
- John Nutor, J.; Duodu, P.A.; Agbadi, P.; Duah, H.O.; Oladimeji, K.E.; Gondwe, K.W. Predictors of high HIV+ prevalence in Mozambique: A complex samples logistic regression modeling and spatial mapping approaches. PLoS ONE 2020, 15, e0234034. [Google Scholar] [CrossRef]
- Nutor, J.J.; Duah, H.O.; Agbadi, P.; Duodu, P.A.; Gondwe, K.W. Spatial analysis of factors associated with HIV infection in Malawi: Indicators for effective prevention. BMC Public Health 2020, 20, 1167. [Google Scholar] [CrossRef]
- Croft, T.N.; Marshall, A.M.; Allen, C.K.; Arnold, F.; Assaf, S.; Balian, S. Guide to DHS Statistics; ICF: Rockville, MD, USA, 2018. [Google Scholar]
- Larmarange, J.; Vallo, R.; Yaro, S.; Msellati, P.; Méda, N. Methods for mapping regional trends of HIV prevalence from Demographic and Health Surveys (DHS). Cybergeo Eur. J. Geogr. 2011. [Google Scholar] [CrossRef]
- MinistÈrio da Saúde—MISAU; Instituto Nacional de EstatÌstica—INE; ICF. InquÈrito de Indicadores de ImunizaÁ„o, Mal·ria e HIV/SIDA em MoÁambique (IMASIDA) 2015. Available online: http://dhsprogram.com/pubs/pdf/AIS12/AIS12.pdf (accessed on 10 January 2020).
- Amu, E.O.; Olatona, F.A.; Onayade, A.A. Factors influencing HIV counselling and testing uptake among corps members in Osun State, Nigeria. IOSR J. Dent. Med Sci. 2014, 13, 14–19. [Google Scholar] [CrossRef]
- Ajayi, A.I.; Awopegba, O.E.; Adeagbo, O.A.; Ushie, B.A. Low coverage of HIV testing among adolescents and young adults in Nigeria: Implication for achieving the UNAIDS first 95. PLoS ONE 2020, 15, e0233368. [Google Scholar] [CrossRef]
- Staveteig, S.; Croft, T.N.; Kampa, K.T.; Head, S.K. Reaching the ‘first 90’: Gaps in coverage of HIV testing among people living with HIV in 16 African countries. PLoS ONE 2017, 12, e0186316. [Google Scholar] [CrossRef] [Green Version]
- dos Anjos Luis, A.; Cabral, P. Geographic accessibility to primary healthcare centers in Mozambique. Int. J. Equity Health 2016, 15, 173. [Google Scholar] [CrossRef] [Green Version]
- Saúde, I.N.D. Mozambique National Survey on Prevalence, Behavioral Risks and Information about HIV and AIDS. Available online: http://www.measuredhs.com/pubs/pdf/SR179/SR179.pdf (accessed on 25 July 2020).
- Ciampa, P.J.; Skinner, S.L.; Patricio, S.R.; Rothman, R.L.; Vermund, S.H.; Audet, C.M. Comprehensive knowledge of HIV among women in rural Mozambique: Development and validation of the HIV knowledge 27 scale. PLoS ONE 2012, 7, e48676. [Google Scholar] [CrossRef]
- Dellar, R.C.; Dlamini, S.; Karim, Q.A. Adolescent girls and young women: Key populations for HIV epidemic control. J. Int. AIDS Soc. 2015, 18, 19408. [Google Scholar] [CrossRef]
- Wong, V.J.; Murray, K.R.; Phelps, B.R.; Vermund, S.H.; McCarraher, D.R. Adolescents, young people, and the 90–90–90 goals: A call to improve HIV testing and linkage to treatment. AIDS 2017, 31, S191–S194. [Google Scholar] [CrossRef] [Green Version]
- Hosek, S.; Pettifor, A. HIV prevention interventions for adolescents. Curr. HIV/AIDS Rep. 2019, 16, 120–128. [Google Scholar] [CrossRef]
- Kinsler, J.; Sneed, C.D.; Morisky, D.E.; Ang, A. Evaluation of a school-based intervention for HIV/AIDS prevention among Belizean adolescents. Health Educ. Res. 2004, 19, 730–738. [Google Scholar] [CrossRef] [Green Version]
- Fonner, V.A.; Armstrong, K.S.; Kennedy, C.E.; O’Reilly, K.R.; Sweat, M.D. School based sex education and HIV prevention in low-and middle-income countries: A systematic review and meta-analysis. PLoS ONE 2014, 9, e89692. [Google Scholar] [CrossRef]
- Yaya, S.; Oladimeji, O.; Oladimeji, K.E.; Bishwajit, G. Determinants of prenatal care use and HIV testing during pregnancy: A population-based, cross-sectional study of 7080 women of reproductive age in Mozambique. BMC Pregnancy Childbirth 2019, 19, 354. [Google Scholar] [CrossRef] [Green Version]
- Inghels, M.; Kouassi, A.K.; Niangoran, S.; Bekelynck, A.; Carillon, S.; Sika, L.; Danel, C.; Kone, M.; du Loû, A.D.; Larmarange, J. Cascade of Provider-Initiated Human Immunodeficiency Virus Testing and Counselling at Specific Life Events (Pregnancy, Sexually Transmitted Infections, Marriage) in Côte d’Ivoire. Sex. Transm. Dis. 2020, 47, 54–61. [Google Scholar] [CrossRef] [PubMed]
- Luginaah, I.N.; Yiridoe, E.K.; Taabazuing, M.-M. From mandatory to voluntary testing: Balancing human rights, religious and cultural values, and HIV/AIDS prevention in Ghana. Soc. Sci. Med. 2005, 61, 1689–1700. [Google Scholar] [CrossRef] [PubMed]
- Musheke, M.; Ntalasha, H.; Gari, S.; Mckenzie, O.; Bond, V.; Martin-Hilber, A.; Merten, S. A systematic review of qualitative findings on factors enabling and deterring uptake of HIV testing in Sub-Saharan Africa. BMC Public Health 2013, 13, 220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- UNAIDS. Addressing a Blind Spot in the Response to HIV—Reaching Out to Men and Boys; UNAIDS: Geneva, Switzerland, 2017. [Google Scholar]
- Cremin, I.; Cauchemez, S.; Garnett, G.P.; Gregson, S. Patterns of uptake of HIV testing in sub-Saharan Africa in the pre-treatment era. Trop. Med. Int. Health 2012, 17, e26–e37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ante-Testard, P.A.; Benmarhnia, T.; Bekelynck, A.; Baggaley, R.; Ouattara, E.; Temime, L.; Jean, K. Temporal trends in socioeconomic inequalities in HIV testing: An analysis of cross-sectional surveys from 16 sub-Saharan African countries. Lancet Glob. Health 2020, 8, e808–e818. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Ever Screened for HIV | χ2, p-Value | ||
|---|---|---|---|---|
| No | Yes | |||
| n (% a) | n (% b) | n (% b) | ||
| 6172 (47.5) | 6823 (52.5) | |||
| Gender | χ2 = 592.90, p ≤ 0.001 | |||
| Male | 5263 (40.5) | 3180 (60.4) | 2083 (39.6) | |
| Female | 7732 (59.5) | 2992 (38.7) | 4740 (61.3) | |
| Age | χ2 = 811.95, p ≤ 0.001 | |||
| 15–19 | 2587 (19.9) | 1733 (67.0) | 854 (33.0) | |
| 20–24 | 2271 (17.5) | 865 (38.1) | 1407 (61.9) | |
| 25–29 | 1776 (13.7) | 595 (33.5) | 1181 (66.5) | |
| 30–34 | 1532 (11.8) | 583 (38.1) | 949 (61.9) | |
| 35–39 | 1391 (10.7) | 534 (38.4) | 857 (61.6) | |
| 40–44 | 1118 (8.6) | 536 (47.9) | 582 (52.1) | |
| 45–49 | 933 (7.2) | 499 (53.4) | 435 (46.6) | |
| 50+ | 1386 (10.7) | 828 (59.7) | 558 (40.3) | |
| Education | χ2 = 461.91, p ≤ 0.001 | |||
| No formal education | 2744 (21.1) | 1555 (56.7) | 1189 (43.3) | |
| Primary | 6857 (52.8) | 3488 (50.9) | 3369 (49.1) | |
| Secondary | 3110 (23.9) | 1098 (35.3) | 2012 (64.7) | |
| Post-Secondary | 284 (2.2) | 31 (10.9) | 253 (89.1) | |
| Marital status | χ2 = 314.23, p ≤ 0.001 | |||
| Never married | 2744 (21.1) | 1713 (62.4) | 1031 (37.6) | |
| Currently married | 8435 (64.9) | 3702 (43.9) | 4733 (56.1) | |
| Previously married | 1816 (14.0) | 757 (41.7) | 1058 (58.3) | |
| Religion | χ2 = 335.55, p ≤ 0.001 | |||
| Catholic | 3949 (30.4) | 2069 (52.4) | 1880 (47.6) | |
| Protestant Christians | 2545 (19.6) | 1459 (57.3) | 1086 (42.7) | |
| Islam | 5113 (39.3) | 1934 (37.8) | 3178 (62.2) | |
| No religion/others | 1389 (10.7) | 710 (51.2) | 678 (48.8) | |
| Total lifetime sexual partners | χ2 = 650.17, p ≤ 0.001 | |||
| 0 | 851 (6.6) | 737 (86.5) | 115 (13.5) | |
| 1 | 3770 (29.0) | 1527 (40.5) | 2244 (59.5) | |
| 2 | 2770 (21.3) | 1217 (43.9) | 1553 (56.1) | |
| 3–4 | 2653 (20.4) | 1163 (43.8) | 1490 (56.2) | |
| 5–9 | 1450 (11.2) | 776 (53.5) | 674 (46.5) | |
| 10+ | 786 (6.0) | 382 (48.6) | 404 (51.4) | |
| Undisclosed | 713 (5.5) | 371 (52.0) | 343 (48.0) | |
| Had any STI last 12 months | χ2 = 18.83, p ≤ 0.001 | |||
| No | 12,506 (96.2) | 5987 (47.9) | 6519 (52.1) | |
| Yes | 489 (3.8) | 185 (37.8) | 304 (62.2) | |
| Household wealth index | χ2 = 842.83, p ≤ 0.001 | |||
| Poorest | 2431 (18.7) | 1536 (63.2) | 895 (36.8) | |
| Poorer | 2460 (18.9) | 1459 (59.3) | 1001 (40.7) | |
| Middle | 2388 (18.4) | 1230 (51.5) | 1158 (48.5) | |
| Richer | 2576 (19.8) | 992 (38.5) | 1584 (61.5) | |
| Richest | 3140 (24.2) | 956 (30.4) | 2184 (69.6) | |
| Rural/Urban Residence | χ2 = 372.84, p ≤ 0.001 | |||
| Urban | 4769 (36.7) | 1736 (36.4) | 3034 (63.6) | |
| Rural | 8226 (63.3) | 4437 (53.9) | 3789 (46.1) | |
| Province | χ2 = 864.34, p ≤ 0.001 | |||
| Niassa | 705 (5.4) | 374 (53.1) | 330 (46.9) | |
| Cabo Delgado | 1304 (10.0) | 780 (59.8) | 525 (40.2) | |
| Nampula | 2787 (21.4) | 1718 (61.6) | 1069 (38.4) | |
| Zambézia | 1473 (11.3) | 854 (57.9) | 620 (42.1) | |
| Tete | 906 (7.0) | 389 (42.9) | 517 (57.1) | |
| Manica | 929 (7.2) | 355 (38.2) | 574 (61.8) | |
| Sofala | 1222 (9.4) | 591 (48.4) | 631 (51.6) | |
| Inhambane | 838 (6.4) | 294 (35.1) | 544 (64.9) | |
| Gaza | 1059 (8.1) | 292 (27.6) | 767 (72.4) | |
| Maputo Provincia | 838 (6.5) | 263 (31.4) | 575 (68.6) | |
| Maputo Cidade | 933 (7.2) | 262 (28.1) | 671 (71.9) | |
| Characteristics | PR [95% CI of PR] | APR [95% CI of APR] |
|---|---|---|
| Gender | ||
| Male | 1 | 1 |
| Female | 1.55 [1.47, 1.64] | 1.56 [1.49, 1.65] |
| Age | ||
| 15–19 | 1 | 1 |
| 20–24 | 1.88 [1.73, 2.04] | 1.37 [1.27, 1.48] |
| 25–29 | 2.01 [1.86, 2.19] | 1.46 [1.34, 1.58] |
| 30–34 | 1.88 [1.71, 2.06] | 1.40 [1.27, 1.53] |
| 35–39 | 1.87 [1.70, 2.05] | 1.43 [1.31, 1.58] |
| 40–44 | 1.58 [1.42, 1.75] | 1.25 [1.13, 1.38] |
| 45–49 | 1.41 [1.07, 1.38] | 1.10 [1.00, 1.20] |
| 50+ | 1.22 [1.07, 1.38] | 0.96 [0.85, 1.08] |
| Education | ||
| No formal education | 1 | 1 |
| Primary | 1.13 [1.05, 1.22] | 1.19 [1.11, 1.28] |
| Secondary | 1.49 [1.38, 1.62] | 1.50 [1.38, 1.63] |
| Post-Secondary | 2.06 [1.88, 2.25] | 1.86 [1.69, 2.06] |
| Marital status | ||
| Never married | 1 | 1 |
| Currently married | 1.49 [1.39, 1.61] | 1.35 [1.27, 1.42] |
| Previously married | 1.55 [1.42, 1.70] | 1.30 [1.21, 1.40] |
| Religion | ||
| Islam | 1 | 1 |
| Catholic | 1.12 [0.99, 1.26] | 1.04 [0.95, 1.14] |
| Protestant Christians | 1.46 [1.32, 1.61] | 1.06 [0.97, 1.15] |
| No religion/others | 1.14 [1.00, 1.30] | 0.98 [0.88, 1.09] |
| Total lifetime sexual partners | ||
| 0 | 1 | 1 |
| 1 | 4.42 [3.66, 5.34] | 3.04 [2.51, 3.67] |
| 2 | 4.17 [3.44, 5.04] | 2.88 [2.39, 3.47] |
| 3–4 | 4.17 [3.46, 5.03] | 2.94 [2.44, 3.54] |
| 5–9 | 3.46 [2.83, 4.22] | 2.90 [2.39, 3.51] |
| 10+ | 3.82 [3.10, 4.71] | 3.35 [2.73, 4.11] |
| Undisclosed | 3.57 [2.82, 4.52] | 2.89 [2.34, 3.56] |
| Had any STI last 12 months | ||
| No | 1 | 1 |
| Yes | 1.19 [1.10, 1.29] | 1.04 [0.97, 1.12] |
| Household wealth index | ||
| Poorest | 1 | 1 |
| Poorer | 1.11 [1.00, 1.22] | 1.07 [0.98, 1.17] |
| Middle | 1.32 [1.18, 1.47] | 1.19 [1.08, 1.32] |
| Richer | 1.67 [1.52, 1.84] | 1.31 [1.19, 1.45] |
| Richest | 1.89 [1.72, 2.07] | 1.37 [1.22, 1.54] |
| Rural/Urban Residence | ||
| Rural | 1 | 1 |
| Urban | 1.38 [1.30, 1.47] | 1.10 [1.01, 1.19] |
| Province | ||
| Cabo Delgado | 1 | 1 |
| Niassa | 1.17 [0.97, 1.40] | 1.20 [1.01, 1.41] |
| Nampula | 0.95 [0.79, 1.15] | 0.95 [0.82, 1.11] |
| Zambézia | 1.05 [0.83, 1.32] | 1.05 [0.88, 1.27] |
| Tete | 1.42 [1.19, 1.69] | 1.43 [1.23, 1.67] |
| Manica | 1.53 [1.29, 1.83] | 1.42 [1.21, 1.65] |
| Sofala | 1.28 [1.08, 1.53] | 1.18 [1.03, 1.36] |
| Inhambane | 1.61 [1.35, 1.92] | 1.46 [1.24, 1.78] |
| Gaza | 1.80 [1.54, 2.10] | 1.56 [1.36, 1.78] |
| Maputo Provincia | 1.70 [1.46, 1.99] | 1.31 [1.15, 1.49] |
| Maputo Cidade | 1.79 [1.53, 2.09] | 1.31 [1.15, 1.49] |
| Females (n = 7732) | Males (n = 5263) | ||
|---|---|---|---|
| PR [95% CI of PR] | PR [95% CI of PR] | Wald Chi-Square Test | |
| Age | F(15, 271) = 49.75, p < 0.001 | ||
| 15–19 | 1 | 1 | |
| 20–24 | 1.75 [1.60, 1.90] | 2.14 [1.79, 2.56] | |
| 25–29 | 1.75 [1.60, 1.91] | 2.73 [2.29, 3.27] | |
| 30–34 | 1.74 [1.58, 1.91] | 2.35 [1.95, 2.59] | |
| 35–39 | 1.58 [1.42, 1.75] | 2.61 [2.15, 3.17] | |
| 40–44 | 1.37 [1.23, 1.52] | 2.22 [1.77, 2.77] | |
| 45–49 | 1.16 [1.02, 1.32] | 2.16 [1.76, 2.66] | |
| 50+ | 0.92 [0.80, 1.05] | 2.15 [1.72, 2.68] | |
| Education | F( 7, 279) = 120.00, p < 0.001 | ||
| No formal education | 1 | 1 | |
| Primary | 1.28 [1.19, 1.37] | 1.35 [1.06, 1.71] | |
| Secondary | 1.56 [1.44, 1.69] | 2.31 [1.80, 2.97] | |
| Post-Secondary | 1.91 [1.75, 2.08] | 3.68 [2.85, 4.75] | |
| Marital status | F( 5, 281) = 72.35, p < 0.001 | ||
| Never married | 1 | 1 | |
| Currently married | 1.41 [1.30, 1.53] | 1.38 [1.23, 1.54] | |
| Previously married | 1.32 [1.19, 1.46] | 1.48 [1.26, 1.72] | |
| Religion | F(7, 279) = 50.23, p < 0.001 | ||
| Islam | 1 | 1 | |
| Catholic | 1.11 [0.99, 1.24] | 1.12 [0.91, 1.38] | |
| Protestant Christians | 1.33 [1.21, 1.46] | 1.66 [1.37, 2.01] | |
| No religion/others | 1.14 [0.99, 1.31] | 1.31 [1.05, 1.62] | |
| Total lifetime sexual partners | F(13, 273) = 37.91, p < 0.001 | ||
| 0 | 1 | 1 | |
| 1 | 5.87 [4.42, 7.80] | 2.06 [1.55, 2.73] | |
| 2 | 4.92 [4.46, 7.87] | 2.23 [1.71, 2.92] | |
| 3–4 | 6.23 [4.70, 8.26] | 2.61 [2.03, 2.04] | |
| 5–9 | 5.81 [4.24, 7.95] | 2.58 [1.98, 3.35] | |
| 10+ | 5.49 [3.58, 8.43] | 3.15 [2.41, 4.12] | |
| Undisclosed | 6.71 [4.91, 9.16] | 2.59 [1.89, 3.55] | |
| Had any STI last 12 months | F(3, 283) = 102.39, p < 0.001 | ||
| No | 1 | 1 | |
| Yes | 1.30 [1.20, 1.41] | 1.15 [0.97, 1.35] | |
| Household wealth index | F(9, 277) = 68.30, p < 0.001 | ||
| Poorest | 1 | 1 | |
| Poorer | 1.12 [1.01, 1.24] | 1.16 [0.97, 1.40] | |
| Middle | 1.29 [1.15, 1.45] | 1.52 [1.26, 1.82] | |
| Richer | 1.58 [1.43, 1.75] | 2.06 [1.75, 2.42] | |
| Richest | 1.68 [1.52, 1.86] | 2.74 [2.32, 3.24] | |
| Rural/Urban Residence | F(3, 283) = 153.70, p < 0.001 | ||
| Rural | 1 | 1 | |
| Urban | 1.30 [1.22, 1.38] | 1.68 [1.51, 1.88] | |
| Province | F(21, 265) = 29.22, p < 0.001 | ||
| Cabo Delgado | 1 | 1 | |
| Niassa | 1.24 [1.06, 1.45] | 0.94 [0.62, 1.43] | |
| Nampula | 0.93 [0.80, 1.09] | 0.96 [0.63, 1.46] | |
| Zambézia | 0.98 [0.77, 1.25] | 1.11 [0.73, 1.70] | |
| Tete | 1.25 [1.07, 1.47] | 1.74 [1.17, 2.58] | |
| Manica | 1.32 [1.13, 1.53] | 2.01 [1.37, 2.94] | |
| Sofala | 1.14 [0.99, 1.32] | 1.55 [1.05, 2.28] | |
| Inhambane | 1.44 [1.26, 1.65] | 1.82 [1.22, 2.71] | |
| Gaza | 1.59 [1.41, 1.78] | 2.08 [1.41, 3.01] | |
| Maputo Provincia | 1.52 [1.34, 1.71] | 2.20 [1.09, 3.17] | |
| Maputo Cidade | 1.46 [1.30, 1.65] | 2.57 [1.78, 3.72] |
| Females | Males | |
|---|---|---|
| APR [95% CI of APR] | APR [95% CI of APR] | |
| Age | ||
| 15–19 | 1 | 1 |
| 20–24 | 1.31 [1.21, 1.42] | 1.75 [1.44, 2.12] |
| 25–29 | 1.33 [1.23, 1.45] | 2.19 [1.74, 2.74] |
| 30–34 | 1.32 [1.20, 1.45] | 2.05 [1.63, 2.59] |
| 35–39 | 1.25 [1.14, 1.38] | 2.49 [1.96, 3.16] |
| 40–44 | 1.07 [0.96, 1.20] | 2.23 [1.73, 2.87] |
| 45–49 | 0.91 [0.81, 1.02] | 2.11 [1.66, 2.69] |
| 50+ | 0.73 [0.64, 0.84] | 2.02 [1.56, 2.61] |
| Education | ||
| No formal education | 1 | 1 |
| Primary | 1.20 [1.12, 1.28] | 1.27 [1.04, 1.56] |
| Secondary | 1.33 [1.23, 1.44] | 1.93 [1.54, 2.41] |
| Post-Secondary | 1.49 [1.35, 1.65] | 2.29 [1.83, 2.87] |
| Marital status | ||
| Never married | 1 | 1 |
| Currently married | 1.24 [1.17, 1.31] | 1.21 [1.08, 1.36] |
| Previously married | 1.24 [1.15, 1.34] | 1.09 [0.92, 1.28] |
| Religion | ||
| Islam | 1 | 1 |
| Catholic | 1.09 [0.99, 1.19] | 0.96 [0.82, 1.13] |
| Protestant Christians | 1.08 [0.98, 1.18] | 1.05 [0.90, 1.21] |
| No religion/others | 1.04 [0.92, 1.18] | 0.88 [0.74, 1.05] |
| Total lifetime sexual partners | ||
| 0 | 1 | 1 |
| 1 | 5.16 [3.90, 6.84] | 1.45 [1.10, 1.91] |
| 2 | 4.88 [3.69, 6.46] | 1.53 [1.18, 1.99] |
| 3–4 | 4.94 [3.74, 6.52] | 1.55 [1.18, 2.04] |
| 5–9 | 4.74 [3.49, 6.44] | 1.52 [1.17, 1.96] |
| 10+ | 4.21 [2.87, 6.16] | 1.75 [1.32, 2.30] |
| Undisclosed | 5.16 [3.81, 6.99] | 1.39 [1.05, 1.84] |
| Had any STI last 12 months | ||
| No | 1 | 1 |
| Yes | 1.07 [1.00, 1.14] | 1.06 [0.91, 1.25] |
| Household wealth index | ||
| Poorest | 1 | 1 |
| Poorer | 1.08 [0.98, 1.19] | 1.06 [0.89, 1.26] |
| Middle | 1.18 [1.06, 1.31] | 1.26 [1.06, 1.50] |
| Richer | 1.25 [1.13, 1.38] | 1.48 [1.25, 1.75] |
| Richest | 1.28 [1.14, 1.43] | 1.70 [1.38, 2.09] |
| Rural/Urban Residence | ||
| Rural | 1 | 1 |
| Urban | 1.14 [1.06, 1.22] | 1.02 [0.89, 1.18] |
| Region | ||
| Cabo Delgado | 1 | 1 |
| Niassa | 1.23 [1.07, 1.42] | 1.02 [0.70, 1.48] |
| Nampula | 0.92 [0.81, 1.03] | 0.97 [0.67, 1.40] |
| Zambézia | 0.97 [0.79, 1.19] | 1.14 [0.79, 1.64] |
| Tete | 1.23 [1.06, 1.43] | 1.85 [1.29, 2.66] |
| Manica | 1.20 [1.05, 1.39] | 1.80 [1.28, 2.54] |
| Sofala | 1.06 [0.93, 1.20] | 1.37 [1.00, 1.89] |
| Inhambane | 1.32 [1.16, 1.50] | 1.70 [1.20, 2.40] |
| Gaza | 1.40 [1.25, 1.57] | 1.93 [1.41, 2.66] |
| Maputo Provincia | 1.18 [1.06, 1.32] | 1.47 [1.09, 1.98] |
| Maputo Cidade | 1.11 [0.99, 1.24] | 1.67 [1.23, 2.27] |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Agbadi, P.; Nutor, J.J.; Darkwah, E.; Duah, H.O.; Duodu, P.A.; Alhassan, R.K.; Baltzell, K. Covariates and Spatial Interpolation of HIV Screening in Mozambique: Insight from the 2015 AIDS Indicator Survey. Int. J. Environ. Res. Public Health 2020, 17, 5630. https://doi.org/10.3390/ijerph17165630
Agbadi P, Nutor JJ, Darkwah E, Duah HO, Duodu PA, Alhassan RK, Baltzell K. Covariates and Spatial Interpolation of HIV Screening in Mozambique: Insight from the 2015 AIDS Indicator Survey. International Journal of Environmental Research and Public Health. 2020; 17(16):5630. https://doi.org/10.3390/ijerph17165630
Chicago/Turabian StyleAgbadi, Pascal, Jerry John Nutor, Ernest Darkwah, Henry Ofori Duah, Precious Adade Duodu, Robert Kaba Alhassan, and Kimberly Baltzell. 2020. "Covariates and Spatial Interpolation of HIV Screening in Mozambique: Insight from the 2015 AIDS Indicator Survey" International Journal of Environmental Research and Public Health 17, no. 16: 5630. https://doi.org/10.3390/ijerph17165630