Association between Allergic Rhinitis and Regular Physical Activity in Adults: A Nationwide Cross-Sectional Study


Abstract
:1. Introduction
2. Materials and Methods
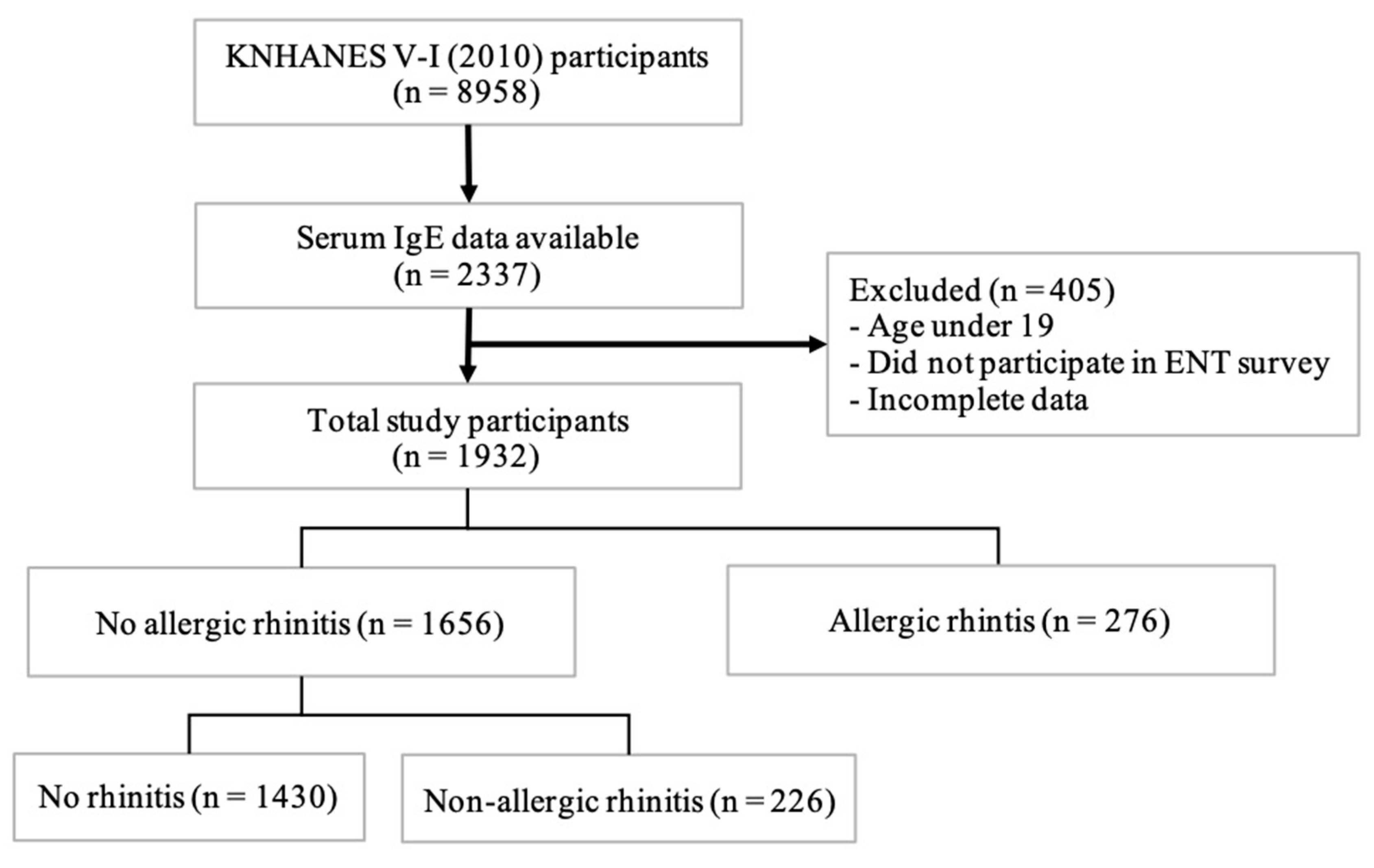
2.1. Survey Used for Data Collection and the Study Population
2.2. Assessment of Variables
2.3. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Association between AR and PA in the Total Study Population
3.3. Associations between AR and PA in the AR Population
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Bousquet, J.; Khaltaev, N.; Cruz, A.A.; Denburg, J.; Fokkens, W.J.; Togias, A.; Zuberbier, T.; Baena-Cagnani, C.E.; Canonica, G.W.; van Weel, C.; et al. Allergic Rhinitis and its Impact on Asthma (ARIA) 2008 update (in collaboration with the World Health Organization, GA (2) LEN and AllerGen). Allergy 2008, 63 (Suppl. S86), 8–160. [Google Scholar] [CrossRef]
- Brozek, J.L.; Bousquet, J.; Agache, I.; Agarwal, A.; Bachert, C.; Bosnic-Anticevich, S.; Brignardello-Petersen, R.; Canonica, G.W.; Casale, T.; Chavannes, N.H.; et al. Allergic Rhinitis and its Impact on Asthma (ARIA) guidelines-2016 revision. J. Allergy Clin. Immunol. 2017, 140, 950–958. [Google Scholar] [CrossRef] [Green Version]
- Meltzer, E.O.; Nathan, R.; Derebery, J.; Stang, P.E.; Campbell, U.B.; Yeh, W.S.; Corrao, M.; Stanford, R. Sleep, quality of life, and productivity impact of nasal symptoms in the United States: Findings from the Burden of Rhinitis in America survey. Allergy Asthma Proc. 2009, 30, 244–254. [Google Scholar] [CrossRef]
- Valovirta, E.; Myrseth, S.E.; Palkonen, S. The voice of the patients: Allergic rhinitis is not a trivial disease. Curr. Opin. Allergy Clin. Immunol. 2008, 8, 1–9. [Google Scholar] [CrossRef]
- Cooper, D.M.; Radom-Aizik, S.; Schwindt, C.; Zaldivar, F., Jr. Dangerous exercise: Lessons learned from dysregulated inflammatory responses to physical activity. J. Appl. Physiol. 2007, 103, 700–709. [Google Scholar] [CrossRef] [Green Version]
- Richerson, H.B.; Seebohm, P.M. Nasal airway response to exercise. J. Allergy 1968, 41, 269–284. [Google Scholar] [CrossRef]
- Syabbalo, N.C.; Bundgaard, A.; Widdicombe, J.G. Effects of exercise on nasal airflow resistance in healthy subjects and in patients with asthma and rhinitis. Bull. Eur. Physiopathol. Respir. 1985, 21, 507–513. [Google Scholar] [PubMed]
- Serra-Batlles, J.; Montserrat, J.M.; Mullol, J.; Ballester, E.; Xaubet, A.; Picado, C. Response of the nose to exercise in healthy subjects and in patients with rhinitis and asthma. Thorax 1994, 49, 128–132. [Google Scholar] [CrossRef] [Green Version]
- Silvers, W.S.; Poole, J.A. Exercise-induced rhinitis: A common disorder that adversely affects allergic and nonallergic athletes. Ann. Allergy Asthma Immunol. 2006, 96, 334–340. [Google Scholar] [CrossRef]
- Vlaski, E.; Stavric, K.; Seckova, L.; Kimovska, M.; Isjanovska, R. Influence of physical activity and television-watching time on asthma and allergic rhinitis among young adolescents: Preventive or aggravating? Allergol. Immunopathol. 2008, 36, 247–253. [Google Scholar] [CrossRef]
- Mitchell, E.A.; Beasley, R.; Bjorksten, B.; Crane, J.; Garcia-Marcos, L.; Keil, U. The association between BMI, vigorous physical activity and television viewing and the risk of symptoms of asthma, rhinoconjunctivitis and eczema in children and adolescents: ISAAC Phase Three. Clin. Exp. Allergy 2013, 43, 73–84. [Google Scholar] [CrossRef] [PubMed]
- Strom, M.A.; Silverberg, J.I. Associations of Physical Activity and Sedentary Behavior with Atopic Disease in United States Children. J. Pediatr. 2016, 174, 247–253.e243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garcia-Marcos, L.; Canflanca, I.M.; Garrido, J.B.; Varela, A.L.; Garcia-Hernandez, G.; Guillen Grima, F.; Gonzalez-Diaz, C.; Carvajal-Uruena, I.; Arnedo-Pena, A.; Busquets-Monge, R.M.; et al. Relationship of asthma and rhinoconjunctivitis with obesity, exercise and Mediterranean diet in Spanish schoolchildren. Thorax 2007, 62, 503–508. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, M.P.; Berdel, D.; Bauer, C.P.; Koletzko, S.; Nowak, D.; Heinrich, J.; Schulz, H. Asthma and rhinitis are associated with less objectively-measured moderate and vigorous physical activity, but similar sport participation, in adolescent German boys: GINIplus and LISAplus Cohorts. PLoS ONE 2016, 11, e0161461. [Google Scholar] [CrossRef]
- Alaranta, A.; Alaranta, H.; Heliovaara, M.; Alha, P.; Palmu, P.; Helenius, I. Allergic rhinitis and pharmacological management in elite athletes. Med. Sci. Sports Exerc. 2005, 37, 707–711. [Google Scholar] [CrossRef]
- Greiner, A.N.; Hellings, P.W.; Rotiroti, G.; Scadding, G.K. Allergic rhinitis. Lancet 2011, 378, 2112–2122. [Google Scholar] [CrossRef]
- Baran, H.; Ozcan, K.M.; Selcuk, A.; Cetin, M.A.; Cayir, S.; Ozcan, M.; Dere, H. Allergic rhinitis and its impact on asthma classification correlations. J. Laryngol. Otol. 2014, 128, 431–437. [Google Scholar] [CrossRef]
- Bauchau, V.; Durham, S.R. Epidemiological characterization of the intermittent and persistent types of allergic rhinitis. Allergy 2005, 60, 350–353. [Google Scholar] [CrossRef]
- Izquierdo-Dominguez, A.; Jauregui, I.; Del Cuvillo, A.; Montoro, J.; Davila, I.; Sastre, J.; Bartra, J.; Ferrer, M.; Alobid, I.; Mullol, J.; et al. Allergy rhinitis: Similarities and differences between children and adults. Rhinology 2017, 55, 326–331. [Google Scholar] [CrossRef]
- Gergen, P.J.; Arbes, S.J., Jr.; Calatroni, A.; Mitchell, H.E.; Zeldin, D.C. Total IgE levels and asthma prevalence in the US population: Results from the National Health and Nutrition Examination Survey 2005–2006. J Allergy Clin. Immunol. 2009, 124, 447–453. [Google Scholar] [CrossRef] [Green Version]
- Haskell, W.L.; Lee, I.M.; Pate, R.R.; Powell, K.E.; Blair, S.N.; Franklin, B.A.; Macera, C.A.; Heath, G.W.; Thompson, P.D.; Bauman, A. Physical activity and public health: Updated recommendation for adults from the American College of Sports Medicine and the American Heart Association. Med. Sci. Sports Exerc. 2007, 39, 1423–1434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, S.-C.; Wang, S.Y.; Pasquale, L.R.; Singh, K.; Lin, S.C. The relation between exercise and glaucoma in a South Korean population-based sample. PLoS ONE 2017, 12, e0171441. [Google Scholar] [CrossRef] [PubMed]
- Xiang, L.; Rehm, K.E.; Marshall, G.D., Jr. Effects of strenuous exercise on Th1/Th2 gene expression from human peripheral blood mononuclear cells of marathon participants. Mol. Immunol. 2014, 60, 129–134. [Google Scholar] [CrossRef] [PubMed]
- Lakier Smith, L. Overtraining, excessive exercise, and altered immunity: Is this a T helper-1 versus T helper-2 lymphocyte response? Sports Med. 2003, 33, 347–364. [Google Scholar] [CrossRef] [PubMed]
- Aldred, S.; Love, J.A.; Tonks, L.A.; Stephens, E.; Jones, D.S.; Blannin, A.K. The effect of steady state exercise on circulating human IgE and IgG in young healthy volunteers with known allergy. J. Sci. Med. Sport 2010, 13, 16–19. [Google Scholar] [CrossRef] [PubMed]
- Dykewicz, M.S.; Fineman, S.; Skoner, D.P.; Nicklas, R.; Lee, R.; Blessing-Moore, J.; Li, J.T.; Bernstein, I.L.; Berger, W.; Spector, S.; et al. Diagnosis and management of rhinitis: Complete guidelines of the Joint Task Force on Practice Parameters in Allergy, Asthma and Immunology. American Academy of Allergy, Asthma, and Immunology. Ann. Allergy Asthma Immunol. 1998, 81, 478–518. [Google Scholar] [CrossRef]
- Surda, P.; Walker, A.; Limpens, J.; Fokkens, W.; Putala, M. Nasal changes associated with exercise in athletes: Systematic review. J. Laryngol. Otol. 2018, 132, 191–197. [Google Scholar] [CrossRef]
- Fransson, M.; Benson, M.; Wennergren, G.; Cardell, L.O. A role for neutrophils in intermittent allergic rhinitis. Acta Otolaryngol. 2004, 124, 616–620. [Google Scholar] [CrossRef]
- Arebro, J.; Ekstedt, S.; Hjalmarsson, E.; Winqvist, O.; Kumlien Georén, S.; Cardell, L.O. A possible role for neutrophils in allergic rhinitis revealed after cellular subclassification. Sci. Rep. 2017, 7, 43568. [Google Scholar] [CrossRef] [Green Version]
- Aggarwal, B.; Mulgirigama, A.; Berend, N. Exercise-induced bronchoconstriction: Prevalence, pathophysiology, patient impact, diagnosis and management. Npj Prim. Care Respir. Med. 2018, 28, 31. [Google Scholar] [CrossRef]
- Casale, T.B.; Dykewicz, M.S. Clinical implications of the allergic rhinitis-asthma link. Am. J. Med. Sci. 2004, 327, 127–138. [Google Scholar] [CrossRef] [PubMed]
- Storms, W.W. Asthma associated with exercise. Immunol. Allergy Clin. N. Am. 2005, 25, 31–43. [Google Scholar] [CrossRef] [PubMed]
- Bonini, S.; Bonini, M.; Bousquet, J.; Brusasco, V.; Canonica, G.W.; Carlsen, K.H.; Corbetta, L.; Cummiskey, J.; Delgado, L.; Del Giacco, S.R.; et al. Rhinitis and asthma in athletes: An ARIA document in collaboration with GA2LEN. Allergy 2006, 61, 681–692. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| AR (−) | AR (+) | p | |
|---|---|---|---|
| n = 1656, N = 31,667,729 | n = 276, N = 5,615,440 | ||
| 84.90% | 15.10% | ||
| Age | 45.64 ± 0.59 | 39.68 ± 1.3 | <0.001 |
| Sex (female) | 851 (51.1) | 130 (46.2) | 0.238 |
| Residence (urban) | 1314 (76.9) | 231 (82.3) | 0.113 |
| Household income (Upper 50%) | 930 (53.7) | 158 (55.0) | 0.758 |
| Household number (≥4) | 732 (48.0) | 134 (53.4) | 0.179 |
| Marriage status (married) | 1354 (80.3) | 178 (63.9) | <0.001 |
| Education (≥12 years) | 1141 (68.2) | 225 (77.8) | 0.016 |
| Occupation (white collar) | 1193 (71.7) | 211 (74.8) | 0.341 |
| Alcohol use (Yes) | 960 (59.1) | 162 (55.8) | 0.362 |
| Smoking (Yes) | 416 (27.5) | 76 (29.0) | 0.685 |
| Obesity (BMI ≥ 25) | 542 (34.0) | 73 (29.7) | 0.257 |
| Sleep (≥8 h) | 480 (29.8) | 88 (30.4) | 0.870 |
| Stress (High) | 430 (27.4) | 87 (35.7) | 0.034 |
| Asthma | 53 (3.4) | 23 (9.4) | 0.001 |
| Atopic dermatitis | 83 (5.3) | 26 (9.9) | 0.010 |
| n (%) | Univariate | Multivariate | ||||
|---|---|---|---|---|---|---|
| AR (−) | AR (+) | Odds Ratio (95% CI) | p | Odds Ratio (95% CI) | p | |
| n = 1656 | n = 276 | |||||
| Vigorous | 272 (17.1) | 52 (18.2) | 1.080 (0.731–1.595) | 0.696 | 0.965 (0.655–1.423) | 0.857 |
| Moderate | 177 (12.0) | 33 (11.1) | 0.914 (0.565–1.480) | 0.714 | 0.998 (0.617–1.614) | 0.993 |
| Walking | 681 (40.6) | 117 (44.8) | 1.185 (0.849–1.654) | 0.316 | 1.126 (0.804–1.577) | 0.888 |
| A | ||||||
| n (%) | Univariate | Multivariate | ||||
| Mild | Moderate–Severe | Odds Ratio (95% CI) | p | Odds Ratio (95% CI) | p | |
| n = 183 | n = 91 | |||||
| Vigorous | 30 (11.8) | 22 (31.2) | 3.403 (1.597–7.249) | 0.002 | 3.392 (1.555–7.398) | 0.002 |
| Moderate | 18 (6.2) | 15 (21.0) | 4.050 (1.667–9.839) | 0.002 | 3.623 (1.444–9.090) | 0.007 |
| Walking | 73 (42.3 | 44 (49.8) | 1.356 (0.736–2.499) | 0.326 | 1.053 (0.548–2.026) | 0.876 |
| B | ||||||
| n (%) | Univariate | Multivariate | ||||
| Intermittent | Persistent | Odds Ratio (95% CI) | p | Odds Ratio (95% CI) | p | |
| n = 196 | n = 78 | |||||
| Vigorous | 30 (13.6) | 22 (30.9) | 2.848 (1.241–6.539) | 0.014 | 3.954 (1.551–10.084) | 0.004 |
| Moderate | 20 (7.2) | 13 (21.7) | 3.555 (1.339–9.440) | 0.011 | 3.411 (1.194–9.748) | 0.022 |
| Walking | 82 (42.9) | 35 (49.9) | 1.327 (0.723–2.436) | 0.358 | 1.383 (0.732–2.611) | 0.314 |
| A | ||||||
| n (%) | Univariate | Multivariate | ||||
| Healthy | Watery Rhinorrhea | Odds Ratio (95% CI) | p | Odds Ratio (95% CI) | p | |
| n = 179 | n = 92 | |||||
| Vigorous | 52 (14.4) | 23 (28.4) | 2.351 (1.071–5.159) | 0.033 | 2.203 (1.006–4.825) | 0.048 |
| Moderate | 23 (10.4) | 10 (13.7) | 1.378 (0.475–3.996) | 0.553 | 1.199 (0.395–3.641) | 0.747 |
| Walking | 80 (47.3) | 36 (39.0) | 0.715 (0.389–1.312) | 0.276 | 0.558 (0.266–1.170) | 0.121 |
| B | ||||||
| n (%) | Univariate | Multivariate | ||||
| Healthy | Pale Mucosa | Odds Ratio (95% CI) | p | Odds Ratio (95% CI) | p | |
| n = 192 | n = 79 | |||||
| Vigorous | 36 (17.6) | 16 (21.4) | 1.279 (0.553–2.955) | 0.562 | 1.293 (0.546–3.063) | 0.556 |
| Moderate | 25 (10.3) | 8 (14.2) | 1.451 (0.564–3.731) | 0.436 | 1.466 (0.551–3.900) | 0.440 |
| Walking | 84 (45.9) | 32 (42.0) | 0.855 (0.478–1.527) | 0.593 | 0.627 (0.311–1.266) | 0.191 |
| A | ||||||
| Mean ± SE | Univariate | Multivariate | ||||
| No PA | PA | Odds Ratio (95% CI) | p | Odds Ratio (95% CI) | p | |
| Vigorous | 2.33 ± 0.047 | 2.24 ± 0.119 | 0.750 (0.337–1.671) | 0.479 | 0.420 (0.161–1.095) | 0.076 |
| Moderate | 2.30 ± 0.046 | 2.40 ± 0.126 | 1.343 (0.600–3.005) | 0.470 | 1.531 (0.531–4.415) | 0.427 |
| Walking | 2.32 ±0.068 | 2.30 ± 0.065 | 0.945 (0.510–1.750) | 0.856 | 0.771 (0.381–1.560) | 0.466 |
| B | ||||||
| Mean ± SE | Univariate | Multivariate | ||||
| No PA | PA | Odds Ratio (95% CI) | p | Odds Ratio (95% CI) | p | |
| Vigorous | 0.51 ± 0.081 | 0.63 ± 0.136 | 1.150 (0.808–1.636) | 0.435 | 1.066 (0.690–1.646) | 0.773 |
| Moderate | 0.54 ± 0.079 | 0.49 ± 0.182 | 0.947 (0.605–1.483) | 0.811 | 0.887 (0.553–1.421) | 0.615 |
| Walking | 0.52 ± 0.091 | 0.55 ± 0.125 | 1.032 (0.718–1.482) | 0.865 | 0.895 (0.602–1.328) | 0.578 |
| C | ||||||
| Mean ± SE | Univariate | Multivariate | ||||
| No PA | PA | Odds Ratio (95% CI) | p | Odds Ratio (95% CI) | p | |
| Vigorous | −1.06 ± 0.057 | −1.04 ± 0.132 | 1.032 (0.600–1.774) | 0.910 | 0.793 (0.396–1.587) | 0.509 |
| Moderate | −1.07 ± 0.058 | −0.97 ± 0.129 | 1.202 (0.720–2.006) | 0.479 | 1.391 (0.728–2.659) | 0.315 |
| Walking | −1.06 ± 0.081 | −1.05 ± 0.083 | 1.026 (0.635–1.659) | 0.915 | 0.902 (0.559–1.455) | 0.669 |
| D | ||||||
| Mean ± SE | Univariate | Multivariate | ||||
| No PA | PA | Odds Ratio (95% CI) | p | Odds Ratio (95% CI) | p | |
| Vigorous | −0.60 ± 0.060 | −0.71 ± 0.143 | 0.803 (0.423–1.522) | 0.498 | 0.550 (0.271–1.116) | 0.097 |
| Moderate | −0.62 ± 0.056 | −0.64 ± 0.162 | 0.961 (0.501–1.846) | 0.905 | 0.932 (0.452–1.919) | 0.846 |
| Walking | −0.60 ± 0.075 | −0.64 ± 0.069 | 0.920 (0.633–1.337) | 0.660 | 0.880 (0.577–1.341) | 0.549 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, J.; Park, J.H.; Park, J.; Choi, J.; Kim, T.H. Association between Allergic Rhinitis and Regular Physical Activity in Adults: A Nationwide Cross-Sectional Study. Int. J. Environ. Res. Public Health 2020, 17, 5662. https://doi.org/10.3390/ijerph17165662
Park J, Park JH, Park J, Choi J, Kim TH. Association between Allergic Rhinitis and Regular Physical Activity in Adults: A Nationwide Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2020; 17(16):5662. https://doi.org/10.3390/ijerph17165662
Chicago/Turabian StylePark, Jewel, Joo Hee Park, Jaehyung Park, Jimi Choi, and Tae Hoon Kim. 2020. "Association between Allergic Rhinitis and Regular Physical Activity in Adults: A Nationwide Cross-Sectional Study" International Journal of Environmental Research and Public Health 17, no. 16: 5662. https://doi.org/10.3390/ijerph17165662