Characterisation of the Expression of Neurotensin and Its Receptors in Human Colorectal Cancer and Its Clinical Implications

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Immunohistochemical Staining
2.3. Quantification
2.4. Statistical Analysis
3. Results
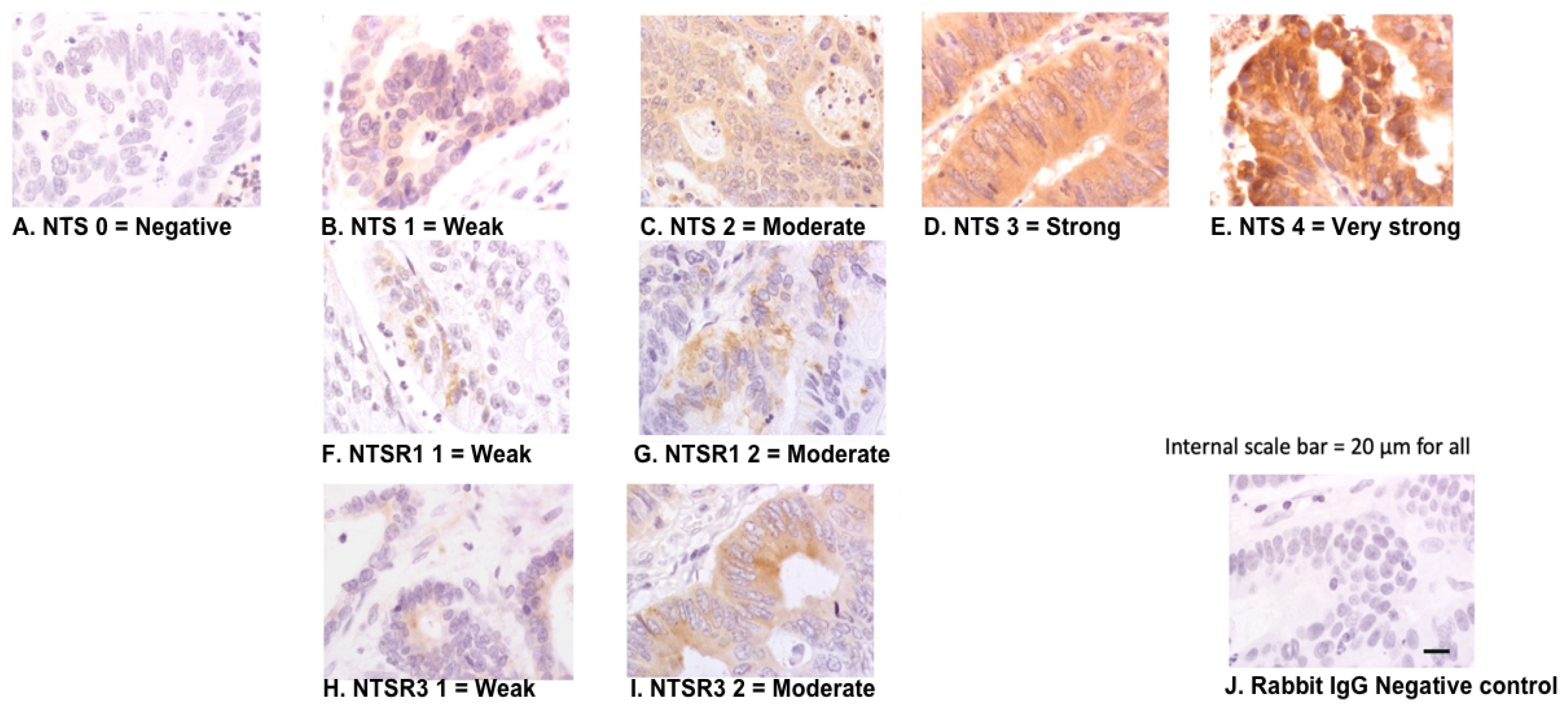
3.1. Morphological Patterns of NTS, NTSR1, and NTSR3 Protein Expression
3.2. Expression of NTS in Cancer Tissue Was Different between Different Histological Grades
3.3. Expressions of NTS, NTSR1, and NTSR3 in Cancer and Normal Surrounding Epithelium
3.4. NTS Expression in Cancer Tissue and Survival Outcomes
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Carraway, R.; Leeman, S.E. The isolation of a new hypotensive peptide, neurotensin, from bovine hypothalami. J. Biol. Chem. 1973, 248, 6854–6861. [Google Scholar] [PubMed]
- Ferris, C.F. Neurotensin. In Comprehensive Physiology; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2010. [Google Scholar] [CrossRef]
- Zhao, D.; Pothoulakis, C. Effects of NT on gastrointestinal motility and secretion, and role in intestinal inflammation. Peptides 2006, 27, 2434–2444. [Google Scholar] [CrossRef] [PubMed]
- Chalon, P.; Vita, N.; Kaghad, M.; Guillemot, M.; Bonnin, J.; Delpech, B.; Le Fur, G.; Ferrara, P.; Caput, D. Molecular cloning of a levocabastine-sensitive neurotensin binding site. FEBS Lett. 1996, 386, 91–94. [Google Scholar] [CrossRef] [Green Version]
- Mazella, J.; Zsurger, N.; Navarro, V.; Chabry, J.; Kaghad, M.; Caput, D.; Ferrara, P.; Vita, N.; Gully, D.; Maffrand, J.P.; et al. The 100-kDa neurotensin receptor is gp95/sortilin, a non-G-protein-coupled receptor. J. Biol. Chem. 1998, 273, 26273–26276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dupouy, S.; Viardot-Foucault, V.; Alifano, M.; Souaze, F.; Plu-Bureau, G.; Chaouat, M.; Lavaur, A.; Hugol, D.; Gespach, C.; Gompel, A.; et al. The neurotensin receptor-1 pathway contributes to human ductal breast cancer progression. PLoS ONE 2009, 4, e4223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Souaze, F.; Dupouy, S.; Viardot-Foucault, V.; Bruyneel, E.; Attoub, S.; Gespach, C.; Gompel, A.; Forgez, P. Expression of neurotensin and NT1 receptor in human breast cancer: A potential role in tumor progression. Cancer Res. 2006, 66, 6243–6249. [Google Scholar] [CrossRef] [Green Version]
- Alifano, M.; Souaze, F.; Dupouy, S.; Camilleri-Broet, S.; Younes, M.; Ahmed-Zaid, S.M.; Takahashi, T.; Cancellieri, A.; Damiani, S.; Boaron, M.; et al. Neurotensin receptor 1 determines the outcome of non-small cell lung cancer. Clin. Cancer Res. 2010, 16, 4401–4410. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.G.; Li, N.N.; Li, H.N.; Cui, L.; Wang, P. Pancreatic cancer bears overexpression of neurotensin and neurotensin receptor subtype-1 and SR 48692 counteracts neurotensin induced cell proliferation in human pancreatic ductal carcinoma cell line PANC-1. Neuropeptides 2011, 45, 151–156. [Google Scholar] [CrossRef]
- Allen, A.E.; Carney, D.N.; Moody, T.W. Neurotensin binds with high affinity to small cell lung cancer cells. Peptides 1988, 9, 57–61. [Google Scholar] [CrossRef]
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Mathers, C.; Parkin, D.M.; Pineros, M.; Znaor, A.; Bray, F. Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods. Int. J. Cancer 2019, 144, 1941–1953. [Google Scholar] [CrossRef] [Green Version]
- Ferlay, J.; Ervik, M.; Lam, F.; Colombet, M.; Mery, L.; Piñeros, M.; Znaor, A.; Soerjomataram, I.; Bray, F. Global Cancer Observatory: Cancer Today; International Agency for Research on Cancer: Lyon, France, 2018; Available online: https://gco.iarc.fr/today (accessed on 2 February 2020).
- NCCN. NCCN Clinical Practice Guidelines in Oncology, Rectal Cancer Version 4, 2018; NCCN: Plymouth Meeting, PA, USA, 2018. [Google Scholar]
- NCCN. NCCN Clinical Practice Guidelines in Oncology, Colon Cancer Version 4, 2018; NCCN: Plymouth Meeting, PA, USA, 2018. [Google Scholar]
- Glynne-Jones, R.; Wyrwicz, L.; Tiret, E.; Brown, G.; Rödel, C.; Cervantes, A.; Arnold, D. Rectal cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2017, 28, iv22–iv40. [Google Scholar] [CrossRef] [PubMed]
- Mandalà, M.; Labianca, R.; Mosconi, S.; Nordlinger, B.; Beretta, G.D.; Cervantes, A.; Arnold, D. Early colon cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2013, 24, vi64–vi72. [Google Scholar] [CrossRef]
- Maoret, J.J.; Pospai, D.; Rouyer-Fessard, C.; Couvineau, A.; Laboisse, C.; Voisin, T.; Laburthe, M. Neurotensin receptor and its mRNA are expressed in many human colon cancer cell lines but not in normal colonic epithelium: Binding studies and RT-PCR experiments. Biochem. Biophys. Res. Commun. 1994, 203, 465–471. [Google Scholar] [CrossRef] [PubMed]
- Bossard, C.; Souaze, F.; Jarry, A.; Bezieau, S.; Mosnier, J.F.; Forgez, P.; Laboisse, C.L. Over-expression of neurotensin high-affinity receptor 1 (NTS1) in relation with its ligand neurotensin (NT) and nuclear beta-catenin in inflammatory bowel disease-related oncogenesis. Peptides 2007, 28, 2030–2035. [Google Scholar] [CrossRef]
- Gui, X.; Guzman, G.; Dobner, P.R.; Kadkol, S.S. Increased neurotensin receptor-1 expression during progression of colonic adenocarcinoma. Peptides 2008, 29, 1609–1615. [Google Scholar] [CrossRef]
- Qiu, S.; Pellino, G.; Fiorentino, F.; Rasheed, S.; Darzi, A.; Tekkis, P.; Kontovounisios, C. A Review of the Role of Neurotensin and Its Receptors in Colorectal Cancer. Gastroenterol. Res. Pract. 2017, 2017, 6456257. [Google Scholar] [CrossRef]
- Cappuzzo, F.; Hirsch, F.R.; Rossi, E.; Bartolini, S.; Ceresoli, G.L.; Bemis, L.; Haney, J.; Witta, S.; Danenberg, K.; Domenichini, I.; et al. Epidermal growth factor receptor gene and protein and gefitinib sensitivity in non-small-cell lung cancer. J. Natl. Cancer Inst. 2005, 97, 643–655. [Google Scholar] [CrossRef]
- Dziadziuszko, R.; Wynes, M.W.; Singh, S.; Asuncion, B.R.; Ranger-Moore, J.; Konopa, K.; Rzyman, W.; Szostakiewicz, B.; Jassem, J.; Hirsch, F.R. Correlation between MET gene copy number by silver in situ hybridization and protein expression by immunohistochemistry in non-small cell lung cancer. J. Thorac. Oncol. Off. Publ. Int. Assoc. Study Lung Cancer 2012, 7, 340–347. [Google Scholar] [CrossRef] [Green Version]
- Aherne, W.A.; Dunnil, M.S. Point counting and morphometry. In Morphometry; Ahearne, W.A., Dunnil, M.S., Eds.; Arnold: London, UK, 1982; pp. 33–35. [Google Scholar]
- Munck Petersen, C.; Nielsen, M.S.; Jacobsen, C.; Tauris, J.; Jacobsen, L.; Gliemann, J.; Moestrup, S.K.; Madsen, P. Propeptide cleavage conditions sortilin/neurotensin receptor-3 for ligand binding. EMBO J. 1999, 18, 595–604. [Google Scholar] [CrossRef]
- Martin, S.; Navarro, V.; Vincent, J.P.; Mazella, J. Neurotensin receptor-1 and -3 complex modulates the cellular signaling of neurotensin in the HT29 cell line. Gastroenterology 2002, 123, 1135–1143. [Google Scholar] [CrossRef]
- Morinville, A.; Martin, S.; Lavallee, M.; Vincent, J.P.; Beaudet, A.; Mazella, J. Internalization and trafficking of neurotensin via NTS3 receptors in HT29 cells. Int. J. Biochem. Cell Biol. 2004, 36, 2153–2168. [Google Scholar] [CrossRef] [PubMed]
- NHS England. Improving Outcomes through Personalised Medicine. Available online: https://www.england.nhs.uk/wp-content/uploads/2016/09/improving-outcomes-personalised-medicine.pdf (accessed on 4 May 2020).
- Van Cutsem, E.; Cervantes, A.; Adam, R.; Sobrero, A.; Van Krieken, J.H.; Aderka, D.; Aranda Aguilar, E.; Bardelli, A.; Benson, A.; Bodoky, G.; et al. ESMO consensus guidelines for the management of patients with metastatic colorectal cancer. Ann. Oncol. 2016, 27, 1386–1422. [Google Scholar] [CrossRef] [PubMed]
- Sepulveda, A.R.; Hamilton, S.R.; Allegra, C.J.; Grody, W.; Cushman-Vokoun, A.M.; Funkhouser, W.K.; Kopetz, S.E.; Lieu, C.; Lindor, N.M.; Minsky, B.D.; et al. Molecular Biomarkers for the Evaluation of Colorectal Cancer: Guideline From the American Society for Clinical Pathology, College of American Pathologists, Association for Molecular Pathology, and the American Society of Clinical Oncology. J. Clin. Oncol. 2017, 35, 1453–1486. [Google Scholar] [CrossRef] [PubMed]
- Dalerba, P.; Sahoo, D.; Paik, S.; Guo, X.; Yothers, G.; Song, N.; Wilcox-Fogel, N.; Forgó, E.; Rajendran, P.S.; Miranda, S.P.; et al. CDX2 as a Prognostic Biomarker in Stage II and Stage III Colon Cancer. N. Engl. J. Med. 2016, 374, 211–222. [Google Scholar] [CrossRef]
- Yu, C.; Hong, H.; Lu, J.; Zhao, X.; Hu, W.; Zhang, S.; Zong, Y.; Mao, Z.; Li, J.; Wang, M.; et al. Prediction of Target Genes and Pathways Associated With Cetuximab Insensitivity in Colorectal Cancer. Technol. Cancer Res. Treat. 2018, 17, 1533033818806905. [Google Scholar] [CrossRef] [Green Version]
- Wu, Q.; Cao, R.; Chen, J.; Xie, X. Screening and identification of biomarkers associated with clinicopathological parameters and prognosis in oral squamous cell carcinoma. Exp. Ther. Med. 2019. [Google Scholar] [CrossRef]
- Zhou, D.; Sun, Y.; Jia, Y.; Liu, D.; Wang, J.; Chen, X.; Zhang, Y.; Ma, X. Bioinformatics and functional analyses of key genes in smoking-associated lung adenocarcinoma. Oncol. Lett. 2019. [Google Scholar] [CrossRef] [Green Version]
- Deng, T.; Gong, Y.Z.; Wang, X.K.; Liao, X.W.; Huang, K.T.; Zhu, G.Z.; Chen, H.N.; Guo, F.Z.; Mo, L.G.; Li, L.Q. Use of Genome-Scale Integrated Analysis to Identify Key Genes and Potential Molecular Mechanisms in Recurrence of Lower-Grade Brain Glioma. Med. Sci. Monit. 2019, 25, 3716–3727. [Google Scholar] [CrossRef]
- Myers, R.M.; Shearman, J.W.; Kitching, M.O.; Ramos-Montoya, A.; Neal, D.E.; Ley, S.V. Cancer, chemistry, and the cell: Molecules that interact with the neurotensin receptors. ACS Chem. Biol. 2009, 4, 503–525. [Google Scholar] [CrossRef]
- Gromova, P.; Rubin, B.P.; Thys, A.; Erneux, C.; Vanderwinden, J.M. Neurotensin receptor 1 is expressed in gastrointestinal stromal tumors but not in interstitial cells of Cajal. PLoS ONE 2011, 6, e14710. [Google Scholar] [CrossRef] [Green Version]
- Norris, E.J.; Zhang, Q.; Jones, W.D.; DeStephanis, D.; Sutker, A.P.; Livasy, C.A.; Ganapathi, R.N.; Tait, D.L.; Ganapathi, M.K. Increased expression of neurotensin in high grade serous ovarian carcinoma with evidence of serous tubal intraepithelial carcinoma. J. Pathol. 2019, 248, 352–362. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akter, H.; Yoon, J.H.; Yoo, Y.S.; Kang, M.J. Validation of Neurotensin Receptor 1 as a Therapeutic Target for Gastric Cancer. Mol. Cells 2018, 41, 591–602. [Google Scholar] [PubMed]
- Maoret, J.J.; Anini, Y.; Rouyer-Fessard, C.; Gully, D.; Laburthe, M. Neurotensin and a non-peptide neurotensin receptor antagonist control human colon cancer cell growth in cell culture and in cells xenografted into nude mice. Int. J. Cancer 1999, 80, 448–454. [Google Scholar] [CrossRef]
- Langbein, T.; Weber, W.A.; Eiber, M. Future of Theranostics: An Outlook on Precision Oncology in Nuclear Medicine. J. Nucl. Med. 2019, 60, 13S–19S. [Google Scholar] [CrossRef] [Green Version]
- He, T.; Wang, M.; Wang, H.; Tan, H.; Tang, Y.; Smith, E.; Wu, Z.; Liao, W.; Hu, S.; Li, Z. Evaluation of neurotensin receptor 1 as potential biomarker for prostate cancer theranostic use. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 2199–2207. [Google Scholar] [CrossRef]
- Schulz, J.; Rohracker, M.; Stiebler, M.; Goldschmidt, J.; Stöber, F.; Noriega, M.; Pethe, A.; Lukas, M.; Osterkamp, F.; Reineke, U.; et al. Proof of Therapeutic Efficacy of a (177)Lu-Labeled Neurotensin Receptor 1 Antagonist in a Colon Carcinoma Xenograft Model. J. Nucl. Med. Off. Publ. Soc. Nucl. Med. 2017, 58, 936–941. [Google Scholar] [CrossRef] [Green Version]
- Wu, Z.; Fournel, L.; Stadler, N.; Liu, J.; Boullier, A.; Hoyeau, N.; Flejou, J.F.; Duchatelle, V.; Djebrani-Oussedik, N.; Agopiantz, M.; et al. Modulation of lung cancer cell plasticity and heterogeneity with the restoration of cisplatin sensitivity by neurotensin antibody. Cancer Lett. 2019, 444, 147–161. [Google Scholar] [CrossRef]
- Baum, R.P.; Singh, A.; Schuchardt, C.; Kulkarni, H.R.; Klette, I.; Wiessalla, S.; Osterkamp, F.; Reineke, U.; Smerling, C. 177Lu-3BP-227 for Neurotensin Receptor 1–Targeted Therapy of Metastatic Pancreatic Adenocarcinoma: First Clinical Results. J. Nucl. Med. 2018, 59, 809–814. [Google Scholar] [CrossRef]
- Qiu, S.; Nikolaou, S.; Fiorentino, F.; Rasheed, S.; Darzi, A.; Cunningham, D.; Tekkis, P.; Kontovounisios, C. Exploratory Analysis of Plasma Neurotensin as a Novel Biomarker for Early Detection of Colorectal Polyp and Cancer. Horm. Cancer 2019, 10, 128–135. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Median | IQR | ||
|---|---|---|---|
| Age (years) | 72.2 | 63.9–82.4 | |
| BMI | 26.9 | 24.4–29.9 | |
| Category | Number | Frequency % | |
| Sex | Male | 30 | 51.7 |
| Female | 28 | 48.3 | |
| Ethnicity | Black | 6 | 10.3 |
| East Asian | 2 | 3.4 | |
| South Asian | 5 | 8.6 | |
| White | 38 | 65.5 | |
| Other | 7 | 12.1 | |
| American Society of | 1 | 13 | 22.4 |
| Anaesthesiologists | 2 | 17 | 29.3 |
| physical status | 3 | 28 | 48.3 |
| 4 | 0 | 0 | |
| American Joint | I | 22 | 37.9 |
| Committee on Cancer | II | 19 | 32.8 |
| Clinical Stage | III | 13 | 22.4 |
| IV | 4 | 6.9 | |
| Length of Hospital Stay (Days) | Median 7.0 | IQR 5.0–10.5 | |
| Perioperative Carcinoembryonic antigen | 2.0 | 1.0–4.0 | |
| Number | Frequency (%) | ||
| Operation | Right Hemicolectomy | 21 | 36.2 |
| Extended Right Hemicolectomy | 6 | 10.3 | |
| Left Hemicolectomy | 4 | 6.9 | |
| Sigmoid Colectomy | 3 | 5.2 | |
| Anterior Resection | 16 | 27.6 | |
| Abdominal Perineal Excision | 4 | 6.9 | |
| Appendicectomy | 1 | 1.7 | |
| Transanal endoscopic mucosal resection | 1 | 1.7 | |
| Hartmann’s Resection | 2 | 3.4 | |
| Laparoscopic | Open | 11 | 19.0 |
| Laparoscopic | 39 | 67.2 | |
| Converted to Open | 8 | 13.8 | |
| Complications | No | 46 | 79.3 |
| Yes | 12 | 20.7 | |
| Clavien-Dindo Grade | 0 | 46 | 79.3 |
| 1 | 0 | 0 | |
| 2 | 1 | 15.5 | |
| 3 | 1 | 1.7 | |
| 4 | 1 | 1.7 | |
| 5 | 1 | 1.7 | |
| Anastomotic Leak | No | 55 | 94.8 |
| Yes | 1 | 1.7 | |
| N/A (Transanal endoscopic mucosal resection/Appendicectomy) | 2 | 3.4 | |
| Neoadjuvant Therapy | No | 55 | 94.8 |
| Yes | 2 | 3.4 | |
| Missing | 1 | 1.7 | |
| Adjuvant Therapy | No | 38 | 65.5 |
| Yes | 19 | 32.7 | |
| Missing | 1 | 1.7 | |
| Median | IQR | ||
|---|---|---|---|
| Number of Lymph Nodes Harvested | 24.5 | 18.5–32.0 | |
| Cancer Maximum Diameter (mm) | 35.0 | 20.0–47.0 | |
| Rectal Cancer Height from Anal Verge (mm) | 90.0 | 67.0–110.0 | |
| Number | Frequency (%) | ||
| Location of Cancer | Caecum | 12 | 20.7 |
| Ascending Colon | 9 | 15.5 | |
| Transverse Colon | 4 | 6.9 | |
| Splenic Flexure | 2 | 3.4 | |
| Descending Colon | 1 | 1.7 | |
| Sigmoid Colon | 9 | 15.5 | |
| Rectum | 18 | 31.0 | |
| Appendix | 1 | 1.7 | |
| Multiple sites | 2 | 3.4 | |
| Grade of Differentiation | Well Differentiated | 2 | 3.4 |
| Moderately Differentiated | 47 | 81.0 | |
| Poorly Differentiated | 8 | 13.8 | |
| Missing | 1 | 1.7 | |
| Background of Serrated Adenoma | Yes | 3 | 5.2 |
| No | 55 | 94.8 | |
| Seen to arising from polyp | Yes | 16 | 27.6 |
| No | 42 | 72.4 | |
| Mucinous Cancer | Yes | 19 (1 signet ring cancer) | 32.7 |
| No | 39 | 67.2 | |
| Extra Mural Vascular Invasion | Yes | 11 | 19.0 |
| No | 48 | 79.3 | |
| Missing | 1 | 1.7 | |
| Lymphovascular Invasion | Yes | 18 | 31.0 |
| No | 39 | 67.2 | |
| Missing | 1 | 1.7 | |
| Perineural Invasion | Yes | 7 | 12.1 |
| No | 49 | 84.5 | |
| Missing | 2 | 3.4 | |
| Tumour Budding | None | 11 | 19 |
| Minimal/Focal | 16 | 27.6 | |
| Present | 16 | 27.6 | |
| Prominent | 12 | 20.7 | |
| Lymphoid Response | None | 12.1 | 13.0 |
| Mild | 27.6 | 29.6 | |
| Moderate | 15.5 | 16.7 | |
| Prominent | 1.3 | 11.1 | |
| Brisk—Crohn’s Like Response | 27.6 | 29.6 | |
| Pathological T-stage | 1 | 8 | 13.8 |
| 2 | 16 | 27.6 | |
| 3 | 21 | 36.2 | |
| 4 | 13 | 22.4 | |
| Pathological N-Stage | 0 | 41 | 70.7 |
| 1 | 11 | 19.0 | |
| 2 | 6 | 10.3 | |
| Resection Margin | 0 | 54 | 93.1 |
| 1 | 4 | 6.9 | |
| 2 | 0 | 0 | |
| M Stage | 0 | 54 | 93.1 |
| 1 | 3 | 5.2 | |
| 2 | 1 | 1.7 | |
| Microsatellite Instability | Present | 6 | 10.3 |
| Not Present | 20 | 34.5 | |
| Not done | 32 | 55.2 | |
| T1 (8) | T2 (16) | T3 (21) | T4 (13) | p | |
|---|---|---|---|---|---|
| NTS Cancer Tissue | |||||
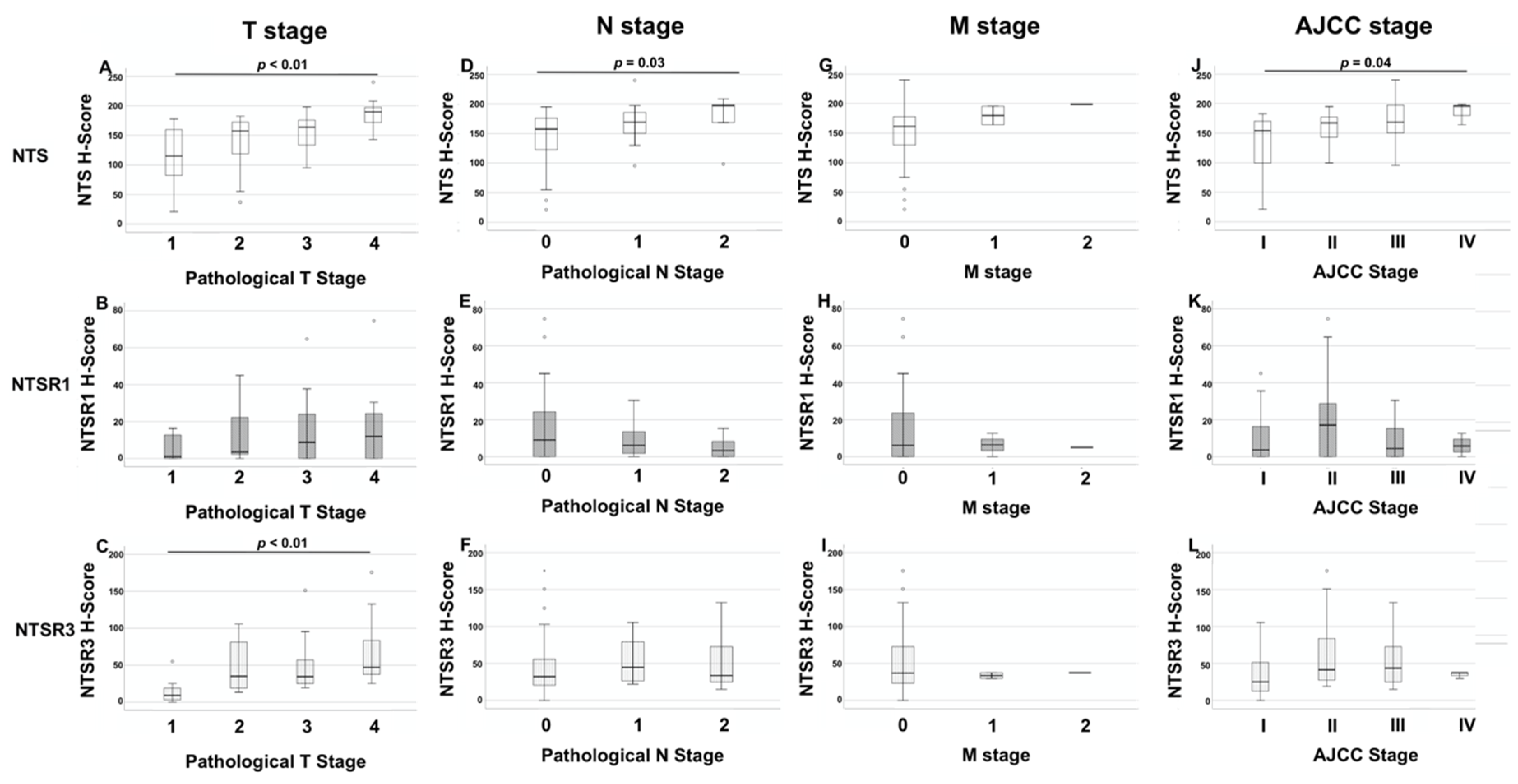
| Median | 115.25 | 157.6 | 163.9 | 189.8 | <0.01 * |
| IQR | 78.7–160.9 | 109.1–173.6 | 131.6–176.3 | 168.1–198.1 | |
| Range | 21.0–178.3 | 37.0–182.5 | 95.5–198.3 | 143.0–240.0 | |
| NTSR1 Cancer Tissue | |||||
| Median | 1.1 | 3.6 | 8.8 | 12.5 | 0.45 * |
| IQR | 0–13.5 | 2.2–24.7 | 0.0–24.1 | 0.0–24.6 | |
| Range | 0–16.3 | 0.0–45.0 | 0.0–64.7 | 0.0–74.5 | |
| NTSR3 Cancer Tissue | |||||
| Median | 8.9 | 34.9 | 34.4 | 46.8 | <0.01 * |
| IQR | 1.4–21.9 | 17.8–82.6 | 25.0–57.4 | 37.1–104.1 | |
| Range | 0.0–54.9 | 13.3–105.5 | 19.3–151.1 | 25.0–175.5 | |
| T1 | T2 | T3 | T4 | p | |
| NTS Normal Epithelium | |||||
| Median | 27.5 | 94.0 | 125.0 | 120.4 | 0.22 * |
| IQR | 21.3–82.8 | 47.0–130.2 | 75.0–149.1 | 82.7–161.5 | |
| Range | 12.5–155.0 | 22.5–173.3 | 25.0–175.5 | 42.1–175.0 | |
| NTSR1 Normal Epithelium | |||||
| Median | 0.0 | 0.00 | 0.0 | 0.0 | 0.98 * |
| IQR | 0.0–0.0 | 0.0–0.0 | 0.0–0.0 | 0.0–0.0 | |
| Range | 0.0–4.5 | 0.0–7.5 | 0.0–21.4 | 0.0–3.5 | |
| NTSR3 Normal Epithelium | |||||
| Median | 0.0 | 24.8 | 24.3 | 31.9 | 0.11 * |
| IQR | 0.0–9.4 | 10.9–54.1 | 9.4–31.8 | 14.5–73.2 | |
| Range | 0.0–34.25 | 0–87.5 | 0.0–162.5 | 0.0–145.7 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qiu, S.; Nikolaou, S.; Zhu, J.; Jeffery, P.; Goldin, R.; Kinross, J.; Alexander, J.L.; Rasheed, S.; Tekkis, P.; Kontovounisios, C. Characterisation of the Expression of Neurotensin and Its Receptors in Human Colorectal Cancer and Its Clinical Implications. Biomolecules 2020, 10, 1145. https://doi.org/10.3390/biom10081145
Qiu S, Nikolaou S, Zhu J, Jeffery P, Goldin R, Kinross J, Alexander JL, Rasheed S, Tekkis P, Kontovounisios C. Characterisation of the Expression of Neurotensin and Its Receptors in Human Colorectal Cancer and Its Clinical Implications. Biomolecules. 2020; 10(8):1145. https://doi.org/10.3390/biom10081145
Chicago/Turabian StyleQiu, Shengyang, Stella Nikolaou, Jie Zhu, Peter Jeffery, Robert Goldin, James Kinross, James L. Alexander, Shahnawaz Rasheed, Paris Tekkis, and Christos Kontovounisios. 2020. "Characterisation of the Expression of Neurotensin and Its Receptors in Human Colorectal Cancer and Its Clinical Implications" Biomolecules 10, no. 8: 1145. https://doi.org/10.3390/biom10081145