Effects of Autologous Platelet-Rich Fibrin in Post-Extraction Alveolar Sockets: A Randomized, Controlled Split-Mouth Trial in Dogs with Spontaneous Periodontal Disease

 ,
,  , ,
, , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Inclusion and Exclusion Criteria
2.2. Therapeutic Protocol
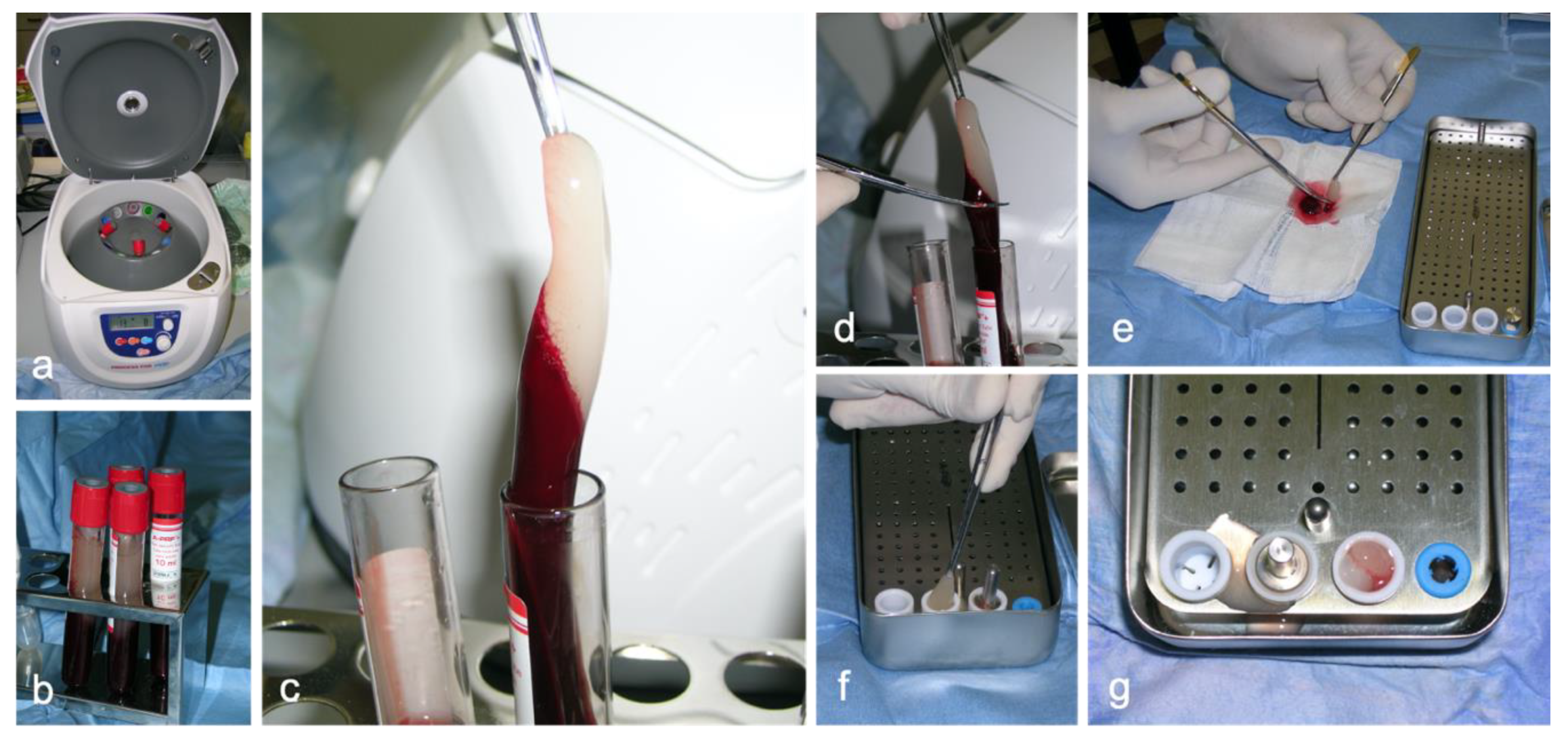
2.2.1. Preparation of Platelet-Rich Fibrin
2.2.2. General Anesthesia Procedure
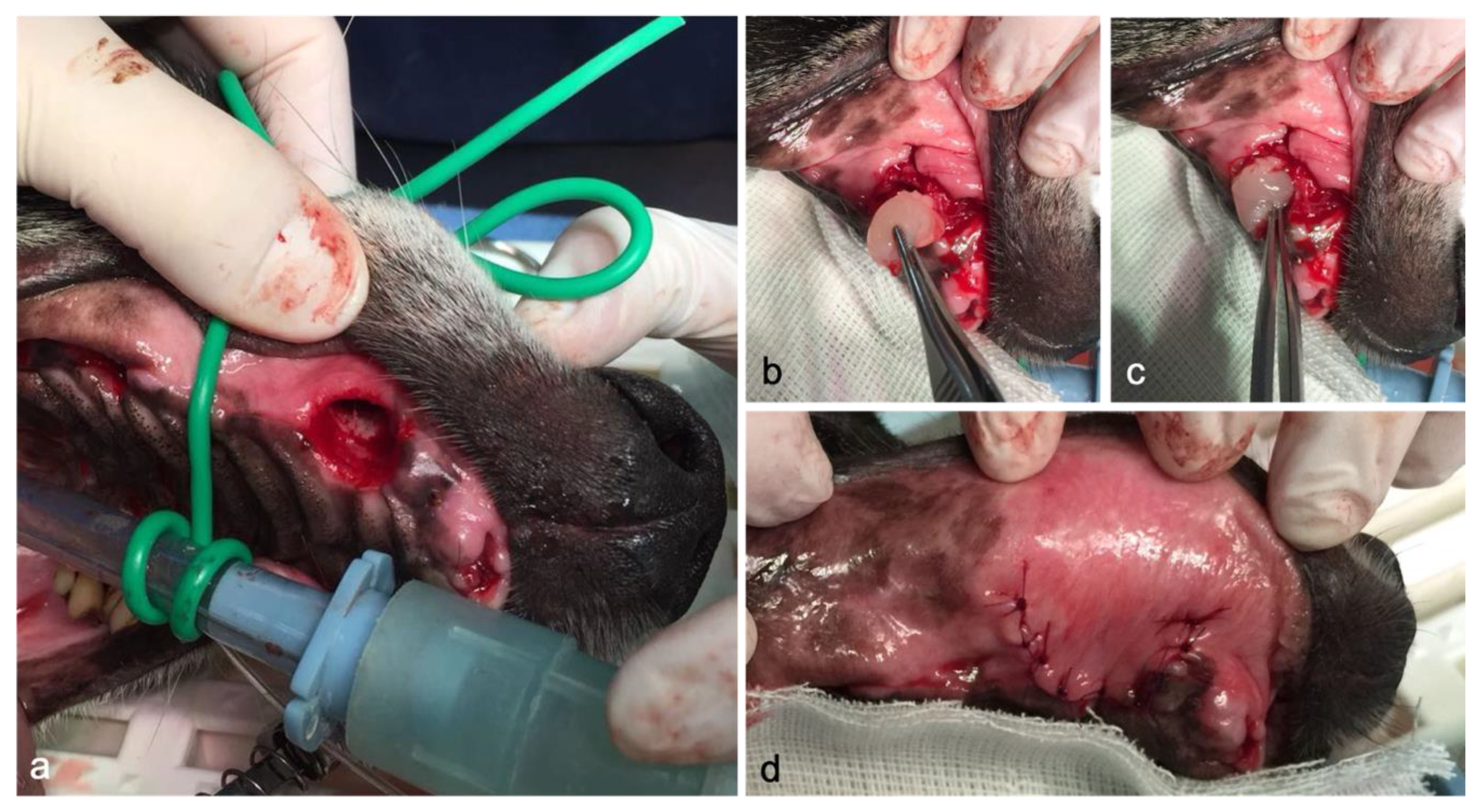
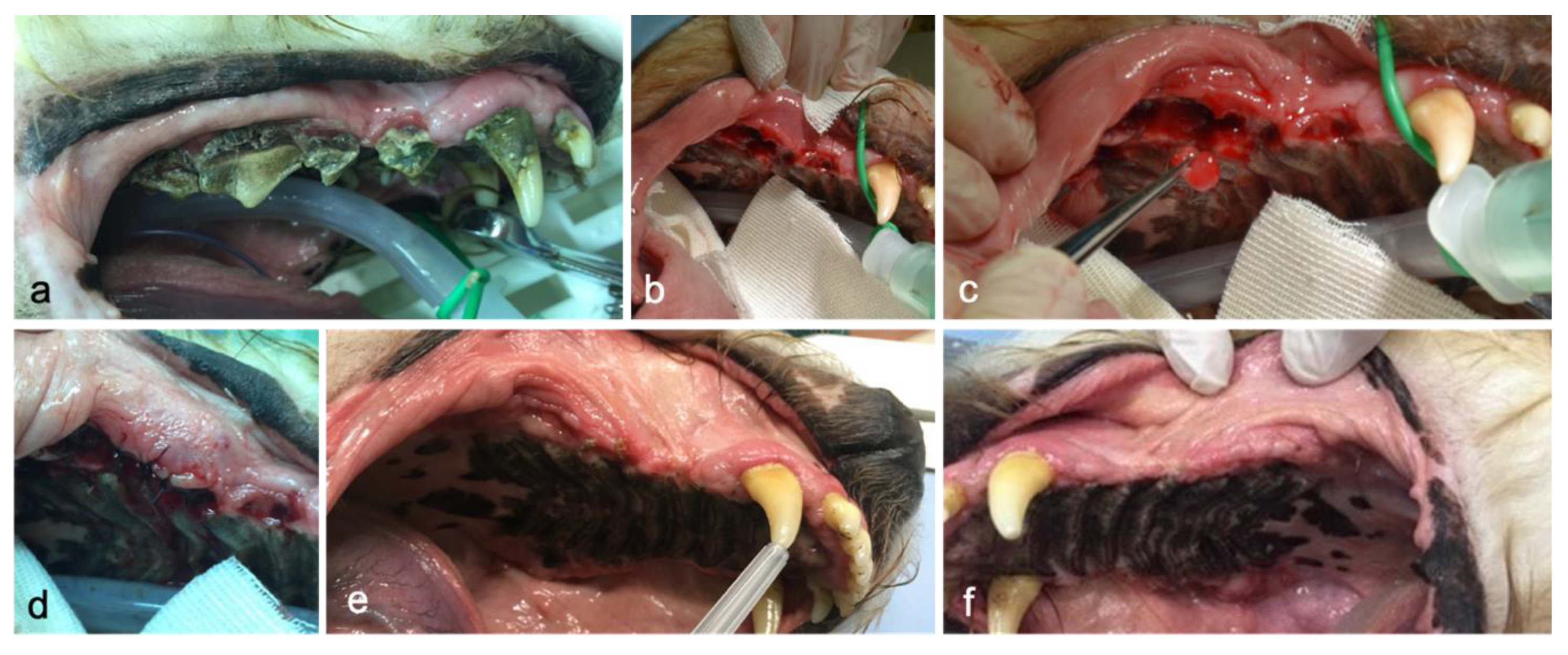
2.2.3. Surgery Procedure
2.2.4. Post-Operatory Care
2.3. Evaluation Protocol and Outcome Measures
2.3.1. Clinical Assessment
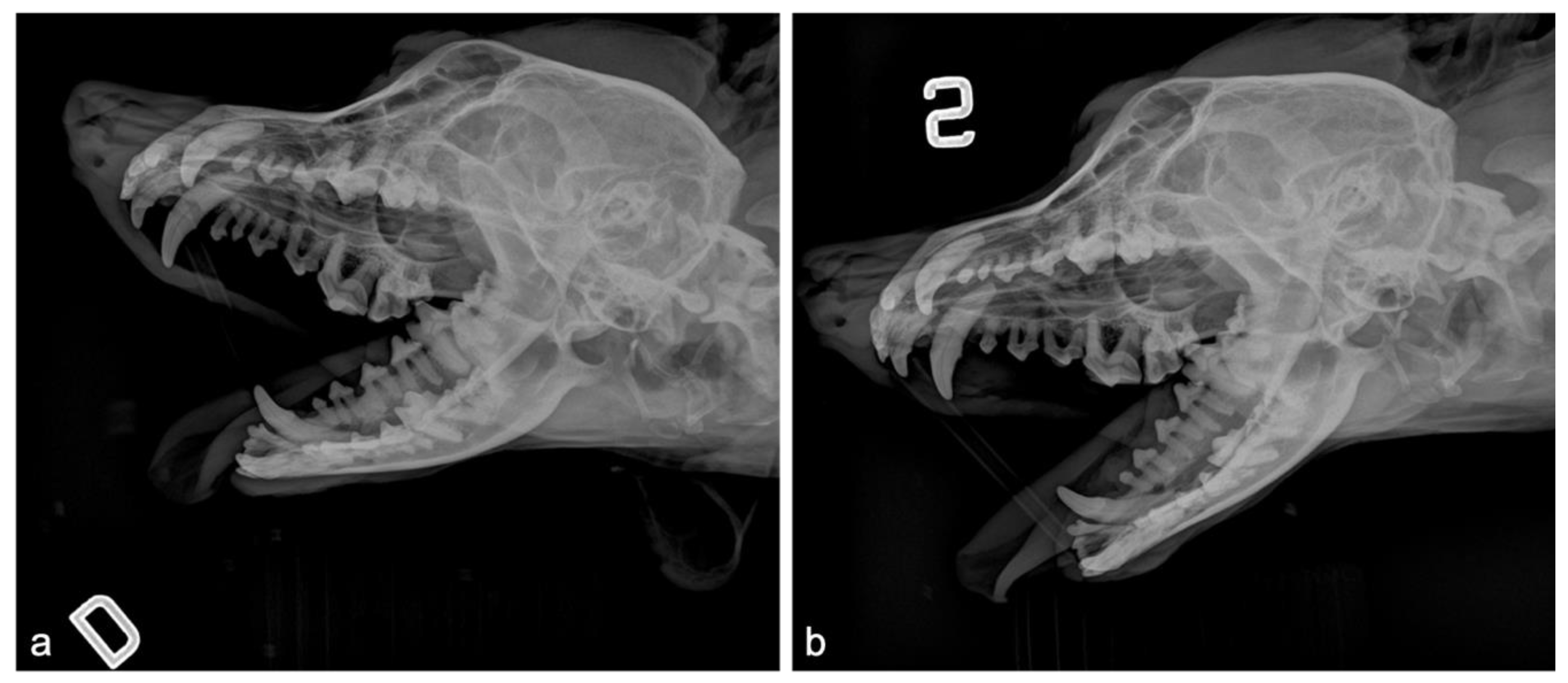
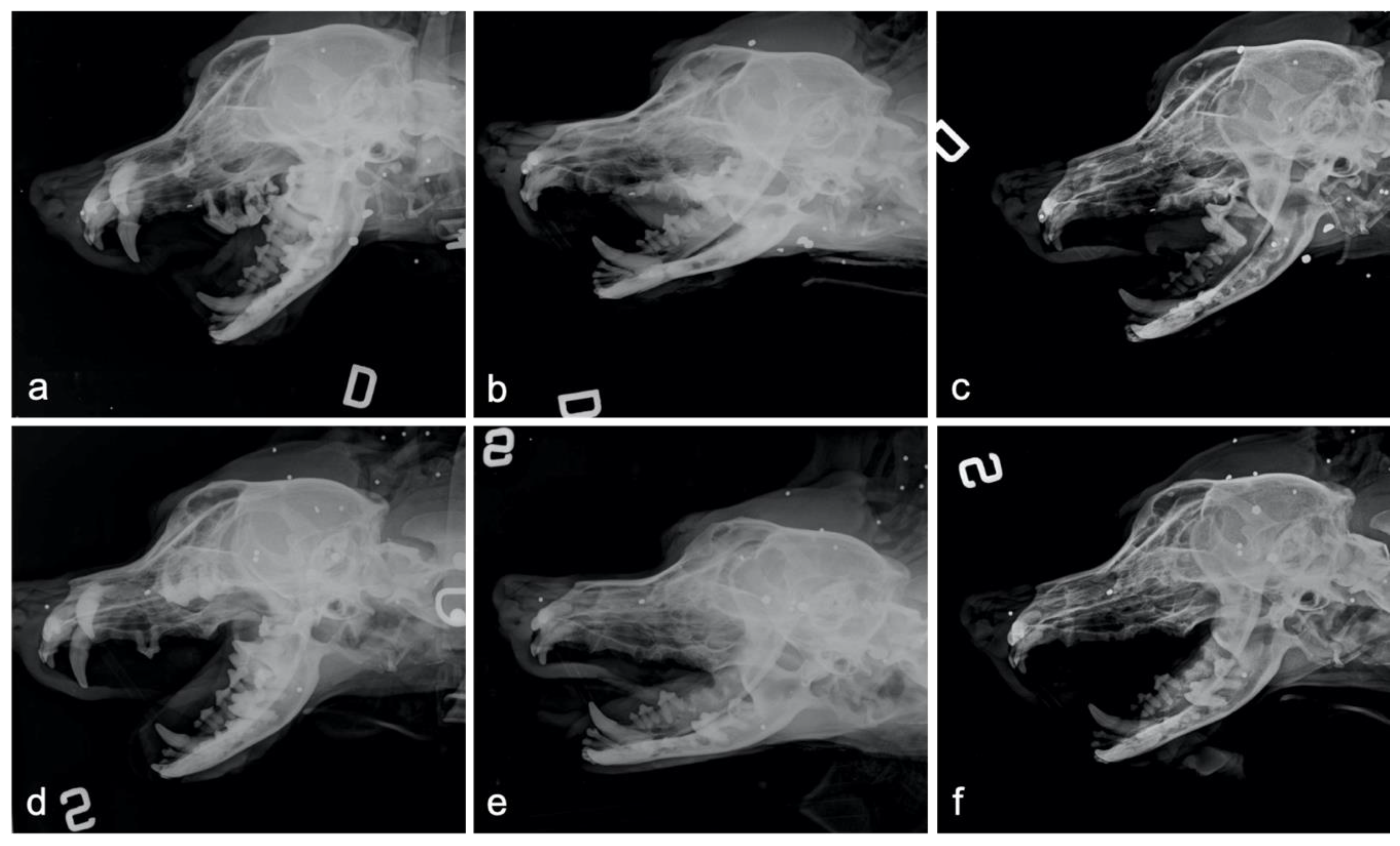
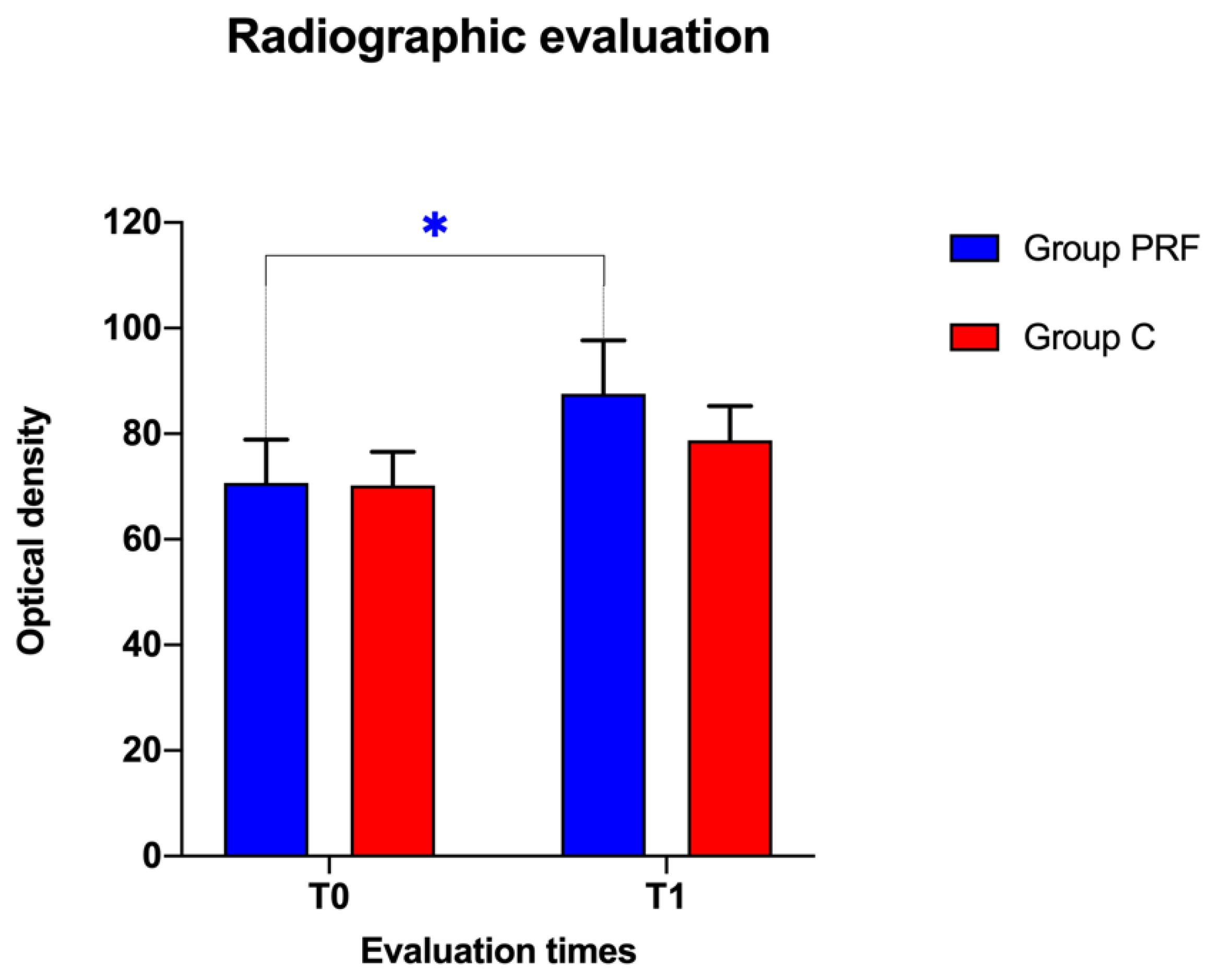
2.3.2. Radiographic Evaluation
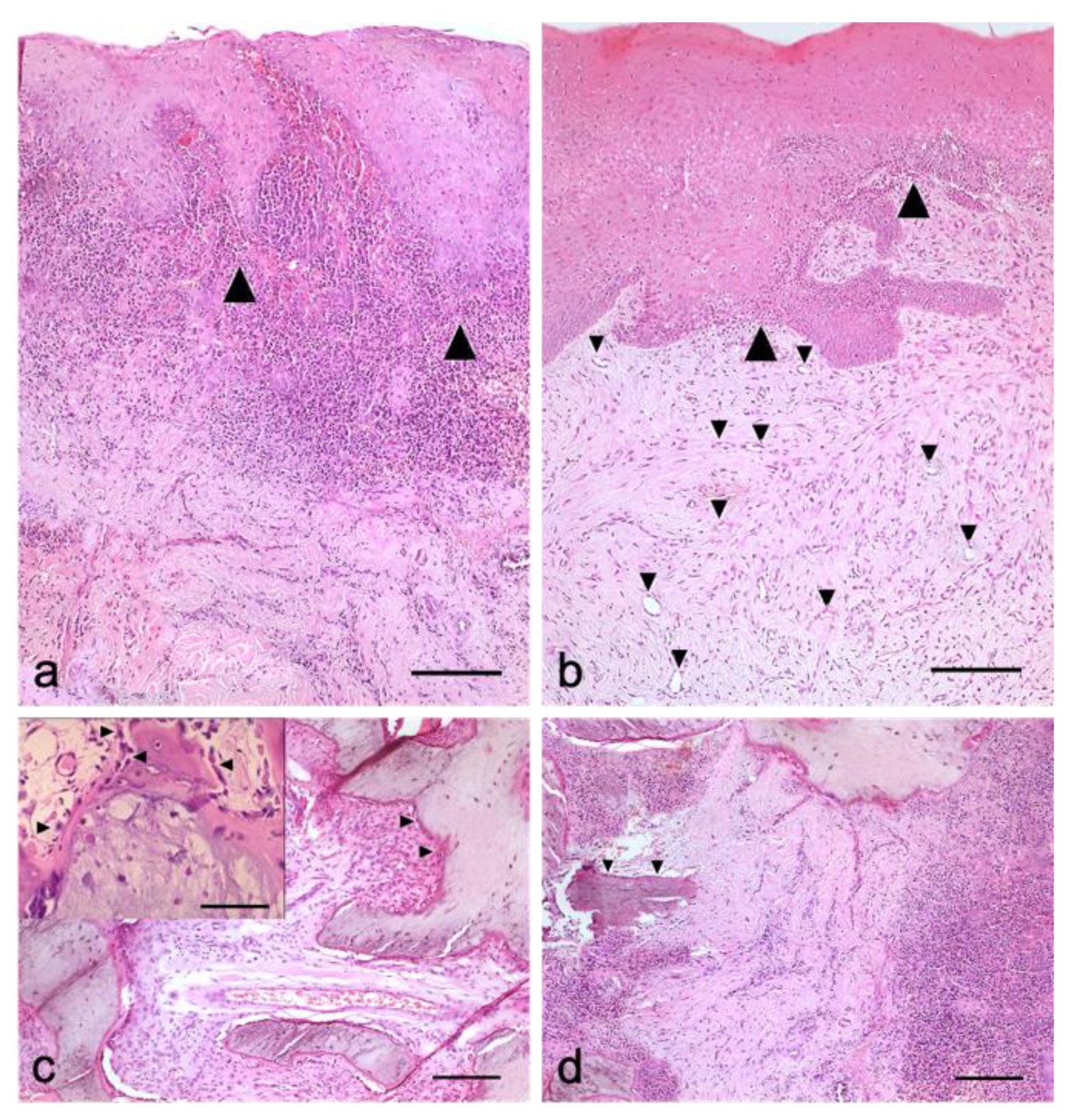
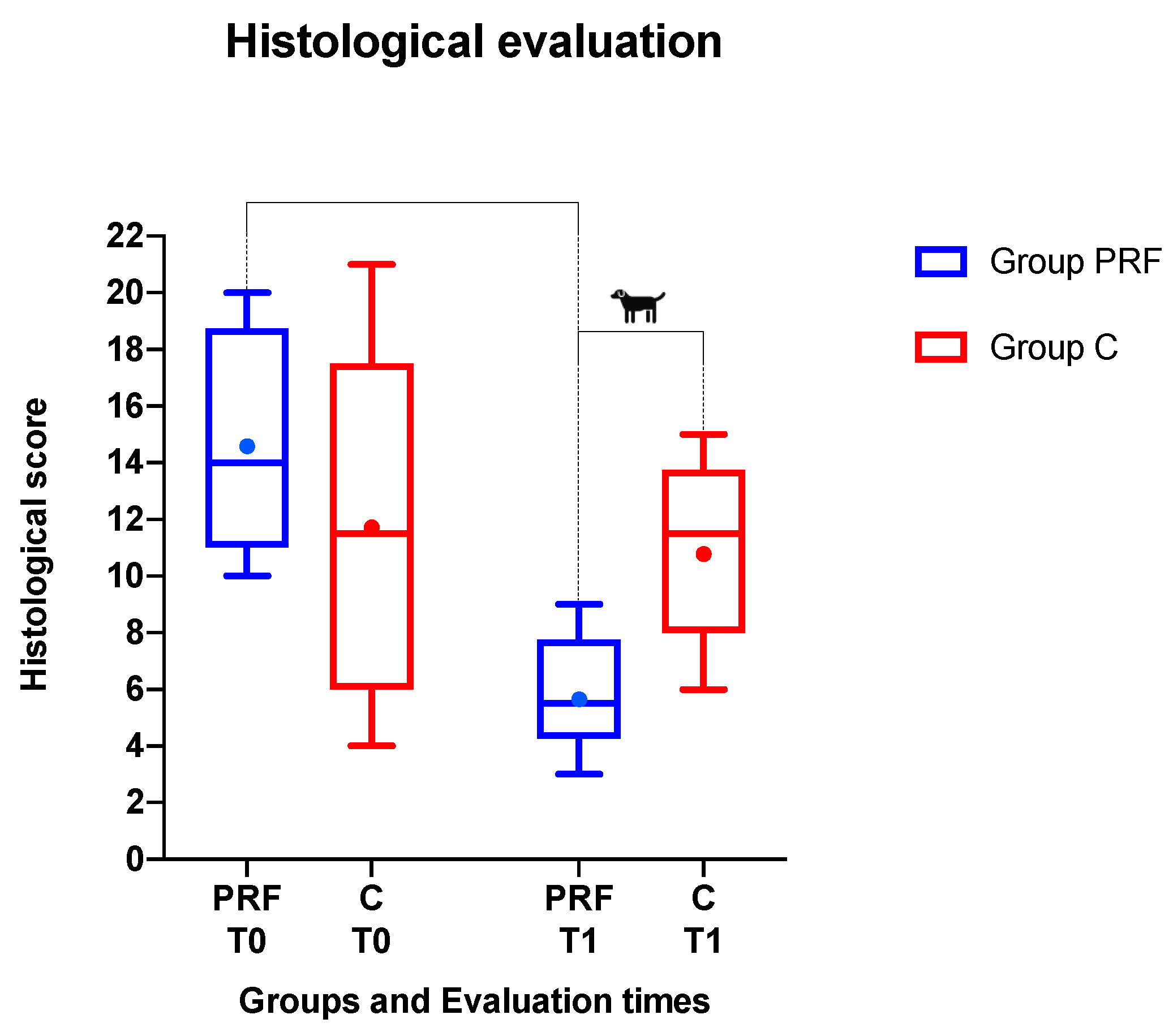
2.3.3. Histological Examination
2.4. Statistical Analysis
3. Results
3.1. Clinical Findings
3.2. Radiographic Findings
3.3. Histological Findings
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Albuquerque, C.; Morinha, F.; Requicha, J.; Martins, T.; Dias, I.; Guedes-Pinto, H.; Bastos, E.; Viegas, C. Canine periodontitis: The dog as an important model for periodontal studies. Vet. J. 2012, 191, 299–305. [Google Scholar] [CrossRef] [PubMed]
- Wiggs, R.; Lobprise, H. Periodontology, in Veterinary Dentistry, Principals and Practice; Lippincott Raven: Philadelphia, PA, USA, 1997. [Google Scholar]
- American Veterinary Dental College (AVDC). Veterinary dental nomenclature. J. Vet. Dent. 2007, 24, 54–57. [Google Scholar] [CrossRef] [PubMed]
- Niemiec, B.A. Periodontal Disease. Top. Companion Anim. Med. 2008, 23, 72–80. [Google Scholar] [CrossRef] [Green Version]
- Kortegaard, H.E.; Eriksen, T.; Baelum, V. Screening for periodontal disease in research dogs - a methodology study. Acta Vet. Scand. 2014, 56, 77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lewis, J.R. Therapeutic Decision Making and Planning in Veterinary Dentistry and Oral Surgery. Vet. Clin. N. Am. Small Anim. Pract. 2013, 43, 471–487. [Google Scholar] [CrossRef]
- Dohan, D.M.; Choukroun, J.; Diss, A.; Dohan, S.L.; Dohan, A.J.J.; Mouhyi, J.; Gogly, B. Platelet-rich fibrin (PRF): A second-generation platelet concentrate. Part I: Technological concepts and evolution. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2006, 101. [Google Scholar] [CrossRef]
- Dohan Ehrenfest, D.M.; Rasmusson, L.; Albrektsson, T. Classification of platelet concentrates: From pure platelet-rich plasma (P-PRP) to leucocyte- and platelet-rich fibrin (L-PRF). Trends Biotechnol. 2009, 27, 158–167. [Google Scholar] [CrossRef]
- Preeja, C.; Arun, S. Platelet-rich fibrin: Its role in periodontal regeneration. Saudi J. Dent. Res. 2014, 5, 117–122. [Google Scholar] [CrossRef] [Green Version]
- Saleh Almutairi, A. Platelet Rich Fibrin in Periodontal Practice, Review. Int. J. Dent. Sci. Res. 2017, 5, 132–136. [Google Scholar] [CrossRef]
- Dohan Ehrenfest, D.M.; De Peppo, G.M.; Doglioli, P.; Sammartino, G. Slow release of growth factors and thrombospondin-1 in Choukroun’s platelet-rich fibrin (PRF): A gold standard to achieve for all surgical platelet concentrates technologies. Growth Factors 2009, 27, 63–69. [Google Scholar] [CrossRef]
- Dohan Ehrenfest, D.M.; Del Corso, M.; Diss, A.; Mouhyi, J.; Charrier, J.-B. Three-Dimensional Architecture and Cell Composition of a Choukroun’s Platelet-Rich Fibrin Clot and Membrane. J. Periodontol. 2010, 81, 546–555. [Google Scholar] [CrossRef] [PubMed]
- Marenzi, G.; Riccitiello, F.; Tia, M.; Di Lauro, A.; Sammartino, G. Influence of leukocyte- and platelet-rich fibrin (L-PRF) in the healing of simple postextraction sockets: A split-mouth study. Biomed Res. Int. 2015, 2015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choukroun, J.; Adda, F.B.; Schoeffler, C.; Vervelle, A.G. Une opportunité en paro-implantologie: Le PRF. Implantodontie 2001, 42, 55–62. [Google Scholar]
- Mazor, Z.; Horowitz, R.A.; Del Corso, M.; Prasad, H.S.; Rohrer, M.D.; Dohan Ehrenfest, D.M. Sinus Floor Augmentation with Simultaneous Implant Placement Using Choukroun’s Platelet-Rich Fibrin as the Sole Grafting Material: A Radiologic and Histologic Study at 6 Months. J. Periodontol. 2009, 80, 2056–2064. [Google Scholar] [CrossRef] [Green Version]
- Eshghpour, M.; Majidi, M.R.; Nejat, A.H. Platelet-rich fibrin: An autologous fibrin matrix in surgical procedures: A case report and review of literature. Iran. J. Otorhinolaryngol. 2012, 24, 197–202. [Google Scholar]
- Kim, T.H.; Kim, S.H.; Sádor, G.K.; Kim, Y.D. Comparison of platelet-rich plasma (PRP), platelet-rich fibrin (PRF), and concentrated growth factor (CGF) in rabbit-skull defect healing. Arch. Oral Biol. 2014, 59, 550–558. [Google Scholar] [CrossRef]
- Boora, P.; Rathee, M.; Bhoria, M. Effect of Platelet Rich Fibrin (PRF) on peri-implant soft tissue and crestal bone in one-stage implant placement: A randomized controlled trial. J. Clin. Diagn. Res. 2015, 9, ZC18–ZC21. [Google Scholar] [CrossRef]
- Shawky, H.; Seifeldin, S.A. Does platelet-rich fibrin enhance bone quality and quantity of alveolar cleft reconstruction? Cleft Palate Craniofacial J. 2016, 53, 597–606. [Google Scholar] [CrossRef]
- Temmerman, A.; Vandessel, J.; Castro, A.; Jacobs, R.; Teughels, W.; Pinto, N.; Quirynen, M. The use of leucocyte and platelet-rich fibrin in socket management and ridge preservation: A split-mouth, randomized, controlled clinical trial. J. Clin. Periodontol. 2016, 43, 990–999. [Google Scholar] [CrossRef]
- Bilginaylar, K. The Use of Platelet-Rich Fibrin for Immediate Closure of Acute Oroantral Communications: An Alternative Approach. J. Oral Maxillofac. Surg. 2018, 76, 278–286. [Google Scholar] [CrossRef]
- Canellas, J.V.d.S.; da Costa, R.C.; Breves, R.C.; de Oliveira, G.P.; Figueredo, C.M.d.S.; Fischer, R.G.; Thole, A.A.; Medeiros, P.J.D.A.; Ritto, F.G. Tomographic and histomorphometric evaluation of socket healing after tooth extraction using leukocyte- and platelet-rich fibrin: A randomized, single-blind, controlled clinical trial. J. Cranio Maxillofac. Surg. 2020, 48, 24–32. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.H.; Tsai, C.H.; Chang, Y.C. Clinical and histologic evaluations of healing in an extraction socket filled with platelet-rich fibrin. J. Dent. Sci. 2011, 6, 116–122. [Google Scholar] [CrossRef] [Green Version]
- Alzahrani, A.A.; Murriky, A.; Shafik, S. Influence of platelet rich fibrin on post-extraction socket healing: A clinical and radiographic study. Saudi Dent. J. 2017, 29, 149–155. [Google Scholar] [CrossRef] [PubMed]
- Balse, N.S.; Baliga, S. Evaluation of wound healing and bone regeneration using autologous platelet-rich plasma and platelet-rich fibrin postextractions: A comparative study. Indian J. Heal. Sci. Biomed. Res. 2017, 10, 167–172. [Google Scholar] [CrossRef]
- Daugela, P.; Grimuta, V.; Sakavicius, D.; Jonaitis, J.; Juodzbalys, G. Influence of leukocyte- and platelet-rich fibrin (L-PRF) on the outcomes of impacted mandibular third molar removal surgery: A split-mouth randomized clinical trial. Quintessence Int. (Berl.) 2018, 49, 377–388. [Google Scholar]
- Jeyaraj, P.E.; Chakranarayan, A. Soft tissue healing and bony regeneration of impacted mandibular third molar extraction sockets, following postoperative incorporation of platelet-rich fibrin. Ann. Maxillofac. Surg. 2018, 8, 10–18. [Google Scholar] [CrossRef]
- Sharma, M.; Lone, P.A.; Singh, R.; Waheed, A. Effects of autologous platelet rich fibrin in bone regeneration in post-extraction mandibular sockets. Int. J. Appl. Dent. Sci. 2018, 4, 309–313. [Google Scholar]
- Srinivas, B.; Das, P.; Rana, M.M.; Qureshi, A.Q.; Vaidya, K.C.; Raziuddin, S.J.A. Wound healing and bone regeneration in postextraction sockets with and without platelet-rich fibrin. Ann. Maxillofac. Surg. 2018, 8, 28–34. [Google Scholar]
- Saravanakumar, B.; Julius, A.; Raghavendra Jayesh, S.; Krishna Prasanth, B. Soft tissue and alveolar bone repair of platelet rich fibrin over platelet rich plasma in extraction of impacted third molars. Indian J. Public Heal. Res. Dev. 2019, 10, 129–131. [Google Scholar] [CrossRef]
- Gürbüzer, B.; Pikdöken, L.; Tunali, M.; Urhan, M.; Küçükodaci, Z.; Ercan, F. Scintigraphic Evaluation of Osteoblastic Activity in Extraction Sockets Treated With Platelet-Rich Fibrin. J. Oral Maxillofac. Surg. 2010, 68, 980–989. [Google Scholar] [CrossRef]
- Farina, R.; Bressan, E.; Taut, A.; Cucchi, A.; Trombelli, L. Plasma rich in growth factors in human extraction sockets: A radiographic and histomorphometric study on early bone deposition. Clin. Oral Implants Res. 2013, 24, 1360–1368. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Areewong, K.; Chantaramungkorn, M.; Khongkhunthian, P. Platelet-rich fibrin to preserve alveolar bone sockets following tooth extraction: A randomized controlled trial. Clin. Implant Dent. Relat. Res. 2019, 21, 1156–1163. [Google Scholar] [CrossRef] [PubMed]
- Bastami, F.; Khojasteh, A. Use of Leukocyte-and Platelet-Rich Fibrin for Bone Regeneration: A Systematic Review. Use Leukoc. Platelet Rich Fibrin Bone Regen. A Syst. Rev. 2016, 1, 47–68. [Google Scholar]
- Verma, U.P.; Yadav, R.K.; Dixit, M.; Gupta, A. Platelet-rich Fibrin: A Paradigm in Periodontal Therapy—A Systematic Review. J. Int. Soc. Prev. Community Dent. 2017, 7, 227–233. [Google Scholar]
- Annunziata, M.; Guida, L.; Nastri, L.; Piccirillo, A.; Sommese, L.; Napoli, C. The Role of Autologous Platelet Concentrates in Alveolar Socket Preservation: A Systematic Review. Transfus. Med. Hemotherapy 2018, 45, 195–203. [Google Scholar] [CrossRef]
- Canellas, J.V.D.S.; Medeiros, P.J.D.; Figueredo, C.M.D.S.; Fischer, R.G.; Ritto, F.G. Platelet-rich fibrin in oral surgical procedures: A systematic review and meta-analysis. Int. J. Oral Maxillofac. Surg. 2019, 48, 395–414. [Google Scholar] [CrossRef] [Green Version]
- Visser, L.C.; Arnoczky, S.P.; Caballero, O.; Gardner, K.L. Evaluation of the use of an autologous platelet-rich fibrin membrane to enhance tendon healing in dogs. Am. J. Vet. Res. 2011, 72, 699–705. [Google Scholar] [CrossRef]
- Alishahi, M.K.; Kazemi, D.; Mohajeri, D.; Mofidpoor, H.; Goli, A.A.; Alishahi, M.A.K. Histopathological evaluation of the effect of platelet-rich fibrin on canine cutaneous incisional wound healing. Iran. J. Vet. Sci. Technol. 2014, 5, 19–32. [Google Scholar]
- Kazemi, D.; Fakhrjou, A. Leukocyte and platelet rich plasma (L-PRP) versus leukocyte and platelet rich fibrin (L-PRF) for articular cartilage repair of the knee: A comparative evaluation in an animal model. Iran. Red Crescent Med. J. 2015, 17. [Google Scholar] [CrossRef] [Green Version]
- Dizaji, V.M.; Kazemi, D.; Rezaei, M. Influence of Platelet Rich Fibrin on Biomechanical Properties of Primary Sutured Cutaneous Incisional Wounds. Taiwan Vet. J. 2016, 42, 69–74. [Google Scholar] [CrossRef]
- Moghaddam, A.J.; Kazemi, D. Evaluating the Feasibility of Esophagotomy Suture Line Reinforcement Using Platelet Rich Fibrin Membrane and Its Effect on Wound Healing. Iran. J. Vet. Surg. 2016, 11, 9–15. [Google Scholar]
- Thanoon, M.G.; Eesa, M.J.; Abed, E.R. Effects of platelets rich fibrin and bone marrow on the healing of distal radial fracture in local dogs: Comparative study. Iraqi J. Vet. Sci. 2019, 33, 419–425. [Google Scholar] [CrossRef]
- You, J.S.; Kim, S.G.; Oh, J.S.; Kim, J.S. Effects of Platelet-Derived Material (Platelet-Rich Fibrin) on Bone Regeneration. Implant Dent. 2019, 28, 244–255. [Google Scholar] [CrossRef] [PubMed]
- Simon, B.I.; Zatcoff, A.L.; Kong, J.J.W.; O’Connell, S.M. Clinical and Histological Comparison of Extraction Socket Healing Following the Use of Autologous Platelet-Rich Fibrin Matrix (PRFM) to Ridge Preservation Procedures Employing Demineralized Freeze Dried Bone Allograft Material and Membrane. Open Dent. J. 2009, 3, 92–99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hatakeyama, I.; Marukawa, E.; Takahashi, Y.; Omura, K. Effects of platelet-poor plasma, platelet-rich plasma, and platelet-rich fibrin on healing of extraction sockets with buccal dehiscence in dogs. Tissue Eng. Part A 2014, 20, 874–882. [Google Scholar] [CrossRef] [Green Version]
- Jeong, S.M.; Lee, C.U.; Son, J.S.; Oh, J.H.; Fang, Y.; Choi, B.H. Simultaneous sinus lift and implantation using platelet-rich fibrin as sole grafting material. J. Cranio Maxillofac. Surg. 2014, 42, 990–994. [Google Scholar] [CrossRef]
- Ji, B.; Sheng, L.; Chen, G.; Guo, S.; Xie, L.; Yang, B.; Guo, W.; Tian, W. The combination use of platelet-rich fibrin and treated dentin matrix for tooth root regeneration by cell homing. Tissue Eng. Part A 2015, 21, 26–34. [Google Scholar] [CrossRef]
- Neiva, R.F.; Gil, L.F.; Tovar, N.; Janal, M.N.; Marao, H.F.; Bonfante, E.A.; Pinto, N.; Coelho, P.G. The synergistic effect of leukocyte platelet-rich fibrin and micrometer/nanometer surface texturing on bone healing around immediately placed implants: An experimental study in dogs. Biomed Res. Int. 2016, 2016. [Google Scholar] [CrossRef]
- Abdelmagid, S.E.; Shaaban, A.M.M.; Ragaa, H.; Nagui, D. Comparison between the Use of Platelet Rich Fibrin with/and without Biphasic Calcium Phosphate for Osseointegration around Implants (Experimental Study). Int. J. Sci. Res. 2017, 6, 1803–1807. [Google Scholar]
- To, M.; Su, C.; Hidaka, K.; Okudera, T.; Matsuo, M. Effect of advanced platelet-rich fibrin on accelerating alveolar bone formation in dogs: A histological and immunofluorescence evaluation. Anat. Sci. Int. 2019, 94, 238–244. [Google Scholar] [CrossRef]
- Kornsuthisopon, C.; Pirarat, N.; Osathanon, T.; Kalpravidh, C. Autologous platelet-rich fibrin stimulates canine periodontal regeneration. Sci. Rep. 2020, 10, 1–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.B.; Lee, J.T.; Hwang, S.; Choi, J.Y.; Rhyu, I.C.; Yeo, I.S.L. Leukocyte- and platelet-rich fibrin is an effective membrane for lateral ridge augmentation: An in vivo study using a canine model with surgically created defects. J. Periodontol. 2020, 91, 120–128. [Google Scholar] [CrossRef] [PubMed]
- Nisengard, R.; Kinder Haake, S.; Newman, M.; Miyasaki, K. Microbial Interactions with the Host in Periodontal Diseases, in Carranza’s Clinical Periodontology; WB Saunders: St Louis, MO, USA, 2006. [Google Scholar]
- Pandis, N.; Walsh, T.; Polychronopoulou, A.; Katsaros, C.; Eliades, T. Split-mouth designs in orthodontics: An overview with applications to orthodontic clinical trials. Eur. J. Orthod. 2013, 35, 783–789. [Google Scholar] [CrossRef] [PubMed]
- Mozzati, M.; Martinasso, G.; Pol, R.; Polastri, C.; Cristiano, A.; Muzio, G.; Canuto, R. The impact of plasma rich in growth factors on clinical and biological factors involved in healing processes after third molar extraction. J. Biomed. Mater. Res. Part A 2010, 95, 741–746. [Google Scholar] [CrossRef]
- Kerry, S.M.; Bland, J.M. Analysis of a trial randomised in clusters. BMJ 1998, 316, 54. [Google Scholar] [CrossRef] [Green Version]
- Miron, R.J.; Fujioka-Kobayashi, M.; Bishara, M.; Zhang, Y.; Hernandez, M.; Choukroun, J. Platelet-Rich Fibrin and Soft Tissue Wound Healing: A Systematic Review. Tissue Eng. Part B Rev. 2017, 23, 83–99. [Google Scholar] [CrossRef] [Green Version]
- Del Corso, M.; Vervelle, A.; Simonpieri, A.; Jimbo, R.; Inchingolo, F.; Sammartino, G.; M. Dohan Ehrenfest, D. Current Knowledge and Perspectives for the Use of Platelet-Rich Plasma (PRP) and Platelet-Rich Fibrin (PRF) in Oral and Maxillofacial Surgery Part 1: Periodontal and Dentoalveolar Surgery. Curr. Pharm. Biotechnol. 2012, 13, 1207–1230. [Google Scholar] [CrossRef] [Green Version]
- Ghanaati, S.; Booms, P.; Orlowska, A.; Kubesch, A.; Lorenz, J.; Rutkowski, J.; Les, C.; Sader, R.; Kirkpatrick, C.J.; Choukroun, J. Advanced platelet-rich fibrin: A new concept for cell-Based tissue engineering by means of inflammatory cells. J. Oral Implantol. 2014, 40, 679–689. [Google Scholar] [CrossRef]
- Kobayashi, E.; Flückiger, L.; Fujioka-kobayashi, M. Comparative release of growth factors from PRP, PRF, and advanced-PRF. Clin. Oral Investig. 2016, 20, 2353–2369. [Google Scholar] [CrossRef]
- Fujioka-kobayashi, M.; Miron, R.J.; Hernandez, M.; Kandalam, U.; Zhang, Y.; Choukroun, J. Optimized Platelet-Rich Fibrin with the low-speed concept: Growth factor release, biocompatibility, and cellular response. J. Periodontol. 2017, 88, 112–121. [Google Scholar] [CrossRef]
- Park, H.C.; Kim, S.G.; Oh, J.S.; You, J.S.; Kim, J.S.; Lim, S.C.; Jeong, M.A.; Kim, J.S.; Jung, C.; Kwon, Y.S.; et al. Early bone formation at a femur defect using CGF and PRF grafts in adult dogs: A comparative study. Implant Dent. 2016, 25, 387–393. [Google Scholar] [CrossRef] [PubMed]








© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tambella, A.M.; Bartocetti, F.; Rossi, G.; Galosi, L.; Catone, G.; Falcone, A.; Vullo, C. Effects of Autologous Platelet-Rich Fibrin in Post-Extraction Alveolar Sockets: A Randomized, Controlled Split-Mouth Trial in Dogs with Spontaneous Periodontal Disease. Animals 2020, 10, 1343. https://doi.org/10.3390/ani10081343
Tambella AM, Bartocetti F, Rossi G, Galosi L, Catone G, Falcone A, Vullo C. Effects of Autologous Platelet-Rich Fibrin in Post-Extraction Alveolar Sockets: A Randomized, Controlled Split-Mouth Trial in Dogs with Spontaneous Periodontal Disease. Animals. 2020; 10(8):1343. https://doi.org/10.3390/ani10081343
Chicago/Turabian StyleTambella, Adolfo Maria, Francesca Bartocetti, Giacomo Rossi, Livio Galosi, Giuseppe Catone, Annastella Falcone, and Cecilia Vullo. 2020. "Effects of Autologous Platelet-Rich Fibrin in Post-Extraction Alveolar Sockets: A Randomized, Controlled Split-Mouth Trial in Dogs with Spontaneous Periodontal Disease" Animals 10, no. 8: 1343. https://doi.org/10.3390/ani10081343