Mechanical Debridement with Antibiotics in the Treatment of Chronic Periodontitis: Effect on Systemic Biomarkers―A Systematic Review


Abstract
:1. Background
2. Methods
2.1. Criteria for Considering Studies for This Review
2.1.1. Types of Studies
2.1.2. Types of Participants
2.1.3. Types of Interventions
Experimental
Control
2.1.4. Types of Outcome Measures
Primary Outcomes
Secondary Outcomes
2.2. Search Methods for Identification of Studies
2.2.1. Electronic Searches
2.2.2. Ongoing Trials Databases
2.2.3. Grey Literature
2.3. Data Collection and Analysis
2.3.1. Selection of Studies
2.3.2. Data Extraction and Management
2.3.3. Assessment of Risk of Bias of Included Studies
2.3.4. Measures of Treatment Effect
2.3.5. Unit of Analysis Issues
2.3.6. Dealing with Missing Data
2.3.7. Data Synthesis
3. Results
3.1. Results of the Search
3.2. Settings, Participants, and Interventions
3.3. Risk of Bias of Included Studies
3.4. Effects of Interventions
3.5. Primary Outcomes
3.5.1. Cytokines/Interleukins
3.5.2. C-Reactive Protein (CRP)
3.5.3. MMP-8
3.5.4. TIMP-1
3.5.5. HbA1c
3.6. Secondary Outcomes
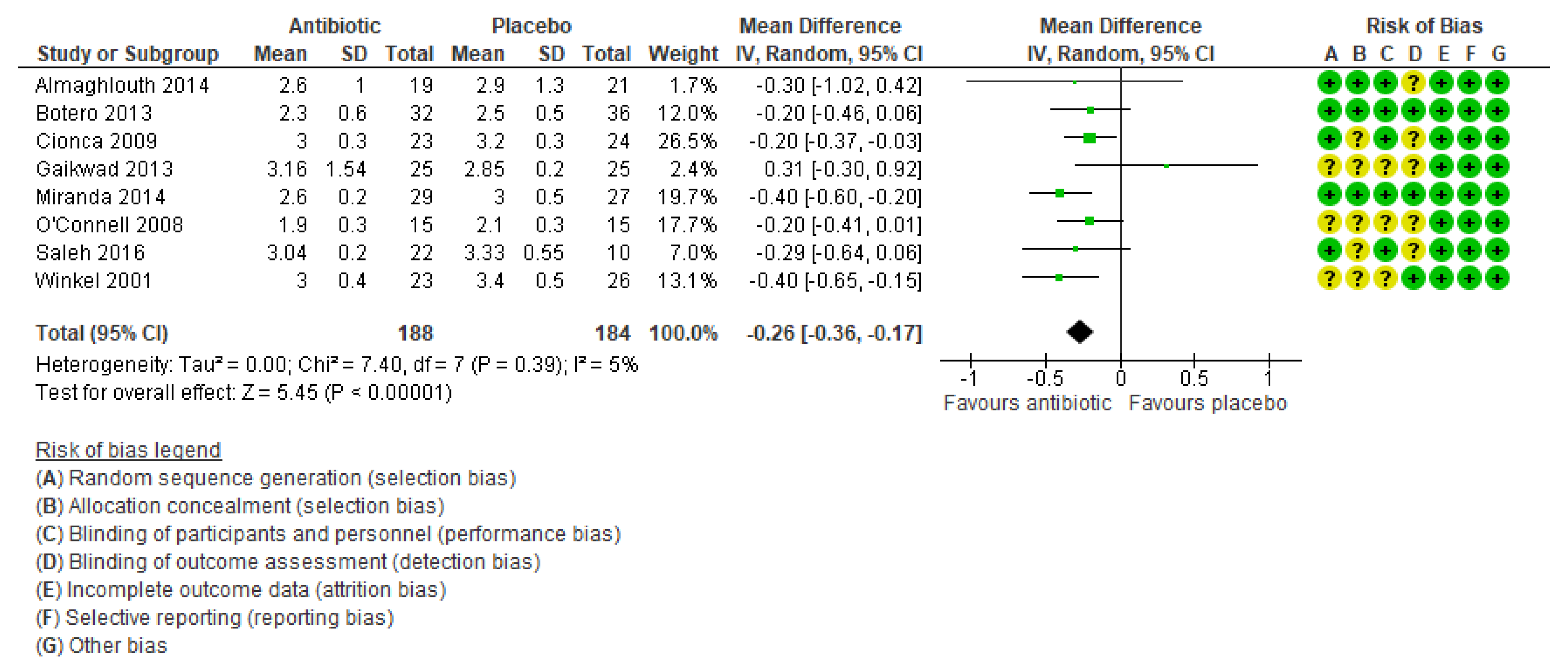
3.6.1. Probing Depth (PD)
(a) PD (mm)
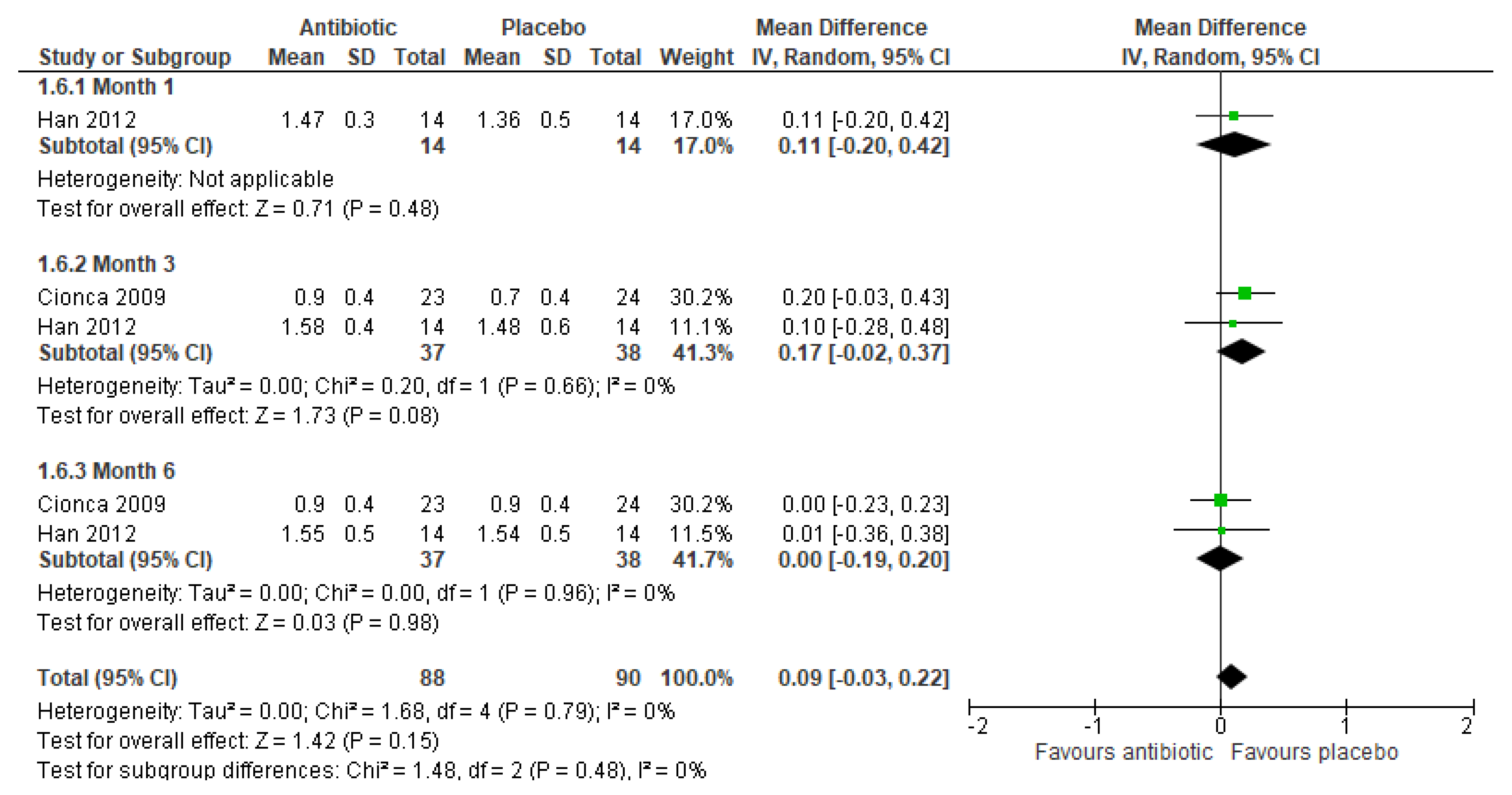
3.6.2. Clinical Attachment Level (CAL)
4. Discussion
5. Conclusions
5.1. Implications for Practice
5.2. Implications for Research
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
References
- WHO. Oral Health. Available online: https://www.who.int/news-room/fact-sheets/detail/oral-health (accessed on 5 May 2020).
- Nazir, M.A. Prevalence of periodontal disease, its association with systemic diseases and prevention. Int. J. Health Sci. Qassim 2017, 11, 72–80. [Google Scholar]
- Caton, J.G.; Armitage, G.; Berglundh, T.; Chapple, I.L.C.; Jepsen, S.; Kornman, K.S. A new classification scheme for periodontal and peri-implant diseases and conditions—Introduction and key changes from the 1999 classification. J. Clin. Periodontol. 2018, 45 (Suppl. 20), S1–S8. [Google Scholar] [CrossRef]
- WHO. Oral Health. What Is the Burden of Oral Disease? Available online: https://www.who.int/oral_health/disease_burden/global/en/ (accessed on 5 May 2020).
- Eke, P.I.; Dye, B.A.; Wei, L.; Slade, G.D.; Thornton-Evans, G.O.; Borgnakke, W.S.; Taylor, G.W.; Page, R.C.; Beck, J.D.; Genco, R.J. Update on Prevalence of Periodontitis in Adults in the United States: NHANES 2009 to 2012. J. Periodontol. 2015, 86, 611–622. [Google Scholar] [CrossRef] [Green Version]
- Kassebaum, N.J.; Bernabé, E.; Dahiya, M.; Bhandari, B.; Murray, C.J.; Marcenes, W. Global burden of severe periodontitis in 1990–2010: A systematic review and meta-regression. J. Dent. Res. 2014, 93, 1045–1053. [Google Scholar] [CrossRef]
- Bolerázska, B.; Mareková, M.; Markovská, N. Trends in Laboratory Diagnostic Methods in Periodontology. Acta Med. Hradec Kralove 2016, 59, 3–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kepic, T.J.; O’Leary, T.J.; Kafrawy, A.H. Total calculus removal: An attainable objective? J. Periodontol. 1990, 61, 16–20. [Google Scholar] [CrossRef]
- Hinrichs, J.E.; Wolff, L.F.; Pihlstrom, B.L.; Schaffer, E.M.; Liljemark, W.F.; Bandt, C.L. Effects of scaling and root planing on subgingival microbial proportions standardized in terms of their naturally occurring distribution. J. Periodontol. 1985, 56, 187–194. [Google Scholar] [CrossRef] [PubMed]
- Matthews, D.C. Prevention and treatment of periodontal diseases in primary care. Evid. Based Dent. 2014, 15, 68–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montebugnoli, L.; Servidio, D.; Miaton, R.A.; Prati, C.; Tricoci, P.; Melloni, C.; Melandri, G. Periodontal health improves systemic inflammatory and haemostatic status in subjects with coronary heart disease. J. Clin. Periodontol. 2005, 32, 188–192. [Google Scholar] [CrossRef]
- Iwamoto, Y.; Nishimura, F.; Soga, Y.; Takeuchi, K.; Kurihara, M.; Takashiba, S.; Murayama, Y. Antimicrobial periodontal treatment decreases serum C-reactive protein, tumor necrosis factor-alpha, but not adiponectin levels in patients with chronic periodontitis. J. Periodontol. 2003, 74, 1231–1236. [Google Scholar] [CrossRef]
- Heitz-Mayfield, L. Systemic antibiotics in periodontal therapy. Aust. Dent. J. 2009, 54, S96–S101. [Google Scholar] [CrossRef] [PubMed]
- Tüter, G.; Kurtiş, B.; Serdar, M.; Aykan, T.; Okyay, K.; Yücel, A.; Toyman, U.; Pinar, S.; Cemri, M.; Çengel, A.; et al. Effects of scaling and root planing and sub-antimicrobial dose doxycycline on oral and systemic biomarkers of disease in patients with both chronic periodontitis and coronary artery disease. J. Clin. Periodontol. 2007, 34, 673–681. [Google Scholar] [CrossRef] [PubMed]
- Emingil, G.; Gürkan, A.; Atilla, G.; Kantarci, A. Subantimicrobial-dose doxycycline and cytokine-chemokine levels in gingival crevicular fluid. J. Periodontol. 2011, 82, 452–461. [Google Scholar] [CrossRef]
- O’Connell, P.A.; Taba, M., Jr.; Nomizo, A.; Foss Freitas, M.C.; Suaid, F.A.; Uyemura, S.A.; Trevisan, G.L.; Novaes, A.B., Jr.; Souza, S.L.S.; Palioto, D.B.; et al. Effects of periodontal therapy on glycemic control and inflammatory markers. J. Periodontol. 2008, 79, 774–783. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Altman, D.G. Assessing risk of bias in included studies. In Cochrane Handbook for Systematic Reviews of Interventions; Cochrane: London, UK, 2008; pp. 187–241. [Google Scholar]
- Guyatt, G.; Oxman, A.D.; Akl, E.A.; Kunz, R.; Vist, G.; Brozek, J.; Norris, S.; Falck-Ytter, Y.; Glasziou, P.; de Beer, H.; et al. GRADE guidelines: 1. Introduction-GRADE evidence profiles and summary of findings tables. J. Clin. Epidemiol. 2011, 64, 383–394. [Google Scholar] [CrossRef] [PubMed]
- Almaghlouth, A.A.; Cionca, N.; Cancela, J.A.; Décaillet, F.; Courvoisier, D.S.; Giannopoulou, C.; Mombelli, A. Effect of periodontal treatment on peak serum levels of inflammatory markers. Clin. Oral. Investig. 2014, 18, 2113–2121. [Google Scholar] [CrossRef]
- Botero, J.E.; Yepes, F.L.; Ochoa, S.P.; Hincapie, J.P.; Roldan, N.; Ospina, C.A.; Castrillon, C.A.; Becerra, M.A. Effects of periodontal non-surgical therapy plus azithromycin on glycemic control in patients with diabetes: A randomized clinical trial. J. Periodontal. Res. 2013, 48, 706–712. [Google Scholar] [CrossRef]
- Cionca, N.; Giannopoulou, C.; Ugolotti, G.; Mombelli, A. Amoxicillin and metronidazole as an adjunct to full-mouth scaling and root planing of chronic periodontitis. J. Periodontol. 2009, 80, 364–371. [Google Scholar] [CrossRef]
- Engebretson, S.P.; Hey-Hadavi, J. Sub-Antimicrobial doxycycline for periodontitis reduces hemoglobin A1c in subjects with type 2 diabetes: A pilot study. Pharmacol. Res. 2011, 64, 624–629. [Google Scholar] [CrossRef] [Green Version]
- Gaikwad, S.P.; Gurav, A.N.; Shete, A.R.; Desarda, H.M. Effect of scaling and root planing combined with systemic doxycycline therapy on glycemic control in diabetes mellitus subjects with chronic generalized periodontitis: A clinical study. J. Periodontal. Implant Sci. 2013, 43, 79–86. [Google Scholar] [CrossRef]
- Gilowski, L.; Kondzielnik, P.; Wiench, R.; Płocica, I.; Strojek, K.; Krzemiński, T.F. Efficacy of short-term adjunctive subantimicrobial dose doxycycline in diabetic patients—Randomized study. Oral Dis. 2012, 18, 763–770. [Google Scholar] [CrossRef]
- Golub, L.M.; McNamara, T.F.; Ryan, M.E.; Kohut, B.; Blieden, T.; Payonk, G.; Sipos, T.; Baron, H.H. Adjunctive treatment with subantimicrobial doses of doxycycline: Effects on gingival fluid collagenase activity and attachment loss in adult periodontitis. J. Clin. Periodontol. 2001, 28, 146–156. [Google Scholar] [CrossRef] [PubMed]
- Golub, L.M.; Lee, H.M.; Stoner, J.A.; Sorsa, T.; Reinhardt, R.A.; Wolff, M.S.; Ryan, M.E.; Nummikoski, P.V.; Payne, J.B. Subantimicrobial-dose doxycycline modulates gingival crevicular fluid biomarkers of periodontitis in postmenopausal osteopenic women. J. Periodontol. 2008, 79, 140–218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Han, B.; Emingil, G.; Özdemir, G.; Tervahartiala, T.; Vural, C.; Atilla, G.; Baylas, H.; Sorsa, T. Azithromycin as an adjunctive treatment of generalized severe chronic periodontitis: Clinical, microbiologic, and biochemical parameters. J. Periodontol. 2012, 83, 1480–1491. [Google Scholar] [CrossRef]
- Jones, J.A.; Miller, D.R.; Wehler, C.J.; Rich, S.E.; Krall-Kaye, E.A.; McCoy, L.C.; Christiansen, C.L.; Rothendler, J.A.; Garcia, R.I. Does periodontal care improve glycemic control? The Department of Veterans Affairs Dental Diabetes Study. J. Clin. Periodontol. 2007, 34, 46–52. [Google Scholar] [CrossRef] [PubMed]
- López, N.J.; Quintero, A.; Casanova, P.A.; Ibieta, C.I.; Baelum, V.; López, R. Effects of periodontal therapy on systemic markers of inflammation in patients with metabolic syndrome: A controlled clinical trial. J. Periodontol. 2012, 83, 267–278. [Google Scholar] [CrossRef]
- Miranda, T.S.; Feres, M.; Perez-Chaparro, P.J.; Faveri, M.; Figueiredo, L.C.; Tamashiro, N.S.; Ferreira Bastos, M.; Mendes Duarte, P. Metronidazole and amoxicillin as adjuncts to scaling and root planing for the treatment of type 2 diabetic subjects with periodontitis: 1-Year outcomes of a randomized placebo-controlled clinical trial. J. Clin. Periodontol. 2014, 41, 890–899. [Google Scholar] [CrossRef]
- Payne, J.B.; Golub, L.M.; Stoner, J.A.; Lee, H.M.; Reinhardt, R.A.; Sorsa, T.; Stepian, M.J. The effect of subantimicrobial-dose-doxycycline periodontal therapy on serum biomarkers of systemic inflammation: A randomized, double-masked, placebo-controlled clinical trial. J. Am. Dent. Assoc. 2011, 142, 262–273. [Google Scholar] [CrossRef]
- Rooney, J.; Wade, W.G.; Sprague, S.V.; Newcombe, R.G.; Addy, M. Adjunctive effects to non-surgical periodontal therapy of systemic metronidazole and amoxycillin alone and combined. A placebo controlled study. J Clin. Periodontol. 2002, 29, 342–350. [Google Scholar] [CrossRef]
- Saleh, A.; Rincon, J.; Tan, A.; Firth, M. Comparison of adjunctive azithromycin and amoxicillin/metronidazole for patients with chronic periodontitis: Preliminary randomized control trial. Aust. Dent. J. 2016, 61, 469–481. [Google Scholar] [CrossRef] [Green Version]
- Winkel, E.G.; Van Winkelhoff, A.J.; Timmerman, M.F.; Van der Velden, U.; Van der Weijden, G.A. Amoxicillin plus metronidazole in the treatment of adult periodontitis patients. A double-blind placebo-controlled study. J. Clin. Periodontol. 2001, 28, 296–305. [Google Scholar] [CrossRef]
- Soto-Franco, J.E.; Aldana, H.F.; Navia, J.M.; Peláez, M.; Quisoboni, J.; O’Meara, M.A.; Contreras, A. Efectos del raspaje y alisado radicular a boca completa con azitromicina sobre los niveles de proteina C reactiva ultra sensible, parametros clínicos y microbiológicos periodontales. Ensayo clinico aleatorizado. Rev. Estomatol. 2016, 24, 14–25. [Google Scholar] [CrossRef]
- Teughels, W.; Feres, M.; Oud, V.; Martín, C.; Matesanz, P.; Herrera, D. Adjunctive effect of systemic antimicrobials in periodontitis therapy. A systematic review and meta-analysis. J. Clin. Periodontol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Keestra, J.A.; Grosjean, I.; Coucke, W.; Quirynen, M.; Teughels, W. Non-Surgical periodontal therapy with systemic antibiotics in patients with untreated chronic periodontitis: A systematic review and meta-analysis. J. Periodontal. Res. 2015, 50, 294–314. [Google Scholar] [CrossRef] [PubMed]
- Borges, I.; Faveri, M.; Figueiredo, L.C.; Duarte, P.M.; Retamal-Valdes, B.; Montenegro, S.C.L.; Feres, M. Different antibiotic protocols in the treatment of severe chronic periodontitis: A 1-year randomized trial. J. Clin. Periodontol. 2017, 44, 822–832. [Google Scholar] [CrossRef] [PubMed]
- Shaddox, L.M.; Walker, C. Microbial testing in periodontics: Value, limitations and future directions. Periodontology 2000 2009, 50, 25–38. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J.J. Programmed cell death in the immune system. In Advances in Immunology; Elsevier: Amsterdam, The Netherlands, 1991; Volume 50, pp. 55–85. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study ID | Country and Setting | Patients | Trial Duration | Intervention | Control |
|---|---|---|---|---|---|
| Almaghlouth 2014 [19] | School of Dental Medicine of the University of Geneva, Switzerland | 40 patients with moderate-to-advanced periodontitis, aged 25–70 years | 3 months | 500 mg Metronidazole+ 375 mg Amoxicillin three times a day for 7 days | No placebo |
| Botero 2013 [20] | San Vicente de Paul Hospital Medellin, Colombia, South America | 105 adults diagnosed with moderate periodontitis and diabetes | 18 months | Azithromycin tablet 500 mg daily for 3 days (Group 1: Az+Scaling, Group 2: Az+Prophylaxis) | Placebo |
| Cionca 2009 [21] | School of Dental Medicine, University of Geneva, Switzerland | 51 adult patients with moderate to advanced periodontitis, between ages of 25–70 years | 1 year | 500 mg Metronidazole & 375 mg Amoxicillin t.i.d × 7 days | Placebo capsules of 500 mg and 375 mg t.i.d. × 7 days |
| Engebretson 2011 [22] | Naomi Berrie Centre and Department of Periodontics, Columbia University Medical Centre, USA | 45 Type 2 diabetes patients with chronic periodontitis, aged 50–56 years. | 3 months | Group 1: 20 mg Sub-antimicrobial dose doxycycline (SDD) b.i.d × 3 months Group 2: 100 mg ADD daily × 3 months | Placebo daily × 3 months |
| Gaikwad 2013 [23] | Department of Periodontics, Tatyasaheb Kore Dental College, India | 50 diabetes patients with chronic generalised periodontitis aged 30–70 years. | 3 months | 100 mg Doxycycline once daily for 15 days | No placebo |
| Gilowski 2012 [24] | Medical University of Silesia, Katowice, Poland | 34 type 2 diabetes patients with chronic periodontitis, aged 36–68 years | 3 months | 20 mg doxycycline hydrochloride three times a day for 3 months | No placebo |
| Golub 2008 [26] and Payne 2011 [31] | University of Nebraska Medical Centre College of Dentistry and the School of Dental Medicine at Stonybrook University, Stoney Brook, USA | 128 Osteopenic post-menopausal women with moderate to advanced periodontitis between the ages of 45–70 years | 2 years | 20 mg Sub-antimicrobial dose doxycycline (SDD) × 3 times a day for 2 years | 20 mg Placebo × 3 times a day for 2 years |
| Golub 2001 [25] | Department of Oral Biology & Pathology, School of Dental Medicine, State University of New York at Stony Brook, USA | 174 adult patients with chronic periodontitis aged 18–75 years | 9 months | Group 1–4 Doxycycline 20 mg × 12 weeks (in different combinations) | Placebo × 12 weeks |
| Han 2012 [27] | Department of Periodontology, School of Dentistry, Ege University, Izmir, Turkey | 36 patients with severe generalised chronic periodontitis in the age range of 35–54 years | 6 months | 500 mg Azithromycin once daily × 3 days | 500 mg Placebo once daily for 3 days |
| Jones 2007 [28] | All four departments of Veterans Administration facilities at Greater Boston, USA | 165 diabetes patients with periodontitis, mean (SD) age of 59.1(11) years | 4 months | 100 mg doxycycline daily for 14 days | Usual care with no placebo |
| Lopez 2012 [29] | Dr. Eloisa Diaz Dental Center, San José Hospital, Santiago, Chile | 165 patients with Metabolic Syndrome (MetS) having periodontitis, between the ages of 35–65 years | 1 year | 250 mg Metronidazole t.i.d AND 500 mg Amoxicillin t.i.d for 7 days | 250 mg placebo t.i.d AND 500 mg placebo t.i.d for 7 days |
| Miranda 2014 [30] | Department of Periodontology, Dental Research Division, Guarulhos University, Sao Paulo, Brazil | 58 Type 2 diabetes patients with generalized chronic periodontitis, aged 35 years or more. | 1 year | 400 mg Metronidazole+ 500 mg Amoxycillin three times a day for 14 days | Placebo |
| O’Connell 2008 [15] | Department of Oral Surgery & Periodontology, University of São Paulo Ribeiro-Preto, Brazil | 30 Type 2 diabetes patients with periodontitis, aged 46–70 years | 3 months | 100 mg Doxycycline once daily for 2 weeks after an initial dose of 200 mg | Placebo once daily for 2 weeks after initial dose of placebo |
| Rooney 2002 [32] | Department of Periodontology at Bristol Dental School and Hospital, USA | 66 patients with advanced chronic periodontal disease between the ages of 20–45 years | 6 months | Group 1 (AM): 250 mg Amoxycillin (capsule) and 200 mg metronidazole (tablet). Group 2 (PM): 200 mg metronidazole (tablet) and placebo (lactose capsules). Group 3 (AP): 250 mg Amoxycillin (capsule) and placebo (calcium lactate tablets). | Placebo (lactose capsules) and placebo (calcium lactate tablets). |
| Saleh 2016 [33] | Oral Health Centre, University of Western Australia, Australia | 37 adults with generalized moderate to advanced chronic periodontitis, age of 30 years and older | 3 months | Group 1: 500 mg Amoxicillin and 200 mg Metronidazole administered every 8 h for 7 days Group 2: 500 mg Azithromycin administered every 8 h for 7 days | Placebo capsules were administered every 8 h for 7 days |
| Soto 2016 [35] | Two university clinics in the city of Cali (Colombia), and the Universidad del Valle (university of Valle) | 81 patients with moderate to severe chronic periodontitis, aged between 25 and 70 years | 12 weeks | 500 mg Azithromycin per day, for 5 days | Placebo |
| Tuter 2007 [13] | Department of periodontology of Gazi University, Ankara, Turkey | 36 patients with both chronic periodontitis and coronary artery disease (CAD), and age < 70 years | 6 weeks | 20 mg Sub-antimicrobial dose doxycycline (SDD) three times daily for 6 weeks | 20 mg Placebo, three times daily for 6 weeks |
| Winkel 2001 [34] | Clinic for Periodontology Amsterdam and the Clinic for Periodontology Utrecht, The Netherlands | 49 patients with generalised severe periodontitis, mean age of at least 40 years | 6 months | 375 mg Amoxicillin in combination with 250 mg metronidazole to be taken every 8 h for next 7 days was given. | Similar placebos every 8 h for next 7 days was given |
| Summary of Findings Table: | ||||||
| Antibiotic compared to placebo in the treatment of chronic periodontitis | ||||||
| Patient or population: Adult patients diagnosed with chronic periodontitis Setting: Academic dentistry hospitals or clinics in developed countries Intervention and Comparison: Antibiotic compared placebo or no antibiotic | ||||||
| Outcomes | Anticipated Absolute Effects * (95% CI) | Relative Effect (95% CI) | № of Participants (studies) | Certainty of the Evidence (GRADE) | Comments | |
| Risk with Placebo | Risk with Antibiotic | |||||
| Pocket depth (mm) at 3 months | The mean pocket depth (mm) at 3 months was 0 | MD 0.26 lower (0.36 lower to 0.17 lower) | - | 372 (8 RCTs) | ⨁⨁⨁◯ MODERATE a | Meta-analysis of eight studies with 372 participants show an antibiotic effect of reducing pocket depth by 0.26 mm compared to the placebo (moderate certainty of evidence). One other study found reduction in favour of the antibiotics, however results were presented as medians and ranges. Three other studies found little or no difference between the antibiotic and placebo groups. |
| Glycosylated Haemoglobin (HbA1c) | See comment | not pooled | - | 487 (7 RCTs) | ⨁◯◯◯ VERY LOW b,c | Six studies with 382 participants found little or no difference in the effect of antibiotics on haemoglobin levels compared to the placebo group. One study with 105 participants was unclear on the differences between the antibiotic and placebo groups. |
| MMP-8 | See comment | not pooled | - | 234 (4 RCTs) | ⨁◯◯◯ VERY LOW c,d | Three small studies with 106 participants found little or no impact of antibiotic therapy on MMP-8 levels. One study with 128 participants found a 60% reduction in favour of antibiotics during a 2-year period. |
| C-Reactive Protein (CRP) | See comment | not pooled | - | 504 (5 RCTs) | ⨁⨁◯◯ LOW c | Three studies with 282 participants found little or no difference in CRP levels between the antibiotic and placebo groups. One study with 40 participants was unclear on the inter-group differences. One study with 182 participants found a small antibiotic effect of 18% decrease. |
| * The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; MD: Mean difference | ||||||
| GRADE Working Group grades of evidence High certainty: We are very confident that the true effect lies close to that of the estimate of the effect Moderate certainty: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low certainty: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect Very low certainty: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect | ||||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Munasur, S.L.; Turawa, E.B.; Chikte, U.M.E.; Musekiwa, A. Mechanical Debridement with Antibiotics in the Treatment of Chronic Periodontitis: Effect on Systemic Biomarkers―A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 5601. https://doi.org/10.3390/ijerph17155601
Munasur SL, Turawa EB, Chikte UME, Musekiwa A. Mechanical Debridement with Antibiotics in the Treatment of Chronic Periodontitis: Effect on Systemic Biomarkers―A Systematic Review. International Journal of Environmental Research and Public Health. 2020; 17(15):5601. https://doi.org/10.3390/ijerph17155601
Chicago/Turabian StyleMunasur, Sudhir L., Eunice B. Turawa, Usuf M.E. Chikte, and Alfred Musekiwa. 2020. "Mechanical Debridement with Antibiotics in the Treatment of Chronic Periodontitis: Effect on Systemic Biomarkers―A Systematic Review" International Journal of Environmental Research and Public Health 17, no. 15: 5601. https://doi.org/10.3390/ijerph17155601