1. Introduction
Medication adherence is important in patients with chronic diseases. These are defined as “conditions that last one year or more and require ongoing medical attention or limit activities of daily living or both” and broadly include diseases such as high blood pressure, stroke, cancer, and chronic lung disease [
1]. Chronic diseases often require patients to take medications throughout their life. Without proper adherence to prescribed medications, patients are prone to progression of disease, death, and increased healthcare use and costs [
2], and research showed that, after the first six months of medication therapy for chronic diseases, the rates of medication adherence drop substantially, by as much as 50% [
3,
4]. Past research showed that the prevalence of medication non-adherence in East Asia ranges from 19.8 to 51.0% across chronic diseases of epilepsy, stroke, diabetes, and high blood pressure [
5,
6,
7,
8]. The reasons for non-adherence mostly corresponded to the five dimensions of adherence defined by the World Health Organization [
9], including social and economic factors, healthcare team and system-related factors, condition-related factors, therapy-related factors, and patient-related factors. In particular, patient-related factors are especially complex due to difficulties in measurement and limited effective interventions.
Several instruments for measuring medication adherence have been developed [
10,
11,
12,
13,
14,
15]. These instruments mostly measure barriers to adherence, adherence to recommendations, and adherence behaviors in patients with chronic diseases via self-administered questionnaires. However, limitations of existing scales have been identified [
16,
17], such as limited reasons for non-adherence captured leading to difficulty for targeted intervention. If the scale is too brief to report the extent of non-adherence and reveal the reasons for non-adherence, the non-adherence rate may be underestimated and the issues contributing to non-adherence may remain unresolved.
To improve upon the limitations of earlier scales, Unni and colleagues [
17,
18] developed the Medication Adherence Reason Scale (MAR-Scale), which contains a comprehensive list of reasons for non-adherence that can be used to inform issues including belief, self-perception, forgetfulness, management, and availability. It has been tested in patients with high cholesterol and asthma in the U.S., with good psychometric properties. An updated MAR-Scale has been further validated in 17 different chronic conditions with acceptable reliability, which shows its utility to capture reasons for medication non-adherence across disease states [
19].
Currently, there are limited scales that aim to provide reasons for non-adherence to blood pressure medications in the Chinese population. Although several Chinese versions were used in measuring adherence to medication in patients with epilepsy, myocardial infarction, and high blood pressure, these are limited in recognizing the potential reasons for non-adherent behaviors in patients [
5,
20,
21,
22]. Therefore, to develop a new adherence scale that is adapted to cultural and healthcare system differences is in demand. The objectives of this study are twofold: (1) translate the MAR-Scale into Chinese and examine its psychometric properties and cultural adaptation among patients with high blood pressure in Taiwan; (2) characterize medication non-adherence issues among these patients using the Chinese version of the Medication Adherence Reasons Scale (ChMAR-Scale).
2. Materials and Methods
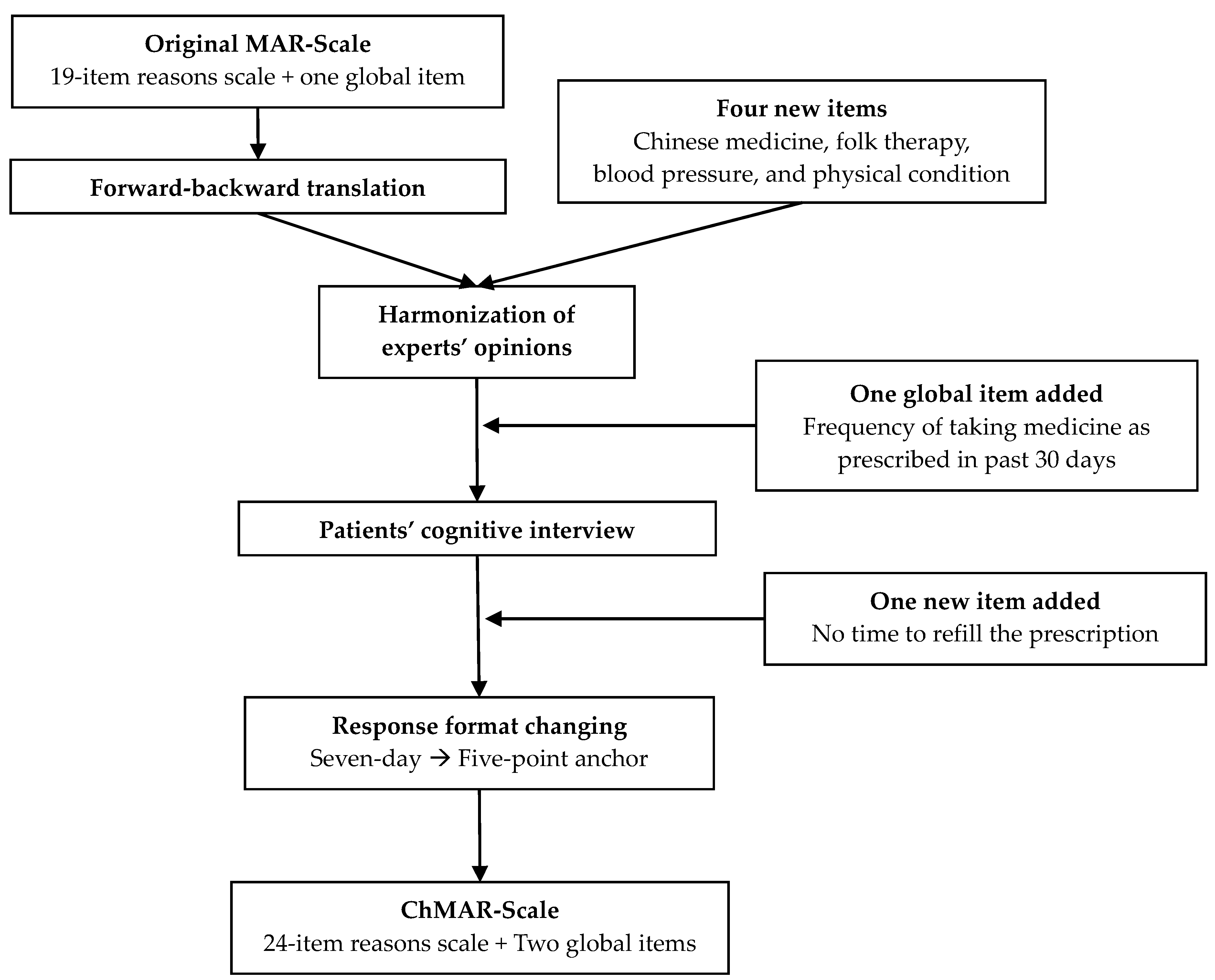
The original MAR-Scale was translated into Chinese (
Figure 1) following the “Principles of Good Practice for the Translation and Cultural Adaptation Process for Patient-Reported Outcomes (PRO) Measures” [
23]. Forward translation of the English version of the MAR-Scale to Chinese was performed by two independent translators who were native speakers of Chinese and proficient in English. After reconciliation, a bilingual pharmacist with a doctor of pharmacy degree back-translated the forward translation into English. The researchers then compared the forward and backward translations and the original text and conducted another round of reconciliation. To ensure content validity, five subject experts (three professors with administrative pharmacy specialty and two hospital pharmacists) were asked to review the translation appropriateness of the “pre-expert review” version and assess the cultural adaptation of each item. The experts recommended changing the response format from a seven-day anchor to a five-point anchor. Another reconciliation was conducted after obtaining the experts’ opinions. The draft of the questionnaire was then distributed to 10 adults with high blood pressure for cognitive interviews based on convenience sampling. A “think aloud process” was used to assess the level of their comprehensibility of each item of the ChMAR-Scale. The patients were asked to complete both the seven-day anchor and five-point anchor scales to determine which of the response formats they would be more likely to complete. After modifying the questionnaire and proofreading, the final version was completed.
At least six revisions of the questionnaire were produced after the initial translation. Firstly, the response format was changed to a five-point scale due to the experts’ opinions and evidence that respondents had difficulty filling out the original seven-day response format. Secondly, the scale focused on medication use over the past month rather than week, as several items were not applicable when asking only about the past week, such as the frequency of medication pick-up, which is typically once monthly. Thirdly, new items based on past research regarding cultural differences, such as “Chinese Medicine or herbal use, folk therapy, change dosage according to blood pressure (BP) or physical condition”, were added into the ChMAR-Scale. “No time to refill the prescription in the pharmacy” was also added to the scale based on cognitive interviews. Fourthly, one additional five-point global item asking, “Over the last 30 days, how often were you able to take your blood pressure medicine exactly as prescribed?” was added. Finally, during the cognitive interviews, several patients filled in the items asking “how often they had this kind of thought” but not “how often they were unable to take the medicine because of these reasons” after cognitive interview. To avoid this confusion, we added a sentence, “The frequency you missed taking medicine as prescribed due to various reasons of the following items”, above every item. The final ChMAR-Scale includes 24 items of non-adherent reasons and two global items of non-adherence.
A cross-sectional survey design was used to validate the data. The survey questionnaire had 45 items, which included medication non-adherence (Visual Analog Scale (VAS), ChMAR-Scale); patient demographics (sex, age, education level, monthly salary, smoking history); disease characteristics (comorbidity and most recent BP measurement); treatment characteristics (treatment duration, regimen, dosing, and Chinese medicine, herbal, and folk therapy use). Following previous MAR-Scale studies, participants were categorized as non-adherent if they did not answer “never” on one or more items. BP was considered controlled if (1) systolic/diastolic BP < 140/90 mmHg in patients with diabetes or chronic kidney disease; (2) systolic/diastolic BP < 140/90 mmHg in patients without diabetes or chronic kidney disease and <60 years old; (3) systolic/diastolic BP < 150/90 mmHg in patients without diabetes or chronic kidney disease and ≥60 years old [
24].
The Visual Analog Scale (VAS) developed by Nau et al. was used to validate the new scale [
25]. The VAS has a single item asking, “What percentage of time over the past 30 days did you take your prescribed blood pressure medicine?” The individuals were guided to mark an “X” on a horizontal line which was anchored by 0% and 100%. The VAS was translated into Chinese by the researchers. Thirteen individuals with pharmacy backgrounds and four lay-persons were asked to read the translated VAS. The Chinese VAS was finalized based on the feedback from these experts.
A cross-sectional design was used, and the study was conducted between February and May 2016. The subjects were recruited in a regional hospital and eight community pharmacies in the Taipei metropolitan area to maintain diversity among patients. The inclusion criteria of the study were (1) 20 years or older and diagnosed with high blood pressure by a physician and (2) people who had taken blood pressure medicine. The exclusion criterion was an inability to communicate in Chinese.
The recruitment was conducted based on convenience sampling by P.F.C. in the hospital, while the recruitment in the community pharmacies was conducted by the community pharmacists. The community pharmacists were individually trained based on a page of standardized instructions about the criteria for recruiting patients, and they were given one reminder about recruiting after a month. Patients were recruited if they were picking up prescriptions for blood pressure medicine and showed an interest in participation after a brief explanation of the study. The recruiters assisted patients in answering the questions regarding which blood pressure medicine they were using. In addition, patients who could not read Chinese were assisted by the recruiters by reading each item for them. Two screening questions were asked at the beginning of the questionnaire to confirm that patients met the two inclusion criteria described above. A gift equivalent to $1 USD was provided as an incentive to each patient completing the questionnaire. The data were transcribed and checked by different investigators to ensure accuracy.
Descriptive analysis was completed to examine the demographic data and responses in the ChMAR-Scale. Item analysis, factor analysis, cross-validation, and Cronbach’s alpha were conducted to assess construct validity and reliability [
26,
27]. Principle axis factoring, varimax rotation, and the Kaiser criterion were used to examine the underlying factors in the exploratory factor analysis. Cramer’s V and the kappa coefficient were used to examine the criterion-related validity between the new scale and the Chinese VAS, Global Item 1 (taking medicine for the past seven days), and Global Item 2 (adherence to the prescription over the past 30 days) [
28]. Listwise deletion was used for missing data. For validation purposes, adherence measures were dichotomized, and non-adherence was defined for each item as the following: (1) participants who did not answer “never” on at least one item in the ChMAR-Scale, (2) those who did not answer “100%” in the VAS, (3) participants who did not state that they took seven days of blood pressure medicine as prescribed over the past week in Global Item 1, and (4) participants who did not answer that they had adhered consistently over the past 30 days in Global Item 2.
The research protocol was approved by the Taipei Medical University Joint Institutional Review Board (N201512008) with a waiver of informed consent.
3. Results
A total of 621 patients were recruited and 574 questionnaires were returned, with an effective sample size of 538 (response rate 86.6%). A total of 64% of the questionnaires were collected in the hospital and 36% were collected in community pharmacies. A total of 36 questionnaires were excluded because respondents did not meet the inclusion criteria for the study for the following reasons: (1) patients not diagnosed with high blood pressure or (2) patients not taking blood pressure medicine. Over half of our respondents were male (55.4%) and less than 65 years old (53.2%) (
Table 1). Participants with less than high school education accounted for a significant proportion (40.3%). Over half of participants (50.3%) had taken blood pressure medicine for more than six years; most of them took the blood pressure medicine once a day (72.8%) and one or less pill (59.6%). Based on the ChMAR-Scale, 61.7% of the respondents were non-adherent with their blood pressure medicine. Overall, 67.5% of the participants had BP under control. In the adherence group, 74.9% had the BP under control, which was significantly higher than the non-adherence group (
Table 2).
3.1. Criterion-Related Validity
In the comparative analysis of the ChMAR-Scale and the VAS, the correlation of the two scales was 0.525 and was significant at the level of 0.001. The performance of the ChMAR-Scale in comparison to the VAS and two global items is listed in
Table 3. There were 142 patients identified as non-adherent by the ChMAR-Scale, but they were identified as adherents by the VAS. Comparatively, there were 10 participants recognized as adherents by the ChMAR-Scale, but they were identified as non-adherents by the VAS. In the comparison of the ChMAR-Scale and the global items, the correlations were 0.436 with Global Item 1 and 0.502 with Global Item 2. Both were significant at the level of 0.001.
3.2. Construct Validity
The Kaiser criterion suggested six factors to be retained in the ChMAR-Scale, and the total variance explained by the factors was 56%. The first factor reflected the concern or belief about social or personal issues that hindered adherence and was named “belief issues”. The second factor was named “self-perception issues” and reflected the idea of controlling their condition based on their physical condition and how they felt. The third extracted factor dealt with non-adherence due to several “forgetfulness” issues. The fourth factor reflected the issue of “managing issues”. “Availability issues” was the fifth extracted factor, reflecting the issue of difficulty in obtaining prescribed medicine in the pharmacy. The last three items about Chinese medicine, folk therapy, and cost issue were named “miscellaneous”, constituting the sixth factor. The factor loading for each item was above acceptable levels and ranged from 0.365 to 0.775 (
Table 4).
3.3. Reliability
The six domains had acceptable Cronbach’s alpha values ranging from 0.649 to 0.852, all above the acceptable value of 0.6. The item-total correlation ranged from 0.362 to 0.719 and demonstrated good reliability. Item analysis suggested dropping items Q11, Q21, and Q24; however, the three items were all retained because of conceptual importance.
3.4. Quantifying Non-Adherence
The ChMAR-Scale was able to identify more non-adherence to medication-taking behavior than the VAS: the ChMAR-Scale identified 61.6% of the respondents as non-adherent while the VAS identified 36.9% as non-adherents. Global Items 1 and 2 only identified 24.1% and 36.4% of participants as non-adherents, respectively.
In the responses to the VAS, the mean adherence score was 89.3%. Most respondents (63.1%) were being adherent “100% of the time” over the last 30 days in the VAS. In Global Item 2, 63.6% of participants indicated that they “always” were able to take the blood pressure medicine exactly as prescribed over the last 30 days. The responses of “always” to Global Item 2 and “100%” in the VAS were consistent. When asked about adherence over the last seven days, most (75.9%) reported that they were able to take their blood pressure medicine every day. The average number of days that participants were able to follow the physicians’ prescription was 3.46 (SD: 0.902), 51% of the time. Patients reported better adherence in a shorter interval (past seven days) than in a longer interval (past 30 days).
Forgetfulness issues were the most common non-adherence reasons among the participants. A total of 36% of the respondents simply missed a dose (Q12), 30.1% had problems forgetting things in daily life (Q13), and 27.5% forgot to take blood pressure medicine due to a busy life (Q14). The next most common reason was belief issues. Many of the participants were non-adherent because of worrying about the side effects (Q1: 26.4%) or the long-term effects (Q2: 27.7%) of the blood pressure medicine. A total of 27% of the respondents were non-adherent due to personal reasons. Additionally, many of the participants stopped taking their blood pressure medicine to see if they still needed it (Q3:24%). Around 22% reported changing the usage of their blood pressure medicine based on their physical condition (Q9: 22.7%) and BP (Q10: 22.1%). The least common reasons for non-adherence were using a non-traditional therapy (Q22: 3.2%; Q23: 5%), the pharmacy having no supply of medicine (Q21: 5%), and cost issues (Q24: 4.5%).
4. Discussion
The ChMAR-Scale was translated from the MAR-Scale and modified based on cultural and healthcare system differences, and its criterion-related validity, construct validity, and reliability each showed acceptable to good psychometric properties. Moreover, the ChMAR-Scale identified more patients with non-adherence than other global items in this study, signifying the value of the new scale in identifying patients needing further attention for medication adherence issues.
Compared to previous validated adherence scales in Chinese, the 24-item ChMAR-Scale provides a comprehensive framework addressing more belief, perception, and management as well as availability issues in medication-taking behaviors. As such, the ChMAR-Scale can serve as a screening tool prior to appointments with healthcare providers, which can not only prepare the patient to ask more questions about their medications but also allow the healthcare provider to examine whether there are areas for improvement in terms of the complexity of treatment and social support needed. This is especially important in the Chinese community because of the large patient volume typically seen in hospitals, leading to limited time per visit as well as patients’ tendency to be conservative and avoid conflicts in communications based on cultural roots [
29].
In addition to serving as a screening tool for healthcare providers, the ChMAR-Scale has the potential to be used as a follow-up and research tool for evaluating the long-term effectiveness of counseling interventions aimed at improving medication adherence. Given that many personal and healthcare system barriers addressed in the ChMAR-Scale are not easy to address in a single visit, the tool can be helpful in developing a long-term plan for improving medication adherence. Future studies could not only examine the sensitivity of the ChMAR-Scale in capturing intervention effectiveness but also examine how healthcare providers can better prioritize how to address different reasons for non-adherence.
The ChMAR-Scale showed psychometric properties similar to the original MAR-Scale, with good factor loadings, item-total correlations, and acceptable Cronbach’s alphas. A major difference is that the ChMAR-Scale identified six domains whereas the original MAR-Scale only had four domains. While belief issues, forgetfulness, and managing issues in the ChMAR-Scale directly correspond to existing domains in the original scale, the ChMAR-Scale highlighted factors regarding self-perception issues, availability, and miscellaneous issues. This finding is reasonable due to two reasons: firstly, there were purposive efforts to culturally adapt the instrument based on differences in healthcare systems and cultural needs in this study, and the findings support the need for the additional items. Secondly, the number of factors contributing to non-adherence may be different across disease states. For example, in this study, blood pressure is a visible outcome for patients to self-manage at home; however, in the validation of the original MAR-Scale, patients used cholesterol lowering and asthma medication as preventive treatments, which are more intangible. Therefore, self-perceptions might have stronger influences on medication adherence in patients with high blood pressure.
Based on the characteristics of non-adherence behaviors in this sample, the most common reasons were forgetfulness, concerns about side effects or long-term effects, and self-adjustment of medications according to BP, physical condition, or to check whether it was still needed. In the US, forgetfulness issues, patients’ concerns about side effects or long-term effects, and cost concerns were also common non-adherence reasons [
30]. One explanation of the differences in cost concern, which is a less important reason for non-adherence in Taiwan, is likely due to most blood pressure medications being covered by National Health Insurance.
Except for the cost issue, few people stop their blood pressure medications to switch to alternative therapy. The reason may be the low responses of non-adherence due to our sampling methods. People who visit the hospital or pharmacy may be less likely to seek non-traditional therapy. Another reason is that people may view non-traditional therapy as interfering with blood pressure medications.
There were limitations in this study. Firstly, data were only collected at one hospital and eight pharmacies in the Taipei metropolitan area, thus limiting the generalizability. Secondly, recall bias, which means recalling information more or less compared to actual situations, might occur as many respondents were not familiar with their medications. Thirdly, social desirability bias, which means the respondent reports favorable answers to researchers, might have influenced the self-reported results to be different from reality. Fourthly, blood pressure values of the most recent measurement were based on self-report and underestimation of blood pressure control is likely. Nevertheless, participants were encouraged to use hospital or pharmacy devices whenever possible. Finally, while we showed reliability in terms of internal consistency measures; we were unable to conduct test-retest reliability due to practical issues in recruitment.
5. Conclusions
The new ChMAR-Scale identified more comprehensive reasons for non-adherence and showed good validity and acceptable to good reliability. It can be incorporated into practice settings for screening and follow-up purposes to facilitate communications between healthcare providers and patients. This study also identified forgetfulness, belief issues, and self-perception issues as common reasons for non-adherence and can be informative for healthcare providers while consulting patients. Future studies could further examine the scale in different disease conditions among variable populations and settings and test the sensitivity of the scale to interventions by healthcare providers.
Author Contributions
Conceptualization, P.-F.C., E.H.C., and E.J.U.; methodology, P.-F.C., E.H.C., E.J.U., and M.H.; software, P.-F.C.; validation, P.-F.C. and E.H.C.; formal analysis, P.-F.C. and E.H.C.; investigation, P.-F.C. and E.H.C.; resources, E.H.C.; data curation, P.-F.C.; writing—original draft preparation, P.-F.C.; writing—review and editing, P.-F.C., E.H.C., E.J.U., and M.H.; visualization, P.-F.C. and E.H.C.; supervision, E.H.C.; project administration, P.-F.C. and E.H.C.; funding acquisition, E.H.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Taipei Medical University, grant number TMU103-AE1-B25.
Acknowledgments
This article was developed from the master’s thesis of P.F.C. from Taipei Medical University. We thank Meng-Jung Wen, Jo-Hsin Chen, Chi-Lien Hsiao, You-Mei Lin, Lucy Lin, Chung-Hsuen Wu, Li-Hsuan Wang, Yu Ko, Ruby Tseng, and Hsiang-Wen Lin for providing help in the development of the ChMAR-Scale, recruitment, and providing feedback on the manuscript. We also thank the pharmacists who helped to distribute the questionnaires and the respondents who participated in the study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Centers for Disease Control and Prevention. National Center for Chronic Disease Prevention and Health Promotion (NCCDPHP). 2019. Available online: https://www.cdc.gov/chronicdisease/about/index.htm (accessed on 31 May 2020).
- Chisholm-Burns, M.A.; Spivey, C.A. The ′cost′ of medication nonadherence: Consequences we cannot afford to accept. J. Am. Pharm. Assoc. 2012, 52, 823–826. [Google Scholar] [CrossRef] [PubMed]
- Osterberg, L.; Blaschke, T. Adherence to medication. N. Engl. J. Med. 2005, 353, 487–497. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cramer, J.; Rosenheck, R.; Kirk, G.; Krol, W.; Krystal, J. Medication compliance feedback and monitoring in a clinical trial: Predictors and outcomes. Value Health 2003, 6, 566–573. [Google Scholar] [CrossRef] [PubMed]
- Yang, A.; Wang, B.; Zhu, G.; Jiao, Z.; Fang, Y.; Tang, F.; Ma, C.; Zhao, Y.; Cheng, C.; Zhong, M. Validation of Chinese version of the Morisky medication adherence scale in patients with epilepsy. Seizure 2014, 23, 295–299. [Google Scholar] [CrossRef] [Green Version]
- Wei, L.; Champman, S.; Li, X.; Li, X.; Li, S.; Chen, R.; Bo, N.; Chater, A.; Horne, R. Beliefs about medicines and non-adherence in patients with stroke, diabetes mellitus and rheumatoid arthritis: A cross-sectional study in China. BMJ Open 2017, 7, e017293. [Google Scholar] [CrossRef]
- Li, W.W.; Kuo, C.T.; Hwang, S.L.; Hsu, H.T. Factors related to medication non-adherence for patients with hypertension in Taiwan. J. Clin. Nurs. 2012, 21, 1816–1824. [Google Scholar] [CrossRef]
- Lam, P.W.; Lum, C.M.; Leung, M.F. Drug non-adherence and associated risk factors among Chinese geriatric patients in Hong Kong. Hong Kong Med. 2007, 13, 284–292. [Google Scholar]
- World Health Organization. Adherence to Long-Term Therapies: Evidence for Action; Sabaté, E., Ed.; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- Morisky, D.E.; Green, L.W.; Levine, D.M. Concurrent and predictive validity of a self-reported measure of medication adherence. Med. Care 1986, 24, 67–74. [Google Scholar] [CrossRef]
- McHorney, C.A. The Adherence Estimator: A brief, proximal screener for patient propensity to adhere to prescription medications for chronic disease. Curr. Med. Res. Opin. 2009, 25, 215–238. [Google Scholar] [CrossRef]
- Matza, L.S.; Park, J.; Coyne, K.S.; Skinner, E.P.; Malley, K.G.; Wolever, R.Q. Derivation and validation of the ASK-12 adherence barrier survey. Ann. Pharmacother. 2009, 43, 1621–1630. [Google Scholar] [CrossRef]
- Svarstad, B.L.; Chewning, B.A.; Sleath, B.L.; Claesson, C. The Brief Medication Questionnaire: A tool for screening patient adherence and barriers to adherence. Patient Educ. Couns. 1999, 37, 113–124. [Google Scholar] [CrossRef]
- Morisky, D.E.; Ang, A.; Krousel-Wood, M.; Ward, H.J. Predictive validity of a medication adherence measure in an outpatient setting. J. Clin. Hypertens. (Greenwich) 2008, 10, 348–354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hays, R.D. The Medical Outcomes Study (MOS) Measures of Patient Adherence; The RAND Corporation: Santa Monica, CA, USA, 1994. [Google Scholar]
- Vik, S.A.; Maxwell, C.J.; Hogan, D.B. Measurement, correlates, and health outcomes of medication adherence among seniors. Ann. Pharmacother. 2004, 38, 303–312. [Google Scholar] [CrossRef] [PubMed]
- Unni, E.J.; Farris, K.B. Development of a new scale to measure self-reported medication nonadherence. Res. Soc. Adm. Pharm. 2015, 11, e133–e143. [Google Scholar] [CrossRef] [PubMed]
- Unni, E.J.; Olson, J.L.; Farris, K.B. Revision and validation of Medication Adherence Reasons Scale (MAR-Scale). Curr. Med. Res. Opin. 2014, 30, 211–221. [Google Scholar] [CrossRef] [PubMed]
- Unni, E.J.; Sternbach, N.; Goren, A. Using the Medication Adherence Reasons Scale (MAR-Scale) to identify the reasons for non-adherence across multiple disease conditions. Patient Prefer. Adherence 2019, 13, 993–1004. [Google Scholar] [CrossRef] [Green Version]
- Hu, W.Y.; Tseng, C.D.; Dai, Y.T.; Chao, Y.M. An Exploration of the Drug Compliant Behaviors and Associated Factors of Hypertensive Patients. Taiwan J. Public Health (Oxf.) 1996, 15, 319–332. [Google Scholar]
- Chen, Y.J.; Chang, J.; Yang, S.Y. Psychometric Evaluation of Chinese Version of Adherence to Refills and Medications Scale (ARMS) and Blood-Pressure Control Among Elderly with Hypertension. Patient Prefer. Adherence 2020, 14, 213–220. [Google Scholar] [CrossRef]
- Yan, J.; You, L.M.; Yang, Q.; Liu, B.; Jin, S.; Zhou, J.; Lin, C.; Morisky, D.E. Translation and validation of a Chinese version of the 8-item Morisky medication adherence scale in myocardial infarction patients. J. Eval. Clin. Pract. 2014, 20, 311–317. [Google Scholar] [CrossRef]
- Wild, D.; Grove, A.; Martin, M.; Eremenco, S.; McElroy, S.; Verjee-Lorenz, A.; Erikson, P. Principles of good practice for the translation and cultural adaptation process for patient-reported outcomes (PRO) measures: Report of the ISPOR Task Force for Translation and Cultural Adaptation. Value Health 2005, 8, 94–104. [Google Scholar] [CrossRef] [Green Version]
- James, P.A.; Oparil, S.; Carter, B.L.; Cushman, W.C.; Dennison-Himmelfarb, C.; Handler, J.; Lackland, D.T.; LeFevre, M.L.; MacKenzie, T.D.; Ogedegbe, O.; et al. 2014 evidence-based guideline for the management of high blood pressure in adults: Report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA 2014, 311, 507–520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nau, D.P.; Steinke, D.T.; Williams, L.K.; Austin, R.; Lafata, J.E.; Divine, G.; Pladevall, M. Adherence analysis using visual analog scale versus claims-based estimation. Ann. Pharmacother. 2007, 41, 1792–1797. [Google Scholar] [CrossRef] [PubMed]
- Hair, J.F.; Black, W.C.; Babin, B.J.; Anderson, R.E.; Tatham, R.L. Multivariate Data Analysis; Pearson Education: Upper Saddle River, NJ, USA, 2006. [Google Scholar]
- Nunnally, J.; Bernstein, I. Psychometric Theory, 3rd ed.; MacGraw-Hill: New York, NY, USA, 1994. [Google Scholar]
- Kohen, J. A coefficient of agreement for nominal scale. Educ. Psychol. Meas. 1960, 20, 37–46. [Google Scholar] [CrossRef]
- Kawaguchi-Suzuki, M.; Law, M.G.; Prisco, J.; Head, K.; Fu, L.; Yumoto, T.; Kamei, J.; Yang, M.; Cheng, K.J.; Hogue, M.D. Cultural Sensitivity and Global Pharmacy Engagement in Asia: China, Japan, South Korea, and Taiwan. J. Am. Pharm. Edu. 2019, 83, 7214. [Google Scholar] [CrossRef]
- Stanton-Robinson, C.; Al-Jumaili, A.A.; Jackson, A.; Catney, C.; Veach, S.; Witry, M.J. Evaluation of community pharmacist-provided telephone interventions to improve adherence to hypertension and diabetes medications. J. Am. Pharm. Assoc. 2018, 58, S120–S124. [Google Scholar] [CrossRef]
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).




{kind=link}