Social Activities and Health-Related Quality of Life in Rural Older Adults in South Korea: A 4-Year Longitudinal Analysis

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Measurements
2.2.1. Sociodemographic and Health Characteristics
2.2.2. Health-Related Quality of Life
2.2.3. Social Activities
In-Person Social Activities
Social Networks
2.3. Ethical Considerations and Data Collection
2.4. Data Analysis
3. Results
3.1. Sample Characteristics
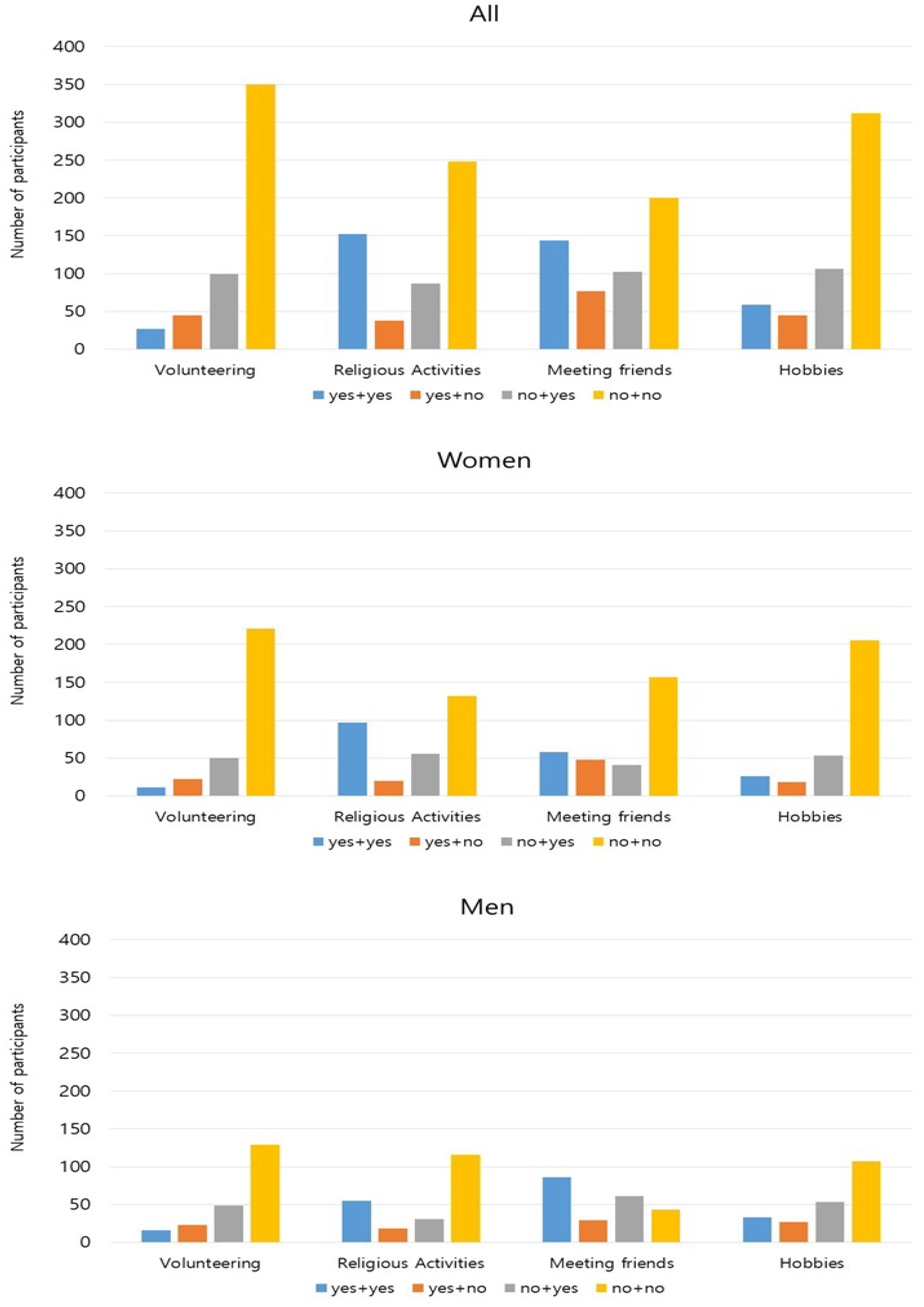
3.2. Changes in in-Person Social Activities, Social Network, and Health-Related Quality of Life over Four Years
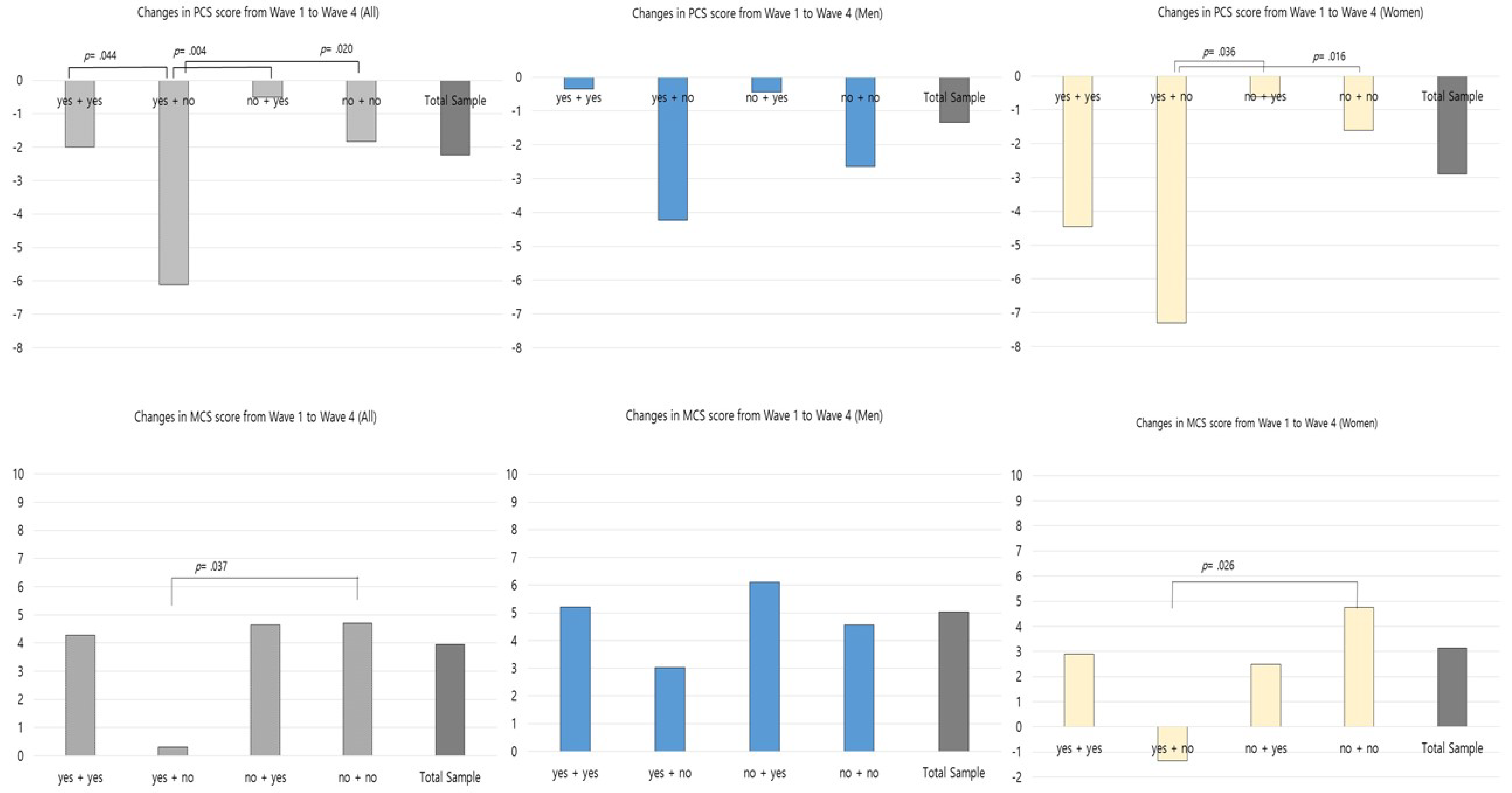
3.3. Changes in Health-Related Quality of Life According to Changes in in-Person Social Activities
4. Discussion
4.1. Longitudinal Changes in Health-Related Quality of Life
4.2. Changes in PCS and MCS Scores by Types of in-Person Social Activities
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- United Nations. World Population Ageing. 2019. Available online: https://www.un.org/en/development/desa/population/publications/pdf/ageing/WorldPopulationAgeing2019-Report.pdf (accessed on 30 June 2020).
- OECD. Elderly Population. Available online: https://doi.org/10.1787/8d805ea1-en (accessed on 21 June 2020).
- Carver, L.F.; Beamish, R.; Phillips, S.; Villeneuve, M. A scoping review: Social participation as a cornerstone of successful aging in place among rural older adults. Geriatrics 2018, 3, 75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- He, Q.; Cui, Y.; Liang, L.; Zhong, Q.; Li, J.; Li, Y.; Lv, X.; Huang, F. Social participation, willingness and quality of life: A population-based study among older adults in rural areas of China. Geriatr. Gerontol. Int. 2017, 17, 1593–1602. [Google Scholar] [CrossRef] [PubMed]
- Park, J.; Kim, K. The residential location choice of the elderly in Korea: A multilevel logit model. J. Rural Stud. 2016, 44, 261–271. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Ageing and Life-Course. Available online: https://www.who.int/ageing/healthy-ageing/en/ (accessed on 4 June 2020).
- Rutherford, B.R.; Taylor, W.D.; Brown, P.J.; Sneed, J.R.; Roose, S.P. Biological aging and the future of geriatric psychiatry. J. Gerontol. A Biol. Sci. Med. Sci. 2017, 72, 343–352. [Google Scholar] [CrossRef]
- Otero-Rodríguez, A.; León-Muñoz, L.M.; Balboa-Castillo, T.; Banegas, J.R.; Rodríguez-Artalejo, F.; Guallar-Castillón, P. Change in health-related quality of life as a predictor of mortality in the older adults. Qual. Life Res. 2010, 19, 15–23. [Google Scholar] [CrossRef]
- Cavrini, G.; Broccoli, S.; Puccini, A.; Zoli, M. EQ-5D as a predictor of mortality and hospitalization in elderly people. Qual. Life Res. 2012, 21, 269–280. [Google Scholar] [CrossRef]
- Haraldstad, K.; Wahl, A.; Andenaes, R.; Andersen, J.R.; Andersen, M.H.; Beisland, E.; Borge, C.R.; Engebretsen, E.; Eisemann, M.; Halvorsrud, L.; et al. A systematic review of quality of life research in medicine and health sciences. Qual. Life Res. 2019, 28, 2641–2650. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.H.; Park, E.C. Impact of socioeconomic status and subjective social class on overall and health-related quality of life. BMC Public Health 2015, 15, 783. [Google Scholar] [CrossRef] [Green Version]
- Ma, X.; McGhee, S.M. A cross-sectional study on socioeconomic status and health-related quality of life among elderly Chinese. BMJ Open 2013, 3, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Bayan-Bravo, A.; Perez-Tasigchana, R.F.; Sayon-Orea, C.; Martinez-Gomez, D.; Lopez-Garcia, E.; Rodriguez-Artalejo, F.; Guallar-Castillon, P. Combined Impact of Traditional and Non-Traditional Healthy Behaviors on Health-Related Quality of Life: A Prospective Study in Older Adults. PLoS ONE 2017, 12, e0170513. [Google Scholar]
- Kim, J.; Choi, Y.; Park, S.; Cho, K.H.; Ju, Y.J.; Park, E.C. The impact of living arrangements on quality of life among Korean elderly: Findings from the Korean longitudinal study of aging (2006–2012). Qual. Life Res. 2017, 26, 1303–1314. [Google Scholar] [CrossRef] [PubMed]
- Douglas, H.; Georgiou, A.; Westbrook, J. Social participation as an indicator of successful aging: An overview of concepts and their associations with health. Aust. Health Rev. 2017, 41, 455–462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Charles, S.T.; Carstensen, L.L. Social and Emotional Aging. Annu. Rev. Psychol. 2010, 61, 383–409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leigh-Hunt, N.; Bagguley, D.; Bash, K.; Turner, V.; Turnbull, S.; Valtorta, N.; Cann, W. An overview of systematic reviews on the public health consequences of social isolation and loneliness. Public Health 2017, 152, 157–171. [Google Scholar] [CrossRef] [Green Version]
- AARP Foundation. A National Survey of Adults 45 and Older: Loneliness and Social Connections. Available online: https://www.aarp.org/content/dam/aarp/research/surveys_statistics/life-leisure/2018/loneliness-social-connections-2018.doi.10.26419-2Fres.00246.001.pdf (accessed on 5 June 2020).
- DiGessa, G.; Grundy, E. The relationship between active ageing and health using longitudinal data from Denmark, France, Italy and England. J. Epidemiol. Community Health 2014, 68, 261–267. [Google Scholar] [CrossRef] [Green Version]
- Gardiner, C.; Geldenhuys, G.; Gott, M. Interventions to reduce social isolation and loneliness among older people: An integrative review. Health Soc. Care Community 2018, 26, 147–157. [Google Scholar] [CrossRef]
- Saias, T.; Beck, F.; Bodard, J.; Guignard, R.; du Roscoat, E. Social participation, social environment and death ideations in later life. PLoS ONE 2012, 7, e46723. [Google Scholar] [CrossRef] [Green Version]
- Annear, M.; Keeling, S.; Wilkinson, T.; Cushman, G.; Gidlow, B.; Hopkins, H. Environmental influences on healthy and active ageing: A systematic review. Ageing Soc. 2014, 34, 590–622. [Google Scholar] [CrossRef]
- Rechel, B.; Džakula, A.; Duran, A.; Fattore, G.; Edwards, N.; Grignon, M.; Haas, M.; Habicht, T.; Marchildon, G.P.; Moreno, A. Hospitals in rural or remote areas: An exploratory review of policies in 8 high-income countries. Health Policy 2016, 120, 758–769. [Google Scholar] [CrossRef]
- Dahlberg, L.; McKee, K. Social exclusion and well-being among older adults in rural and urban areas. Arch. Gerontol. Geriatr. 2018, 79, 176–184. [Google Scholar] [CrossRef]
- Hong, N.; Kim, K.; Lee, S.J.; Kim, C.O.; Kim, H.C.; Rhee, Y.; Youm, Y.; Choi, J.Y.; Park, H.Y. Cohort profile: Korean Urban Rural Elderly (KURE) study, a prospective cohort on ageing and health in Korea. BMJ Open 2019, 9, e031018. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Henning-Smith, C.; Echlund, A.; Kozhimannil, K. Rural-urban differences in social isolation and its relationship to health. Innov. Aging 2018, 2, 770. [Google Scholar] [CrossRef] [Green Version]
- Ide, K.; Tsuji, T.; Kanamori, S.; Jeong, S.; Nagamine, Y.; Kondo, K. Social Participation and Functional Decline: A Comparative Study of Rural and Urban Older People, Using Japan Gerontological Evaluation Study Longitudinal Data. Int. J. Environ. Res. Public Health 2020, 17, 617. [Google Scholar] [CrossRef] [Green Version]
- Levasseur, M.; Cohen, A.; Dubois, M.; Genereux, M.; Richard, L.; Therrien, F.; Payette, H. Environmental Factors Associated With Social Participation of Older Adults Living in Metropolitan, Urban, and Rural Areas: The NuAge Study. Am. J. Public Health 2015, 105, 1718–1725. [Google Scholar] [CrossRef] [PubMed]
- Vogelsang, E.M. Older adult social participation and its relationship with health: Rural-urban differences. Health Place 2016, 42, 111–119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Henchoz, Y.; Abolhassani, N.; Bula, C.; Guessous, I.; Goy, R.; Santos-Eggimann, B. Change in quality of life among community-dwelling older adults: Population-based longitudinal study. Qual. Life Res. 2019, 28, 1305–1314. [Google Scholar] [CrossRef] [PubMed]
- Ward, M.; McGarrigle, C.A.; Kenny, R.A. More than health: Quality of life trajectories among older adults-findings from The Irish Longitudinal Study of Ageing (TILDA). Qual. Life Res. 2019, 28, 429–439. [Google Scholar] [CrossRef]
- Chung, S.S.; Joung, K.H. Factors related to quality of life among middle-aged and older korean adults in 2006 and 2014: A nationally representative study. Arch. Psychiatr. Nurs. 2018, 32, 861–867. [Google Scholar] [CrossRef]
- Lim, H.J.; Min, D.K.; Thorpe, L.; Lee, C.H. Multidimensional construct of life satisfaction in older adults in Korea: A six-year follow-up study. BMC Geriatr. 2016, 16, 197. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.M.; Lee, W.J.; Kim, H.C.; Choi, W.; Lee, J.; Sung, K.; Chu, S.H.; Park, Y.R.; Youm, Y. The Korean social life, health, health and aging project-health examination cohort. Epidemiol. Health 2014, 36, e2014003. [Google Scholar] [CrossRef] [Green Version]
- Youm, Y.; Laumann, E.O.; Ferraro, K.F.; Waite, L.J.; Kim, H.C.; Park, Y.R.; Chu, S.H.; Joo, W.T.; Lee, J.A. Social network properties and self-rated health in later life: Comparisons from the Korean social life, health, and aging project and the national social life, health and aging project. BMC Geriatr. 2014, 14, 102. [Google Scholar] [CrossRef] [Green Version]
- Winter, J.E.; MacInnis, R.J.; Wattanapenpaiboon, N.; Nowson, C.A. BMI and all-cause mortality in older adults: A meta-analysis. Am. J. Clin. Nutr. 2004, 99, 875–890. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, T.H.; Jhoo, J.H.; Park, J.H.; Kim, J.L.; Ryu, S.H.; Moon, S.W.; Choo, I.H.; Lee, D.W.; Yoon, J.C.; Do, Y.J.; et al. Korean Version of Mini Mental Status Examination for Dementia Screening and Its’ Short Form. Psychiatry Investig. 2010, 7, 102–108. [Google Scholar] [CrossRef]
- Podsiadlo, D.; Richardson, S. The timed Up and Go: A test of basic functional mobility for frail elderly persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Ware, J.E.; Kosinski, M.; Keller, S.D. How to Score the SF-12 Physical and Mental Health Summary Scales, 3rd ed.; Quality Metric Incorporated: Lincoln, RI, USA, 1998. [Google Scholar]
- Baek, J.; Hur, N.W.; Kim, H.C.; Youm, Y. Sex-specific effects of social networks on the prevalence, awareness, and control of hypertension among older Korean adults. J. Geriatr. Cardiol. 2016, 13, 580. [Google Scholar] [PubMed]
- Vanleerberghe, P.; De Witte, N.; Claes, C.; Schalock, R.L.; Verté, D. The quality of life of older people aging in place: A literature review. Qual. Life Res. 2017, 26, 2899–2907. [Google Scholar] [CrossRef] [PubMed]
- Feng, D.; Ji, L.; Xu, L. Effect of subjective economic status on psychological distress among farmers and non-farmers of rural China. Aust. J. Rural Health 2015, 23, 215–220. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Lee, H.; Cho, E.; Lee, K.H.; Park, C.G.; Cho, B.H. Multilevel Effects of Community Capacity on Active Aging in Community-Dwelling Older Adults in South Korea. Asian Nurs. Res. 2020, 14, 36–43. [Google Scholar] [CrossRef]
- Baernholdt, M.; Yan, G.; Hinton, I.; Rose, K.; Mattos, M. Quality of life in rural and urban adults 65 years and older: Findings from the National Health and Nutrition Examination survey. J. Rural Health 2012, 28, 339–347. [Google Scholar] [CrossRef] [Green Version]
- Naveiro-Rilo, J.; Diez-Juarez, D.; Flores-Zurutuza, M.; Pérez, A. Quality of life in the elderly on polymedication and with multiple morbidities. Rev. Esp. Geriatr. Gerontol. 2014, 49, 158–164. [Google Scholar] [CrossRef]
- König, H.H.; Heider, D.; Lehnert, T.; Riedel-Heller, S.G.; Angermeyer, M.C.; Matschinger, H.; Vilagut, G.; Bruffaerts, R.; Haro, J.M.; de Girolamo, G. Health status of the advanced elderly in six European countries: Results from a representative survey using EQ-5D and SF-12. Health Qual. Life Outcomes 2010, 8, 143. [Google Scholar] [CrossRef] [PubMed]
- Lee, G.; Park, J.; Oh, S.W.; Joh, H.K.; Hwang, S.S.; Kim, J.; Park, D. Association between body mass index and quality of life in elderly people over 60 years of age. Korean J. Fam. Med. 2017, 38, 181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blanco-Reina, E.; Valdellós, J.; Ocaña-Riola, R.; García-Merino, M.R.; Aguilar-Cano, L.; Ariza-Zafra, G.; Bellido-Estévez, I. Factors Associated with Health-Related Quality of Life in Community-Dwelling Older Adults: A Multinomial Logistic Analysis. J. Clin. Med. 2019, 8, 1810. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baladón, L.; Rubio-Valera, M.; Serrano-Blanco, A.; Palao, D.J.; Fernández, A. Gender differences in the impact of mental disorders and chronic physical conditions on health-related quality of life among non-demented primary care elderly patients. Qual. Life Res. 2016, 25, 1461–1474. [Google Scholar] [CrossRef] [PubMed]
- Padua, L.; Pasqualetti, P.; Coraci, D.; Imbimbo, I.; Giordani, A.; Loreti, C.; Marra, C.; Molino-Lova, R.; Pasquini, G.; Simonelli, I. Gender effect on well-being of the oldest old: A survey of nonagenarians living in Tuscany: The Mugello study. Neurol. Sci. 2018, 39, 509–517. [Google Scholar] [CrossRef]
- McPhee, J.S.; French, D.P.; Jackson, D.; Nazroo, J.; Pendleton, N.; Degens, H. Physical activity in older age: Perspectives for healthy ageing and frailty. Biogerontology 2016, 17, 567–580. [Google Scholar] [CrossRef]
- Huxhold, O.; Miche, M.; Schüz, B. Benefits of having friends in older ages: Differential effects of informal social activities on well-being in middle-aged and older adults. J. Gerontol. B Psychol. Sci. Soc. Sci. 2014, 69, 366–375. [Google Scholar] [CrossRef]
- George, L.K. Eighteen—Perceived Quality of Life. In Handbook of Aging and the Social Sciences, 6th ed.; Binstock, R.H., George, L.K., Cutler, S.J., Hendricks, J., Schulz, J.H., Eds.; Academic Press: Burlington, NJ, USA, 2006; pp. 320–336. ISBN 978-0-12-088388-2. [Google Scholar]
- Ejiri, M.; Kawai, H.; Fujiwara, Y.; Ihara, K.; Watanabe, Y.; Hirano, H.; Kim, H.K.; Ishii, K.; Oka, K.; Obuchi, S. Social participation reduces isolation among Japanese older people in urban area: A 3-year longitudinal study. PLoS ONE 2019, 14, e0222887. [Google Scholar] [CrossRef]
- Cruwys, T.; Dingle, G.A.; Haslam, C.; Haslam, S.A.; Jetten, J.; Morton, T.A. Social group memberships protect against future depression, alleviate depression symptoms and prevent depression relapse. Soc. Sci. Med. 2013, 98, 179–186. [Google Scholar] [CrossRef]
- Kanamori, S.; Kai, Y.; Aida, J.; Kondo, K.; Kawachi, I.; Hirai, H.; Shirai, K.; Ishikawa, Y.; Suzuki, K. Social participation and the prevention of functional disability in older Japanese: The JAGES cohort study. PLoS ONE 2014, 9, e99638. [Google Scholar] [CrossRef]
- Lam, B.C.; Haslam, C.; Haslam, S.A.; Steffens, N.K.; Cruwys, T.; Jetten, J.; Yang, J. Multiple social groups support adjustment to retirement across cultures. Soc. Sci. Med. 2018, 208, 200–208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, J.; Rozelle, S.; Xu, Q.; Yu, N.; Zhou, T. Social Engagement and Elderly Health in China: Evidence from the China Health and Retirement Longitudinal Survey (CHARLS). Int. J. Environ. Res. Public Health 2019, 16, 278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hess, T.M.; Ennis, G.E. Age differences in the effort and costs associated with cognitive activity. J. Gerontol. B Psychol. Sci. Soc. Sci. 2012, 67, 447–455. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mair, C.A.; Thivierge-Rikard, R. The strength of strong ties for older rural adults: Regional distinctions in the relationship between social interaction and subjective well-being. Int. J. Aging Hum. Dev. 2010, 70, 119–143. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics Categories | Wave 1 | Wave 4 | p-Value | |||||
|---|---|---|---|---|---|---|---|---|
| Total (N = 525) n (%) | Men (n = 220) n (%) | Women (n = 305) n (%) | Total (N = 525) n (%) | Men (n = 220) n (%) | Women (n = 305) n (%) | |||
| Age (in years): Mean (SD) | 71.17 (6.20) | 70.90 (5.99) | 71.36 (6.34) | 75.1 (6.3) | 74.75 (5.98) | 75.30 (6.45) | N/A | |
| BMI (kg/m2): Mean (SD) | 24.18 (3.25) | 23.97 (3.12) | 24.32 (3.33) | - | N/A | |||
| BMI | Underweight (<18.5 kg/m2) | 17 (3.6) | 5 (2.6) | 12 (4.3) | - | N/A | ||
| Normal (18.5–22.9 kg/m2) | 152 (32.2) | 68 (35.6) | 84 (29.9) | - | ||||
| Overweight (23–24.9 kg/m2) | 122 (25.8) | 52 (27.2) | 70 (24.9) | - | ||||
| Obesity (>25 kg/m2) | 181 (38.3) | 66 (34.6) | 115 (40.9) | - | ||||
| Education | No education | 157 (29.9) | 24 (11.0) | 133 (44.0) | - | N/A | ||
| Elementary school | 225 (42.9) | 92 (42.0) | 133 (44.0) | - | ||||
| Middle school | 74 (14.1) | 53 (24.2) | 21 (7.0) | - | ||||
| High school | 49 (9.3) | 39 (17.8) | 10 (3.3) | - | ||||
| College or higher | 16 (3.0) | 11 (5.0) | 5 (1.7) | - | ||||
| Work Status | Yes | 385 (73.3) | 185 (84.1) | 200 (65.6) | 398 (75.8) | 185 (84.1) | 213 (69.8) | a < 0.001 b < 0.001 c < 0.001 |
| No | 140 (26.7) | 35 (15.9) | 105 (34.4) | 127 (24.2) | 35 (15.9) | 92 (30.2) | ||
| Marital Status | Living with spouse | 399 (76.0) | 203 (92.3) | 196 (64.3) | 369 (70.3) | 201 (91.4) | 168 (55.1) | a < 0.001 b < 0.001 c < 0.001 |
| Separated | 2 (0.4) | 1 (0.5) | 1 (0.3) | 3 (0.6) | 3 (1.4) | 0 (0) | ||
| Widowed | 121 (23.0) | 13 (5.9) | 108 (35.6) | 147 (28.0) | 15 (6.8) | 132 (43.3) | ||
| Divorced | 0 (0) | 0 (0) | 0 (0) | 4 (0.8) | 0 (0) | 4 (1.3) | ||
| Never married | 3 (0.6) | 3 (1.4) | 0 (0) | 2 (0.3) | 1 (0.5) | 1 (0.3) | ||
| Religion | No religion | 295 (56.2) | 135 (61.4) | 160 (52.5) | 244 (46.5) | 120 (54.5) | 124 (40.7) | a < 0.001 b < 0.001 c < 0.001 |
| Protestant | 140 (26.7) | 51 (23.2) | 89 (29.2) | 169 (32.2) | 64 (29.1) | 105 (34.4) | ||
| Catholic | 28 (5.3) | 11 (5.0) | 17 (5.6) | 24 (4.6) | 9 (4.1) | 15 (4.9) | ||
| Buddhism | 55 (10.5) | 19 (8.6) | 36 (11.8) | 65 (12.4) | 19 (8.6) | 46 (15.1) | ||
| Other | 7 (1.3) | 4 (1.8) | 3 (1.0) | 23 (4.3) | 8 (3.6) | 15 (4.9) | ||
| Smoking Status | Past and current smoker | 56 (10.7) | 49 (22.3) | 7 (2.3) | 35 (6.7) | 35 (15.9) | 0 (0) | a < 0.001 b < 0.001 c = 0.947 |
| Past smoker but not now | 91 (17.3) | 91 (41.4) | 0 (0) | 124 (23.6) | 120 (54.5) | 4 (1.3) | ||
| Have never smoked | 372 (70.9) | 75 (34.1) | 297 (97.4) | 366 (69.7) | 65 (29.5) | 301 (98.7) | ||
| Recently started smoking | 6 (1.1) | 5 (2.3) | 1 (0.3) | 0 (0) | 0 (0) | 0 (0) | ||
| Drinking Habit | Never | 334 (63.6) | 82 (37.2) | 252 (82.6) | 362 (69.0) | 100 (45.5) | 262 (85.9) | a < 0.001 b < 0.001 c < 0.001 |
| Rarely | 68 (13.0) | 36 (16.4) | 32 (10.5) | 66 (12.6) | 29 (13.2) | 37 (12.1) | ||
| Once a week or more | 123 (23.4) | 102(46.4) | 21 (6.9) | 97 (18.4) | 91 (41.4) | 6 (2.0) | ||
| Hypertension | Yes | 277 (52.8) | 98 (44.5) | 179 (58.7) | 307 (58.5) | 108 (49.1) | 199 (65.2) | a < 0.001 b < 0.001 c < 0.001 |
| No | 248 (47.2) | 122 (55.5) | 126 (41.3) | 218 (41.5) | 112 (50.9) | 106 (34.8) | ||
| Hyperlipidemia | Yes | 57 (10.9) | 23 (10.5) | 34 (11.2) | 111 (21.1) | 36 (16.4) | 75 (24.6) | a < 0.001 b < 0.001 c < 0.001 |
| No | 467 (89.1) | 197 (89.5) | 270 (88.8) | 414 (78.9) | 184 (83.6) | 230 (75.4) | ||
| Arthritis | Yes | 219 (41.9) | 50 (22.8) | 169 (55.6) | - | - | - | N/A |
| No | 304 (58.1) | 169 (77.2) | 135 (44.4) | - | - | - | ||
| Osteoporosis | Yes | 133 (25.3) | 14 (6.4) | 119 (39.0) | 105 (20.0) | 4 (1.8) | 101 (33.1) | a < 0.001 b < 0.001 c < 0.001 |
| No | 392 (74.7) | 206 (93.6) | 186 (61.0) | 420 (80.0) | 216 (98.2) | 204 (66.9) | ||
| MMSE-DS: Mean (SD) | 24.25 (4.09) | 25.39 (3.59) | 23.43 (4.24) | 24.38 (4.18) | 25.40 (3.44) | 23.64 (4.51) | a = 0.518 b = 0.963 c = 0.428 | |
| Timed Up and Go Test (in sec): Mean (SD) | 12.56 (2.94) | 12.04 (3.01) | 12.94 (2.84) | 13.34 (3.98) | 12.70 (4.71) | 13.80 (3.31) | a < 0.001 b < 0.001 c < 0.001 | |
| Variables | Categories | Wave 1 | Wave 4 | p-Value | ||||
|---|---|---|---|---|---|---|---|---|
| Total (N = 525) n (%) | Men (n = 220) n (%) | Women (n = 305) n (%) | Total (N = 525) n (%) | Men (n = 220) n (%) | Women (n = 305) n (%) | |||
| In-Person Social Activities | ||||||||
| Volunteering | Yes | 72 (13.8) | 39 (18.0) | 33 (10.9) | 126 (24.0) | 65 (29.5) | 61 (20.0) | a = 0.004 b = 0.096 c = 0.044 |
| No | 449 (86.2) | 178 (82.0) | 271 (89.1) | 399 (76.0) | 155 (70.5) | 244 (80.0) | ||
| Religious Activities | Yes | 190 (36.2) | 73 (33.2) | 117 (38.4) | 239 (45.5) | 86 (39.1) | 153 (50.2) | a < 0.001 b < 0.001 c < 0.001 |
| No | 335 (63.8) | 147 (66.8) | 188 (61.6) | 286 (54.5) | 134 (60.9) | 152 (49.8) | ||
| Meeting friends | Yes | 221 (42.3) | 73 (33.2) | 106 (34.9) | 247 (47.0) | 147 (66.8) | 100 (32.8) | a < 0.001 b = 0.011 c < 0.001 |
| No | 302 (57.7) | 147 (66.8) | 198 (65.1) | 278 (53.0) | 73 (33.2) | 205 (67.2) | ||
| Hobbies | Yes | 104 (19.9) | 115 (52.5) | 44 (14.6) | 166 (31.6) | 86 (39.1) | 80 (26.2) | a < 0.001 b = 0.003 c < 0.001 |
| No | 418 (80.1) | 104 (47.5) | 258 (85.4) | 359 (68.4) | 134 (60.9) | 225 (73.8) | ||
| Social Network | ||||||||
| Network size (discussion network members); Mean (SD) | 2.41 (1.17) | 2.51 (1.18) | 2.33 (1.15) | 2.78 (1.38) | 2.85 (1.47) | 2.72 (1.32) | a < 0.001 b = 0.005 c < 0.001 | |
| Network density; Mean (SD) | 0.98 (0.12) | 0.99 (0.07) | 0.97 (0.15) | 0.96 (0.12) | 0.96 (0.13) | 0.97 (0.12) | a = 0.178 b = 0.006 c = 0.737 | |
| Health-related Quality of Life | ||||||||
| SF-12 Physical Component Summary: Mean (SD) | 46.26 (8.74) | 49.11 (7.92) | 44.20 (8.75) | 43.96 (10.90) | 47.71 (9.43) | 41.25 (11.10) | a < 0.001 b < 0.041 c < 0.001 | |
| SF-12 Mental Component Summary: Mean (SD) | 49.09 (8.08) | 49.99 (7.89) | 48.44 (8.16) | 52.99 (10.19) | 55.01 (9.03) | 51.55 (10.74) | a < 0.001 b < 0.001 c < 0.001 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, J.; Yang, K.; Chu, S.H.; Youm, Y.; Kim, H.C.; Park, Y.-R.; Son, Y.-J. Social Activities and Health-Related Quality of Life in Rural Older Adults in South Korea: A 4-Year Longitudinal Analysis. Int. J. Environ. Res. Public Health 2020, 17, 5553. https://doi.org/10.3390/ijerph17155553
Choi J, Yang K, Chu SH, Youm Y, Kim HC, Park Y-R, Son Y-J. Social Activities and Health-Related Quality of Life in Rural Older Adults in South Korea: A 4-Year Longitudinal Analysis. International Journal of Environmental Research and Public Health. 2020; 17(15):5553. https://doi.org/10.3390/ijerph17155553
Chicago/Turabian StyleChoi, JiYeon, Kyeongra Yang, Sang Hui Chu, Yoosik Youm, Hyeon Chang Kim, Yeong-Ran Park, and Youn-Jung Son. 2020. "Social Activities and Health-Related Quality of Life in Rural Older Adults in South Korea: A 4-Year Longitudinal Analysis" International Journal of Environmental Research and Public Health 17, no. 15: 5553. https://doi.org/10.3390/ijerph17155553