Effects of Depressive Symptoms, Feelings, and Interoception on Reward-Based Decision-Making: Investigation Using Reinforcement Learning Model


Abstract
:1. Introduction
2. Materials and Methods
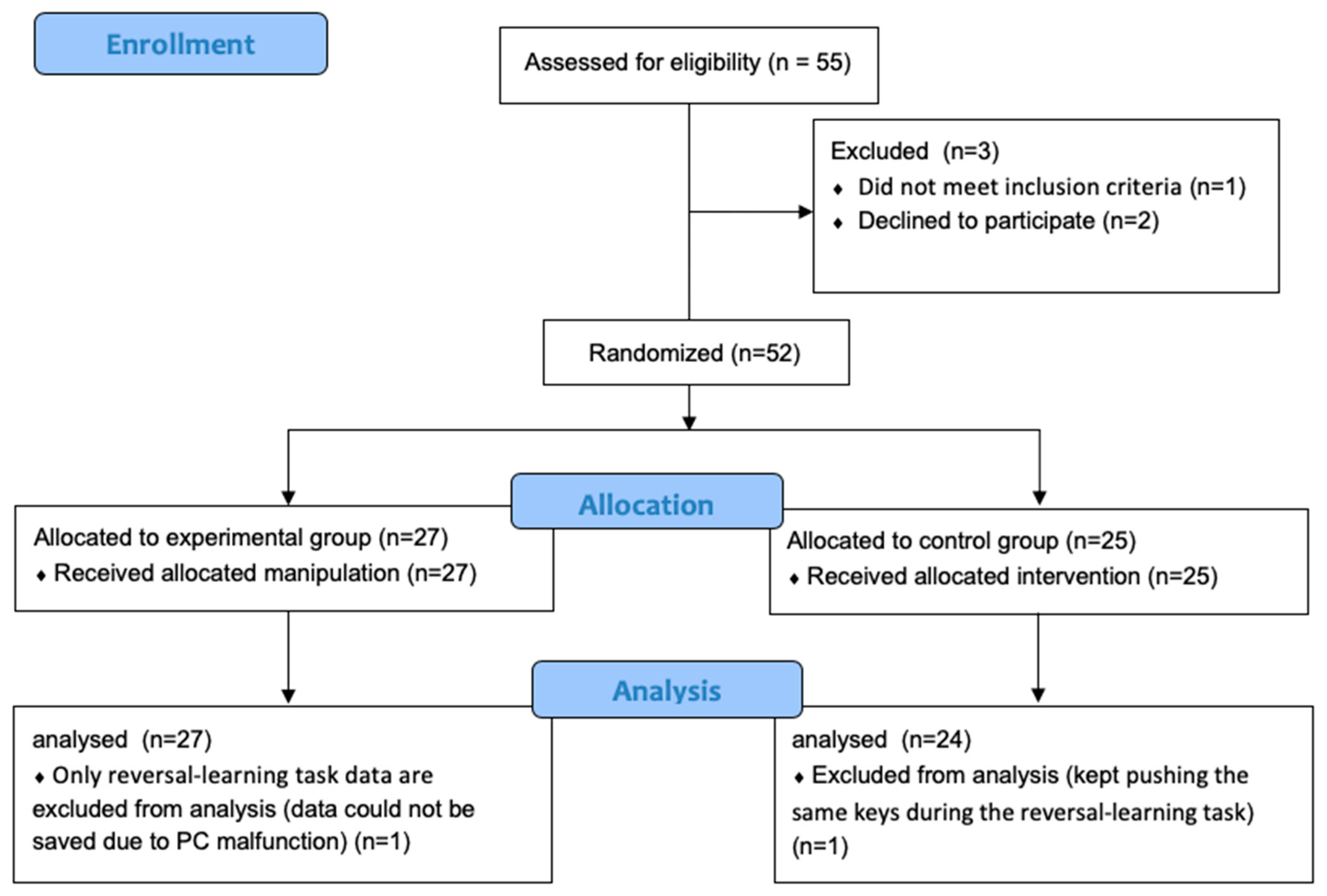
2.1. Participants and Design
2.2. Experimental Procedure
2.3. Experimental Tasks
2.3.1. Reversal-Learning Task
2.3.2. Probe-Detection Task
2.3.3. Heartbeat-Counting Task
2.4. Intervention Procedure
2.4.1. Experimental Group
2.4.2. Control Group
2.5. Electrophysiological Recording
2.5.1. Skin Conductance Response
2.5.2. Heart Rate
2.6. Reinforcement Learning Parameter
2.6.1. Experience-Weighted Attraction Model
2.6.2. Choice Probabilities
2.6.3. Parameter Estimation
2.6.4. Fitness of Data
2.6.5. Data Modeling
2.7. Data Analysis
3. Results
3.1. Preliminary Analysis
3.2. Correlations between Depressive Symptoms and Reinforcement Learning Parameters in the Pre-Test Results
3.3. Correlations between Interoception/Feelings and Reinforcement Learning Parameters in the Pre-Test Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Alloy, L.B.; Olino, T.; Freed, R.D.; Nusslock, R. Role of reward sensitivity and processing in major depressive and bipolar spectrum disorders. Behav. Ther. 2016, 47, 600–621. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Treadway, M.T.; Bossaller, N.A.; Shelton, R.C.; Zald, D.H. Effort-based decision-making in major depressive disorder: A translational model of motivational anhedonia. J. Abnorm. Psychol. 2012, 121, 553–558. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rupprechter, S.; Stankevicius, A.; Huys, Q.J.M.; Steele, J.D.; Seriès, P. Major depression impairs the use of reward values for decision-making. Sci. Rep. 2018, 8, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Admon, R.; Pizzagalli, D.A. Dysfunctional reward processing in depression. Curr. Opin. Psychol. 2015, 4, 114–118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, C.; Takahashi, T.; Nakagawa, S.; Inoue, T.; Kusumi, I. Reinforcement learning in depression: A review of computational research. Neurosci. Biobehav. Rev. 2015, 55, 247–267. [Google Scholar] [CrossRef]
- Rescorla, R.A.; Wagner, A.R. A theory of Pavlovian conditioning: Variations in the effectiveness of reinforcement and nonreinforcement. Curr. Res. Theory 1972, 64–99. [Google Scholar]
- Ahn, W.-Y.; Haines, N.; Zhang, L. Revealing neurocomputational mechanisms of reinforcement learning and decision-making with the hBayesDM package. Comput. Psychiatry 2017, 1, 24–57. [Google Scholar] [CrossRef]
- Robinson, O.J.; Chase, H.W. Learning and choice in mood disorders: Searching for the computational parameters of anhedonia. Comput. Psychiatry 2017, 1, 208–233. [Google Scholar] [CrossRef]
- Kunisato, Y.; Okamoto, Y.; Ueda, K.; Onoda, K.; Okada, G.; Yoshimura, S.; Suzuki, S.I.; Samejima, K.; Yamawaki, S. Effects of depression on reward-based decision making and variability of action in probabilistic learning. J. Behav. Ther. Exp. Psychiatry 2012, 43, 1088–1094. [Google Scholar] [CrossRef]
- Huys, Q.J.; Pizzagalli, D.A.; Bogdan, R.; Dayan, P. Mapping anhedonia onto reinforcement learning: A behavioural meta-analysis. Biol. Mood Anxiety Disord. 2013, 3, 1–16. [Google Scholar] [CrossRef] [Green Version]
- Dombrovski, A.; Clark, L.; Siegle, G.J.; Butters, M.A.; Sahakian, B.J.; Szanto, K. Reward/punishment reversal learning in older suicide attempters. Am. J. Psychiatry 2010, 167, 699–707. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chase, H.W.; Frank, M.J.; Michael, A.; Bullmore, E.T.; Sahakian, B.J.; Robbins, T.W. Approach and avoidance learning in patients with major depression and healthy controls: Relation to anhedonia. Psychol. Med. 2010, 40, 433–440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khalsa, S.S.; Adolphs, R.; Cameron, O.G.; Critchley, H.D.; Davenport, P.W.; Feinstein, J.S.; Feusner, J.D.; Garfinkel, S.N.; Lane, R.D.; Mehling, W.E.; et al. Interoception and mental health: A roadmap. Biol. Psychiatry Cogn. Neurosci. Neuroimaging 2018, 3, 501–513. [Google Scholar] [CrossRef] [PubMed]
- Furman, D.J.; Waugh, C.E.; Bhattacharjee, K.; Thompson, R.J.; Gotlib, I.H. Interoceptive awareness, positive affect, and decision making in major depressive disorder. J. Affect. Disord. 2013, 151, 780–785. [Google Scholar] [CrossRef] [Green Version]
- Herbert, B.M.; Herbert, C.; Pollatos, O. On the relationship between interoceptive awareness and alexithymia: Is interoceptive awareness related to emotional awareness? J. Pers. 2011, 79, 1149–1175. [Google Scholar] [CrossRef]
- Eggart, M.; Lange, A.; Binser, M.J.; Queri, S.; Müller-Oerlinghausen, B. Major depressive disorder is associated with impaired interoceptive accuracy: A systematic review. Brain Sci. 2019, 9, 131. [Google Scholar] [CrossRef] [Green Version]
- Craig, A.D. How do you feel? Interoception: The sense of the physiological condition of the body. Nat. Rev. Neurosci. 2002, 3, 655–666. [Google Scholar] [CrossRef]
- Craig, A.D. How do you feel—Now? The anterior insula and human awareness. Nat. Rev. Neurosci. 2009, 10, 59–70. [Google Scholar] [CrossRef]
- Sliz, D.; Hayley, S. Major depressive disorder and alterations in insular cortical activity: A review of current functional magnetic imaging research. Front. Hum. Neurosci. 2012, 6, 323. [Google Scholar] [CrossRef] [Green Version]
- Stephan, K.E.; Manjaly, Z.M.; Mathys, C.D.; Weber, L.A.E.; Paliwal, S.; Gard, T.; Tittgemeyer, M.; Fleming, S.M.; Haker, H.; Seth, A.K.; et al. Allostatic self-efficacy: A metacognitive theory of dyshomeostasis-induced fatigue and depression. Front. Hum. Neurosci. 2016, 10. [Google Scholar] [CrossRef] [Green Version]
- Barrett, L.F.; Quigley, K.S.; Hamilton, P. An active inference theory of allostasis and interoception in depression. Philos. Trans. R. Soc. B Biol. Sci. 2016, 371, 20160011. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sterling, P. Allostasis: A model of predictive regulation. Physiol. Behav. 2012, 106, 5–15. [Google Scholar] [CrossRef] [PubMed]
- Seth, A.K.; Friston, K.J. Active interoceptive inference and the emotional brain. Philos. Trans. R. Soc. Lond. B Biol. Sci. 2016, 371, 20160007. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barrett, L.F.; Russell, J.A. The structure of current affect: Controversies and emerging consensus. Curr. Dir. Psychol. Sci. 1999, 8, 10–14. [Google Scholar] [CrossRef]
- Kuppens, P.; Tuerlinckx, F.; Russell, J.A.; Barrett, L.F. The relation between valence and arousal in subjective experience. Psychol. Bull. 2013, 139, 917–940. [Google Scholar] [CrossRef] [PubMed]
- Shima, S.; Shikano, T.; Kitamura, T. A new self-report depression scale. Clin. Psychiatry 1985, 27, 717–723. (In Japanese) [Google Scholar]
- Sato, A.; Yasuda, A. Development of the Japanese version of Positive and Negative Affect Schedule (PANAS) scales. Jpn. J. Personal. 2001, 9, 138–139. (In Japanese) [Google Scholar] [CrossRef] [Green Version]
- Fukui, I. The Depression and Anxiety Mood Scale (DAMS): Scale development and validation. Jpn. J. Behav. Ther. 1997, 23, 83–93. (In Japanese) [Google Scholar]
- Whitmer, A.J.; Banich, M.T. Repetitive thought and reversal learning deficits. Cognit. Ther. Res. 2012, 36, 714–721. [Google Scholar] [CrossRef]
- Mansell, W.; Clark, D.M.; Ehlers, A. Internal versus external attention in social anxiety: An investigation using a novel paradigm. Behav. Res. Ther. 2003, 41, 555–572. [Google Scholar] [CrossRef]
- Zhou, Z.W.; Lan, X.Q.; Fang, Y.T.; Gong, Y.; Zang, Y.F.; Luo, H.; Zhang, H. The inter-regional connectivity within the default mode network during the attentional processes of internal focus and external focus: An fmri study of continuous finger force feedback. Front. Psychol. 2019, 10, 2198. [Google Scholar] [CrossRef]
- Pineles, S.L.; Mineka, S. Attentional biases to internal and external sources of potential threat in social anxiety. J. Abnorm. Psychol. 2005, 114, 314–318. [Google Scholar] [CrossRef] [PubMed]
- Kanai, Y.; Nittono, H.; Kubo, K.; Sasaki-Aoki, S.; Iwanaga, M. Early somatosensory event-related potentials reveal attentional bias for internal stimuli in social anxiety. Biol. Psychol. 2012, 89, 591–597. [Google Scholar] [CrossRef] [PubMed]
- Center for the Study of Emotion and Attention [CSEA-NIMH]. International Affective Picture System: Digitized Photographs; The Center for Research in Psychophysiology, University of Florida: Gainesvile, FL, USA, 1999. [Google Scholar]
- Schandry, R. Heart beat perception and emotional experience. Psychophysiology 1981, 18, 483–488. [Google Scholar] [CrossRef] [PubMed]
- Harshaw, C. Interoceptive dysfunction: Toward an integrated framework for understanding somatic and affective disturbance in depression. Psychol. Bull. 2015, 141, 311–363. [Google Scholar] [CrossRef] [Green Version]
- Camerer, C.; Ho, T.-H. Experience-weighted attraction learning in normal form games. Econometrica 1999, 67, 827–874. [Google Scholar] [CrossRef] [Green Version]
- Den Ouden, H.E.M.; Daw, N.D.; Elshout, J.A.; Rijpkema, M.; Hoogman, M.; Franke, B.; Cools, R. Dissociable effects of dopamine and serotonin on reversal learning. Neuron 2013, 80, 1090–1100. [Google Scholar] [CrossRef] [Green Version]
- Watanabe, S. Equations of states in singular statistical estimation. Neural Networks 2010, 23, 20–34. [Google Scholar] [CrossRef] [Green Version]
- Neyman, J.; Pearson, E.S. On the problems of the most efficient tests of statistical hypotheses. Philos. Trans. R. Soc. London 1933, 231, 694–796. [Google Scholar]
- Pennebaker, J.W.; Roberts, T.-A. Toward a His and Hers Theory of Emotion: Gender Differences in Visceral Perception. J. Soc. Clin. Psychol. 1992, 11, 199–212. [Google Scholar] [CrossRef]
- Vaitl, D. Interoception. Biol. Psychol. 1996, 42, 1–27. [Google Scholar] [CrossRef]
- Beevers, C.G.; Mullarkey, M.C.; Dainer-Best, J.; Stewart, R.A.; Labrada, J.; Allen, J.J.B.; McGeary, J.E.; Shumake, J. Association between negative cognitive bias and depression: A symptom-level approach. J. Abnorm. Psychol. 2019, 128, 212–227. [Google Scholar] [CrossRef] [PubMed]
- Linden, S.C.; Jackson, M.C.; Subramanian, L.; Healy, D.; Linden, D.E.J. Sad benefit in face working memory: An emotional bias of melancholic depression. J. Affect. Disord. 2011, 135, 251–257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wortha, F.; Azevedo, R.; Taub, M.; Narciss, S. Multiple negative emotions during learning with digital learning environments—Evidence on their detrimental effect on learning from two methodological approaches. Front. Psychol. 2019, 10, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Xie, H.; Jiang, D.; Zhang, D. Individuals with depressive tendencies experience difficulty in forgetting negative material: Two mechanisms revealed by ERP data in the directed forgetting paradigm. Sci. Rep. 2018, 8, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Bechara, A.; Damasio, H.; Tranel, D.; Damasio, A.R. Deciding advantageous before knowing the advantageous strategy. Science 1997, 275, 1293–1294. [Google Scholar] [CrossRef] [Green Version]
- Lavie, N.; Beck, D.M.; Konstantinou, N. Blinded by the load: Attention, awareness and the role of perceptual load. Philos. Trans. R. Soc. B Biol. Sci. 2014, 369, 20130205. [Google Scholar] [CrossRef] [Green Version]
- Meyerholz, L.; Irzinger, J.; Witthöft, M.; Gerlach, A.L.; Pohl, A. Contingent biofeedback outperforms other methods to enhance the accuracy of cardiac interoception: A comparison of short interventions. J. Behav. Ther. Exp. Psychiatry 2019, 63, 12–20. [Google Scholar] [CrossRef]
- Holzel, B.K.; Lazar, S.W.; Gard, T.; Schuman-Olivier, Z.; Vago, D.R.; Ott, U. How does mindfulness meditation work? Proposing mechanisms of action from a conceptual and neural perspective. Perspect. Psychol. Sci. 2011, 6, 537–559. [Google Scholar] [CrossRef]
- Kirk, U.; Montague, P.R. Mindfulness meditation modulates reward prediction errors in a passive conditioning task. Front. Psychol. 2015, 6, 90. [Google Scholar] [CrossRef] [Green Version]
- Terhaar, J.; Campos, F.; Bär, K.; Debener, S. Heartbeat evoked potentials mirror altered body perception in depressed patients. Clin. Neurophysiol. 2012, 123, 1950–1957. [Google Scholar] [CrossRef] [PubMed]
- Zamariola, G.; Maurage, P.; Luminet, O.; Corneille, O. Interoceptive accuracy scores from the heartbeat counting task are problematic: Evidence from simple bivariate correlations. Biol. Psychol. 2018, 137, 12–17. [Google Scholar] [CrossRef] [PubMed]
- Raglan, G.B.; Schulkin, J. Decision making, mindfulness and mood: How mindfulness techniques can reduce the impact of biases and heuristics through improved decision making and positive affect. J. Depress. Anxiety 2014, 4, 12–17. [Google Scholar] [CrossRef]
- Kirk, U.; Downar, J.; Montague, P.R. Interoception drives increased rational decision-making in meditators playing the ultimatum game. Front. Neurosci. 2011, 5, 49. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Pre | Post | ||||
|---|---|---|---|---|---|
| Experiment | Control | t Value | Experiment | Control | |
| Depressive Symptom | |||||
| CES-D | 17.74 (11.05) | 15.08 (7.23) | t(50) = 1.02 (p = 0.31) | ||
| Feeling state | |||||
| DAMS | 8.67 (3.92) | 8.70 (3.37) | t(50) = 0.38 (p = 0.71) | 6.44 (2.87) | 6.32 (3.36) |
| PANAS-PA | 29.81 (5.25) | 29.44 (7.05) | t(50) = 0.22 (p = 0.83) | 26.78 (6.88) | 23.28 (6.74) |
| PANAS-NA | 23.15 (10.03) | 22.08 (7.69) | t(50) = 0.43 (p = 0.67) | 18.26 (7.57) | 16.84 (7.13) |
| Intereception | |||||
| Awareness | 0.56 (0.29) | 0.61 (0.28) | t(50) = −0.55 (p = 0.58) | 0.60 (0.24) | 0.67 (0.24) |
| Attention | 0.02 (0.06) | 0.03 (0.06) | t(50) = −0.68 (p = 0.50) | 0.03 (0.05) | 0.03 (0.05) |
| Reversal learning | |||||
| Learning rate (α) | 0.61 (0.19) | 0.65 (0.19) | t(49) = 0.73 (p = 0.46) | 0.62 (0.16) | 0.65 (0.20) |
| Memory rate (ρ) | 0.31 (0.19) | 0.35 (0.24) | t(49) = −0.50 (p = 0.61) | 0.26 (0.13) | 0.30 (0.23) |
| Exploration rate (β) | 1.47 (0.46) | 1.48 (0.36) | t(49) = −0.02 (p = 0.99) | 1.62 (0.35) | 1.62 (0.35) |
| The number of correct answers | 31.11 (4.36) | 29.72 (6.70) | t(50) = 0.89 (p = 0.38) | 32.69 (3.41) | 31.60 (3.87) |
| Error rate (before reversal) | 0.21 (0.06) | 0.24 (0.08) | t(50) = −1.02 (p = 0.31) | 0.20 (0.08) | 0.22 (0.09) |
| Error rate (after reversal) | 0.26 (0.10) | 0.29 (0.16) | t(50) = 0.89 (p = 0.38) | 0.22 (0.08) | 0.25 (0.09) |
| Symptom | Mood | Interoception | ||||
|---|---|---|---|---|---|---|
| CES-D | DAMS-D | PANAS-PA | PANAS-NA | Attention | Awarness | |
| Symptom | ||||||
| CES-D | 0.702 *** (p = 0.000) | −0.244 † (p = 0.081) | 0.547 *** (p = 0.000) | −0.053 (p = 0.714) | −0.093 (p = 0.513) | |
| Reversal learning parameters | ||||||
| Learning rate (α) | −0.093 (p = 0.514) | −0.099 (p = 0.488) | 0.368 ** (p = 0.008) | 0.176 (p = 0.217) | 0.178 (p = 0.216) | 0.005 (p = 0.970) |
| Memory rate (ρ) | −0.083 (p = 0.561) | 0.124 (p = 0.386) | −0.054 (p = 0.707) | −0.033 (p = 0.818) | −0.116 (p = 0.423) | −0.021 (p = 0.885) |
| Exploration rate (β) | −0.240 † (p = 0.090) | −0.419 ** (p = 0.002) | 0.234 † (p = 0.099) | −0.038 (p = 0.791) | 0.361 * (p = 0.010) | 0.233 † (p = 0.099) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ogishima, H.; Maeda, S.; Tanaka, Y.; Shimada, H. Effects of Depressive Symptoms, Feelings, and Interoception on Reward-Based Decision-Making: Investigation Using Reinforcement Learning Model. Brain Sci. 2020, 10, 508. https://doi.org/10.3390/brainsci10080508
Ogishima H, Maeda S, Tanaka Y, Shimada H. Effects of Depressive Symptoms, Feelings, and Interoception on Reward-Based Decision-Making: Investigation Using Reinforcement Learning Model. Brain Sciences. 2020; 10(8):508. https://doi.org/10.3390/brainsci10080508
Chicago/Turabian StyleOgishima, Hiroyoshi, Shunta Maeda, Yuki Tanaka, and Hironori Shimada. 2020. "Effects of Depressive Symptoms, Feelings, and Interoception on Reward-Based Decision-Making: Investigation Using Reinforcement Learning Model" Brain Sciences 10, no. 8: 508. https://doi.org/10.3390/brainsci10080508