Sex Difference Impacts on the Relationship between Paraoxonase-1 (PON1) and Type 2 Diabetes

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Serum Sampling and Biochemical Assays
2.3. Statistical Analysis
3. Results
3.1. Population Characteristics
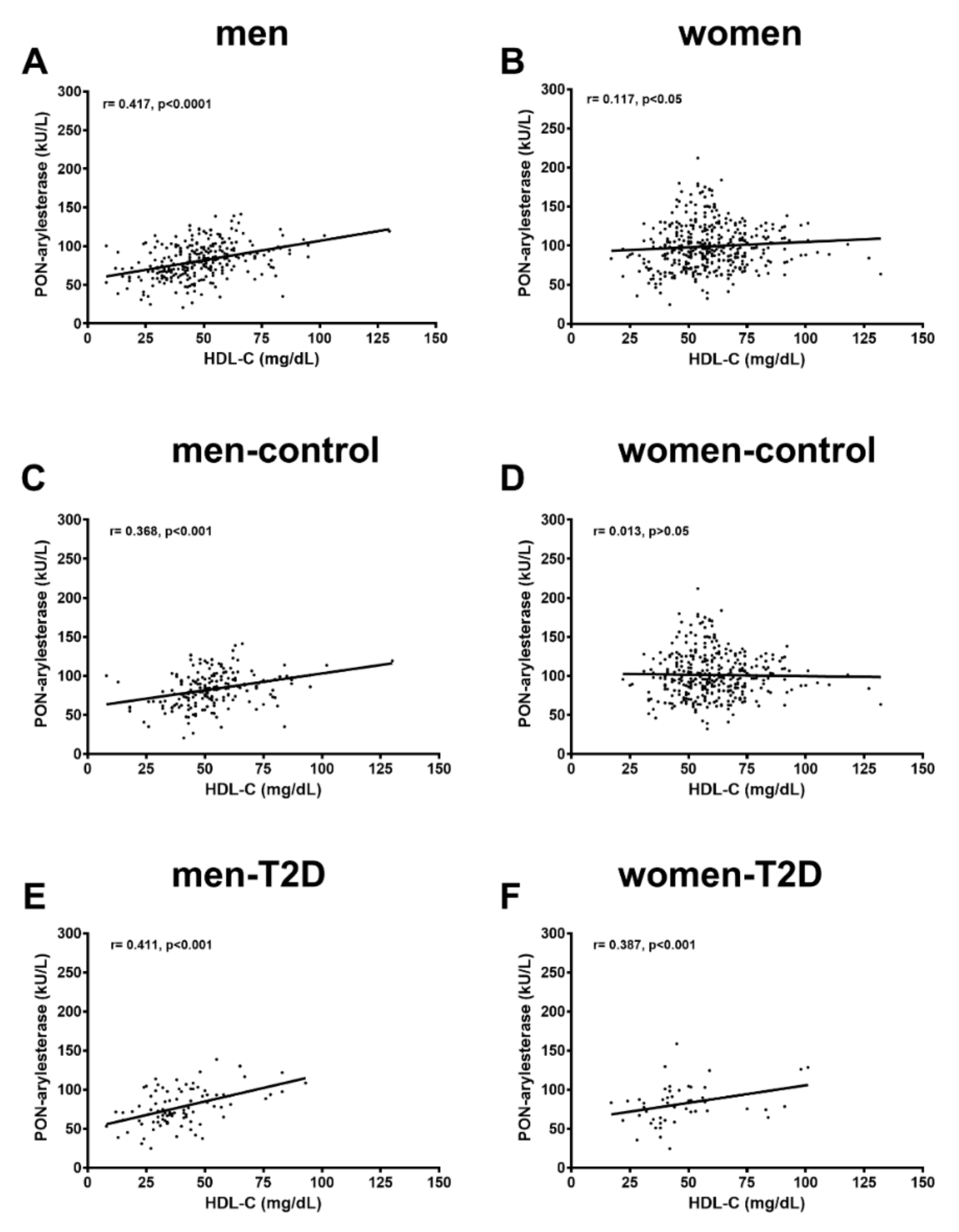
3.2. PON-Arylesterase in Diabetic and Non-Diabetic Women and Men
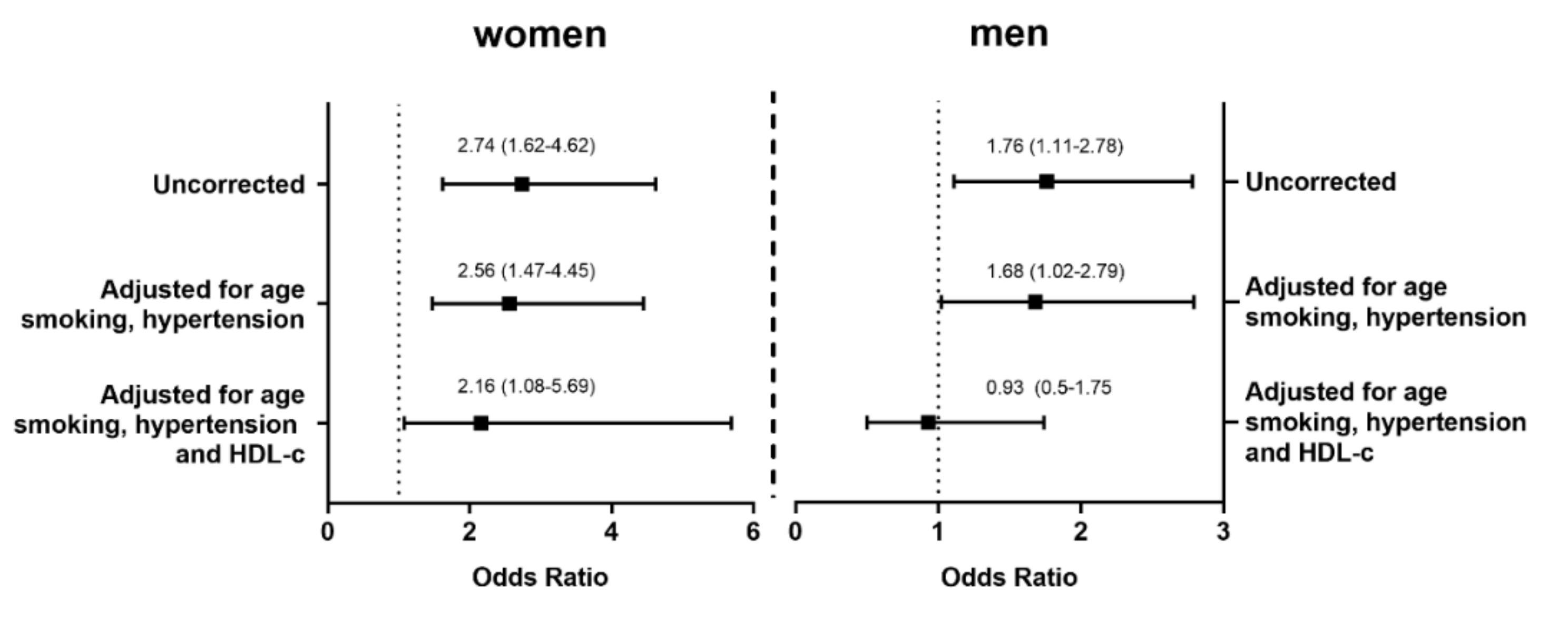
3.3. Logistic Regression Analysis for the Association of PON1 Decrease and T2D in Relation to Sex
4. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Mascarenhas-Melo, F.; Marado, D.; Palavra, F.; Sereno, J.; Coelho, Á.; Pinto, R.; Teixeira-Lemos, E.; Teixeira, F.; Reis, F. Diabetes abrogates sex differences and aggravates cardiometabolic risk in postmenopausal women. Cardiovasc. Diabetol. 2013, 12, 61. [Google Scholar] [CrossRef] [Green Version]
- Gale, E.A.M.; Gillespie, K.M. Diabetes and gender. Diabetologia 2001, 44, 3–15. [Google Scholar] [CrossRef] [Green Version]
- Kautzky-Willer, A.; Harreiter, J.; Pacini, G. Sex and Gender Differences in Risk, Pathophysiology and Complications of Type 2 Diabetes Mellitus. Endocr. Rev. 2016, 37, 278–316. [Google Scholar] [CrossRef] [Green Version]
- Kannel, W.B. Diabetes and cardiovascular disease. The Framingham study. JAMA J. Am. Med. Assoc. 1979, 241, 2035–2038. [Google Scholar] [CrossRef]
- Franconi, F.; Campesi, I.; Occhioni, S.; Tonolo, G. Sex-Gender Differences in Diabetes Vascular Complications and Treatment. Endocr. Metab. Immune Disord. Drug Targets 2012, 12, 179–196. [Google Scholar] [CrossRef] [PubMed]
- Durrington, P.N. Diabetic dyslipidaemia. Baillieres. Best Pr. Res. Clin. Endocrinol. Metab. 1999, 13, 265–278. [Google Scholar] [CrossRef]
- Jenkins, A.J.; Lyons, T.J.; Zheng, D.; Otvos, J.D.; Lackland, D.T.; McGee, D.; Garvey, W.T.; Klein, R.L. DCC/EDIC Research Group Serum lipoproteins in the diabetes control and complications trial/epidemiology of diabetes intervention and complications cohort: Associations with gender and glycemia. Diabetes Care 2003, 26, 810–818. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hovingh, G.K.; de Groot, E.; van der Steeg, W.; Boekholdt, S.M.; Hutten, B.A.; Kuivenhoven, J.A.; Kastelein, J.J.P. Inherited disorders of HDL metabolism and atherosclerosis. Curr. Opin. Lipidol. 2005, 16, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Rosenson, R.S.; Brewer, H.B.; Ansell, B.J.; Barter, P.; Chapman, M.J.; Heinecke, J.W.; Kontush, A.; Tall, A.R.; Webb, N.R. Dysfunctional HDL and atherosclerotic cardiovascular disease. Nat. Rev. Cardiol. 2015, 13, 48–60. [Google Scholar] [CrossRef] [PubMed]
- Pirillo, A.; Catapano, A.L.; Norata, G.D. Biological Consequences of Dysfunctional HDL. Curr. Med. Chem. 2019, 26, 1644–1664. [Google Scholar] [CrossRef]
- Rosenson, R.S.; Stafforini, D.M. Modulation of oxidative stress, inflammation, and atherosclerosis by lipoprotein-associated phospholipase A2. J. Lipid Res. 2012, 53, 1767–1782. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mineo, C.; Shaul, P.W. Novel biological functions of high-density lipoprotein cholesterol. Circ. Res. 2012, 111, 1079–1090. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ebtehaj, S.; Gruppen, E.G.; Parvizi, M.; Tietge, U.J.F.; Dullaart, R.P.F. The anti-inflammatory function of HDL is impaired in type 2 diabetes: Role of hyperglycemia, paraoxonase-1 and low grade inflammation. Cardiovasc. Diabetol. 2017, 16, 132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mackness, M.; Mackness, B. Human paraoxonase-1 (PON1): Gene structure and expression, promiscuous activities and multiple physiological roles. Gene 2015, 567, 12–21. [Google Scholar] [CrossRef] [Green Version]
- Cervellati, C.; Vigna, G.B.; Trentini, A.; Sanz, J.M.; Zimetti, F.; Dalla Nora, E.; Morieri, M.L.; Zuliani, G.; Passaro, A. Paraoxonase-1 activities in individuals with different HDL circulating levels: Implication in reverse cholesterol transport and early vascular damage. Atherosclerosis 2019, 285, 64–70. [Google Scholar] [CrossRef]
- Marín, M.; Moya, C.; Máñez, S. Mutual Influences between Nitric Oxide and Paraoxonase 1. Antioxidants (Basel) 2019, 8, 619. [Google Scholar] [CrossRef] [Green Version]
- Furlong, C.E.; Marsillach, J.; Jarvik, G.P.; Costa, L.G. Paraoxonases-1, -2 and -3: What are their functions? Chem. Biol. Interact. 2016, 259, 51–62. [Google Scholar] [CrossRef] [Green Version]
- Rosenblat, M.; Karry, R.; Aviram, M. Paraoxonase 1 (PON1) is a more potent antioxidant and stimulant of macrophage cholesterol efflux, when present in HDL than in lipoprotein-deficient serum: Relevance to diabetes. Atherosclerosis 2006, 187, 74–81. [Google Scholar] [CrossRef]
- Rosenblat, M.; Gaidukov, L.; Khersonsky, O.; Vaya, J.; Oren, R.; Tawfik, D.S.; Aviram, M. The catalytic histidine dyad of high density lipoprotein-associated serum paraoxonase-1 (PON1) is essential for PON1-mediated inhibition of low density lipoprotein oxidation and stimulation of macrophage cholesterol efflux. J. Biol. Chem. 2006, 281, 7657–7665. [Google Scholar] [CrossRef] [Green Version]
- Tavori, H.; Khatib, S.; Aviram, M.; Vaya, J. Characterization of the PON1 active site using modeling simulation, in relation to PON1 lactonase activity. Bioorg. Med. Chem. 2008, 16, 7504–7509. [Google Scholar] [CrossRef]
- Lyons, T.J.; Li, W.; Wells-Knecht, M.C.; Jokl, R. Toxicity of mildly modified low-density lipoproteins to cultured retinal capillary endothelial cells and pericytes. Diabetes 1994, 43, 1090–1095. [Google Scholar] [CrossRef] [PubMed]
- Kattoor, A.J.; Goel, A.; Mehta, J.L. LOX-1: Regulation, Signaling and Its Role in Atherosclerosis. Antioxid. (Basel) 2019, 8, 218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trentini, A.; Bellini, T.; Bonaccorsi, G.; Cavicchio, C.; Hanau, S.; Passaro, A.; Cervellati, C. Sex difference: An important issue to consider in epidemiological and clinical studies dealing with serum paraoxonase-1. J. Clin. Biochem. Nutr. 2019, 64, 250–256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costa, L.G.; Vitalone, A.; Cole, T.B.; Furlong, C.E. Modulation of paraoxonase (PON1) activity. Biochem. Pharm. 2005, 69, 541–550. [Google Scholar] [CrossRef]
- Cheng, X.; Klaassen, C.D. Hormonal and chemical regulation of paraoxonases in mice. J. Pharm. Exp. 2012, 342, 688–695. [Google Scholar] [CrossRef] [Green Version]
- Ahmad, S.; Scott, J.E. Estradiol enhances cell-associated paraoxonase 1 (PON1) activity in vitro without altering PON1 expression. Biochem. Biophys. Res. Commun. 2010, 397, 441–446. [Google Scholar] [CrossRef] [Green Version]
- Wamique, M.; Ali, W.; Himanshu, D. Association of SRB1 and PON1 gene polymorphisms with type 2 diabetes mellitus: A case control study. Int. J. Diabetes Dev. Ctries. 2020. [Google Scholar] [CrossRef]
- Mastorikou, M.; Mackness, B.; Liu, Y.; Mackness, M. Glycation of paraoxonase-1 inhibits its activity and impairs the ability of high-density lipoprotein to metabolize membrane lipid hydroperoxides. Diabet. Med. 2008, 25, 1049–1055. [Google Scholar] [CrossRef] [Green Version]
- Camps, J.; Marsillach, J.; Joven, J. The paraoxonases: Role in human diseases and methodological difficulties in measurement. Crit. Rev. Clin. Lab. Sci. 2009, 46, 83–106. [Google Scholar] [CrossRef]
- Stefanović, A.; Kotur-Stevuljević, J.; Spasić, S.; Vekić, J.; Zeljković, A.; Spasojević-Kalimanovska, V.; Jelić-Ivanović, Z. HDL 2 particles are associated with hyperglycaemia, lower PON1 activity and oxidative stress in type 2 diabetes mellitus patients. Clin. Biochem. 2010, 43, 1230–1235. [Google Scholar] [CrossRef]
- Ferretti, G.; Bacchetti, T.; Busni, D.; Rabini, R.A.; Curatola, G. Protective Effect of Paraoxonase Activity in High-Density Lipoproteins against Erythrocyte Membranes Peroxidation: A Comparison between Healthy Subjects and Type 1 Diabetic Patients. J. Clin. Endocrinol. Metab. 2004, 89, 2957–2962. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cervellati, C.; Pansini, F.S.; Bonaccorsi, G.; Bergamini, C.M.; Patella, A.; Casali, F.; Fantini, G.F.; Pascale, G.; Castaldini, C.; Ferrazzini, S.; et al. 17β-estradiol levels and oxidative balance in a population of pre-, peri-, and post-menopausal women. Gynecol. Endocrinol. 2011, 27, 1028–1032. [Google Scholar] [CrossRef]
- Cervellati, C.; Bonaccorsi, G.; Trentini, A.; Valacchi, G.; Sanz, J.M.; Squerzanti, M.; Spagnolo, M.; Massari, L.; Crivellari, I.; Greco, P.; et al. Paraoxonase, arylesterase and lactonase activities of paraoxonase-1 (PON1) in obese and severely obese women. Scand. J. Clin. Lab. Invest. 2018, 78, 18–24. [Google Scholar] [CrossRef] [PubMed]
- Castellazzi, M.; Trentini, A.; Romani, A.; Valacchi, G.; Bellini, T.; Bonaccorsi, G.; Fainardi, E.; Cavicchio, C.; Passaro, A.; Zuliani, G.; et al. Decreased arylesterase activity of paraoxonase-1 (PON-1) might be a common denominator of neuroinflammatory and neurodegenerative diseases. Int. J. Biochem. Cell Biol. 2016, 81, 356–363. [Google Scholar] [CrossRef]
- Patra, S.K.; Singh, K.; Singh, R. Paraoxonase 1: A better atherosclerotic risk predictor than HDL in type 2 diabetes mellitus. Diabetes Metab. Syndr. 2013, 7, 108–111. [Google Scholar] [CrossRef] [PubMed]
- Abbott, C.A.; Mackness, M.I.; Kumar, S.; Boulton, A.J.; Durrington, P.N. Serum Paraoxonase Activity, Concentration, and Phenotype Distribution in Diabetes Mellitus and Its Relationship to Serum Lipids and Lipoproteins. Arter. Thromb. Vasc. Biol. 1995, 15, 1812–1818. [Google Scholar] [CrossRef]
- Ikeda, Y.; Suehiro, T.; Inoue, M.; Nakauchi, Y.; Morita, T.; Arii, K.; Ito, H.; Kumon, Y.; Hashimoto, K. Serum paraoxonase activity and its relationship to diabetic complications in patients with non—Insulin-dependent diabetes mellitus. Metabolism 1998, 47, 598–602. [Google Scholar] [CrossRef]
- Tisato, V.; Romani, A.; Tavanti, E.; Melloni, E.; Milani, D.; Bonaccorsi, G.; Sanz, J.M.; Gemmati, D.; Passaro, A.; Cervellati, C. Crosstalk Between Adipokines and Paraoxonase 1: A New Potential Axis Linking Oxidative Stress and Inflammation. Antioxidants 2019, 8, 287. [Google Scholar] [CrossRef] [Green Version]
- Marsillach, J.; Costa, L.G.; Furlong, C.E. Paraoxonase-1 and Early-Life Environmental Exposures. Ann. Glob. Heal. 2016, 82, 100–110. [Google Scholar] [CrossRef]
- Luo, J.-Q.; Ren, H.; Liu, M.-Z.; Fang, P.-F.; Xiang, D.-X. European versus Asian differences for the associations between paraoxonase-1 genetic polymorphisms and susceptibility to type 2 diabetes mellitus. J. Cell. Mol. Med. 2018, 22, 1720–1732. [Google Scholar] [CrossRef] [Green Version]
- Koren-Gluzer, M.; Aviram, M.; Meilin, E.; Hayek, T. The antioxidant HDL-associated paraoxonase-1 (PON1) attenuates diabetes development and stimulates β-cell insulin release. Atherosclerosis 2011, 219, 510–518. [Google Scholar] [CrossRef] [PubMed]
- Shokri, Y.; Variji, A.; Nosrati, M.; Khonakdar-Tarsi, A.; Kianmehr, A.; Kashi, Z.; Bahar, A.; Bagheri, A.; Mahrooz, A. Importance of paraoxonase 1 (PON1) as an antioxidant and antiatherogenic enzyme in the cardiovascular complications of type 2 diabetes: Genotypic and phenotypic evaluation. Diabetes Res. Clin. Pr. 2020, 161, 108067. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, S.D.; Hung, N.D.; Cheon-Ho, P.; Ree, K.M.; Dai-Eun, S. Oxidative inactivation of lactonase activity of purified human paraoxonase 1 (PON1). Biochim. Biophys. Acta 2009, 1790, 155–160. [Google Scholar] [CrossRef] [PubMed]
- Perségol, L.; Vergès, B.; Foissac, M.; Gambert, P.; Duvillard, L. Inability of HDL from type 2 diabetic patients to counteract the inhibitory effect of oxidised LDL on endothelium-dependent vasorelaxation. Diabetologia 2006, 49, 1380–1386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sorrentino, S.A.; Besler, C.; Rohrer, L.; Meyer, M.; Heinrich, K.; Bahlmann, F.H.; Mueller, M.; Horváth, T.; Doerries, C.; Heinemann, M.; et al. Endothelial-vasoprotective effects of high-density lipoprotein are impaired in patients with type 2 diabetes mellitus but are improved after extended-release niacin therapy. Circulation 2010, 121, 110–122. [Google Scholar] [CrossRef] [Green Version]
- Connelly, P.W.; Zinman, B.; Maguire, G.F.; Mamakeesick, M.; Harris, S.B.; Hegele, R.A.; Retnakaran, R.; Hanley, A.J.G. Association of the novel cardiovascular risk factors paraoxonase 1 and cystatin C in type 2 diabetes. J. Lipid Res. 2009, 50, 1216–1222. [Google Scholar] [CrossRef] [Green Version]
- Yang, X.P.; Reckelhoff, J.F. Estrogen, hormonal replacement therapy and cardiovascular disease. Curr. Opin. Nephrol. Hypertens. 2011, 20, 133–138. [Google Scholar] [CrossRef] [Green Version]
- Panico, S.; Mattiello, A. Epidemiology of cardiovascular diseases in women in Europe. Nutr. Metab. Cardiovasc. Dis. 2010, 20, 379–385. [Google Scholar] [CrossRef]
- bin Ali, A.; Zhang, Q.; Lim, Y.K.; Fang, D.; Retnam, L.; Lim, S.-K. Expression of major HDL-associated antioxidant PON-1 is gender dependent and regulated during inflammation. Free Radic. Biol. Med. 2003, 34, 824–829. [Google Scholar] [CrossRef]
- James, R.W.; Deakin, S.P. The importance of high-density lipoproteins for paraoxonase-1 secretion, stability, and activity. Free Radic. Biol. Med. 2004, 37, 1986–1994. [Google Scholar] [CrossRef]
- Passaro, A.; Vigna, G.B.; Romani, A.; Sanz, J.M.; Cavicchio, C.; Bonaccorsi, G.; Valacchi, G.; Cervellati, C. Distribution of Paraoxonase-1 (PON-1) and Lipoprotein Phospholipase A2 (Lp-PLA2) across Lipoprotein Subclasses in Subjects with Type 2 Diabetes. Oxid. Med. Cell. Longev. 2018, 2018, 1752940. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Whole Population | Women | Men | ||||
|---|---|---|---|---|---|---|
| Controls (n = 581) | T2D (n = 197) | Controls (n = 383) | Diabetes (n = 79) | Controls (n = 198) | Diabetes (n = 118) | |
| Age, years | 64 ± 12 | 65 ± 10 | 63 ± 11 | 64 ± 11 | 67 ± 11 | 67 ± 10 |
| Hypertension, n (%) | 233 (40) | 161 (81) a | 138 (36) | 62 (72) a | 95 (48) | 99 (84) a |
| CVD, n (%) | 29 (5) | 56 (28) a | 10 (3) | 20 (25) a | 18 (9) | 36 (31) a |
| Smoking, n (%) | 121 (21) | 29 (15) | 88 (23) | 15 (19) | 45 (23) | 13 (11) b |
| Glucose, mg/dL * | 95 ± 11 | 141 ± 38 a | 93 ± 10 | 129 ± 35 | 98 ± 10 a | 146 ± 38 a |
| Lipid lowering drugs § | 127 (20) | 130 (66) a | 107 (28) | 39 (50) a | 20 (10) | 91 (77) a |
| Lipid profile # | ||||||
| HDL-c, mg/dL | 56 (47–67) | 40 (31–65) a | 58 (50–69) | 42 (38–56) a | 52 (44–60) | 37 (30–47) a |
| LDL-C, mg/dL | 132 ± 35 | 113 ± 42 a | 136 ± 32 | 126 ± 46 b | 124 ± 38 | 106 ± 37 a |
| Triglycerides, mg/dL | 91 (69–129) | 148 (103–215) a | 90 (70–123) | 147 (112–203) a | 92 (68–119) | 149 (99–225) a |
| Total cholesterol, mg/dL | 210 ± 40 | 190 ± 45 a | 217 ± 37 | 208 ± 46 | 194 ± 41 | 180 ± 41 a |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rosta, V.; Trentini, A.; Passaro, A.; Zuliani, G.; Sanz, J.M.; Bosi, C.; Bonaccorsi, G.; Bellini, T.; Cervellati, C. Sex Difference Impacts on the Relationship between Paraoxonase-1 (PON1) and Type 2 Diabetes. Antioxidants 2020, 9, 683. https://doi.org/10.3390/antiox9080683
Rosta V, Trentini A, Passaro A, Zuliani G, Sanz JM, Bosi C, Bonaccorsi G, Bellini T, Cervellati C. Sex Difference Impacts on the Relationship between Paraoxonase-1 (PON1) and Type 2 Diabetes. Antioxidants. 2020; 9(8):683. https://doi.org/10.3390/antiox9080683
Chicago/Turabian StyleRosta, Valentina, Alessandro Trentini, Angelina Passaro, Giovanni Zuliani, Juana Maria Sanz, Cristina Bosi, Gloria Bonaccorsi, Tiziana Bellini, and Carlo Cervellati. 2020. "Sex Difference Impacts on the Relationship between Paraoxonase-1 (PON1) and Type 2 Diabetes" Antioxidants 9, no. 8: 683. https://doi.org/10.3390/antiox9080683